exploring the work of nurses who administer chemotherapy ... · exploring the work of nurses who...
TRANSCRIPT

Exploring the Work of
Nurses who Administer
Chemotherapy:
A Multi-Method Study December 2005
D
Dr Theresa Wiseman
Ms Rebecca Verity
Dr Emma Ream
Miss Emma Alderman
Professor Alison Richardson

ii
This study was supported by a European Oncology Nursing Society (EONS/Roche) grant (research award) and funding from King’s College London. This report should be referenced as: Wiseman T, Verity R, Ream E, Alderman E, Richardson A. (2005) “Exploring the work of nurses who administer chemotherapy: A multi-method study”. London: King’s College London December 2005 © King’s College London

iii
Acknowledgements We would like to express our gratitude to all the nurses & patients who participated in this study, without their enthusiasm and honesty this study would not have been possible. Particular thanks go to the lead nurses for their help in the recruitment process. We are grateful for the grant from EONS/Roche. The money that came with this grant provided the foundation with which to undertake this work and was augmented with resources from the Florence Nightingale School of Nursing and Midwifery, King’s College London.

iv
Contents Section Page 1 Introduction and Aims.............................................................................................................. 1
Introduction ................................................................................................................................. 1
Purpose of the study ................................................................................................................... 2
2 Literature Review .................................................................................................................... 3
Introduction ................................................................................................................................. 3
The Literature Search ................................................................................................................. 3
The Chemotherapy Process........................................................................................................ 3
The Role and Responsibilities of the Nurse................................................................................. 4
Chemotherapy Treatment Environment....................................................................................... 5
Patient Satisfaction, Education and Communication ................................................................... 6
Communication and Patient Psychological Support .................................................................... 6
Nurses’ Attitudes towards Chemotherapy and Cancer ................................................................ 7
Nurses’ Concerns and Feelings .................................................................................................. 8
Occupational Risks of Exposure.................................................................................................. 9
Attitudes towards Occupational Risks of Exposure.................................................................... 10
Chemotherapy Administration Errors ........................................................................................ 10
Preparation and Support for the Role........................................................................................ 11
Conclusion ................................................................................................................................ 12
3 Method.................................................................................................................................. 14
Introduction ............................................................................................................................... 14
Component One - Survey.......................................................................................................... 14
Survey aims .......................................................................................................................... 14
Rationale for Survey Methodology......................................................................................... 14
Survey Instrument and Design .............................................................................................. 14
Questionnaire Development .................................................................................................. 15
Revisions Made To Original Questionnaire ........................................................................... 16
Population and Sample ......................................................................................................... 16
Study Sites and Setting ......................................................................................................... 16
Sample Size.......................................................................................................................... 17
Ascertaining and Accessing Sample ..................................................................................... 17
Procedures for Survey Administration ................................................................................... 18
Reliability and Validity ........................................................................................................... 19
Pre-test ................................................................................................................................. 20
Data Preparation ................................................................................................................... 20

v
Ethical and Research Governance Approval ......................................................................... 21
Component two – ethnography ................................................................................................. 22
Aims of the ethnography ....................................................................................................... 22
Rationale for ethnographic method ........................................................................................... 22
The settings .............................................................................................................................. 22
Participants ........................................................................................................................... 23
Data Collection.......................................................................................................................... 23
Analysis .................................................................................................................................... 24
Issues of Rigour .................................................................................................................... 24
Ethical considerations and approvals ........................................................................................ 24
Time Frame for Both Elements ................................................................................................. 25
Study Activities.......................................................................................................................... 25
4 Results from component 1..................................................................................................... 26
Introduction ............................................................................................................................... 26
Response rate........................................................................................................................... 26
Sample demographics .............................................................................................................. 26
Respondents Educational Preparation ...................................................................................... 29
Pre-registration...................................................................................................................... 29
Post-registration .................................................................................................................... 29
Formal Chemotherapy Education.......................................................................................... 31
Feelings towards chemotherapy administration......................................................................... 33
Issues of Practice...................................................................................................................... 34
Support for Nurses ................................................................................................................ 35
Worries about administering Chemotherapy.............................................................................. 36
Cross tabulations .................................................................................................................. 37
Non-Parametric tests – Mann Whitney .................................................................................. 39
Attitudes towards Chemotherapy administration ....................................................................... 39
Cross tabulations – Somer’s d............................................................................................... 41
Non-Parametric tests determining difference in attitudes....................................................... 42
Ordinal Regression ................................................................................................................... 43
5 Results from Component two – ethnography......................................................................... 47
Introduction ............................................................................................................................... 47
Chemotherapy Day Unit 1 (CDU 1) ........................................................................................... 47
Factors which facilitate nurses’ work ..................................................................................... 47
Factors which impinge on the work of chemotherapy nurses - CDU 1...................................... 52
Chemotherapy Day Unit 2 (CDU 2) ........................................................................................... 53
Factors which facilitate nurses’ work ......................................................................................... 53
Factors which impinge on nurses’ work (CDU 2)...................................................................... 54

vi
Conclusion ................................................................................................................................ 58
5 Discussion............................................................................................................................. 58
Introduction ............................................................................................................................... 59
Summary of Findings ................................................................................................................ 59
Feelings, Attitudes and Beliefs .............................................................................................. 59
The nature and extent of educational preparation ................................................................. 60
The challenges of chemotherapy administration ....................................................................... 61
Limitations of the study ............................................................................................................. 62
Component One.................................................................................................................... 62
Component Two.................................................................................................................... 63
Implications for Practice and Recommendations....................................................................... 63
Conclusion ................................................................................................................................ 64
6 References............................................................................................................................ 65
7 Appendices ........................................................................................................................... 71
Appendix 1: Questionnaire ................................................................................................I
Appendix 2: Revisions to Questions.................................................................................II
Appendix 3: Questions Added.........................................................................................III
Appendix 4: Information for Lead Cancer Nurses .......................................................... IV
Appendix 5: Cover letter to participants........................................................................... V
Appendix 6: Nurse Information Sheet............................................................................. VI

vii
Figures Figure 4.1 Frequency of Chemotherapy Administration.......................................................... 27
Figure 4.2 Chemotherapy Teaching Format.............................................................................. 30
Figure 4.3 Formats for Further Education................................................................................. 32
Figure 4.4 Support of nurses with regards to their queries and concerns about
chemotherapy administration ............................................................................................ 35
Figure 4.5 Nursing support for decisions not to give chemotherapy...................................... 36
Figure 4.7 Nurses’ Response to Attitude Statements .............................................................. 41

viii
TABLES Table 3.1: Example questions and response formats .............................................................. 15
Table 3.2: Number of hospital sites and nurses who administer chemotherapy within each
London Cancer Network............................................................................................................. 18
Table 3.3: Time Frame for Both Elements................................................................................. 25
Table 4.1 Response rate across Cancer Networks................................................................... 26
Table 4.2 Response rate across hospital sites ......................................................................... 26
Table 4.3 Sample Characteristics .............................................................................................. 27
Table 4.4 Distribution of clinical areas within the sample........................................................ 28
Table 4.5 Nursing grade ............................................................................................................. 28
Table 4.6 Professional qualifications obtained or currently being undertaken...................... 28
Table 4.7 Amount of chemotherapy education of those in receipt of some pre-registration
training. ....................................................................................................................................... 29
Table 4.8 Adequacy of the amount of chemotherapy teaching pre-registration .................... 29
Table 4.9 Amount of chemotherapy education of those in receipt of some post-registration
training ........................................................................................................................................ 30
Table 4.10 Adequacy of the amount of chemotherapy teaching post-registration ................ 30
Table 4.11 Formal chemotherapy education received and further education required. ........ 31
Table 4.12 Most important issues of chemotherapy education as rated sample ................... 33
Table 4.13 Feelings about Administering Chemotherapy ........................................................ 33
Table 4.14 Reasons given as to when it is not safe to administer chemotherapy ................. 34
Table 4.15: Frequency of those who felt supported in decision to not give chemotherapy.. 35
Table 4.16 Associations between nursing grade and worries ................................................. 38
Table 4.17 Cross tabulations between nursing grade and not worrying about chemotherapy
administration ............................................................................................................................. 38
Table 4.18 Associations between clinical area and worries .................................................... 38
Table 4.19 Cross tabulations between clinical area and worries............................................. 39
Table 4.20 Attitudes towards chemotherapy administration ................................................... 40
Table 4.21 Significant associations between attitude and nursing grade .............................. 42
Table 4.22 Significant associations between attitudes and place of work ............................. 42
Table 4.23 Mann Whitney results- Attitude by chemotherapy experience.............................. 43
Table 4. 24 Ordinal regression model for worries about chemotherapy role ......................... 44
Table 4.26a Ordinal regression model for attitudes towards chemotherapy (Site and Educational
level)................................................................................................................................................................ 45
Table 4.26b Ordinal regression model for attitudes towards chemotherapy (Nursing grade and
Experience) .................................................................................................................................................... 46

1
1 Introduction and Aims
Introduction
Chemotherapy is presently the main systemic treatment available to treat cancer. Of the one in three people diagnosed with cancer (Department of Health, 2002) approximately 60% will receive chemotherapy as part of their treatment (Bremnes, 1999). It is, however, a treatment that can potentially cause much harm, both to those receiving it and those administering it. Over the last two decades chemotherapy administration has increasingly become the role of the nurse. Nurses have four main roles in the chemotherapy administration process: educating patients and their families about this form of therapy, administering the chemotherapy agents safely and managing any side effects patients may have (Tanghe et al., 1994). In addition, nurses need to support patients emotionally through the process (Dennison, 1995; Richardson, 1996; Wilkinson, 1991) A number of studies have indicated that patients are often unsatisfied with aspects of the chemotherapy administration process including communication and psychological support; waiting times; assessment and management of side effects; and information giving (see for example (Mun et al., 2001; Sitza & Wood, 1998a). Although nurses are competent in providing information, they rarely make any assessment of patients’ feelings about their treatment (Dennison, 1995). In addition, poor management of chemotherapy induced side effects, such as nausea and vomiting has been shown to adversely affect patients’ quality of life (Brown et al., 2001; Richardson, Marks, & Levine, 1998) and levels of anxiety about treatment (Mun et al., 2001). However, when patients are assessed, given information and their side effects managed effectively, their anxieties decrease and their compliance with treatment improves (Sitza & Wood, 1998a). One area patients are rarely dissatisfied with is the nursing skills involved in the technical aspects of chemotherapy administration (Mun et al., 2001). When trying to explain their findings researchers have identified a need to explore the chemotherapy process in more depth. While there is research investigating patient satisfaction with chemotherapy nursing care there is currently a dearth of research from nurses’ perspectives. It is argued that to give quality emotional and physical support to the individual with cancer and their families, the nurse’s perception and experience of work in this field of care needs to be explored in some depth (McCray, 1997). Recent national clinical guidelines for the administration of cytotoxic chemotherapy recommended that more research is urgently required to understand factors which may influence effective practice. Two areas particularly highlighted were:
• Nature of staff and others’ beliefs and knowledge deficits
• Impact on practice of beliefs, knowledge and knowledge deficits (Goodman, 1998a)
Some of these issues were explored using an investigator designed, self-completion, questionnaire sent to 260 nurses working within a specialist cancer hospital (Verity, 2002). Results showed that factors influencing patient care included; staff education and experience, pressures of time and workload, nurses receiving regular knowledge updates; and working with more experienced and knowledgeable nurses. The findings also suggested that nurses who were educationally prepared and underwent practice supervision had a positive attitude towards their role in chemotherapy. There also

2
appeared to be wide variation in educational preparation for the role, a cause for concern, given the implications of chemotherapy administration. Although this study was useful in terms of its findings, it was a small, local, study so the results cannot be generalized. Care that was once delivered in hospital is now being delivered in busy outpatient settings due to reduced resources, increasing monetary constraints, increased workload and increased demand for treatment (Fitzsimmons et al., 2002). Administration of chemotherapy is one such area where restructuring of services has led to the majority of patients now receiving chemotherapy in outpatient departments. As chemotherapy regimes have developed and become more amenable to delivery in an out patient setting, it is important that current chemotherapy practice be examined to understand factors which may impinge or enhance care received by patients. Evaluation of the role of nurses is imperative because it can inform decision-making, influence educational programme development and ultimately impact on nursing practice (Kearney, 2000).
Purpose of the study
This overall purpose of this study was to explore the process and context of nurses administering cytotoxic chemotherapy. The study sought to:
• Observe and describe nurses’ practice of chemotherapy administration.
• Explore attitudes, feelings and beliefs of nurses’ administering chemotherapy.
• Highlight any discrepancies between attitudes and behaviours.
• Understand the factors that contribute to these discrepancies. In order to fulfil these aims methodological and investigator triangulation was considered necessary; this research therefore, consisted of two elements. Element one involved undertaking a questionnaire survey to investigate nurses’ perspectives of administering chemotherapy. Element two was an ethnographic study exploring the work of nurses in two chemotherapy outpatient settings. This allowed for collection of both quantitative and qualitative data which, it was believed, would lead to a more comprehensive understanding of chemotherapy administration from a nurse’s perspective. In addition, the use of more than one research strategy would enable more robust testing of the validity and reliability of research findings (Aldridge & Levine, 2001)

3
2 Literature Review
Introduction
Cytotoxic chemotherapy is the main systemic treatment currently used to treat cancer. It is a treatment, which can without exception, cause extreme harm to patients, staff and the environment if the drugs are not prescribed, handled and administered safely and correctly. It continues to be a rapidly expanding treatment modality for many malignant and some non-malignant diseases. Treatment regimes are also becoming increasingly complex. Nurses are undertaking this role not only in specialist cancer centres but also in general hospital settings and the community. Furthermore, chemotherapy is now more likely to be administered on an outpatient basis; this trend will continue to rise over the coming years due to the significant increasing numbers of patients receiving chemotherapy and financial constraints (Taylor & Birch, 2004) While oncology nurses have appeared to embrace this extended role there has been little work exploring nurses’ experiences, attitudes and feelings in relation to the chemotherapy administration process. Little is also known nationally in the UK about the educational standards, needs and competence of practitioners in this area, due to a dearth of research and audit findings. To clarify the purpose and rationale for this study this next section will critically examine the available past and current literature within the area of the nurses’ role in chemotherapy administration.
The Literature Search
Extensive searches were undertaken through the following databases:
• The Cumulative Index to Nursing and Allied Health Literature (CINAHL) 1982- August 2005
• Medline 1975-August 2005 Key words used included: cytotoxic, chemotherapy, antineoplastic agents/adverse effects, neoplasm’s/drug therapy, education, stress, burnout, communication, oncology nurses/nursing, cancer nursing/nurses; drug administration; occupational risk/exposure, quality assurance, patient satisfaction, outpatients, nurse-led clinics.
The Chemotherapy Process
Administering cytotoxic drugs should be viewed more as process rather than the isolated act of just giving these drugs to patients (Goodman, 1998b; Grundy, 1999)The findings of a quality assurance case study undertaken by (Tanghe et al., 1996) identified that chemotherapy administration is a four-stage process incorporating the prescribing of the drug, preparation, administration and post-chemotherapy assessment. The Royal College of Nursing (RCN) guidelines for the administration of chemotherapy state that this process incorporates three components, that of the drug, patient and staff pathways, which converge at the point of administration (Goodman, 1998b). While Tanghe et al (1996) contend that nurses are involved in this process from the point of preparation of the drug; it is argued that nurses are involved in the prescription phase of these drugs, for example

4
ensuring informed consent, assessing patient fitness for treatment and checking that the prescription is correct. It should also be recognised that nurses are not the only health-care professionals involved within this process. Goodman (1998b) suggests that it is a collaborative activity involving a multi-disciplinary approach and should always involve the patient.
The Role and Responsibilities of the Nurse
Where once chemotherapy administration was the domain of doctors it has been the nurse in the last two decades who is responsible for ensuring that patients receive their treatments safely. During this time there have been significant changes in the number of patients undergoing chemotherapy treatments and the way it is administered. Tanghe et al (1994) suggest that the nurse has three main roles in the chemotherapy administration process (to educate patients, administer and manage side effects). It is also identified that nurses must provide emotional support to patients and their relatives (Dennison, 1995; Wilkinson, 1991) and act as a facilitator of learning and a role model to less experienced staff (Verity & Bloomfield, 2005). Other nursing responsibilities include taking all necessary actions to ensure that the environment and the nurse themselves are safe, e.g. disposing of waste safely and wearing protective clothing. Nurses therefore have a legal and professional responsibility to feel competent in this role and follow all of the procedures laid down by the organisation within which they work, to ensure the safe handling, delivery and disposal of cytotoxic drugs (Allwood, Stanley, & Wright, 2002)
Developments in chemotherapy practice and increasing numbers of patients receiving chemotherapy in the UK will mean that many more nurses are needed in various clinical settings to undertake this role. Worryingly it has been reported that there is a national shortage of qualified nurses working in this area (Taylor & Birch, 2004). What is apparent is that oncology nurses are playing a pivotal role in the rapid developments occurring in chemotherapy practice and as such the role is continually evolving. Hence we are also now seeing an increasing number of nurse-led chemotherapy clinics (Fitzsimmons et al., 2005; Harrold, 2002; Munro, 2005) and chemotherapy triage telephone services (Groves, 2005). Future developments for the nurses’ role have also emerged in the literature. Taylor and Birch (2004) describe the implementation of a new pilot role that of chemotherapy support worker (CSW), this initiative involved extending the role of the health care assistant (HCA). The HCA was provided with knowledge and skills to then support the nursing team but not actually administer chemotherapy in the chemotherapy setting. The educational support received appears comprehensive and was delivered over a four-day HCA ‘training in cancer care course’ and then a further ten specific study days to meet identified learning needs. Clinical skills, such as cannulation, flushing lines and disconnecting treatment, were taught in the clinical area and supported by an experienced practitioner acting as an enthusiastic mentor. Overall, this initiative was positively evaluated and the CSW was viewed as a valuable addition to the team, so much so that Taylor and Birch (2004) contend that this role in the future could be expanded to include administrating chemotherapy. With the advent NHS Knowledge and Skills Framework (Skills for Health, 2005), this is plausible. The role of the nurse in the chemotherapy process should be explored to ensure future developments, such as the CSW, role are properly developed and supported in other clinical settings.

5
Chemotherapy Treatment Environment
Chemotherapy is administered to patients in both inpatient and outpatient settings. However, over the last two decades the rising trend has been to administer chemotherapy in out-patient and day care settings, in the community, and in patients’ own homes. While this is because of the increasing numbers of patients receiving chemotherapy and the subsequent financial implications (Wood, Hyde, & Salter, 2005), it is mainly feasible due to more sophisticated delivery methods, new oral preparations of these drugs and improved management of side-effects enabling patients to tolerate their treatments without the need for being hospitalised. Very few chemotherapy treatments now actually need to be administered in an inpatient setting (Allwood et al., 2002). These changes in chemotherapy delivery settings however, have significant implications for the management of these patients and for the nurses caring for them. Patients who are receiving their treatments as an outpatient and in their homes are likely to face problems alone with limited opportunities to receive support from specialists who work with chemotherapy. They will therefore require from health professionals detailed information and education on how to manage side effects and how to recognise when medical intervention is required. However, Dennison & Shute (2000) found that the nurse’s role in the general oncology outpatient setting tends to focus on non-nursing duties, including administration, chaperoning and organising notes rather than supporting and educating patients. Blay, Cairns, Chisholm, & O'Baugh's (2002) study, undertaken in Australia, investigated the workload and roles of oncology nurses within an outpatient setting where treatment was also given. They found that over 60% of the nurses’ time was spent on indirect nursing activities, as also observed in Dennison and Shute’s (2000) study. McCaughan & Thompson (2000) argue that the challenge for nurses in the chemotherapy outpatient setting is finding ways to organise the service so that patients are given the appropriate information and guidance to ensure promotion of self-care whilst having treatments that can cause life-threatening and/or debilitating side effects. Interestingly, little consideration has actually been given to the physical environment where chemotherapy is administered. Allwood et al (2002) contend that it is often frequently inadequate. Unless the chemotherapy outpatient setting has been specifically designed with the administration of chemotherapy in mind (which few have been), chemotherapy is often administered in areas too small to cope with the increasing numbers of patients and with little consideration to the safety aspects of administering these drugs (Allwood et al., 2002). Many inpatient settings are also inappropriate and patients can receive their treatments on general wards (unless in specialist centres) where there are competing patient care priorities for the nurses, such as caring for a dying patient whilst trying to ensure the chemotherapy is administered on time (Allwood et al., 2002). Mohan et al (2005) found that nurses caring for patients with cancer in non-specialist wards had concerns related to their lack of knowledge about treatments and hence felt that they were not able to support patients and relatives appropriately. These nurses also believed that patients would feel better cared for in an environment where they could share their experiences with others in similar situations (Mohan, Wilkes, & Walker, 2005). Patient satisfaction with treatment can also be adversely affected by factors in the physical environment. Sitza & Wood (1998a) suggest that those factors involved include accessibility to treatment, such as transport, car-parking issues and waiting times.

6
Expressed concerns of nurses working in an Australian haematology/oncology day unit were the impetus for an action research project undertaken by Wallis & Tyson (2003) to improve the nursing management of patients. These nursing concerns related to increased numbers of patients, with subsequent increased patient waiting times and this led to more patient complaints. Nurses also worried that there was an increased risk of chemotherapy administration errors and patients were not receiving the appropriate support from both the nurses and others in the multi-disciplinary team. Changes were made to both the appointment booking system and nursing workload resulting in an improved service. Problems such as those described above have been found to have a direct link to increased levels of patient anxiety (Sitza & Wood, 1998a). The impact of these factors on the work of the nurse in chemotherapy environment has not been explored in-depth in the UK but there is anecdotal evidence from nurses to suggest that these factors do impinge on the care that they give.
Patient Satisfaction, Education and Communication
The literature suggests patients’ satisfaction and acceptance of this therapy also relies upon the provision of information, advice and explanation; and the need to discuss the emotional consequences caused by the treatment (Davidson, 2005; Sitza & Wood, 1998a; Soothill, Morris, & Thomas, 2003). Patients have been found however, to be often dissatisfied with aspects of the administration process including, communication and psychological support; waiting times; assessment and management of side effects; and information giving (Mun et al., 2001; Sitza & Wood, 1998b) Dennison (1995) found that although nurses were competent in providing information, they rarely made any assessment of patients’ feelings about their treatment. In addition, research has shown that poor management of chemotherapy-induced side effects, such, as nausea and vomiting can adversely affect quality of life (Brown et al., 2001; Richardson et al., 1998) and their level of anxiety about treatment (Mun et al., 2001). Assessing and managing these side effects effectively, and also providing necessary information, can increase patients’ satisfaction and also, decrease anxiety and significantly increase patient compliance (Sitza & Wood, 1998a). Yet, (Holmes & Eburn, 1989) suggest that nurses do not accurately perceive the extent of chemotherapy-induced problems, particularly the less visible ones such as nausea. Interestingly, one area patients are rarely dissatisfied with is nursing skills involved in the technical care of chemotherapy administration (Mun et al., 2001; Sitza & Wood, 1998b). When trying to explore their findings researchers have identified a need to explore the chemotherapy process in more depth so that factors contributing to the findings may be revealed.
Communication and Patient Psychological Support
Wilkinson (1991) found that nurses who had not completed post-basic education in cancer care were poor facilitators of communication compared to those that had, who were much better at communicating with patients. Nurses use avoidance tactics in order not to have to confront the emotional fallout caused by chemotherapy and its side effects (Dennison, 1995; Lanceley, 1995; Maguire, 1985). It is not made clear why nurses feel the need to avoid this aspect of care when research has indicated that nurses are very aware that patients need psychological support (Batchelor, 2001; Jacobsen et al., 2002). Arantzamendi & Kearney (2004) explored the perceptions of a group of cancer nurses regarding the psychological needs of chemotherapy patients. While the small convenient

7
sample limits generalization, findings do indicate that there are a number of factors why nurses feel they may not be able to support patients’ psychological needs. These included lack of private space and time. Also, while most of the nurses in this study felt they did provide psychological care they admitted that they generally waited for patients to offer information, which usually they didn’t; no formal tool was in place to systematically assess psychological needs. Interestingly, in a small study exploring the nurses’ perspectives of administering chemotherapy undertaken by Verity (2002) using an investigator designed, self-completion, exploratory questionnaire, 65% (n=102) of the respondents felt that their practice would benefit from further formal education in the psychological consequences of treatment. Again the small, convenient sample accessed from a specialised hospital utilised in this study makes it difficult to generalise the findings. Wilkinson (1991) suggests that many cancer nurses do want to communicate openly with their patients but often find it too stressful to continually expose themselves to their patients’ emotional distress. Verity (2002) reported that 46% of the sample (n=102) found it distressing to see patients affected by the chemotherapy they had administered. Purandare (1997) offers a different perspective suggesting that negative attitudes held by health care professionals and the general public towards the disease can create barriers to effective communication with the newly diagnosed cancer patient. Negative attitudes towards chemotherapy may create similar barriers.
Nurses’ Attitudes towards Chemotherapy and Cancer
Psychologists argue that the attitudes we hold towards something will influence our behaviour towards it (Miller, Kearney, & Smith, 2000). There appears to be little research undertaken to investigate nurses’ attitudes and beliefs regarding chemotherapy. There has been some work investigating nurses’ attitudes towards cancer as an illness. Corner (1988) critically reviewed research methods used to investigate nurses’ attitudes towards cancer and found that
‘the research to date seems to reflect a consistent pattern of nurses’ and other health carers’ attitudes towards cancer which is largely negative and stereotyped, with cancer being seen as more devastating than other life threatening diseases’
From the findings of a further study undertaken by Corner & Wilson-Barnett (1992). Corner (1993) produced the Attitudes towards Cancer model to depict those factors, which were found to affect nurses’ attitudes, beliefs and feelings in relation to cancer. These included professional preparation for the role, culturally held beliefs and personal and professional experiences of cancer. Elkind (1982) surveyed 785 nurses to investigate what type of impression nurses may give the general public about cancer through their attitudes towards the disease, a number of nurses were found to hold very negative views of cancer. Elkind (1982) also found that while training and experience lead to a better understanding of the disease, the more experienced and knowledgeable nurses were likely to have doubts about the value of treatment for cancer. Only 21% of the nurses surveyed agreed with the statement ‘a patient with cancer can never be really cured’, whereas, 75% of the trained nurses surveyed agreed with the statement ‘treating cancer patients can do more harm than good’ (Elkind, 1982)

8
Slevin et al. (1990) British survey compared attitudes of medical oncologists, radiologists, oncology nurses, general practitioners, the general public and cancer patients, regarding the use of chemotherapy when the hypothetical probability of cure or benefit was varied. It was found that cancer patients were more likely to opt for aggressive treatment with a high degree of toxicity and minimal chance of benefit than any other group. At the same time, the radiologists and nurses were the least likely of all the groups to accept treatment. A later study undertaken in the United States by Damrosch et al. (1993) focused on comparing nurse and physician cancer specialists’ attitudes toward aggressive cancer treatments. They postulated that differences between nurses’ and physicians’ attitudes towards aggressive treatment were a source of conflict between the two and an important cause of stress for the nurse. This view was reflected in the studies findings. The evidence from the literature, therefore, suggests nurses have a generally negative attitude towards chemotherapy and this must be cause for concern. Nurses need to have a positive approach to treatment regimes to help patients effectively (Wherney-Tedder, 1997). However, all these studies identified above have not primarily investigated nurses’ feelings about administrating chemotherapy in any depth and are somewhat dated. Conversely findings from Verity’s (2002) study indicated that the participants tended to have a positive attitude towards chemotherapy. Verity (2002) concluded that this finding was due to the sample being a generally experienced and educated one, who could easily access expert support and who was working within a specialist centre for cancer. Once again it is difficult to generalise these findings.
Nurses’ Concerns and Feelings
Very few studies were identified in the literature search, which explored in-depth, nurses’ feelings towards caring for patients who experience chemotherapy-induced side effects. Findings from Fall & Rose (1999) small qualitative study indicated that nurses felt that helping and caring for these patients through their treatments was both a rewarding and stressful experience. The rewarding elements included the powerful relationships made during treatment between the nurse and the patient. As a result of this relationship nurses felt that they were successful in helping the patient through their treatment, controlling the adverse side effects. Others have also described the special, intimate, relationships forged between the oncology nurse and the patient undergoing cancer treatments (Campbell, 1984; Glaus, Campbell, Kearney, & Richardson, 2000). Guilt however, was expressed by one participant, in the Fall and Rose (1999) study, for being part of the chemotherapy treatment process. Administering the drugs and thus, having then to confront the patients’ suffering, caused intense stress at times for those who participated in the study. A criticism of this study is that a purposive form of sampling was used and the five participants were extremely experienced and thus, the impact of caring for patients through their treatments for less experienced nurses was not explored. Conversely, the findings suggested that the key to these nurses coping successfully with the stress caused by watching patients suffer from treatment that they had administered, was that subjects reported an awareness that they needed to distance themselves from the treatment situation. These nurses were also found to have devised personal strategies to cope with stress. It is questionable that less experienced nurses may be able to cope as successfully or separate themselves in a way that was not detrimental for the patient. Many authors have attributed nurses distancing themselves from patients as a symptom of professional burnout (Glaus et al., 2000)
9
Other authors have also indicated that one of the main reasons for oncology nurses experiencing stress and burnout is associated with administering cytotoxic drugs (Barraclough, 1994; Delvaux, Razavi, & Farvacques, 1988). Why this should be the case has not been clearly defined. The findings from Wilkinson (1990)study briefly suggested that cancer nurses found factors such as chemotherapy induced side effects, the uninformed patient and their own lack of knowledge regarding chemotherapy treatment as potential factors. Clearly more investigation is required to determine the causes of stress for nurses in this role. Verity (2002) found that nurses had a number of significant concerns. These included patients’ experiencing adverse reactions to treatment, extravasation and cytotoxic spillage. Extensive training, which most had received on safety issues, did not seem to lessen these anxieties. Verity (2002) argued that these concerns could be viewed as a positive consequence of administering chemotherapy. Nurses need to be constantly vigilant to these effects so that they can either be avoided or quickly identified and managed effectively. The participants in Verity’s (2002) study also expressed concerns at administering chemotherapy at night when there was little skilled support available from colleagues, when the clinical area was busy or short-staffed. Considering the potential ‘stressful’ factors of this role Fall and Rose (1999, p. 907) suggest ‘the appropriate support systems at both the managerial level and the collegial level for nurses who administer chemotherapy should be explored’. There is still however, very little documented evidence to suggest what these systems should be.
Occupational Risks of Exposure
During the 1980’s much was written in the literature about the safety aspects of giving chemotherapy and concerns regarding the potential occupational hazards to health care workers who handle cytotoxic agents (Darbyshire, 1986; Goodman, 1985; Miller, 1987; Selvey, 1985a, 1985b) There is a consensus in this literature that some cytotoxic drugs are carcinogenic and teratogenic to humans. What is not known, however, is the risk, if any, of long-term, continuous exposure to small amounts of cytotoxic drugs or indeed identified safe staff exposure limits (Gregoire, Segal, & Hale, 1987; Lee, 1993; Miller, 1987). Some studies have indicated that health-care workers are at risk from not only handling the cytotoxic drugs, (spillages, leakage, inhalation or skin contamination) but also from handling excreta and body fluids from patients who are receiving chemotherapy (Bingham, 1985; Nygren & Lundgren, 1997). Valanis & Browne (1985) found that for nursing staff one of the commonest daily forms of cytotoxic exposure was excreta from patients. Sessink, Boer, Scheefhals, Anzion, & Bos (1992) found cytotoxic drug contamination in areas where high quantities of drugs were used, including on the floors of drug preparation rooms and patient’s rooms; in cleaned urinals and bed pans, on the outer packing and vials of drugs; and on gloves used for preparing and cleaning activities. In 1988 (updated in 1996) the Control of Substances Hazardous to Health (COSHH) regulations were introduced by the Health and Safety Executive. These regulations also included guidelines on the safe handling of cytotoxic drugs so that individuals handling cytotoxic drugs are protected. Employers are now obliged to identify risk, and implement and provide safety measures and clothing to protect their staff. Most institutions should now have policies and procedures in place concerning the safe handling of these drugs, but as Grundy (1999) found most policies content and standards vary enormously, if

10
indeed there is one at all. Even if there is a comprehensive policy regarding this practice in place how much nurses adhere to these policies is also debatable (Dougherty, 1999; Goodman, 1998b). The findings from Christensen, Lemasters, & Wakeman (1990) study did find that the existence of a formal hospital policy for handling cytotoxics had a positive influence on the use of personal protective equipment. There is also considerable debate on what type of clothing is considered to offer the most effective protection, although there are minimal requirements for the design, type and protection standards in place (Allwood et al., 2002; Sims, 2005). Other studies have also shown that women who are pregnant (especially if exposed in the first trimester) are at risk of spontaneous abortions and giving birth to malformed infants (Hemminki, 1985; Kalter, 1986). Valanis, Vollmer, Labuhn, & Glass (1997) findings suggest that there is a higher risk of infertility in those occupationally exposed to cytotoxics (nurses and pharmacists) than those who are not. Therefore, women should be able to decline preparing or delivering cytotoxic drugs whilst pregnant, planning a pregnancy or breast-feeding without fear of sanctions (Holmes, 1997). Many UK Trust policies regarding administering chemotherapy while pregnant clearly state that there is ‘no evidence’ that chemotherapy drugs are harmful to those that are administering it if all safety procedures are followed (Goodman, 1998b). It can be seen that controversy still surrounds this issue of safety and nearly twenty years since some of these studies were conducted many questions regarding the safety of handling cytotoxic drugs remain unanswered.
Attitudes towards Occupational Risks of Exposure
Historically in the UK nurses have been reluctant to use personal protective clothing for reasons such as fear of frightening the patients, having lack of time and having an attitude that they were personally immune to the dangers of these hazardous substances (Valanis & Browne, 1985). Goodman’s (1985) small descriptive study found that nurses’ had few concerns about the dangers of handling cytotoxic drugs. Nurses’ attitudes towards this issue appear to be changing; one of the deciding factors to undertake this current research study was that nurses within our own South East London Cancer Network had raised concerns about the risk of occupational exposure. Verity (2002) also found that a number of nurses had concerns about this issue, and 28 (n=102) were also concerned about administering chemotherapy when pregnant.
Chemotherapy Administration Errors
Chemotherapy prescription, preparation and administration errors can be fatal. Recent media coverage both in the USA and the UK has underlined this (Schlmeister, 1999). However, the nature and outcomes of most chemotherapy errors is unknown, for two reasons. A reluctance of staff to report errors for fear of reprisals means that the factors contributing to these errors are not clearly known. Secondly, there is no national mandatory system in place, for reporting, recording or publishing errors (Goodman, 1998b). Schulmeister (1999) investigated nurses’ descriptions of the nature and severity of chemotherapy, using an investigator developed postal survey. Even with the knowledge that response rates can be poor for this type of research, in this study only one hundred and two (26%) of the sample returned the questionnaire. While taking this limitation into account however, the findings of this study do give cause for concern. Chemotherapy administration errors were reported to have occurred in the workplace by 63% of the respondents. These errors included under and overdosing patients, schedule and timing mistakes, administering the wrong drugs, infusion rate errors, inadequate pre-

11
administration checks and tests, incorrect preparation of the drugs and even chemotherapy being given to the wrong patient. Schulmeister (1999) also asked what respondents thought these errors could be contributed too. Twenty-five percent of the respondents reported under-staffing, 20% cited lack of experience, 16% stress and 15% said these errors were caused by unclear orders. O'Shea's (1999) review of the literature examining factors which contribute to nursing medication errors (not specifically chemotherapy) found interruptions and distractions during preparation and administration of drugs to be a contributory factor. Other factors cited included - poor mathematical skills of nurses, lack of nursing experience, overwork, long length of shift, badly written prescriptions and nurses’ lack of knowledge concerning the drugs. Goodman’s (1998b) review of the literature regarding cytotoxic errors (made mostly by doctors) also reports a wide range of causes and contributing factors these included prescription ambiguity, communication difficulties and insufficient staff knowledge. Goodman (1998b) goes on to recommend that, to prevent errors in practice all junior staff should have the appropriate supervision and support, what this is exactly, is not made clear. It is stated however, that
‘staff need timely access to up-to-date, accurate information which they understand
and can act on re: individual cytotoxic drugs, regimens/protocols and individual
recipients’. (Goodman, 1998b, p.174)
Preparation and Support for the Role
Nurses must have confidence in their knowledge, ability and technical expertise if they are going to provide effective, safe and beneficial patient care. Verity’s (2002) study found the majority of the participants had not been adequately prepared for the role and did not have confidence in their abilities, knowledge and skills when they first administered chemotherapy. Ninety-nine nurses (n=102) described how they felt when they first started giving chemotherapy, of these eighty-five of the respondents used words such as ‘terrified’, ‘very anxious’, ‘nervous’, ‘scared’ and ‘very unsure’ (Verity, 2002). Very few of the participants had received education about this process prior to administering chemotherapy. The Joint Council for Clinical Oncology (1994) recommended that all nurses who administer chemotherapy must attend one of the recognised courses on cancer chemotherapy, Presently, there is no national standard of chemotherapy training in the UK, and Trusts and employers are compelled to draw up local policies and education packs, the standard and content of which vary widely (Goodman, 1998b) Some courses such as the ENB 92, ENB 237 and ENB N59 did include instruction about chemotherapy as part of the content of the course. Since the English National Board, for Nursing Midwifery and Health Visiting (ENB) has disbanded, universities and colleges of higher education have begun to offer cancer nursing courses, which include caring for the chemotherapy patient. Again standards and content have been found to vary. (Kearney, 2000) suggests that it is likely that ‘variations in clinical nursing expertise and knowledge, have a detrimental effect on patient care’ This variation in educational standards was highlighted in an audit undertaken by Grundy (1999), which examined current chemotherapy administration practices of nurses in Scotland. Of the sixty-two nurses who were interviewed, thirty-two were considered senior,

12
experienced nurses (F Grade or above) and thirty were less experienced, junior nurses. Of the overall sample 39% had been prepared for this role by ‘learning on the job’ and only 18% had undertaken a recognised course. (Grundy, 1999) did not express surprise at the senior nurse’s reports that they had ‘learnt on the job’, many had been involved in the chemotherapy process before the hazards of cytotoxic drugs were really known and education was offered in this area. However, she was disconcerted at the finding that more senior nurses had undertaken a recognised course than junior nurses. Some 53% of the junior nurses stated that, they had also only learnt about chemotherapy in clinical practice. These findings were also reflected in Verity’s (2002) study where 33% (n= 102) of the sample had ‘learnt on the job’, interestingly, 76% of the sample also stated that at times they were worried about their colleagues’ knowledge and education deficits. Interestingly many of the sample stated that their confidence increased due to working with knowledgeable role models from whom they could gain support and advice (Verity, 2002). While it is recognised that clinical experience is necessary to gain knowledge about caring for cancer patients, for nurses to do so effectively it must be done in tandem with education (Kearney, 2000). Nearly half the sample in Grundy’s (1999) audit felt that receiving more education about anticancer agents would be a means of enhancing their practice. The majority of the nurses in Verity’s (2002) study required ongoing professional development and stated that they would benefit from further knowledge in the following areas – developments in chemotherapy, psychological consequences of treatment, safety issues and management of side effects. Preferred form and delivery of this required further education included informal clinical teaching, study days and workshops. Grundy (1999) and Verity (2002) both concluded that educational preparation in this area must be improved and recommend that ongoing collaborative and co-ordinated educational strategies (including regular updates) on a national level in the UK should be developed if we are to ensure that we sustain and support a competent workforce. The Nursing Contribution to Cancer Care document (DOH, 2002) recognised a need for developing cancer nursing education and in response to this need there has been work undertaken to develop core generic competencies for chemotherapy care (Skills for Health, 2005). However, it is difficult to know how nursing competency in this role might be measured without comprehensive evaluation of both the role and education in the practice of chemotherapy administration.
Conclusion
There is a dearth of research and audit evaluating nurses’ roles and competence in the chemotherapy process. The main reason perhaps for this lack of evaluation is that not all cancer centres or units in the UK follow exactly the same policies with regard to chemotherapy practice (Holmes, 1997). Although there are evidence-based, multidisciplinary, UK clinical guidelines for the administration of cytotoxic chemotherapy produced by The Royal College of Nursing (Goodman, 1998a/b) few organisations have implemented them. These RCN guidelines also recommend that more research is urgently required to understand factors, which may influence effective practice. Two areas (out of many) that the review suggests should be covered include:
• ‘Nature of staff and others beliefs and knowledge deficits’
• Impact upon practice of beliefs, knowledge and knowledge deficits’ (Goodman, 1998a)

13
The literature suggests that there are wide variations in educational preparation for this role and practice, which must be cause for concern, given the implications of chemotherapy administration. Evaluation of this role is imperative because it can inform decision-making, influence educational programme development and ultimately impact on nursing practice (Kearney, 2000). It is evident that there is an urgent need for research to be undertaken to examine and observe the work of the nurses who administer chemotherapy to understand factors, which may impinge or enhance care received by patients.

14
3 Method
Introduction
This section describes the methodology used to undertake this mixed methods study. Component one pursued a quantitative approach and consisted of a survey. Component two, qualitative in nature, involved an ethnography. The methods used to undertake each component will be described separately.
Component One - Survey
Survey aims
The aim of this component was to investigate nurses’ perspectives of administering chemotherapy to patients with cancer. Specifically, the survey sought to:
• Determine the attitudes and beliefs of nurses who administer chemotherapy
• Ascertain the nature and extent of educational preparation that nurses who administer chemotherapy have received and whether this is perceived to be sufficient
• Determine whether experience and/or education have an impact on nurses’ attitudes or concerns
• Characterise some of the challenges nurses experience during the process of chemotherapy administration
Rationale for Survey Methodology
The survey method is considered an invaluable research approach for obtaining data to describe, compare or explain nurses’ beliefs, knowledge, behaviour and attitudes (Fink, 2003; Mccoll et al., 2001). Surveys that utilise postal questionnaires as the method of data collection are an extremely useful and relatively inexpensive method for gathering accurate and consistent information that is comparable across a wide range of people (Aldridge & Levine, 2001), and are especially suited to collecting data from a large sample. The questionnaire used in this survey aimed to obtain valid, reliable data from a representative sample of nurses who administer chemotherapy. A cross sectional design was employed which aimed to provide descriptive data on nurses’ opinions at a single time point (Fink, 2003)
Survey Instrument and Design
The survey instrument used in this study comprised the Chemotherapy: Education, Worries and Attitudes Questionnaire – Hospital Version. It consists of a 25-item, self-completion postal questionnaire comprising seven sections which include: General Information about Chemotherapy Role, Educational Preparation, Feelings, Issues of Practice, Worries about Chemotherapy, Attitudes and Professional Details (appendix 1). Key areas of questioning include attitudes, beliefs and concerns regarding the nurses’ role, their support mechanisms and educational preparation. It uses various questioning

15
techniques including both closed and open questions. The open questions were included so that richer, more diverse data could be obtained. In addition, the inclusion of open questions can prevent respondents from feeling frustrated and constrained by the fixed choice answers of closed questioning (Coolican, 1993). The majority of the closed questions called for a nominal response choice. The section of the questionnaire concerned with attitudes towards chemotherapy administration required an ordinal response via a 4-point Likert scale. For examples of the various question types and corresponding response formats see table one.
Table 3.1: Example questions and response formats
Example Question Question
Type Response format
Please state the three most important issues that should be included when educating nurses about chemotherapy administration?
OPEN
FREE TEXT
1. ……………………………………………………… 2. ……………………………………………………… 3. ………………………………………………………
In your current job do you administer chemotherapy to patients?
CLOSED
NOMINAL RESPONSE CHOICE
Daily �
Weekly �
Several times a month �
Occasionally �
Never �
When presented with complications caused by chemotherapy I feel confident in my competency.
CLOSED
4-POINT LIKERT SCALE
Strongly Agree � Agree � Disagree � Strongly Disagree �
Questionnaire Development
The questionnaire was based on that developed by Verity (2002) as part of study that aimed to investigate factors that influenced care of patients receiving chemotherapy. The topic areas and specific questions for this original questionnaire were generated by a number of methods including an extensive review of pertinent literature, informal conversations and interviews with colleagues and experts in the field of chemotherapy nursing and from the researcher’s own experience (Verity, 2002). Content and face validity of the original questionnaire were established through grounding the items in the literature and through critical review by clinical experts (Verity, 2002). It was subjected to pre testing prior to use in the 2002 study to determine its acceptability, utility and ease of use.

16
Revisions Made To Original Questionnaire
The original questionnaire developed by Verity (2002) was reviewed for relevance and usability within the context of the current study. Some revisions were made including sections being more clearly titled; two questions re-sequenced to enhance flow of questioning; and some words changed to clarify their meaning and for easier handling when undertaking statistical testing (revisions are shown in appendix II). A number of questions were added, as they were considered relevant to the population under examination. Finally, three further questions concerned with attitudes were added, as it was apparent from experience of using the original questionnaire that this aspect could be enhanced (additions are listed in appendix 3).
To improve appearance and readability the questionnaire was produced in a booklet format with white pages and a lilac coloured front cover. All questions were printed in black ink (Mccoll et al., 2001).
Population and Sample
The target population was all nurses who administered chemotherapy across the five London Cancer Networks. This included nurses working across twenty-six NHS Trust Hospitals where patients received chemotherapy. Although it was initially thought that some form of probability sampling could be utilised for this study it became apparent that due to the relatively small numbers of nurses administering chemotherapy in London that this approach would compromise the sample size. Therefore, the total population of nurses administering chemotherapy became the sample; accessed via a multi-stage approach.
The sample included individuals who:
• Were Registered Nurses on Part 12 (General Nursing) of the Nursing and Midwifery Council (NMC) Register.
• Worked at an NHS Trust that is part of one of the 5 London cancer networks
• Administered chemotherapy to adult patients with cancer as part of their role within a cancer unit or cancer centre.
Nurses were excluded if they:
• Were not currently involved in administering chemotherapy
• Were employed by an Agency and therefore, not permanently contracted to the Trust.
• Worked in private hospitals
• Administered chemotherapy to children
• Were not registered on Part 12 of the NMC Register
Study Sites and Setting
Although there are thirty-two NHS hospitals in the five participating London Cancer Networks, only twenty-eight of these were identified as places that administered chemotherapy to adult cancer patients. Of these twenty-eight, a further two hospitals were not included. One had already been involved in a previous study undertaken by Verity (2002) utilising the questionnaire. The other was not included as this particular Trust did

17
not have a Research and Development Committee functioning at the time that approval and access were being sought. Thus 26 hospitals were invited to take part.
Sample Size
A statistician was consulted in order to inform the required sample size. However, there is no simple rule for sample size that can be used for surveys. Nevertheless, it should be sufficient to make the results representative of the population although no more than necessary to achieve this and always considering the size of the population (American Statistical Association 2004). It was deemed that for descriptive and comparative statistical analysis 200 completed questionnaires would be needed for the study to achieve its aims (at the 5% level of significance (α) with 80% power (1-β), (Cohen, 1992) this took into account that we intended to test multiple hypotheses. With an anticipated response rate of 40%, a total sample size of 500 was required.
Ascertaining and Accessing Sample
To access the sample it was necessary to progress through a number of stages, mainly because of the limitations imposed by the Data Protection Act (OPSI, 1998). Initially, the Lead Cancer Nurse (LCN) at each hospital site was identified via the relevant Network Nurse Director. Each LCN was provided with written information (appendix 4) regarding the study including the aims, procedure and expectations of the questionnaire survey. Following approval from the relevant Research and Development Committees (see section on Ethical and Research Governance Approval) LCNs were provided with letters and asked to distribute these to all nurses who met the inclusion criteria within their Trust. These letters asked whether the nurses would agree to have their names forwarded to the research team. This invitation letter enabled each nurse to decline his or her name being forwarded by returning a “tear off” slip to the LCN. Only the LCN would have the names of those who declined. Following receipt of these slips the LCN compiled a list of the nurses who fulfilled the eligibility criteria and were willing to consider participation in the survey. This list of potential participant names was then sent to the research team. As a result 526 trained nurses who were administering chemotherapy across the five London Cancer Networks were identified for inclusion in this survey. Participation ranged from 2 to 112 nurses per hospital site (see table 3.2). A total population sampling method was adopted in that every potential participant on the list provided by each LCN was sent a questionnaire pack. The survey sample consisted therefore of all the nurses who were sent a questionnaire pack.

18
Table 3.2: Number of hospital sites and nurses who administer chemotherapy within each London Cancer Network
London Cancer Networks
Number Of Hospital Sites
Number Of Nurses Within Each Cancer Network Who Administer Chemotherapy
Final Sample: Number Of Nurses Who Agreed To Participate In Study
North 5 102 97
North East 5 111 111
South East 6 122 121
South West 4 53 53
West 6 157 144
Total 26 545 526
Procedures for Survey Administration
A unique study identification number was assigned to nurses who consented to their name being forwarded to the research team. Questionnaire packs consisting of a cover letter (appendix 5), a nurse information sheet (appendix 6) and a questionnaire (appendix 1) were sent to each individual nurse, to their work address. A stamped addressed envelope was sent with the questionnaire to encourage response. In order to maintain confidentiality only the study identification number was included on the questionnaire and participants were asked not to write their names anywhere on the questionnaire. Following best practice in relation to survey response rates a reminder letter was sent to non-respondents 2-3 weeks after the initial questionnaire pack had been sent out. After 4-6 weeks, a further reminder letter and copy of the questionnaire with a stamped addressed envelope again was sent to those nurses who had not responded (Mccoll et al., 2001). Figure 1 gives a summary of the process used to ascertain the sample

19
Figure 1: A Flowchart Illustrating Multi-Stage Approach Utilised for Ascertaining and Accessing Sample
Reliability and Validity
Pre-testing of the questionnaire was undertaken to build on the testing carried out during the tools original development (see section on questionnaire development). A common concern when using survey/questionnaire data collection tools generally is whether the tool is a true reflection of the body of knowledge pertaining to the concept of the study, and whether it is able to elicit information needed to meet the aims of the research. Commonly the following aspects of validity are tested for: face, content, construct and criterion validity (Fink, 2003). In the case of this tool content validity was
Study information provided to
the Lead Cancer Nurse (LCN)
at each site
Nurse invitation letters
provided to each LCN
Trust R and D approval
obtained
RESEARCH
TEAM
Nurse invitation letters distributed
to all nurses who administered
chemotherapy
Lists of all nurses who wanted to
participate and were eligible to do
so were compiled by LCN and sent
to research team
LEAD
CANCER
NURSE
Questionnaire packs sent to all
names on the list provided by
the LCN.
RESEARCH
TEAM
Tear off slips returned to LCN
identifying those who did not
wish to participate

20
established through review of the literature, during its initial development and evaluation of the questionnaire by those considered expert in the field.
Pre-test
A pre-test was undertaken to determine the acceptability, appropriateness and feasibility of the revised questionnaire. Twenty pre-test questionnaires were distributed to nurses who administered chemotherapy at a private London hospital. This hospital was not participating in the main study. Eight questionnaires were completed and feedback obtained. No changes were made to the wording of the questionnaire; however the questionnaire appearance was altered from lilac coloured pages throughout to white pages with a lilac front cover. This was due to the pre-test respondents reporting that the questions on the lilac paper were hard to read. The average time taken to complete the questionnaire was thirty minutes.
Data Preparation
Data Entry
An SPSS database was created. A codebook was devised based on the questionnaire to aid scoring and data entry procedures. The findings from the open-ended questions were entered verbatim in a Microsoft Excel spreadsheet.
Data Cleaning
To ensure the accuracy of the database, the data were systematically cleaned following the guidelines of (Davidson, 1996). Initially a series of computerised descriptive analyses were performed on all items of the questionnaire to check for any impossible (a data value on a variable that cannot exist) or implausible values (a data value which is possible but highly unlikely). These data were then checked manually for any obvious typographical errors ensuring, for example, that the total number of responses for each item did not exceed the total number of survey respondents and the minimum and maximum values were within the variable coding range. A visual check of the database was also carried out to identify blocks of missing data and expected patterns in data. Then a complete manual check was carried out on 10% of the data (25 questionnaires). Every 10th questionnaire was manually checked in full against the database and the error rate was calculated to be 0.2%. All errors were rectified and the correct data values entered into the database.
Data analysis
Descriptive statistics such as frequency distributions were used to describe/summarise the characteristics of the sample and the variation in response. Each section of the questionnaire was analysed descriptively in turn. Cross-tabulations utilising Somers ‘d test were undertaken to examine how the responses on two of the variables were related. These were undertaken to explore the relationship between nurses’ attitudes towards chemotherapy and their present grade; attitudes and years of experience; attitudes and amount and adequacy of teaching received; and attitudes and frequency of administration.

21
Cross- tabulations utilising Somers ‘d test were also undertaken to explore the relationship between nurses’ worries about chemotherapy and all of the variables stated above. Independent sample t-Tests were also undertaken to explore if there were any notable differences between group means. The overall group size was considered sufficient for a significant level to be set at alpha 0.05. Nurses’ attitudes towards chemotherapy were further analysed by calculating the overall score achieved on the attitude scale for each respondent. This would reflect whether the nurses in this sample have a favourable or unfavourable attitude towards chemotherapy administration. The attitude scale included 21 items statements; as a 4-point Likert scale was used, the highest possible score indicating a positive attitude would be 84. The attitude scale included both positive and negative item statements. Positive attitude statements were scored 4 =strongly agree, 3= agree, 2=disagree, 1= strongly disagree, conversely negative attitude statements were scored 1 =strongly agree, 2= agree, 3=disagree, 4= strongly disagree. The direction of scoring on the Likert scale was not included on the questionnaire administered to the respondents. An ordinal regression model was employed to determine which factors impact upon the process of nurses administering chemotherapy, specifically, which factors influence attitudes towards and worries about chemotherapy administration.
The qualitative results obtained from the open-ended questions were typed verbatim into the computer. These findings were then coded into themes and categories, so that the data could be more easily described. To ensure that the analysed data was a fair representation of what was recorded two people participated in the analysis process of the open-ended questions, ensuring inter-rater reliability.
Ethical and Research Governance Approval
The research proposal was submitted to, and approved by, a Multi Research Ethics Committee [Ref no: 04/Q0603/51]. In addition, approval was obtained from each participating Hospital Trust’s Research and Development Committee. To comply with the Data Protection Act (1998) the information letter that was distributed to all nurses who fulfilled the eligibility criteria, included a “tear-off” slip for nurses to indicate if they did not wish their name forwarded to the research team. Questionnaires were only sent to nurses who appeared on the ‘potential participants’ list prepared by the Lead Cancer Nurse. To maintain confidentiality, questionnaires were allocated a study ID number, thus ensuring all responses were anonymous. The list linking the study ID numbers to the names of the participants was kept in a separate, locked filing cabinet and password protected on the researcher’s computer. This list was only accessed when reminders were due. As the sample was accessed through Lead Cancer Nurses, there were concerns that nurses may feel pressurised or coerced into taking part in the study as their manager was potentially approaching them. The Lead Cancer Nurses were given clear instructions about the nature of the study and it was stressed that participation was voluntary; this was also explicit in the invitation letter to the nurses.
22
One further ethical concern was that potential participants might misinterpret the aims of the survey and think their level of knowledge was being assessed. It did not aim to measure nurses’ knowledge deficits regarding chemotherapy practice. To ensure that there were no misunderstandings the aims were clearly explained and it was highlighted both in the information sheet and the questionnaire that it was the nurses’ perceived knowledge deficits that were of interest.
Component two – ethnography
Aims of the ethnography
The aim of the ethnography was to develop an understanding, in context, of the work of nurses administering chemotherapy in an outpatient clinic. The ethnography sought to:
• Observe and describe nurses’ practice of chemotherapy administration
• To explore knowledge, feelings and beliefs of nurses administering chemotherapy
• To highlight any discrepancies between what people do and what they say they do
• To understand the factors which contribute to these discrepancies.
Rationale for ethnographic method
To fulfil the aims of components two, an ethnographic approach was considered an invaluable source of obtaining data to understand the nurses’ perspective of chemotherapy administration and how it translated into practice. Within this approach, participant observation of nurses’ work and interactions with patients and other personnel allowed the researcher to see both what people do and what they say they do. An ethnographic approach offered a way in which the context could be included within the research enterprise and take into account the effects the context had on the actions of the participants (Savage, 2000). The relationships developed in ethnography offer an opportunity for researchers to gain an insider (emic) view which allows those aspects of nurses’ knowledge that are grounded in everyday life to be explored (Savage, 1995). The study examined two different locations in London in different Cancer Networks. Although the data formed separate descriptions, the findings from each location gave a wider picture of the work. This design is acceptable practice when examining nurses’ work (Allan, 1999; Jarret, 1996; Savage, 1995) and addressed the recommendation that research examining nursing in cancer care should use observational methods (Kruijver, Kerkstra, Bensing, & Van de Weil, 2000)
The settings
The setting for the ethnography consisted of two chemotherapy day units. In setting 1, the Chemotherapy Day Unit (CDU1) is situated in the basement with easy access for cars and transport. It is located within a larger department that houses the Radiotherapy Unit and the Oncology Outpatient Clinics. On other floors within this block are the pathology laboratories, cancer support services and other outpatient clinics (such as surgery). The staff compliment is one sister and four senior staff nurses. The unit opens at 09.00 hours on Monday to Thursday and 10.00 on Friday (for staff meeting 9-10.00). The clinic closes at 17.00 hours or when the last patient has finished treatment. On average 32-34 patients are seen in a day. Patients are scheduled with an appointment.

23
They come to the clinic two days previously to have bloods taken, see the doctor if necessary and have their treatment prescribed. On the day they come to the clinic, their results would have been put on to the computer and their chemotherapy dispensed. For the most part, there was minimal waiting time. Setting 2 (CDU2) is situated in the main hospital building on the second floor and geographically is some distance away from the outpatients’ clinic. The staff compliment included one sister, five senior staff nurses and one receptionist. The unit is open from 08.30 and closes at 16.30, or when the last patient has finished treatment. The number of patients seen in any day varies from 15 to 32. Patients come on an ad hoc basis, have their blood taken for assay and then see the doctor who prescribes their treatment. They then wait for blood results and for their chemotherapy to be dispensed before treatment is commenced. Waiting times are lengthy and range from 3-7 hours.
Participants
The primary participants of this study were nurses administering chemotherapy in the two settings. All nurses employed by the Trusts as chemotherapy nurses working in the relevant Chemotherapy Day Units (CDU) were invited to take part. Initially, the lead nurses and ward managers of potential settings were approached about the project. A presentation was made to determine possible interest in taking part. From this, two areas were chosen in different cancer networks in order to give a wider picture of the work of chemotherapy nurses. Presentations of the study were then made to the relevant staff on the CDU’s, staff received invitations and information letters, and there was opportunity for potential participants to meet individually with the researcher to discuss the research further and ask any questions. Nurses were then given consent forms and asked to return them to the researcher if they wished to take part. In both CDUs all nurses chose to participate. As a consequence, the patients these nurses were caring for were invited as secondary participants. All patients who were approached consented to take part. It was reiterated at each observation that participants could chose to withdraw at any time or ask the researcher to not be present for certain procedures. This opportunity was not taken up.
Data Collection
Participant Observation
As participant observation is time-consuming and labour intensive, it was decided to use two researchers for data collection, each researcher observing one of the units. This method of data collection is termed team ethnography and is associated with increased rigor and reflexivity as there is a systematic sharing of observations, and ongoing questioning of data and interpretation (Erickson & Stull, 1998). Participant observation was carried out in the two units for a four-hour period, for a number of times a week for a period of 16 weeks. In this study the role of the researchers was that of a novice helper, similar to a healthcare assistant, helping the nurse with simple tasks so that the researcher could observe practice and clarify understanding of primary data collected (Wiseman, 2002). Observation began with a pilot period to increase validity, consistency and research rigor (Wolcott, 1999). Observation included, for example, the process of chemotherapy administration, nurse-patient interactions, information giving and noted what the nurse did, verbal and non-verbal communication. During observations nurses would explain to the researchers what they were doing and why and the researchers had the opportunity to ask

24
any questions or clarify any points they did not understand. Informal interviews were often carried out with patients, nurses and other healthcare workers (for example the unit receptionist). During periods of observation the researcher would take time out to record notes as aide memoirs either in a pocket notebook or on a dictaphone. Field notes would be recorded in more detail immediately following the period of observation.
Interviews
Interviews were semi-structured and aimed at understanding the nurses’ experience of the chemotherapy administration process and clarifying any discrepancies in attitudes and observation. Themes emerging from the observation and questionnaire data formed the basis of the interview structure. Interviews were tape recorded and transcribed verbatim. Following common practice (Allan, 1999; Heyl, 2001) the transcript of the interview was shown to the participant for further comment and clarification.
Analysis
Preliminary data analysis began at the point of participant observation. Once data collection was completed, data from each unit were analysed separately using a modified thematic analysis (Wiseman, 2002). As themes emerged, data were then subject to further questioning and analysis as is common with ethnographic research (Coffey & Atkinson, 1996). Findings from both settings were discussed separately, and then considered together to give a wider perspective of the work of nurses administering chemotherapy in a day care unit. This process is common in team ethnography (Erickson & Stull, 1998).
Issues of Rigour
In qualitative research rigor is associated with openness, adherence to a philosophical perspective, thoroughness in collecting data and reflexivity (Burns & Grove, 2005). Reflexivity is a constant examining of the part the researcher plays in the construction of the data (Davies, 1999).Throughout any study, the researchers constantly re-examined their approach to the work, the participants and the theoretical perspective from which they were working (Brunt, 2001). Using an ethnographic framework enabled the researchers to emphasise the importance of understanding the work of chemotherapy nurses from their perspective. Participant observation allowed the researchers the opportunity to check meanings and test assumptions with the participants (Heyl, 2001). In addition within the present study, as team ethnography was used, the data were discussed and assumptions questioned within regular meetings of the research team (Erickson & Stull, 1998). Findings were discussed with the participants for verification and they will have a copy of the final report.
Ethical considerations and approvals
The research proposal for the ethnographic element was submitted to the relevant Local Research Ethics Committees (Ref no: 04/Q0705/28; 04/Q0603/51) and approved.
There may have been a possibility of coercion of nurses by the Lead Nurse not to opt out and nurses may have felt obliged to take part. However, from discussions with the potential participants away from their managers, they seemed keen to take part. In

25
addition, assurances related to non-participation, withdrawal, anonymity and confidentiality were offered to participants. Though their consent was gained in advance, it was reconfirmed on an ongoing basis on each occasion that data were collected (Moore & Savage, 2002).
To maintain confidentiality consent forms and assigned pseudonyms were stored separately in a locked cabinet at the university and password protected on the researcher’s computer. The raw data contained no real names of the participants.
Tapes of interviews were kept in the researcher's office in a locked cupboard and were identified by ID code only. Data were stored on the researcher's password protected computer, anonymised from the outset, in accordance with regulations found in the Data Protection Act (1998). In compliance with the Research Governance Framework (Department of Health 2001), interview transcripts and field notes will be kept in a locked cupboard for seven years following the research. Interview tapes were made blank as soon as analysis was completed.
In addition, before the final report is released it will be given to the participants and they will be asked if they are satisfied and comfortable with the level of anonymity.
Time Frame for Both Elements
Table 3.3 describes the time frame for both elements of the study.
Table 3.3: Time Frame for Both Elements
Study Timeframe
Study Activities Element 1 (questionnaire
survey) Element 2 (ethnography)
Ethical Approval process
July 2004-Sept 2004 Sept 2004-Nov 2004
Research and Development Approval process
Oct 2004-May 2005 Sept 2004- Dec 2004
Pre-test Oct 2004 N/A
Data collection Jan 2005- July 2005 Jan 2005-July 2005
Data analysis Aug 2005-Nov 2005 August 2005-Nov 2005
Final report Dec 2005 Dec 2005

26
4 Results from component 1
Introduction
This next section will present all the findings from the Chemotherapy: Education, Worries and Attitudes Questionnaire – Hospital Version. Outcomes of analyses conducted to determine factors that influenced nurses’ attitudes and concerns will also be included.
Response rate
In total, 526 questionnaires were sent out and 257 returned (response rate was 49%). Of these 253 were valid and complete questionnaires. Response to the survey was fairly evenly distributed across the five Cancer Networks but varied by hospital site as depicted in tables 4.1 and 4.2.
Table 4.1 Response rate across Cancer Networks
London Cancer Network Response rate
North 49.5%
South East 53.7%
South West 50.9%
North East 42.3%
West 48.6%
Table 4.2 Response rate across hospital sites
Site no
No of questionnaire
s sent
No of questionnaire
s returned
Response rate %
Site no
No of questionnaires
sent
No of questionnaires
returned
Response rate %
1 11 9 81 14 3 2 66.7
2 52 21 40.4 15 24 6 25.0
3 28 14 50.0 16 5 3 60.0
4 3 2 66.7 17 12 9 75.0
5 3 2 66.7 18 87 30 34.5
6 11 5 45.5 19 5 4 80.0
7 35 20 57.1 20 2 1 50.0
8 34 15 44.1 21 2 1 50.0
9 8 5 62.5 22 2 2 100.0
10 9 8 88.9 23 10 4 40.0
11 24 12 50.0 24 7 4 57.1
12 18 14 77.8 25 112 53 47.3
13 8 5 62.5 26 11 6 54.5
Sample demographics
The nurses within this sample had on average been qualified fro almost 13 years. Table
4.3 illustrates respondents’ range and average years of experience both working within
oncology and administering chemotherapy.

27
Table 4.3 Sample Characteristics
Range in years/months Mean
Time as a qualified nurse
2 years – 42 years,
6 months
12 years 11 months
Time spent working within oncology 6 months – 26 years 7 years, 8 months
Time spent administering chemotherapy 3 months – 25 years,
3 months
6 years, 5 month
Figure 4.1 indicates that chemotherapy administration is frequently undertaken as part of these nurses’ current role, with 171 respondents (67.6%) reporting that they administer chemotherapy on a daily or weekly basis. 118 respondents (47%) reported that they work in outpatients departments and 182 respondents (72%) work on a ward. There is some overlap and thirty-five of these respondents (19.2 %) reported that they work both on a ward and in an outpatients department.
Figure 4.1 Frequency of Chemotherapy Administration
0%
10%
20%
30%
40%
50%
60%
Daily Several times a
month
Weekly Occasionally
% of respondents
Table 4.4 illustrates the distribution of the sample across clinical areas. It can be seen that 131 of the sample (51.8%) reported that they worked in haematology inpatient or out patient departments. Seventy-nine respondents (31.2%) worked in oncology departments.

28
Table 4.4 Distribution of clinical areas within the sample
Clinical Speciality Frequency (n=253)
%
Haematology Outpatients 55 21.7 Haematology Inpatients 76 30.0 Oncology Outpatients 43 17.0 Oncology Inpatients 36 14.2 HIV and other 35 13.8 No response 8 3.2
Table 4.5 shows the distribution of nursing grades within the sample. The majority of the sample were F grades, while only six of the sample were D grade nurses and nine participants did not report their present grade. Table 4.5 Nursing grade Grade Frequency
(n=244) %
D 6 2.5 E 69 28.3 F 82 33.6 G 56 23.0
H 31 12.7 The sample’s professional qualifications (either obtained or currently being undertaken) are shown in Table 4.6. It can be seen that 150 nurses in the sample (59.2%) were qualified to degree level or above. Only 43 nurses (17%) were qualified to degree level of above in cancer nursing/palliative care. Table 4.6 Professional qualifications obtained or currently being undertaken Qualifications Frequency
%
Diploma Nursing 113 44.7 BA or BSc Nursing 98 38.7 MSc/MA Nursing 9 3.6 Diploma Cancer Nursing 28 11.1 BA or BSc Cancer Nursing 35 13.8
MSc/MA Cancer Nursing 7 2.8 MSc/MA Palliative Care Nursing 1 0.4
ENB N59 (Chemotherapy) 43 17 ENB 237 (Oncology) 83 32.8 ENB 285 (Palliative Care) 10 4.0 ENB A27 (Haematology) 39 15.4

29
Respondents Educational Preparation
Pre-registration
Approximately two thirds of the respondents (65.1%) reported that they did not receive any teaching regarding chemotherapy during their pre-registration training. Twenty-two individuals (8%) did not respond to this question or were uncertain about whether they had received education pre-registration. Only 67 respondents (27%) reported that they had received teaching on chemotherapy during pre-registration training and these nurses stated that this teaching was typically 1-5 hours in duration (see table 4.7).
Table 4.7 Amount of chemotherapy education of those in receipt of some pre-
registration training.
(n=68) %
Less than one hour 9 13.2 1-5 hours 31 45.6 >5-10 hours 9 13.2
Over 10 hours 10 14.7 Uncertain 9 13.2
Respondents were also asked to rate the adequacy of chemotherapy teaching that they had received in pre-registration training from ‘Comprehensive’ to ‘Inadequate’. Table 4.8 illustrates how adequate nurses felt their pre-registration education in chemotherapy had been. It can be seen that 134 respondents (53%) found the amount of pre-registration chemotherapy teaching inadequate. Only 42 respondents (16.6%) reported that the amount of chemotherapy teaching was adequate.
Table 4.8 Adequacy of the amount of chemotherapy teaching pre-registration
Frequency % Comprehensive 12 4.7
Adequate 42 16.6 Uncertain 36 14.2 Inadequate 134 53.0 No response 29 11.5 Total 253 100.0
Post-registration
When asked about their post-registration training, 243 respondents (96.4%) stated that they had received some teaching on chemotherapy since qualifying and that this typically amounted to over 10 hours (71.1%). The amount of time given to chemotherapy teaching since qualification can be seen in Table 4.9

30
Table 4.9 Amount of chemotherapy education of those in receipt of some post-registration training
Frequency %
Less than one hour 4 1.7 1-5 hours 26 10.7 >5-10 hours 22 9.1 Over 10 hours 172 71.1 Uncertain 18 7.4
Again respondents were asked to rate how adequate this amount of post-registration chemotherapy teaching had proved. Table 4.10 shows the reported adequacy of the amount of chemotherapy teaching post-registration. It can be seen that 119 respondents (47%) had found the amount of chemotherapy teaching received to be adequate and 20 respondents (7.9%) reported that it had been inadequate. Table 4.10 Adequacy of the amount of chemotherapy teaching post-registration
Frequency %
Comprehensive 105 41.5 Adequate 119 47.0 Uncertain 8 3.2 Inadequate 20 7.9 No response 1 .4 Total 253 100.0
Figure 4.2 illustrates the manner in which the post-registration chemotherapy teaching had been provided. Respondents were asked to tick one or more of the formats illustrated in the figure 4.2. One hundred and sixty-five respondents (67%) reported that chemotherapy teaching was delivered by informal clinical teaching. One hundred and fifty-eight respondents (63.7%) attended a study day and 149 respondents (60.3%) indicated that they had had a lecture during a course. Figure 4.2 Chemotherapy Teaching Format
0%
10%
20%
30%
40%
50%
60%
70%
Study Day Lecture in course Conference Other Uncertain
% of respondents

31
Formal Chemotherapy Education
Table 4.11 illustrates the topics that respondents had covered during formal education and reports areas where they perceived further education would benefit their practice. It can be seen that a large proportion of the sample (> 80%) had received education on 10 of the 12 topics incorporated in the survey questionnaire. Only the topics ‘Developments in chemotherapy treatment’ (reportedly received by 180 respondents, 73.2%) and ‘Chemotherapy reconstitution on the ward’ (reportedly received by 57 respondents, 23.8%) were received by less than 80% of the sample. Equally large numbers reported that they would find more education in these chemotherapy topics beneficial. Specifically, the sample reported that they would benefit from more education in ‘Developments in chemotherapy treatment’ (93.9%), ‘Managing long-term consequences of chemotherapy treatments’ (79.4%) and ‘Managing emotional/ psychological consequences of chemotherapy treatment’ (72.6%). Interestingly, although 236 respondents (94.8%) reported that they had received education in ‘Managing chemotherapy related side effects’, 155 respondents (67.1%) perceived that more education in this topic would be beneficial. Table 4.11 Formal chemotherapy education received and further education required.
Education Received Further Education Required Perceived as Beneficial for Practice
Topics
n % n %
Safety issues concerning chemotherapy
235 94.8 142 61.2
Managing chemotherapy related side effects
236 94.8 155 67.1
Extravasation 229 92 148 64.3
Practical administration of chemotherapy
226 91.1 109 47.6
Managing anaphylactic/allergic reactions to chemotherapy
215 87.0 161 70.6
How to inform patients about their chemotherapy treatment
211 84.7 137 59.6
Handling excreta from chemotherapy patients
208 84.2 113 50
Long-term consequences of chemotherapy treatments
206 83.1 189 79.4
Managing emotional/psychological consequences of chemotherapy treatment
203 82.2 170 72.6
Appropriate use of pumps/equipment 201 80.7 114 50.2
Developments in chemotherapy treatment
180 73.2 229 93.9
Chemotherapy reconstitution on the ward
57 23.8 114 50.4
Figure 4.3 represents the format that respondents stated they would like further education to take. Respondents were asked to tick one or more of the formats illustrated in the figure 4.3. As can be seen 139 respondents (60%) stated they would prefer their future education to be delivered during a study day. One hundred and nineteen respondents (51.5%) chose workshops as their preferred teaching format and 93 respondents (40.3%) indicated they would prefer informal clinical teaching.

32
Figure 4.3 Formats for Further Education
0
5
10
15
20
25
30
35
40
45
Informal clinical
teaching
Lecture in course Conference E-base learning Distance learning
% of respondents
Respondents were given the opportunity to state any other areas related to chemotherapy and its administration where additional education would benefit them. Sixty-five nurses answered this question. Of these 65 respondents, 38 (59%) reported that they would find regular updates beneficial. For example one respondent said,
“Regular reviewing of chemo education would keep my knowledge fresh – enabling me to be
a safer practitioner”
Another respondent commented,
“Updating staff with the current issues regarding chemotherapy administration, proper
protective clothing and research drugs for cancer treatments”
Sixteen respondents (24.6%) stated that they would benefit from more knowledge about pharmacological aspects of chemotherapy. For example,
“How each drug works in killing the cancer cells”
Six respondents (9.2%) said that they would like to learn more about fertility issues and chemotherapy. As one respondent put it,
“Fertility and chemotherapy is an issue I would like to study further as I feel it is never
addressed during courses”
Respondents were further asked to state the three most important issues that should be included when educating nurses about chemotherapy administration. As illustrated in table 4.12 one-hundred and fifty-two respondents rated health and safety issues of highest importance

33
Table 4.12 Most important issues of chemotherapy education as rated sample Important issues Number of
respondents Percentage of respondents
%
Health and safety – re: patients, environment and nurse 152 59.1
Side effects 105 40.8
Practical administration 73 28.4
Extravasation 59 22.9
Information and consent 54 21
How chemotherapy works 48 18.7
Psychological needs 23 8.9
Managing chemotherapy induced emergencies 23 8.9
Venous access and cannulation 9 3.5
Disposing of patient excreta 4 1.6
Fertility and sexuality 1 0.4
Feelings towards chemotherapy administration
Of the sample 247 respondents (98%) described how they felt when they first started administering chemotherapy. Typically, respondents described negative feelings towards chemotherapy administration such as feeling ‘nervous’, ‘anxious’, ‘scared’, ‘apprehensive’ and ‘uncertain’. Only 5% of respondents described feeling ‘comfortable, well supported or excited’ about their new role. Examples of the typical feelings described by the respondents can be seen in Table 4.13. Table 4.13 Feelings about Administering Chemotherapy
Feelings described when first started to handle/administer chemotherapy
Negative feelings (n=234) Positive feelings (n=13)
“Very anxious and unsure I kept watching out for any untoward events such as extravasation as I kept thinking that if it occurred I was not confident I would manage” “It was quite frightening you were always worried about what could go wrong and worried whether you would be able to answer all the patients’ questions” “Quite terrified – bit like working in Chernobyl”
“Having had over 3 months of supervised practice I felt safe and confident and quite privileged to be able to administer chemo” “Excited at prospect of giving drugs designed to kill tumours and about patients being cured”
However, 218 respondents (86.2%) reported that their feelings towards chemotherapy handling/administration had changed over time. At the time data were collected, the sample typically reported that they were feeling more confident (208 respondents, 87.3%). Eleven of the sample (4.6%) used terms such as capable, comfortable or competent, only 8 of the sample (3.4%) still reported feeling worried or nervous.

34
Of the 218 nurses who reported that their feelings about administering chemotherapy had changed from when they first started, 211 described the factors that contributed to this change. Typical reasons reported were ‘experience/increased practice’ (55.5%) for example:
“Giving lots of chemo and gaining experience”
Eighty-seven respondents gave ‘chemotherapy education/increased knowledge’ as the catalyst:
“Knowledge is power. Chemo study day and workbook have helped me gain
theoretical knowledge, applying it in practice has made me confident and
competent”.
“Continual learning and updating my knowledge of chemotherapy”
Seven respondents cited support as their reason, as exemplified below:
“Guidance and support of superiors and specialist nurses”
Issues of Practice
Prior to administering chemotherapy 94% of respondents always or often checked with patients the information they had received, however only 59% of the respondents always or often discussed with the medical team information that had been given to patients. Respondents were also asked whether they thought there were times when it was not safe to administer/handle chemotherapy. One hundred and ninety-three respondents (76.3%) occasionally felt that it was not safe to administer it. Reasons given for this are detailed in Table 4.14. Table 4.14 Reasons given as to when it is not safe to administer chemotherapy Times when it is not safe to administer chemotherapy
Number of respondents
Percentage of respondents
% Patient status unstable 88 34.3 Pregnant (nurse 64 24.9
Inadequate staffing levels/ ward busy 40 15.6 Uninformed patient/no consent 40 15.6 Outside normal hours (not 9-5) 40 15.6 Poor I.V access 30 11.7 Blood Counts – outside normal ranges
29 11.3
Not knowing drug/regime/protocol 19 7.4 Staff not trained 17 6.6

35
Support for Nurses
Respondents were asked who they got support from when they had queries or concerns regarding administering chemotherapy to patients. Respondents could provide one or more replies. Figure 4.4 shows from who typically they could turn to. One hundred and thirty respondents (53.1 %) reported that they received support from the medical team, 129 respondents (53%) from pharmacy and 87 respondents (36%) from nursing colleagues.
Figure 4.4 Support of nurses with regards to their queries and concerns about
chemotherapy administration
28.2
36
22.4
53 53.1
5.4
0
10
20
30
40
50
60
% o
f re
sp
on
de
nts
Ward
manager/sister
Colleagues Nurse Specialist Pharmacy M edical Team
(consultants, Drs)
Other
One hundred and eighty respondents (71.1%) reported there had been occasions when they had not wanted to administer chemotherapy. Table 4.15 illustrates how often respondents felt supported in their decision to not give it.
Table 4.15: Frequency of those who felt supported in decision to not give chemotherapy
Frequency % Never 14 5.5 Occasionally 49 19.4 Often 37 14.6 Always 75 29.6
No response 78 30.8 Seventy-five respondents (29.6%) reported that they were always supported in their decision to not give chemotherapy. However 49 respondents (19.4%) reported that they were only occasionally supported their decision. Data relating to degree of support offered were cross-tabulated with nursing grade to see whether nursing grade influenced response to their decision not to give chemotherapy. No statistically significant relationship was evident.

36
Respondents were also asked who supported them in decisions not to give chemotherapy. Respondents could provide one or more response. Figure 4.5 shows that support to not give chemotherapy was typically received from senior nurses. Figure 4.5 Nursing support for decisions not to give chemotherapy
0
5
10
15
20
25
30
35
% o
f R
espondents
Senior nurses Medics/Doctors Nursing
colleagues
Pharmacists Relatives Patient Occupational
Health
Worries about administering Chemotherapy
Respondents where asked how often they worried with regards to various aspects of their chemotherapy role. Sixteen aspects of their role were presented in the questionnaire and respondents were requested to tick whether they worried ‘Never’, ‘Occasionally’, ‘Often’ or ‘Always’ about them. Figure 4.6 depicts how often nurses in the sample worried about administering chemotherapy. One hundred and seventy-six respondents (71%) felt occasionally worried about understanding chemotherapy prescriptions/protocols. Whereas 116 nurses (46.3%) were always or often worried about the education/knowledge deficits of other nursing staff and 109 (44.3%) were always or often worried about extravasation. In addition, other factors that the nurses worried about also reported in the questionnaires. For example one respondent commented that,
“Not having enough time to spend educating patients/relatives - the day unit can seem rather
like a conveyor belt at times. Also not being able to spend listening to patients/relatives on
follow-up visits re: any problems they may have” Another respondent said,
“I worry about some attitude of nursing staff who pretend to have lots of experience in
giving chemo when in fact they just learn to give chemo recently and with no proper training
in giving/handling cytotoxic drugs” One nurse noted that,

37
“Mistakes being made due to ever increasing daily work load and the amount of time that
each patient can have with a nurse during their treatment” Figure 4.6 depicts the frequency of these worries reported by the sample Figure 4.6 Frequency of Worry
0%
10%
20%
30%
40%
50%
60%
70%
80%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Never
Occasionally
Always/Often
Key: Worry Statements
1 Understanding of chemotherapy prescriptions/protocols
2 Handling cytotoxic drugs
3 Reconstituting chemotherapy on the ward
4 The risk of exposure to self
5 Extravasation
6 Treatment side effects
7 Patient allergic reactions
8 Patient anaphylactic reactions
9 Accidental spillage
10 Disposal of cytotoxics
11 Giving information about treatments
12 Giving information about side effects of treatment
13 Supporting the patient emotionally
14 Supporting relatives emotionally
15 Patient distress about their treatment
16 Education/knowledge deficits of other nursing staff
Cross tabulations
Cross tabulations and Somer’s d tests were undertaken to depict associations between the worry statements and the following aspects of their role: the amount and adequacy of education both pre-registration and post-registration received; place of work and frequency of administration and nursing grade; few statistically relationships were found. The only statistical significant associations were between nurses grades and four of the expressed worries (Table 4.16)
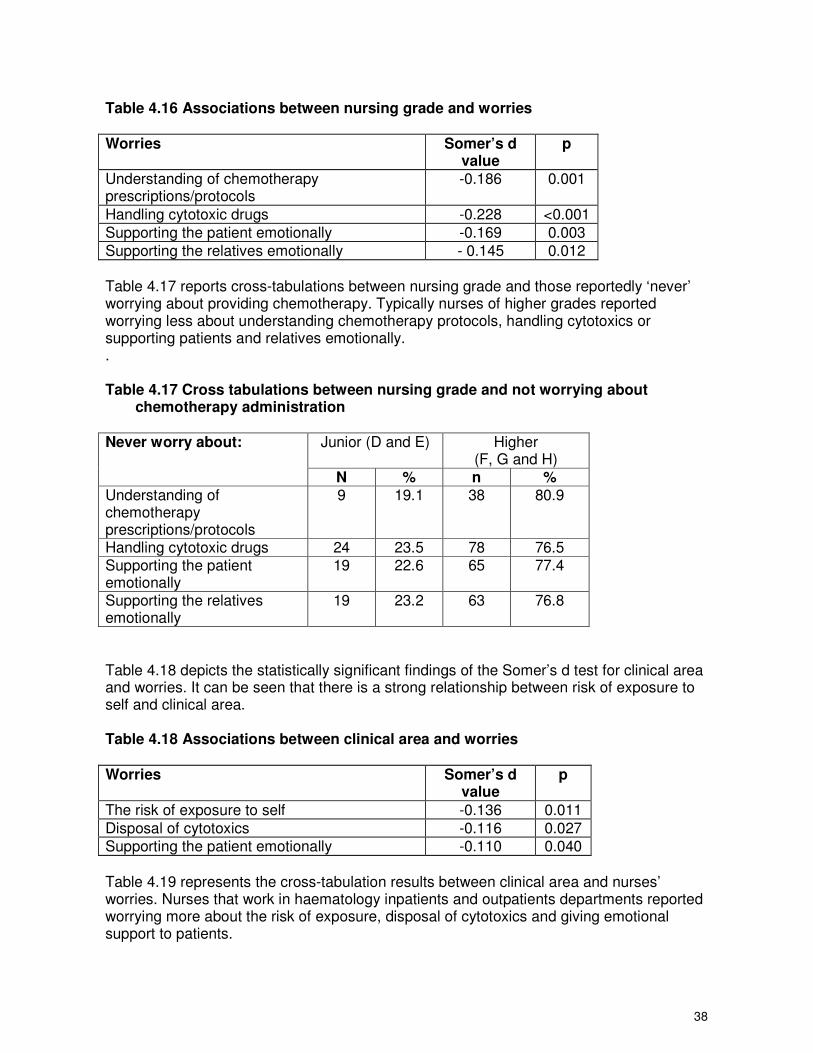
38
Table 4.16 Associations between nursing grade and worries
Worries Somer’s d value
p
Understanding of chemotherapy prescriptions/protocols
-0.186 0.001
Handling cytotoxic drugs -0.228 <0.001
Supporting the patient emotionally -0.169 0.003
Supporting the relatives emotionally - 0.145 0.012
Table 4.17 reports cross-tabulations between nursing grade and those reportedly ‘never’ worrying about providing chemotherapy. Typically nurses of higher grades reported worrying less about understanding chemotherapy protocols, handling cytotoxics or supporting patients and relatives emotionally. . Table 4.17 Cross tabulations between nursing grade and not worrying about
chemotherapy administration
Junior (D and E) Higher (F, G and H)
Never worry about:
N % n % Understanding of chemotherapy prescriptions/protocols
9 19.1 38 80.9
Handling cytotoxic drugs 24 23.5 78 76.5 Supporting the patient emotionally
19 22.6 65 77.4
Supporting the relatives emotionally
19 23.2 63 76.8
Table 4.18 depicts the statistically significant findings of the Somer’s d test for clinical area and worries. It can be seen that there is a strong relationship between risk of exposure to self and clinical area. Table 4.18 Associations between clinical area and worries
Worries Somer’s d value
p
The risk of exposure to self -0.136 0.011
Disposal of cytotoxics -0.116 0.027
Supporting the patient emotionally -0.110 0.040
Table 4.19 represents the cross-tabulation results between clinical area and nurses’ worries. Nurses that work in haematology inpatients and outpatients departments reported worrying more about the risk of exposure, disposal of cytotoxics and giving emotional support to patients.

39
Table 4.19 Cross tabulations between clinical area and worries
Haematology (in/outpatients)
Oncology (in/outpatients)
Other Always worry about:
n % n % n % The risk of exposure to self 24 70.6 7 20.6 3 8.8 Disposal of cytotoxics 14 63.6 5 22.7 3 13.6 Supporting the patient emotionally
12 63.2 4 21.1 3 15.8
Non-Parametric tests – Mann Whitney
Educational level
Non-parametric independent samples tests were carried out on each of the worry statements to determine whether nurses’ worries were influenced by educational level. However no statistically significant differences were found in worry statements and educational level.
Chemotherapy administration experience
Further Mann Whitney tests were conducted to determine differences in worries according to chemotherapy administration experience. To enable this, the sample were divided into two groups (i.e. less experienced <5 years and more experienced >5 years). These tests determined that more experienced nurses worried significantly less about ‘handling cytotoxic drugs’ (Z= -2.162, p=0.031) or about ‘understanding chemotherapy
prescriptions/protocols’ (Z= -2.339, p=0.019), than nurses with less than five years experience.
Attitudes towards Chemotherapy administration
Table 4.20 indicates respondents’ attitudes to 21 different statements about their chemotherapy practice. Two hundred and fourteen respondents (85.3%) strongly agree that ‘patients should always be informed about their treatment’. One hundred and sixty five respondents (65.5%) agreed that they ‘know enough about chemotherapy to answer patients’ questions adequately’ and one hundred and thirty one respondents (52.6%) strongly disagreed that ‘Administering/ handling chemotherapy is no different than administering/ handling intravenous antibiotics’.

40
Table 4.20 Attitudes towards chemotherapy administration
Number and percentage of respondents
Attitude statements Strongly agree
Agree Disagree Strongly disagree
a. When presented with complications caused by chemotherapy I feel confident in my competency. (P)
79 (30.7%)
162 (63%)
8 (3.1%)
1 0.4%)
b. It causes me distress when I see patients affected by chemotherapy I have given them (N)
31 (12 %)
117 (45.5%)
87 (33.9%)
13 (5%)
c. I know enough about chemotherapy to answer patients’ questions adequately (P)
50 (19.5%)
165 (64.2%)
34 (13.2%)
3 (1.2%)
d. When presented with emergencies caused by chemotherapy I do NOT feel confident in my competency(N)
2 (0.8%)
28 (10.9%)
159 (61.9%)
60 (23.4%)
e. Chemotherapy causes more harm than good. (N) 2 (0.8%)
22 (8.6%)
160 (62.3%)
62 (24.1%)
f. I handle and administer chemotherapy without hurrying (P)
90 (35%)
122 (47.5%)
34 (13.2%)
4 (1.6%)
g. I handle and administer chemotherapy without interruptions. (P)
46 (17.9%)
85 (33%)
103 (40.1%)
16 (6.3%)
h. Giving chemotherapy to patients makes me feel guilty. (N)
2 (0.8%)
12 (4.7%)
125 (48.6%)
112 (43.6%)
I. I know that all precautions are taken to ensure that I am not at risk from chemotherapy. (P)
56 (21.8%)
136 (52.9%)
48 (18.7%)
9 (3.5%)
j. Patients should always be informed about their treatment. (N)
214 (83.3%)
35 (13.6%)
0
2 (0.8%)
k. I know that when I administer chemotherapy patients have understood as much as they wish to about their treatment. (P)
99 (38.5%)
131 (51%)
21 (8.2%)
1 (0.4%)
l. I always feel that I have supported patients during their chemotherapy treatment. (P)
95 (37%)
144 (56%)
13 (5%)
0
m. Giving chemotherapy impedes communication with patients. (N)
6 (2.3%)
17 (6.6%)
122 (47.5%)
96 (37.4%)
n. It is easy to inform patients about their treatment but harder to help them emotionally. (N)
31 (12%)
150 (58.4%)
63 (24.5%)
6 (2.3%)
o. I focus entirely on the practical aspects of the task when giving/handling chemotherapy (N)
19 (7.4%)
52 (20.2%)
143 (55.6%)
36 (14%)
p. I try to avoid patients that are experiencing bad side effects from chemotherapy I have given them (N)
6 (2.3%)
5 (1.9%)
112 (43.6%)
129 (50.2%)
q. Administering/ handling chemotherapy is no different than administering/ handling intravenous antibiotics (N)
10 (3.9%)
8 (3.1%)
100 (38.9%)
131 (51%)
r. Talking with patients about their treatments is stressful (N)
8 (3.1%)
77 (30%)
133 (51.8%)
30 (11.7%)
s. Patients know more about their chemotherapy than I do (N)
3 (1.2%)
23 (9%)
164 (63.8%)
57 (22.2%)
t. Administering/ handling chemotherapy is a satisfying part of my role. (P)
49 (19%)
162 (63%)
35 (13.6%)
4 (1.6%)
u. I do not find administering/ handling chemotherapy a challenging part of my role (P)
10 (3.9%)
42 (16.3%)
154 (59.9%)
44 (17.1%)
(P) = positive statements (N) = negative statements In addition, scores given by respondents to the attitude items were summed to provide a total attitude score per respondent. The attitude scale included 21 items statements; as a 4-point Likert scale was used, the highest possible score indicating a positive attitude would be 84. The attitude scale included both positive and negative item statements. Positive attitude statements were scored 4 =strongly agree, 3= agree, 2=disagree, 1= strongly disagree, conversely negative attitude statements were scored 1 =strongly agree, 2= agree, 3=disagree, 4= strongly disagree. Scores reported by the sample ranged from 47-79 (mean score 63).

41
Figure 4.7 illustrates the proportion of the sample that agrees or disagrees with each attitude statement. The majority of respondents agreed with statement a: When presented with complications caused by chemotherapy I feel confident in my competency (96.4%) and statement j: Patients should always be informed about their treatment (99.2%). Conversely, most respondents disagreed with statement h: Giving chemotherapy to patients makes me feel guilty (94.4%) and statement p: I try to avoid patients that are experiencing bad side effects from chemotherapy I have given them (95.6%).
Figure 4.7 Nurses’ Response to Attitude Statements
0
20
40
60
80
100
120
a b c d e f g h I j k l m n o p q r s t u
Attitude statements
%
Agree/Strongly Agree
Disagree/Strongly disagree
Cross tabulations – Somer’s d
Cross tabulations were performed with the attitude statements against the variables: nursing grade, amount of education pre- and post-registration, adequacy of education pre- and post-registration, place of work (i.e. unit or centre), clinical area and frequency of administration. A Somer’s d test was also carried out to measure the association between each of these variables and the attitude statements. No statistically significant relationship was found between nurses’ attitudes towards chemotherapy administration and the following variables: the amount and adequacy of chemotherapy education pre- and post-registration, clinical area and frequency of administration. However there was some association between nurses’ attitudes and their nursing grade and place of work. Table 4.22 shows the cross tabulations for those with statistically significant associations between attitudes and nursing grade.

42
Table 4.21 Significant associations between attitude and nursing grade
Disagree with: Higher (F, G and
H)
Junior (D and E)
Somer’s d value
p
n % n %
I handle chemotherapy without interruptions
78 79.5 20 20.4 -0.185 <0.001
I focus entirely on the practical aspects of the task when giving/handling chemotherapy
101 74.3 35 25.7 0.257 <0.001
It can be seen that the higher grades tend to disagree more with these attitudes statements. Table 4.22 shows the cross tabulations where, there were statistically significant associations between attitudes and place of work (centre/unit). Table 4.22 Significant associations between attitudes and place of work
Agree with: Centre Unit Somer’s d value
p
n % n % I know enough about chemotherapy to answer patients’ questions adequately
115 69.7 50 30.3 0.147 0.026
I know that all precautions are taken to ensure that I am not at risk from chemotherapy
85 62.5 51 37.5 0.152 0.022
I always feel that I have supported patients during their chemotherapy treatment
104 72.2 40 27.8 0.229 0.001
Non-Parametric tests determining difference in attitudes
Educational Level
A non-parametric independent samples test was carried out on each of the attitude statements to determine if there were differences in attitudes according to nurses’ educational level. The sample was divided into two groups those not educated to degree level or above and those who were. There were statistically significant differences in attitudes recorded on two items according to education. Those with higher qualifications were more likely to agree with the following statements:
‘When presented with complications caused by chemotherapy I feel confident in my competency’ (Z=-2.160, p=0.031)

43
‘I handle and administer chemotherapy without interruptions’ (Z=-2.210, p=0.027).
Chemotherapy administration experience
A non-parametric independent samples test was carried out to identify any differences between nurses’ attitudes according to their level of chemotherapy administration experience. Nine statements showed statistically significant associations between group differences. (Table 4.23) Typically those with greater experience showed a more positive attitude to chemotherapy and exhibited statistically significant greater confidence in their competence. Table 4.23 Mann Whitney results- Attitude by chemotherapy experience Attitudes Mann Whitney p When presented with complications caused by chemotherapy I feel confident in my competency
-4.183 <0.001
I know enough about chemotherapy to answer patients’ questions adequately
-3.076 0.002
When presented with emergencies caused by chemotherapy I do NOT feel confident in my competency
-3.856 <0.001
Chemotherapy causes more harm than good -2.327 0.020 I handle and administer chemotherapy without interruptions -2.023 0.043 Giving chemotherapy to patients makes me feel guilty -2.721 0.007 I focus entirely on the practical aspects of the task when giving/handling chemotherapy
-2.777 0.005
Patients know more about their chemotherapy than I do -4.720 <0.001
Ordinal Regression
The explanatory variables: site (centre/unit), educational level, grade and experience were entered into a regression model in an attempt to explain variability in differences regarding worries about chemotherapy role. However, since grade appeared to be the only significant factor, the model was re-run with grade as the only independent factor, the outcomes of this final model are shown in Table 4.24.

44
Table 4. 24 Ordinal regression model for worries about chemotherapy role
Nursing Grade
D-E
F G
Worries about chemotherapy
β se(β) β se(β) β se(β) χ2 3df) p
a. Worries about your understanding of chemotherapy 1.656 0.468 1.078 0.444 0.901 0.471 12.748 0.005 b. Worries about handling cytotoxic drugs 1.475 0.438 0.802 0.430 0.554 0.454 14.036 0.003 c. Worries about reconstituting chemotherapy on the ward 1.180 0.570 0.839 0.573 0.989 0.606 4.447 0.22 d. Worries about the risk of exposure to yourself
1 2.279 0.652 1.066 0.661 0.693 0.702 25.116 <0.001
e. Worries about extravasation 1.372 0.427 1.083 0.420 0.703 0.442 11.636 0.009 f. Worries about treatment side effects 1.266 0.417 1.018 0.408 0.278 0.431 14.197 0.003 g. Worries about allergic reactions 1.040 0.431 1.051 0.425 0.493 0.449 8.467 0.037 h. Worries about patient anaphylactic reactions
1 1.249 0.513 0.991 0.509 0.666 0.539 6.912 0.075
i. Worries about accidental spillage 1.106 0.427 1.136 0.422 0.734 0.444 8.487 0.037 j. Worries about disposal of cytotoxics 0.914 0.429 0.419 0.427 0.432 0.451 5.624 0.13 k. Worries about giving information about treatments 1.172 0.422 0.455 0.413 0.197 0.440 12.128 0.007 l. Worries about giving information about side effects of treatment 1.092 0.421 0.409 0.413 0.135 0.440 11.173 0.011 m. Worries about supporting the patient emotionally 0.781 0.405 0.028 0.398 -0.304 0.426 11.816 0.008 n. Worries about supporting relatives emotionally 0.650 0.408 0.078 0.400 -0.269 0.427 8.041 0.045 o. Worries about patient distress about their treatment 0.539 0.405 -0.206 0.400 -0.399 0.425 9.404 0.024 p. Worries about education/knowledge deficits of other nursing staff -0.507 0.396 -0.398 0.390 -0.134 0.412 2.381 0.50
It can be seen that nursing grade had a significant impact on the worries nurses had about their chemotherapy role as 12 of the 16 worry statements showed significant relationships with nursing grade. Similarly regression modelling was undertaken to determine how the variables: site (centre/unit), educational level, grade and experience impacted on ‘attitudes towards chemotherapy’. Table 4.26a and 4.26b show the results of the regression with attitudes. The effect of site, educational level, job grade and experience vary across items. Site is significantly associated three times, educational level once, grade twice, and experience four times. Only one item "I always feel that I have supported patients during their chemotherapy" has two significant factors. Thus it appears that there was no one factor that explains variability in attitudes, although aspects one would expect to be impacted by experience did appear to be so, for example, feelings of competency.

45
Table 4.26a Ordinal regression model for attitudes towards chemotherapy (Site and Educational level)
Site Educational Level Centre HE educated
Attitude statements ββββ se(ββββ) p ββββ se(ββββ) p
a. When presented with complications caused by chemotherapy I feel confident in my competency. -0.053 0.330 0.87 0.542 0.387 0.16
b. It causes me distress when I see patients affected by chemotherapy I have given them 0.348 0.279 0.21 -0.692 0.348 0.047
c. I know enough about chemotherapy to answer patients’ questions adequately -0.446 0.304 0.14 -0.057 0.374 0.88
d. When presented with emergencies caused by chemotherapy I do NOT feel confident in my competency -0.249 0.300 0.41 0.382 0.367 0.30
e. Chemotherapy causes more harm than good. -0.002 0.308 1.00 -0.580 0.387 0.13
f. I handle and administer chemotherapy without hurrying 0.147 0.277 0.60 -0.343 0.345 0.32
g. I handle and administer chemotherapy without interruptions. -0.026 0.272 0.92 -0.518 0.343 0.13
h. Giving chemotherapy to patients makes me feel guilty. -0.253 0.290 0.38 -0.373 0.362 0.30
I. I know that all precautions are taken to ensure that I am not at risk from chemotherapy. -0.593 0.284 0.036 -0.367 0.35 0.29
j. Patients should always be informed about their treatment. -0.251 0.454 0.58 -0.093 0.554 0.87
k. I know that when I administer chemotherapy patients have understood as much as they wish to about their treatment. -0.436 0.285 0.13 0.310 0.355 0.38 l. I always feel that I have supported patients during their chemotherapy treatment. -0.880 0.296 0.003 -0.171 0.372 0.65
m. Giving chemotherapy impedes communication with patients. 0.192 0.288 0.51 0.183 0.358 0.61
n. It is easy to inform patients about their treatment but harder to help them emotionally. 0.394 0.293 0.18 -0.090 0.362 0.80
o. I focus entirely on the practical aspects of the task when giving/handling chemotherapy 0.338 0.284 0.23 -0.195 0.355 0.58
p. I try to avoid patients that are experiencing bad side effects from chemotherapy I have given them 0.041 0.296 0.89 0.009 0.368 0.98
q. Administering/ handling chemotherapy is no different than administering/ handling intravenous antibiotics -0.063 0.289 0.83 -0.144 0.353 0.68
r. Talking with patients about their treatments is stressful 0.297 0.285 0.30 -0.509 0.352 0.15
s. Patients know more about their chemotherapy than I do 0.017 0.310 0.96 -0.312 0.381 0.41
t. Administering/ handling chemotherapy is a satisfying part of my role. -0.670 0.301 0.026 -0.090 0.371 0.81
u. I do not find administering/ handling chemotherapy a challenging part of my role -0.194 0.296 0.51 -0.273 0.367 0.46

46
Table 4.26b Ordinal regression model for attitudes towards chemotherapy (Nursing grade and Experience)
Nursing Grade Experience
D-E F G
Attitude statements
β se(β) β se(β) β se(β) p β se(β) p
a. When presented with complications caused by chemotherapy I feel confident in my competency. -1.176 0.569 -0.848 0.506 -1.090 0.513 0.14 -0.693 0.335 0.038
b. It causes me distress when I see patients affected by chemotherapy I have given them. -0.282 0.501 -0.224 0.458 0.358 0.464 0.33 -0.396 0.286 0.17
c. I know enough about chemotherapy to answer patients’ questions adequately -1.325 0.546 -0.810 0.492 -0.462 0.491 0.079 -0.306 0.316 0.33
d. When presented with emergencies caused by chemotherapy I do NOT feel confident in my competency -0.444 0.538 -0.089 0.490 -0.029 0.490 0.70 -0.861 0.316 0.006
e. Chemotherapy causes more harm than good. -1.405 0.550 -0.894 0.496 -0.972 0.500 0.081 -0.268 0.322 0.41
f. I handle and administer chemotherapy without hurrying 0.220 0.502 -0.142 0.458 -0.692 0.463 0.097 -0.019 0.290 0.95
g. I handle and administer chemotherapy without interruptions. 0.803 0.492 0.283 0.449 -0.018 0.455 0.13 0.165 0.279 0.55
h. Giving chemotherapy to patients makes me feel guilty. -0.142 0.523 0.227 0.480 0.482 0.487 0.38 -0.577 0.299 0.054
I. I know that all precautions are taken to ensure that I am not at risk from chemotherapy. -0.146 0.503 -0.364 0.46 -0.348 0.465 0.78 0.307 0.289 0.29
j. Patients should always be informed about their treatment. -1.204 0.905 -1.193 0.847 -0.262 0.922 0.28 0.334 0.425 0.43
k. I know that when I administer chemotherapy patients have understood as much as they wish to about their treatment. -0.604 0.514 -0.355 0.469 0.003 0.474 0.44 0.568 0.297 0.056
l. I always feel that I have supported patients during their chemotherapy treatment. -0.448 0.533 -0.637 0.491 -0.111 0.490 0.45 0.644 0.314 0.040
m. Giving chemotherapy impedes communication with patients. -0.668 0.523 -0.557 0.469 -0.202 0.472 0.50 0.103 0.299 0.73
n. It is easy to inform patients about their treatment but harder to help them emotionally. -1.189 0.532 -0.618 0.479 -0.452 0.482 0.12 0.233 0.304 0.44
o. I focus entirely on the practical aspects of the task when giving/handling chemotherapy -1.895 0.531 -1.453 0.484 -0.733 0.484 0.002 -0.175 0.294 0.55
p. I try to avoid patients that are experiencing bad side effects from chemotherapy I have given them -0.583 0.531 -0.008 0.483 0.356 0.492 0.13 -0.023 0.306 0.94
q. Administering/ handling chemotherapy is no different than administering/ handling intravenous antibiotics 0.740 0.519 0.702 0.474 0.427 0.474 0.47 -0.159 0.298 0.60
r. Talking with patients about their treatments is stressful -1.123 0.523 -0.769 0.475 -0.619 0.481 0.20 0.445 0.294 0.13
s. Patients know more about their chemotherapy than I do -0.994 0.554 -0.704 0.497 -0.529 0.502 0.35 -1.058 0.337 0.002
t. Administering/ handling chemotherapy is a satisfying part of my role. -0.231 0.537 -0.170 0.491 -0.438 0.497 0.82 0.413 0.311 0.18
u. I do not find administering/ handling chemotherapy a challenging part of my role -1.067 0.537 -0.669 0.488 0.189 0.483 0.020 -0.036 0.306 0.91

47
5 Results from Component two – ethnography
Introduction
The two units were very different in terms of their make-up, work practices and the context in which nurses worked. Although the settings were researched independently by different researchers, themes emerging were the same albeit from opposite ends of a continuum. The themes centred around factors which facilitated chemotherapy nurses’ work and factors which impinged on their work. What was interesting was that factors that facilitated nurses’ work in one unit were the same factors that impinged on the nurses’ work in the other. This section will begin by describing the work organisation within the different units before continuing to discuss the themes emerging from the study.
Chemotherapy Day Unit 1 (CDU 1)
Factors which facilitate nurses’ work
Organisation of work
In CDU 1 patients were scheduled with an appointment. They came to the clinic two days previously to have their blood taken, see the doctor and nurse if necessary, and have their treatment prescribed. Each nurse on the unit was allocated a particular specialist clinic so that there is continuity with the consultants, doctors, patients, and their chemotherapy regimes. As chemotherapy regimes and treatment trials change rapidly, the nurse gets to know the regimes/treatments very well so can pick up early if there are any anomalies in the patient’s condition. At the end of the clinic, the nurse would get the patients results and write them on the prescription chart before it went to pharmacy for the chemotherapy to be dispensed. If the results were not within an acceptable range, the nurse could discuss this with the doctor and if necessary telephone the patient. There were times when patients needed a blood transfusion or had to wait for extended recovery time before being able to have more chemotherapy. There were also times when regimes needed to be changed because they were having such a debilitating effect on the patient’s condition. When patients were referred for chemotherapy, the nurse allocated to that specialty would telephone the patient and make an appointment for the patient to come in and have what was referred to as a “work up”. This was an assessment interview where the nurse would assess the patient’s physical condition, explain the process of chemotherapy, the particular regime and possible side effects. The nurse would also talk to the patient and assess how the chemotherapy would affect them personally and the impact it may have on the person’s life. At this time the nurse would book subsequent appointments for the patient depending on what time suited them and the length of the chemotherapy administration process. The appointment book is divided into 4 columns representing 4 nurses (1 nurse is in clinic). Patients are booked onto a slot and the number of hours it will take to treat them is blocked out. At the beginning of the day in CDU 1, a nurse goes to pharmacy, which is a short distance from the unit, and collects the drug charts and chemotherapy for patients expected that day. The drugs and charts are taken to the treatment room where they remain until they are administered. They are checked at this point so that if there are drugs missing or not dispensed, these can be followed up early. Drugs, still packaged, are laid out with the drug chart. The patients and drugs are checked with the appointment sheet for that day to

48
ensure all patients expected have drugs. If there are anomalies at this point they can be followed up early. There are often drug charts missing or still in pharmacy at this point which nurses follow up. The nurses then decide who is to take which column (of the appointment book) and hence which patients. When patients arrive they go to the desk at the entrance of the unit and greet Jane1, the receptionist. Once Jane knows they have arrived the patients go and wait in the main waiting area, which has a television and magazines etc for people as they wait. Jane goes to the treatment room and lets the nurses know which patients have arrived. The nurse goes to greet the patients and bring them in to the unit. The nurses do not wear uniform, at this point the nurse is not wearing gloves or an apron. The nurse brings the patient in and sits them down. For the most part patients are accompanied by friends or relatives. The nurse sits down and chats with the patient, asks them how they are and how they have been since the last treatment. Invariably, the relative or the nurse gets the patient a drink from the kitchen space at the corner of the room. The nurse then goes to the treatment room, puts on an apron, washes her hands and begins to prepare the aseptic tray. When the nurse has the drugs ready, she gets a trolley that has all the equipment for cannulation and goes back to the patient. She invariably does a set of observations and begins to cannulate the patient to administer the chemotherapy. The nurses like working in this planned way. Before the work was organised through the appointment system or scheduling, the patients would turn up and have to have their bloods taken, see the doctor or wait for him to prescribe the chemotherapy, wait for the drugs to be dispensed and wait for a nurse to be free to administer the chemotherapy. The nurses reported how stressful this was as can be seen by the following quote:
There were often angry patients who had been waiting too long. It was really stressful. We were helpless until
they had the results and the drugs. Often patients who were quite ill were waiting for hours which was not
good for them. Also if the patient was too unwell to have the chemo they would still be sitting here waiting for
half the day to have confirmed what you knew by looking at them. It was terrible. And the clinic was always
late. You spent all morning waiting with nothing to do and racing around having no time to talk to anyone. It
was really stressful.
Nurses spoke about how the old system made both nurses and patients more anxious. Once people came in and the waiting started. Nurses would be anxious cos you could never know what time
you were going to start let alone finish. Patients were so anxious and they were everywhere. Every time you
went passed they were “where’s my treatment, where’s my treatment”. We used to walk passed with our heads
down trying not to give eye contact.
For the most part patients liked having their treatment scheduled especially, as they could have their blood taken locally and phone through or have the hospital phone through the results. However, there were one or two patients who preferred the old system.
I know it wasn’t good for everyone but it suited me. I was quite well with my treatment and didn’t want to be
up here more than I had to. Some people were very ill and you could see it took its toll…all that waiting.
The way the work was organised through scheduling facilitated the nurses administering chemotherapy in a number of ways. It meant that the nurses could organise their work themselves and were not waiting either for results, for doctors to see patients and write up prescription or for drugs to be dispensed. It also meant that there was less stress within the unit and there was a relaxed atmosphere. Nurses seemed to have more time to spend with patients. The nurses did not go off the ward for their tea break. Instead, whoever was making a drink would make one for whoever wanted one. It could be patients, relatives, Jane or the nurses. Some nurses smoked so would go for a cigarette break. However, the nurses
1 All names have been changed.

49
always went off for their lunch break. They would go in pairs so that they could go out of the hospital, get some air and have a change of environment. Throughout the whole of data collection there was only one time (when there were only 2 nurses on duty) the nurses had to stay on the unit for their lunch break.
The ward team
The ward team on CDU1 was very cohesive and they worked well together. All 5 nurses were experienced nurses with both formal education and experience in giving chemotherapy. They helped each other with their work and discussed treatment options and patient problems. There seemed a large degree of trust and respect among the nurses as can be seen in this quote:
We are a good team and we work off one another. We help each other and are almost fluid in the way we work.
We can discuss things if you are not happy with something…it makes a difference to be able to discuss it with
your peers and decide what you are going to do. It wasn’t always like that. We had one nurse who used to
change the whole atmosphere if she had a row with her boyfriend…it was terrible. Luckily she left.
Each Friday an hour was put aside for a staff meeting. The unit did not open until 10.00. The meeting was used so that Alice could feedback any information from the cancer directorate or the Trust. It was also used for presentations from drug representatives about new drugs; or from the research team or doctors if there was a new treatment. These presentations were usually accompanied by breakfast so the staff looked forward to them. Alice would also use the meeting to comment on how the week had gone and if there were any issues. All staff also had an opportunity to put items on the agenda. An example follows:
When everyone had gone round, Alice thanked everyone for their hard work this week. She said it had been
difficult as holiday and sickness meant they were low in numbers on most days. However, she said although we
have done really well, we haven’t done well with the follow up letters and the admin work. This is as important
as giving the chemo. “I am as much to blame but I suggest we use the rest of the hour until the patients arrive
to go through our patients’ notes and make sure they are up to date.”
Relationships with patients and relatives
All staff spoke about how their relationships with patients helped facilitate their work. Patients coming to the CDU were very thoughtful to each other and helpful to the nurses. They often helped each other, making drinks for each other and the nurses, or sitting down and chatting. One woman always came early and made tea before she was due to be seen. Sian explains
The patients are so lovely. When you think about what they are going through….they also are always buying
us treats or bring goodies for everyone to eat. Some are hard work obviously but usually they are few and far
between.
Relationships with Support staff
The unit receptionist, Jane, was seen to be a real asset by nurses, patients, doctors and pharmacy. Jane helped to co-ordinate the work of the unit. She ensured patients were booked in, chased up any results or notes that were missing at the beginning of the day. She was often the first port of call when patients telephoned for advice. She knew the patients and often spent time with them. Jane was responsible for a lot of the administration work, recording numbers of patients treated for example.

50
There were also good relationships between the portering services and the transport services. If the nurses needed the porters to collect any samples for the laboratories or collect some blood for blood transfusions, they seemed to be efficient and responded quickly to the request. The transport services were especially helpful to the nurses. The transport office was just opposite the CDU so the transport workers knew the nurses. One particular example from field work illustrates this:
Alice is worried about an elderly who has not been collected by transport. She is due to have Cisplatin which
takes hours and Alice doe not want her going home late and missing her meals on wheels. Julie goes to see
Beth in transport. Beth says there is no record of the request. She tells Julie to get Alex to fill out another
request which Julie does. “We will try and get her as soon as possible” Beth says. “Let us know if they pick
her up before 12 that would be ok by the time she is here and settled. But if she is not picked up by 12 we will
have to leave it for tomorrow. Beth is in agreement with this and speaks to the driver by mobile. Unfortunately,
there are problems with road works and traffic. Alice and Julie are in contact with Rose on the phone. By 12
the driver calls in to say he is not going to make it. Beth books it for early the next day, Alice telephones Rose
to have the chemotherapy first thing the next day. Rather than blaming each other and wasting time on who’s
at fault, everybody just got on trying to resolve the situation.
Other healthcare professionals
For the most part, nurses had good relationships with medical staff. The nurses worked fairly autonomously. If they were unhappy giving a patient chemotherapy, they would talk to the patient first then inform the doctor, explaining their rationale. The doctors respected the nurses’ decisions and would often telephone the nurses to ask their opinion of the patient if there were any queries. It was accepted that the nurses knew the patients well and the way in which they normally reacted to their chemotherapy regimes. There were many examples during data collection where consultants would bring new doctors or visiting doctors to meet the nurses in the unit as this extract from fieldnotes illustrates: .
Dr Black walked into the treatment room. Alice, Jane and myself were there. “And this is Alice and the team.
They can really help you get to grips with how things work. Alice, Jane and oh I don’t you, are you new?”
There seemed to be a great deal of respect for the nurses and their level of knowledge and experience. There were a few exceptions, one consultant, who liked the other hospital in the cancer unit, would not bring their patients to the CDU. The nurses also had good relationships with the pharmacy staff. The pharmacy staff ensured that the chemotherapy drugs were dispensed as soon as possible and if there were anomalies would bring the chart to the nurses to discuss the prescription. This cut down on any waiting time. Both teams worked together to ensure the chemotherapy was administered to the patients as quickly as possible. Alice explains:
They are really good here, the pharmacy, .they work with us not against us.
The environment Managing emotions
Both nurses and patients spoke about the importance of the atmosphere in the CDU. There is a relaxed atmosphere. There is much joking and calling over from one patient to another. Notes from fieldwork show how patients group and joke together:
There is a group of men sitting on one side joking with each other. Alice has to move one of them because she
needs a plug for his infusion. There is much joking about her breaking them up because they are too rowdy. It
comes from them and Alice joins in. “We can’t have you in gangs”. One of the men says he will move so that
his friend can have his plug.
The importance of having fun in the unit was stressed as a way of helping people to cope with the treatment by nurses and patients. One woman having chemotherapy for liver cancer said:
51
I need to have a bit of a joke, it helps. I need to keep my spirits up, for the nurses to bouy me up while I am
having this. I need to keep as strong as possible. I can think about how awful it is and was later but not now. I
need to be focussed on good things.
Though there was much joking, the nurses also assessed the impact treatment was having on the patients and their families. The importance of having fun but also being serious is noted in the following fieldnotes.
Sian and her patient and his wife are joking with Alice and her patient. He is really laughing as he sneezes and
blows his nose. Sian says he is allergic to Alice. She waits for her patient to stop laughing, then turns more
into him and asks him how he has been. She is looking intently at his eyes and face. He says “fine”. She is then
more specific. “How many times roughly are you passing urine in a day, how much are you eating, has your
month been sore or dry, have you been itchy. The questions are concerning his physical state initially then
move into other areas. Are you sleeping, how is your mood, how are you both coping with all this. She is really
huddled over the couple.
Patients and their relatives seemed very comfortable within the CDU. They often wandered over to other patients to see how they were, made each other (and the staff) drinks at times. If a patient looked not very well, invariably others would come over and see if there was anything they could do. The following notes from fieldwork are a typical example:
As soon as Debra was feeling better, she asked for the curtains to be drawn back again. Faye, another patient,
went in to see Debra. She was wheeling her dripstand as she went. “You worried me there” she said to Debra.
“I’m sorry, I could see you worry.” “Its silly really, I know nothing can happen and the nurses always keep
everything under control but you never know…”. The patients get quite close to each other as they meet up on
the same day and often have similar diagnoses.
Knowledge and education
All participants (nurses and patients) spoke about the importance of knowledge and education in the work of chemotherapy nurses. All nurses on CDU 1 had formal chemotherapy education as well as a lot of experience. Patients spoke about needing to trust that the nurse knew what they were doing. As Jake stresses:
You are putting your life literally in their hands. You can tell if they know what they are doing. They are all
very experienced here. I have been some places where the nurse is shaking as she is doing it. It doesn’t give
you confidence. You can tell when you ask a question whether they really know the answer or if they are
bluffing.
Most nurses also spoke about how their experience helped increase their knowledge and skill as Beth’s comment shows:
I had done my N59 so I knew the theory and what I should be doing and looking for. But because I was on a
ward and we didn’t give chemotherapy that often I don’t think I was very good. There was no-one with
experience, a role model, who I could learn the idiosyncrasies.
This quote also shows the importance of role models, as Sian indicates: I had had the theory but I was terrified of doing it. Luckily the sister on the ward was very old fashioned. She
insisted people had a mentor and observed a certain number before first trying on someone with good veins
and gradually learning techniques for people with difficult veins. It was like an apprenticeship. It made you
feel guided.
Job satisfaction
Enjoying their role and the effect they had on people was important for nurses. Most spoke about how important they thought the role of the CDU was in people’s cancer journey.

52
They also spoke about the importance of enjoying their work and the relationships they had with people.
You know its funny when I tell people what I do, they say…oh that must be awful and sometimes I think I must
be weird because I really like it. I have my weekends off; I work with good people and we have a laugh. I like
the fact that I am good at it. I like getting to know the patients, seeing them relax and see their trust.
The telephone
The telephone was a dominant feature of fieldwork. There were three or four handsets dotted around in various places in the CDU. It was constantly ringing with queries from patients, relatives, doctors, district nurses, liaison workers, pharmacy, or with results. However, the telephone was not seen as an intrusion. On the contrary, nurses regarded the telephone as a real asset to their work. Jo explains:
You do need to have it fairly close cos its always ringing. But at least that means you can get things sorted out
before they become a problem. We tell the patients to never worry about ringing us. Often it something minor,
they just want to check something but other times…If we are worried about what they are saying ..we can call
the doctors and alert them, we can get them an ambulance and bring them in. There are also times we need to
call them. Say their results have come back low. We can ring them and say…have a rest for another couple of
days or come and have some blood etc. I remember on the ward I used to really worry about calling people, it
seemed you only did it if you had bad news…its not like that here.
Factors which impinge on the work of chemotherapy nurses - CDU 1
The Environment
Both nurses and patients spoke about how the layout and décor of the CDU impinged on the chemotherapy administration process. CDU 1 was in the basement so did not get any natural sunlight. The lighting was fairly stark and the decoration was drab. There was also a consensus of opinion that there was not enough space or facilities for the through-put of patients. Mary indicates the effect it has in the following:
Looking at the area sometimes really gets you down. The décor is oppressive. I am sure it was bright once but
it just looks dingy. There is not enough space, we need more sockets. We never see daylight. If it dies that to
us..imagine how it must be for the patients who only have to look at the walls whilst they are having chemo.
It’s great that we are in with the clinics and radiotherapy etc but we need to have it looked at. It would be
good to get one of those programmes to design it for us!
The environment also affected the communication between the nurse and the patients. Nurses said they would like some more space between patients so that they could talk freely to patients. Jo reports:
It’s hard enough for people but sometimes they are almost sitting on top of each other. If we want to talk to
them about something personal, its really hard.
There was an interview room off the CDU but for the most part that was used for planned conversations eg initial workup interview or breaking bad news. Nurses felt it drew attention to patients and made them more anxious. Alice explains:
There are times I know we could talk to patients more, things like sexuality, how they are coping, their
relationships with their loved ones.; but to say shall we go into the other room and chat seems to single them
out more as people look at you going off. We still do it…if they seem upset or if they seem to have something
on their mind BUT it would be good to have a system where we could routinely have some private time with
them, and space to do that.
Another aspect of shortage of space was that of patient privacy. A number of patients said they were often embarrassed by their Hickman or PICC lines if other patients were too close.

53
It’s a bit much sometimes because I have to unbutton my shirt and sometimes there’s ladies too near by. And
when you go to the toilet..everyone knows..and can hear!!!
Lack of time – increased workload
The nurses on the CDU were extremely busy. The only time they sat down was when they were cannulating a patient or giving them their chemotherapy drugs. Nurses and patients spoke about the increased number of patients being treated and the effect this had on the unit. One patient, Jackie, who had had chemotherapy the previous year remarked:
I can’t believe how busy it is now. There was always a lot of people in the waiting room cos we were waiting,
but now there are so many in here having treatment. Has the number of people with cancer gone up?
There was documentary evidence of the increase in numbers according to the Directorate figures. However, there was no corresponding increase in staff numbers. In fact even when there was a poor staffing levels, the nurses still seemed to be left to cope on their own. This particular incident reported in fieldnotes acts as an example:
Today there are 32 patients and only 2 nurses on the unit due to the vacancy, holiday and sickness. Alice and
Jo are really busy giving chemo. In the treatment room they are haring around but when they go outside they
move fast but not frantic as they do in the treatment room. I get sandwiches and we eat in the sister’s office.
There is no time for a break. At the end of the day they have treated all the patients …but they look exhausted.
Alice spoke about days like this in her interview: It’s terrible. Although you do try to talk to people, all the time your mind is on the next thing you have to do.
By the end of the day you feel as if all you have been doing is shoving drugs into people. That’s important but
it’s not all that this is about…there’s so much more we need to do.
Chemotherapy Day Unit 2 (CDU 2)
The beginning of data collection was a difficult time for this unit. There were 3 staff vacancies and one nurse was on maternity leave. They were therefore very short staffed and had to rely on agency nurses. The modern matron was new in post and new to the hospital and the sister’s post filled by an experienced chemotherapy nurse “acting up” until a new appointment was made. Recruitment and retention were issues for this unit that had an impact on the context of care. Consequently there weren’t great deal of factors facilitating the nurses’ work.
Factors which facilitate nurses’ work
Relationships with support staff
The support staff on the unit played an important part in the running and organization of the unit. Carol, the receptionist, seemed to help to ensure the nurses had what they needed in terms of notes and information to “process” the patients through. These fieldnotes indicate the role she played
Carol was very friendly and had good relationships with all the patients. They greeted her like a long lost
friend. She in turn would greet them, ask them how they were and, after sitting them down put their name on
the board. She knew all there was to know about each patient, not from their notes but what they told her.

54
Relationships with patients
CDU 2 operated with a “named nurse” framework where the patients were allocated a particular nurse at the start of their treatment. If the nurse was on duty when the patient came in for treatment, she/he would be allocated to give the chemotherapy. Nurses and patients liked this system as it allowed them to develop relationships and get to know each other, as is evident on the following quote from fieldwork
We really get to know our patients. We see the same patients every week and we try to keep the same patient to
the same nurse. You can’t help but build up relationships with them.
Patients really enjoyed knowing who was going to give them their treatment:
The nurses are lovely but sometimes very busy. You get used to waiting, it is off-putting but the nurses are so
nice, you really get to know them. Sometimes you don’t see the same one…its so short staffed.
Patients showed their appreciation of the nurses by bring many gifts of chocolate, biscuits etc. The nurses appreciated this and remarked how it made them feel cared for:
The patients are lovely. They know we don’t get proper breaks so they are always bringing us chocolate and
things to eat.
Factors which impinge on nurses’ work (CDU 2)
As stated earlier, the beginning of data collection was a difficult time for CDU 2. It did seem that there were more factors that impinged on the work of chemotherapy nurses than facilitated them.
Organisation of work
Patients followed a system very much like the one in place in CDU 1 before they had scheduling. However, the clinic and labs were not in the same location. At the end of the day, the work for the following day would be divided between the staff guided by the outpatient’s appointment book. The patients came in early in the morning, had their blood taken and waited for their results, which sometimes took up to 2 hours. If the bloods showed abnormal results, the patients had to wait and see the doctor who had a consulting room in the unit. However, it seemed most patients saw the doctor before treatment. Once the results were seen and were satisfactory, the drugs were prescribed and the patient waited for them to be dispensed before treatment. The unit often stayed open late. Even though opening times were meant to be 08.30 to 16.00, there were often people being treated at 18.00 and later. Nurses felt very frustrated with this system but thought the waiting was inevitable. Nurses and patients would become anxious because of the wait. The patient, wondering how long they would be there, the nurse wondering what time she/he would get home. The following quote is from a patient resigned to the wait:
I know when I come here I am going to be here all day. I come on my own, its too long a day for anyone to
come…its too tiring talking to someone all day …and its not natural. You just have to get on with it.
Because the nurses’ work was so busy, they did not take any breaks which had a detrimental effect on them. Jill explains:
No-one takes lunch here so around 3 everyone started to get really ratty
At the end of data collection, it had been decided that unit would begin to be organized through a scheduling system, similar to CDU 1. It would be interesting to see the effect this will have on the nurses’ work. Staffing levels

55
As already stated staffing levels were very poor on the unit for most of the duration of data collection, which had a detrimental effect on the nurses’ work and experiences. These notes from fieldwork show the constant strain it put on nurses:
There were four nurses on duty, only one was a permanent member of staff. The other three were either bank
or from another ward. Temps are an added strain on the sister and the rest of the permanent staff as they have
to take time to show them around and check they are safe etc…its constantly looking at them.
Constantly checking people meant nurses were not able to give patients the attention they should have, as Mike indicates here:
I feel like a factory worker, I have no time for the patients. just have to check the line is going
Another problem associated with the lack of staff were that important safety issues were being missed as the following extract from fieldnotes shows:
Jack tells the patient that his creatinine and urea seem high. He explains that “toxicity levels are high”. The
daughter asks what that means and then shouts to her father. The patient gets agitated, “that happened last
week” Jack explains that he will need to check with the doctor. “You will have to speak up” The daughter
explains that “he has been like this for 4 days. He was a bit deaf before but now he is terrible”.
However, towards the end of the period a number of people had been recruited filling the vacancies, which gave people hope for the future.
The nursing team
Because the staffing levels were poor and erratic, the team were not very cohesive. For the most part, they seemed to get on with each other but because of sickness and the tension on the unit with patients waiting, the nurses seemed to work for the most part in isolation. They tended to concentrate on their own work and did not help each other as this extract from fieldwork shows:
If a patient is allocated to a nurse, no other nurse goes near that patient. Even if they need their chemotherapy
etc changing. Mike says “people really do not like it if their work is interfered with”. He said it may be
something to do with lack of knowledge ….people tend to hide what they are doing when they are uncertain.
The atmosphere on the unit was very erratic depending on which staff were on duty which made it very difficult to predict the type of day it was going to be. These quotes from different days show how it changed at times.
Entered the unit, no-one acknowledged me. Said hello to Tracey, she grunted back. The tension today is almost
palpable, everybody has their head down, no eye contact.
Got onto the unit, Jack and Sara are laughing. They call over to me and greet me warmly. Everybody seems in
a good mood today.
Relationships with other healthcare workers and other departments
The data from CDU 1 showed how the nurses’ work was facilitated by their relationships with other healthcare workers and other departments. Data from CDU 2 indicate that the relationships with other departments often impinged on the nurses’ work. Two particular examples have been chosen as they illustrate this well but within the data set there are many examples. It did seem that staff in other departments did not appear to consider the impact of their actions on the work of the unit.
Rose suddenly exclaimed loudly “I swear I am going to scream! The porters picked up the bloods at 9 and they
have still not delivered them to the labs. She telephoned the porters. She was fuming when she came off the
phone. “they have just said “Well the labs usually loose them anyway.

56
It may be that because the workforce was so erratic, relationships were not strong with other departments. There was also a lack of communication from departments to the unit, this may be because of difficulty getting through on the telephone. However this often had major implication for the staff on the unit as this example shows:
I went and sat at the workstation. There seemed to be more people than usual. One lady was looking
perplexed and met my eye. “We have been sent back here from the phlebotomists for our bloods to be taken
here as the waiting time in the lab in 3 hours” I went to talk to the staff. The staff on the unit had not been
informed first, the patients were just sent straight up.
Stress
Without exception all nurses spoke about the amount of stress they encountered in the work. Sources of stress included the work organization and waiting. Nurses reported that it seemed everybody was waiting – patients, nurses, doctors. Nurses reported that the waiting made them feel uncomfortable, as Ellen explains:
I think its because you know what they need..they need to get the chemo and get home. But there’s nothing you
can do. You know you are not giving them what they need. And all the time they are ….”is my chemo ready
yet”. You feel awful. Some patients only have an hour treatment and they are here all day.
Nurses reported that having the patient waiting resulted in them using defensive behaviour and avoiding patients. Nurses is CDU 1 remarked on this aspect of their behaviour before they used the scheduling system. These fieldnotes record what nurses do to cope with waiting and patients watching.
The patients constantly watch the nurses. However, the nurses really only communicate with the patients when
they are ready to treat them. It is as if they concentrate on the task at hand and nothing else. Jill says how
difficult it feels to have everyone waiting “You feel their eyes boring into the back of you. You have to keep
your head down. There’s nothing you can do til everything is ready and you are free.
One aspect of stress from the organization of work not immediately obvious, was that nurses felt they had no control over their work.
You never know where you are. You can never plan anything in advance like going out from work or going on
a course without worrying “will I get out in time; am I leaving everyone in the lurch. Some days there 16
patients and 7 nurses, the next there are 32 and 2, it is really stressful
In addition to the organization of work, the increase in actual workload and numbers of patients to be treated resulted in increased stress for nurses, as Gina indicates:
I find it really hard sometimes and feel overwhelmed there is so much to do. Patients are loosing out, it makes
you feel guilty and frustrated.
Another cause of stress for nurses was the nature of cancer and the patient’s suffering. Its very upsetting sometimes. Look at John, he is so young and such a lovely lad but he is so ill and not doing
very well. I had a patient I was thinking about the other day who was meant to come for treatment and I
wondered where she was. I looked her up on the computer. She was short of breath the last time she was here.
Well she had been admitted and died. That was supposed to be her last treatment.
Nurses also spoke in interviews about their relationships with other staff on the unit. It seemed that one staff member in particular was having an effect on others. As this interview with Rebecca shows:
As soon as she comes in you can feel the atmosphere change. It really stressed me out, just drained me so I
went on annual leave everytime I knew I had to be with her.
Knowledge and education
One of the greatest differences between the units apart from the organization of work, was the education and experience level of the nurses. In CDU 1, all nurses had had formal

57
education concerning chemotherapy administration, supervised practice and also had a lot of experience. In CDU 2 most nurses did not have any formal education concerning chemotherapy. A senior staff nurse explain her experience in her interview:
It wasn’t deemed necessary to have study days but there was a lecturer who visited 2 or 3 times and told us
what to do.
A number of people were worried about the lack of knowledge and experience of the nurses. This remark from a senior staff nurse shows how nurses worried about each others lack of knowledge and skill as this extract from fieldnotes shows:
Kate has very strong concerns about chemotherapy in the Trust. She feels that nurses should be educated
properly about chemotherapy and have a mentor and supervised practice before they give any chemotherapy.
Lack of knowledge, education and experience had an affect on practice in that there were a number of safety issues. One illustration is in the example given previously of a patient going deaf with an increased urea level (4.2.3.2). These also included the fact that nurses did not use infusion pumps to regulate the rate of infusion and often their knowledge deficits were revealed in the advice they gave patients:
There is a phone call from a distressed relative. He was sent home the day before with ambulatory chemo via a
portacath. The infusion was due to finish at 1300hours but has finished at 6am. The patient was feeling very
nauseous. Jill is quite abrupt and tells the woman it’s not a problem that it has run through quicker than it was
meant and have you rung the GP about his nausea?
Time
As with CDU 1 all nurses spoke about how they did not feel they had enough time to spend with patients as patient throughput had increased.
I came into CDU because I wanted patient contact, going through their issues with them, have they got
problems I can help them solve. But now I very very rarely have the time to sit with a patient and talk to them
about their treatment and the wider issues….its like a conveyer belt just giving chemo, hello here you are
goodbye gone.
Environment
Again as with CDU 1 nurses complained about the environment. That it was not designed for chemotherapy administration and that it was depressing to be in. These notes from fieldwork give a first impression:
There are a few windows but they are high up, light is blocked due to surrounding buildings outside. The views
are limited to walls of other buildings. The décor is dull, walls are dirty and hardly any pictures. Lots of
treatment chairs surround the room perimeter but are all over the place with no sense of organization. The
room feels depressing.
However, during the data collection period the unit was redecorated, which occurred whilst patients were still receiving chemotherapy.
The telephone
In CDU 1 the telephone was seen as a very positive contribution which facilitated nurses work in the chemotherapy administration process as the nurses felt they could have an idea of what was happening to patients in between visits and that if patients were worried they could ring straight away without waiting for the next visit. The staff on CDU 2 saw the telephone as one of the factors that impinged on their work as the following quote shows:
The unit, he says has constant telephones ringing, we are always on the phone and not with patients. It drives you mad.
You feel as if you can never get away from people.

58
Conclusion
This chapter has detailed the findings of the ethnographies from the two chemotherapy day units. Though the different areas were observed, analysed and reported separately, it can be seen that the themes that emerged are important to the participants, albeit from different ends of a continuum. As an overview, the findings suggest that the context, work organization, the nursing team, education and experience and staffing levels, all impact on the nurses’ work in chemotherapy day units.
5 Discussion

59
Introduction
Having reported the findings of each component of the study separately, this next section will discuss the findings of both components and interpret them in light of the literature. Implications for practice and recommendations for future research will also be included.
Summary of Findings
Feelings, Attitudes and Beliefs
The findings overall suggest that the nurses in this study have a positive attitude towards their role in the chemotherapy process, but most did not initially embrace this role nor appear to have positive feelings towards it. Many nurses admitted to feeling nervous or frightened when first caring for patients receiving chemotherapy. These initial fears are not dissimilar to newly registered nurses’ reported feelings in Corner and Wilson-Barnett’s (1992) study investigating attitudes towards cancer. In contrast to Corner’s (1993) assertion that professional experiences then continue to have a scaring and negative effect on nurses’ attitudes towards cancer; in this study, experience, gaining more knowledge about chemotherapy and having support from more experienced practitioners appear to have had a positive effect. Equally, most of the respondents in component one disagreed with the statement; chemotherapy does more harm than good unlike those in the study by Elkind (1982). Furthermore, nurses in practice fully appreciated the important role chemotherapy plays within cancer and palliative care. Unlike Fall and Rose’s (1999) qualitative study, which explored nurses’ feelings towards chemotherapy practice, guilt about administering chemotherapy was expressed by very few questionnaire respondents. It maybe in order to avoid feeling guilty nurses are more proactive in preventing and managing side effects now. Though questionnaire results showed nurses felt distressed, when they see patients affected by the chemotherapy they had administered; this was not evident in practice. What is evident is that nurses’ experience and feelings towards chemotherapy practice are likely to be different depending on the context in which they work. Ethnographic findings suggest that the environment and work practices can facilitate nurses’ work in chemotherapy administration which increase their job satisfaction and reduce perceived stress. The findings show nurses perceive that they are comfortable with communicating with patients about chemotherapy. They perceive they have the skills to provide emotional support to patients and their relatives, that resonates with Aratzamendi and Kearney’s (2004) findings where most of participants believed that they did provide psychological care. It may be that because many of the nurses in this study have a wealth of experience of dealing with the emotional consequences of cancer and chemotherapy, providing psychological support does not appear to cause anxiety for these nurses. However, what was clear was that the organisation of care and the environment often adversely effect nurses’ ability to provide the level of psychological support that they would like. The lack of space, time and a private place to be with the patient inhibited nurses’ work in this area. Junior nurses do appear to worry more about the emotional aspect of their role than those of a more senior grade. Interestingly many of this sample identified that they required more education to help them support patients and their relatives with the emotional/psychological consequences of chemotherapy. Many participants reported worries related to patients having adverse reactions to treatment, extravasation and cytotoxic spillage. Although nearly all the respondents

60
reported that they had received education in these areas, it did not seem to lessen these concerns. Verity (2002) also found that nurses worried about these aspects of care however, she concluded that worrying about extravasation and safety issues should be considered a positive, inevitable consequence of administering cytotoxic drugs. Nurses need to be constantly vigilant of these adverse effects, so that, they can either be avoided or effectively managed. However, it is also known that policies and guidelines related to the management of adverse effects such as extravasation are not universally agreed and differ from hospital to hospital (Dougherty, 2005; Holmes, 1997). Confusion about the appropriate management of such events will inevitably lead to increased anxiety for nurses who administer chemotherapy. A positive finding is that few nurses worry about reconstituting cytotoxic drugs, a number of participants stated that this ‘worry’ was not applicable to them as they were not expected to do this anymore in the ward environment. Although confusingly over 50% of those surveyed stated that they would benefit from more education in this area. While many respondents believe that all necessary precautions are taken to ensure that they are not at risk from the hazards of chemotherapy, it is not clear from the findings whether this is because of their own safe practice or from the environment in which they work. However, a number of insightful comments suggest that nurses do have concerns about the long-term risks of exposure to chemotherapy. A number of nurses also worry about the effectiveness of the protective clothing used to administer chemotherapy. The statistical analysis indicated that there are a number of factors, which influence nurses’ worries and attitudes towards chemotherapy practice, these include nursing grade, working in either Cancer Centres or Unit sites, educational level and experience. The finding that factors that affect nurses’ worries are different from those that affect their attitudes is an interesting finding. The overall factor of experience seems to influence nurses attitudes (as depicted by the ordinal regression model) more than education. While, education does appear to have an impact it is difficult to determine the extent from the survey findings. However, in practice it is evident that those who had received more formal education were more competent and confident. The ordinal regression model indicated that worries seem to be influenced by nursing grade. For example, junior nurses worry more about understanding prescriptions/protocols, handling cytotoxic drugs and giving emotional support to patients and relatives. Ethnographic evidence suggests that lack of knowledge, education and experience leads nurses to exhibit more defensive behaviour and makes it more difficult for them to engage and communicate with patients.
The nature and extent of educational preparation
It is apparent that the participants perceive themselves to be educationally equipped to provide information and support to patients, whilst administering chemotherapy. What is clear is that nearly all of the nurses in the survey did not have confidence in their knowledge and skills when they first administered chemotherapy, which is corroborated by interview data. Consequently, they felt nervous or frightened when initially starting this role. Only 27% of the survey sample stated that their pre-registration training had included education about chemotherapy. This finding is consistent with the overall conclusions from Corner and Wilson-Barnett’s (1992) study; where nurses were not adequately prepared to care for cancer patients and as a consequence held negative views about the disease and its treatment. Student nurses need to be made aware of the value of cancer therapy not just in terms of survival but also in terms of the quality of survival that can be achieved. This awareness must also come from clinical experience.

61
Though survey findings indicate that the majority of nurses have had some form of formal education in this practice, this was not corroborated in the ethnographic evidence, which showed that in one chemotherapy day unit none of the nursing staff had received formal education. It is interesting to note that only 27% of the survey sample had been educated to diploma level or above in cancer nursing care. Questions then arise about the quality and standard of education these nurses state that they have received in chemotherapy practice, even though 71% of the sample indicate that the amount of time spent receiving education was over ten hours. Most of the nurses surveyed also thought that receiving more formal education would be beneficial as a means of enhancing their practice. While this study’s intention was not in any way to investigate nurses’ actual knowledge deficits, the results do suggest that there are wide variations in the training and education that this sample has undertaken. Similar to that of Grundy’s (1999) and Verity’s (2002) findings, it appears that many nurses have gained knowledge in practice vicariously in the absence of formal education. Given the potential harmful effects of chemotherapy drugs, this must be cause for concern. Interestingly, 76% of the survey participants were at times worried about colleagues' knowledge and education deficits. What is not clear is if these nurses are worried about the knowledge deficits of staff new to the oncology arena or the staff who have worked in this area for some time. The findings suggest that nurses who are new to the oncology/chemotherapy arena must be given the appropriate education and supervised practice before administering chemotherapy. These findings therefore, are in agreement with the recommendations made by the Joint Council for Clinical Oncology (1994) and Goodman (1998b) that all nurses before they undertake the role of chemotherapy administration must undertake a recognised course and be given the appropriate support. Although the nurses in the present study perceived they were educated and experienced, there was an underlying feeling that nurses are aware that chemotherapy practice is constantly evolving and they need educational support to maintain their knowledge and skills. For example developments in chemotherapy treatments was an area that 94% of the survey sample wanted more education in. Nurses therefore, clearly require continued, ongoing professional development to ensure their knowledge is regularly updated.
The challenges of chemotherapy administration
One of the challenges for nurses is related to time. Being busy on the ward or having staff shortages and lack of trained staff to administer chemotherapy was cited by some, as reasons for when it was inappropriate to handle chemotherapy or when it should not be given at all. Nineteen of the survey respondents wrote that they were very concerned about time pressures, lack of trained staff, patient workload increasing and the subsequent risk of more errors occurring. This finding was substantiated by ethnographic evidence. When considering that many patients who have a cancer diagnosis will have chemotherapy at some stage in their disease trajectory and, given the surprisingly low number of nurses identified in this study who administer chemotherapy in London, this issue of increasing workload is a legitimate cause for concern. It is vital that consideration is given to the recruitment and retention of a competent chemotherapy workforce when it has been identified that a lack of trained staff and time pressures are major causes for chemotherapy and medication administration errors (O’Shea, 1999; Goodman, 1998b). Time pressures were also cited as a reason for concern in six of the sample, who due to lack of time admitted to not being able to support and educate others as well as they would

62
like. Overall, however, the majority of nurses in this study appeared to be well supported either by other colleagues or more senior nursing staff and it is evident that when nurses do have concerns about treatment, they seek support and information. They also appear to be well supported by the medical team and to lesser extent pharmacists. However, for some of the sample administering chemotherapy did cause conflict with doctors, but only when the nurse felt that the patient was too unwell to receive treatment or when other ethical issues arose, such as lack of informed consent. This finding was not influenced by grade or experience. Forty nurses in this study stated that chemotherapy should not be administered at night when there might be a lack of adequate staff and expert support. From both components of the study it is evident that consideration must be given to the organisation of chemotherapy. Ethnographic evidence suggests that organisation of work practices and the nature of relationships, both within the nursing team and with other healthcare professionals, may either facilitate or impinge on chemotherapy nurses work and their ability to give optimum patient care. Though time pressures were shown to be important, findings from the ethnographic component of the study suggested the way time was used was equally important. Work practices that result in large amounts of time wasted in waiting have been found to cause stress for nurses and patients and relatives. Considering the increased workload within chemotherapy day units, it is important to adopt work schedules which reduce waiting times. Chemotherapy scheduling which allows nurses and patients the opportunity to organise their own time has the potential to reduce stress and increase satisfaction with care. The findings show that the environment severely influenced the process of care within the Chemotherapy Day Units. Though nurses did address patients’ psychological needs to a degree, they reported the lack of private space with patients as a barrier to more meaningful assessment of the impact of treatment on the patient’s life. Though many were satisfied with their level of skill in the present system, they also reported a desire for more education and training with protected time for patients to ensure their psychological needs were assessed and met.
Limitations of the study
Component One
A number of limitations should be considered when interpreting the findings of component one. Due to the recruitment of participants from one geographical location in the UK the findings of this study should not be considered as representative of the population as a whole. A low response rate is expected when self-completion, postal questionnaires are used for collecting data; therefore, although the response rate of 49% was a disappointment it was not a surprise. Reasons for non-response have not been obtained and this then means that we know nothing about those who chose not to take part. It raises the question whether the findings are representative of all the population of nurses who administer chemotherapy in London. Although there is a good spread of grades and experience the low response rate does preclude the ability to make clear statistical comparisons on subgroups of the sample, for example to compare responses of junior staff to that of more senior nurses. However, cross-tabulations were performed on all data to identify if there were any emergent trends between the groups (which there were). Seeking permission from twenty-six Research and Development Committees to access the sample was time-consuming and at times problematic. A factor that may have influenced the initial response rate in terms of those agreeing to have a questionnaire sent

63
to them was the utilisation the Lead Cancer Nurse (LCN) as gate-keeper to access the sample in each Trust. Many would have viewed the LCN as their manager and therefore, may have felt obliged to agree to participate. This may also have influenced their responses to the questions giving the expected ‘text-book’ answers rather than their actual feelings and attitudes towards this role. Because of the somewhat low response rate findings and possible implications of this study cannot be generalised and should be viewed with some caution. The tool utilised in this study has not undergone any formal assessment of its reliability and validity and before further use should be subjected to testing. Nevertheless the questionnaire did appear to perform well overall. There was one particular question that yielded responses that were difficult to interpret. This was question 21 related to the clinical area/speciality the respondent worked in. Responses were not clear and therefore, it was difficult to make comparisons between groups. There does appear to be a relationship between different clinical areas and worries and attitudes, for example those that work in haematology areas do worry more about the risk of personal exposure than those who work in general oncology areas. In any future study clinical areas where respondents work need to be determined more clearly. It is also difficult to be certain that the Likert scale used for measuring respondent attitudes produced reliable and valid results. There is the possibility that respondents gave answers that portrayed ideal practice and socially acceptable answers rather than their actual attitudes. Giving the participant time to think about these statements can also bias the responses. Attitudes are known to fluctuate with time, as does their expression (Corner, 1988).
Component Two
A limitation of component two is that, as with any ethnographic research, it represents a reality that each researcher shared with the nurses and patients. The findings are an interpretation of that reality and it is recognised that there may be other possible ways of interpreting it (Davies 1999). Although interpretation of findings has been discussed within the project team and with participants to increase rigor (Erickson and Stull 1998), this fact needs to be considered when reading the report. Equally it needs to be noted that the findings represent a particular setting, in a particular time frame and concerns particular people (Murphy & Dingwall, 2001). It may be that if any one of these elements were changed, it would affect the findings. The findings are, therefore, not generalisable. Both settings involved in the ethnographic component were cancer centres as it was thought this would give greater insight as to the experience of nurses’ work in the Cancer Centre. However, this does mean that the work of chemotherapy nurses in the Cancer Units have not be explored at all.
Implications for Practice and Recommendations
The most important implications from this study concern the preparation of nurses taking on roles within the chemotherapy administration process. The findings indicate a need for core education and skills, clear measurement and indicators of competency and an agreed level of supervision and support. There are future developments currently underway by the National Chemotherapy Advisory Group, as part of the portfolio of work of the Cancer Action Team to explore issues of nursing workforce and skills. Working collaboratively with the Knowledge Skills Framework (Skills for Health 2005) national core competencies for

64
nurses administering chemotherapy have been agreed but these have not yet been published at the time of writing this report. Further work is needed in order to agree models of education in order to disseminate the competencies in practice. As chemotherapy is a dynamic area within cancer care, there needs to be debate as to future mode of practice and direction of chemotherapy services. Once the direction has been debated and agreed, issues such as who delivers the service, in which way, in which location and the nature of the service may be planned together with models of support and supervision for optimum physical and psychological care. The ethnographic component of this study was set in cancer centres, future research, especially observational studies, are needed to explore the process of care within cancer units as well as the cancer centres. It is important to explore whether the delivery of care is different in cancer units. If it is different, the impact of the difference on nurses and patients experience and outcome needs to be identified.
Conclusion
The intention of this study was to explore the process and context of nurses’ administering chemotherapy. Overall, nurses appear to have a positive attitude towards chemotherapy. They realise that chemotherapy is a more involved process than just administering intravenous drugs and have an awareness of the safety issues and consequences of administration. It is evident that nurses must have formal education and support in clinical practice before taking on this role. Experience in this process has positively influenced not only nurses’ attitudes towards chemotherapy but also their interactions with patients and colleagues. However, what both components of this study have clearly highlighted is the impact of the context on nurses’ work. A number of factors were identified as key to facilitating nurses’ work in chemotherapy administration. These include organisation of work, staffing levels and skill mix, educational preparation and supervised practice, pressures of time and workload. The challenge therefore is to provide the educational underpinnings, positive physical environment and effective working practices nurses need in order to achieve optimum care. The nature of the methodology of this study has produced data from a number of different sources. The findings offer a range of insights into nurses’ and patients’ everyday experience of the chemotherapy administration process and contribute to our understanding of the different factors that influence patient care. This is especially important in the light of current policies concerning cancer treatment (DoH 2000; NICE 2004) and future planning and development of services.

65
6 References Aldridge, A., & Levine, K. (2001). Surveying the Social World. Principles and practice in survey research.Buckingham.: Open University Press. Allan, H. (1999). "Sister will see you now" Managing emotions in a Fertility Clinic Unpublished PhD thesis. University of Manchester. Allwood, M., Stanley, A., & Wright, P. (2002). The Cytotoxics Handbook.Oxford: Radcliffe Medical Press. Arantzamendi, M., & Kearney, N. (2004). The psychological needs of patients receiving chemotherapy: an exploration of nurse perceptions. European Journal of Cancer Care, 13(1), 23-31. Barraclough, J. (1994). Cancer and Emotion.Chichester: John Wiley and Sons. Batchelor, D. (2001). Hair and cancer chemotherapy; consequences and nursing care - a literature study. European Journal of Cancer Care, 10, 147-163. Bingham, E. (1985). Hazards to health care workers from antineoplastic drugs. New England Journal of Medicine, 313, 1048-1051. Blay, N., Cairns, J., Chisholm, J., & O'Baugh, J. (2002). Research into the workload and roles of oncology nurses within an outpatient oncology unit. European Journal of Oncology Nursing, 6(1), 6-12. Bremnes, R. (1999). Experience with and attitudes to chemotherapy among newly employed nurses in oncology and surgical departments: A longditudinal study. Supportive Care in
Cancer, 7(1), 11-16. Brown, V., Sitza, J., Richardson, A., Hughes, J., Hannon, H., & Oakley, C. (2001). The development of the Chemotherapy Symptom Assessment Scale (C-SAS): a scale for the routine clinical assessment of the symptom experiences of patients receiving cytotoxic chemotherapy. International Journal of Nursing Studies, 38, 497-510. Brunt, L. (2001). Into the community. In Atkinson P. Coffey A Delamont S Lofland J Lofland L (Eds) Handbook of ethnography.London: Sage Publications. Burns, N., & Grove, S. (2005). The practice of nursing research (5th ed.). Missouri: Elsevier Saunders. Campbell, A. (1984). Nursing, Nurturing and Sexism. In Campbell A (ed), Moderated Love a theology of professional care.London: SPCK. Christensen, J., Lemasters, G., & Wakeman, M. (1990). Work practices and policies of hospital pharmacist preparing antineoplastic agents. Journal of Occupational Medicine, 32(6), 508-512. Coffey, A., & Atkinson, P. (1996). Making Sense of Qualitative Data.London: Sage Publications. Cohen, J. (1992). Statistical power anaylsis for behavioural sciences.London: Academic Press. Coolican, H. (1993). Research Methods and Statistics in Psychology.London: Hodder Stoughton.

66
Corner, J. (1988). Assessment of nurses' attitudes towards cancer: a critical review of research methods. Journal of Advanced Nursing, 13, 640-648. Corner, J., & Wilson-Barnett, J. (1992). The newly registered nurse and the cancer patient: an educational evaluation. International Journal of Nursing Studies, 29(2), 177-190. Corner, J. L. (1993). The impact of nurses' encounters with cancer on their attitudes towards the disease. Journal of Clinical Nursing, 2(6), 363-372. Damrosch, S., Denicoff, A., St. Germain, D., Welsch, C., Blash, J., Jackson, T., et al. (1993). Oncology and physician attitudes towards aggressive chemotherapy treatment. Cancer Nursing, 16(2), 107-112. Darbyshire, P. (1986). Handle with Care. Nursing Times, 37-38. Davidson, F. (1996). Principles of statistical data handling. London: Sage. Davidson, R. (2005). Cancer patients' satisfaction with communication, information and quality of care in a UK region. European Journal of Cancer Care, 14(1), 83-90. Davies, C. (1999). Reflexivity. London: Sage. Delvaux, N., Razavi, D., & Farvacques, C. (1988). Cancer care - A stress for health professionals. Social Science Medicine, 27(2), 159-166. Dennison, S. (1995). An exploration of the communication that takes place between nurses and patients whilst cancer chemotherapy is administered. Journal of Clinical Nursing, 4, 227-233. Dennison, S., & Shute, T. (2000). Identifying patient concerns: Improving the quality of patient visits to the oncology out-patient department - a pilot audit. European Journal of Oncology Nursing, 4(2), 91-98. Department of Health. (2002). The Nursing Contribution to Cancer Care.London: The Stationary Office. Dougherty, L. (1999). Intravenous Cytotoxic Drugs. In Dougherty L. and Lamb J. (eds) Intravenous Therapy in Nursing Practice.Edinburgh: Churchill Livingstone. Elkind, A. (1982). Nurses' views about cancer. Journal of Advanced Nursing, 7, 43-45. Erickson, K., & Stull, D. (1998). Doing Team ethnography.London: Sage Publications. Fall, J., & Rose, L. (1999). Caring for patients who experience chemotherapy - induced side effects: The meaning for oncology nurses. Oncology Nursing Forum, 26(5), 901-907. Fink, A. (2003). The Survey Handbook.London: Sage. Fitzsimmons, D., Hawker, S. E., Johnson, C., Simmonds, P., George, S. L., Middleton, J., et al. (2002). Phase 1 Exploratory Study of a Nurse-specialist managed chemotherapy service. University of Southhampton. Fitzsimmons, D., Hawker, S. E., Simmonds, P., George, S. L., Johnson, C., & Corner, J. L. (2005). Nurse-led models of chemotherapy care: mixed economy or nurse-doctor substitution? Journal of Advanced Nursing, 50(3), 244-252. Glaus, A., Campbell, P., Kearney, N., & Richardson, A. (2000). Leadership and management: influencing the shape of advanced cancer nursing practice. In Kearney N, Richardson A and Di

67
Giulio P. (eds), Cancer Nursing Practice: A Textbook for the Specialist Nurse.London: Churchill Livingstone. Goodman, C. (1985, November 20th). Cytotoxic drugs: their handling and use. Nursing Times, 36-38. Goodman, I. (1998a). The administration of cytotoxic chemotherapy - Recommendations.London: Royal College of Nursing. Goodman, I. (1998b). The administration of cytotoxic chemotherapy - Technical Report.London: Royal College of Nursing. Gregoire, R. E., Segal, R., & Hale, K. M. (1987). Handling antineoplastic drug admixtures at cancer centres: Practices and pharmacists' attitudes. American Journal of Hospital Pharmacy, 44, 1090-1095. Groves, E. L. (2005). Auditing a chemotherapy triage telephone service. Cancer Nursing Practice, 6(25-29). Grundy, M. (1999). Chemotherapy administration by nurses: An Audit of Practice and Educational Preparation.Edinburgh: National Board for Nursing, Midwifery and Health Visiting for Scotland. Harrold, K. (2002). Development of a nurse-led service for patients receiving oral capecitabine. Cancer Nursing Practice, 1(8), 19-24. Hemminki. (1985). Spontaneous abortions and malformations in the offspring of nurses exposed to anaesthetic gases, cytotoxic drugs and other potential hazards. Journal of Epidemiology Community Health, 39, 141-147. Heyl, B. (2001). Ethnographic interviewing. In Atkinson P. Coffey A Delamont S Lofland J Lofland L (Eds) Handbook of ethnography.London: Sage Publications. Holmes, S. (1997). Cancer chemotherapy: A guide for practice.Dorking: Asset Books. Holmes, S., & Eburn, E. (1989). Patients' and nurses' perceptions of symptom distress in cancer. Journal of Advanced Nursing, 14, 840-846. Jacobsen, P., Meade, C., Stein, K., Chirikos, T., Small, B., & Ruckdeschel, J. (2002). Efficacy and costs of two forms of stress management training for cancer patients undergoing chemotherapy. Journal of Clinical Oncology, 20, 2851-2862. Jarret, N. (1996). Confortable conversation:nurse-patient communication in the cancer care context. Unpublished PhD thesis. University of Southampton. Joint Council for Clinical Oncology. (1994). Quality Control in cancer chemotherapy: managerial and procedural aspects.London: Royal College of Physicians and Royal College of Radiologists. Kalter, H. (1986). Antineoplastic drugs and spontaneous abortion in nurses. New England Journal of Medicine, 314, 1173-1178. Kearney, N. (2000). Nursing Education in Cancer Care. In Kearney N, Richardson A and Di Giulio P. (eds), Cancer Nursing Practice: A Textbook for the Specialist Nurse.London: Churchill Livingstone. Kruijver, I., Kerkstra, A., Bensing, J., & Van de Weil, B. (2000). Nurse-patient communication in cancer care: A review of the literature. Cancer Nursing, 23(1), 20-31.

68
Lanceley, A. (1995). Emotional disclosure between cancer patients and nurses. In Richardson A. and Wilson-Barnett J. (eds.) Nursing research in cancer care: Scutari Press. Lee, L. (1993). The risks of handling cytotoxic therapy. Nursing Standard, 7(49), 25-28. Maguire, P. (1985). Barriers to psychological care of the dying. British Medical Journal, 291, 1711-1713. McCaughan, E. M., & Thompson, K. A. (2000). Information needs of cancer patients receiving chemotherapy at a day-case unit in Northern Ireland. Journal of Clinical Nursing, 9, 851-858. Mccoll, E., Jacoby, A., Thomas, L., Soutter, J., Bamford, C., Steen, N., et al. (2001). Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients. Health Technology Assessment, 5(31). McCray, N. D. (1997). Psychosocial and quality of life issues. In Otto, S. Oncology Nursing.St. Louis: Mosby. Miller, M., Kearney, N., & Smith, K. (2000). Measurement of cancer attitudes: a review. European Journal of Oncology Nursing, 4(4), 233-245. Miller, S. (1987). Issues in cytotoxic drug handling safety. Seminars in Oncology Nursing, 3(2), 133-141. Mohan, S., Wilkes, L. M., & Walker, A. (2005). Caring for patients with cancer in non-specialist wards: the nurse experience. European Journal of Cancer Care, 14, 256-263. Moore, L., & Savage, J. (2002). Participant observation, informed consent and ethical approval. Nurse Researcher, 9(4), 58-69. Mun, L. Y., Ping, C. M., Fai, W. K., Molassiotis, A., Ki, Y. T., & Jing, C. S. (2001). An evaluation of the quality of a chemotherapy administration service established by nurses in an oncology day care centre. 5(4), 244-253. Munro, A. (2005). Decision making in cancer care. In Kearney N and Richardson A (eds) Nursing Patients with Cancer, Principles and Practice.Edinburgh.: Elsevier Churchill Livingstone. Murphy, E., & Dingwall, R. (2001). The ethics of ethnography. In Atkinson, P Coffey A. Delamont S. Lofland J and Lofland L (Eds) Handbook of ethnography.London: Sage Publications. Nygren, O., & Lundgren, C. (1997). Determination of platinum in workroom air and in blood and urine from nursing staff attending patients receiving cisplatin chemotherapy. International Archives Occupational and Environmental Health, 70(3), 209-214. O'Shea, E. (1999). Factors contributing to medication errors: a literature review. Journal of Clinical Nursing, 8, 496-504. Purandare, L. (1997). Attitudes to cancer may create a barrier to communication between the patient and caregiver. European Journal of Cancer Care, 6, 92-99. Richardson, A. (1996). The Royal Marsden Hospital - Manual of core care plans for cancer nursing.London: Balliere Tindall. Richardson, J. L., Marks, G., & Levine, A. (1998). The influence of symptoms of disease and side-effects of treatment on compliance with cancer therapy. Journal of Clinical Oncology, 6, 1746-1751.

69
Savage, J. (1995). Nursaing Intimacy. An ethnographic approach to nurse-patient interaction.Harrow: Scutari Projects Ltd. Savage, J. (2000). Ethnography and healthcare. British Medical Journal, 321, 1400-1402. Schlmeister, L. (1999). Chemotherapy medication errors: Descriptions, severity and contributing factors. Oncology Nursing Forum, 26(6), 1033-1042. Selvey, D. (1985a). Cytotoxic drugs: their handling and their use. Nursing Times, 36-38. Selvey, D. (1985b). Cabinet security. Nursing Times, 39. Sessink, P., Boer, K., Scheefhals, A., Anzion, R., & Bos, R. (1992). Occupational exposure to antineoplastic agents at several departments in a hospital. International Archives of Occupational and Environmental Health., 64, 105-112. Sims, J. (2005). Risk Management, In Brighton D and Wood M (eds) The Royal Marsden Hospital Handbook of Cancer Chemotherapy.Edinburgh: Elsevier Churchill Livingstone. Sitza, J., & Wood, N. (1998a). Patient satisfaction with cancer chemotherapy nursing: a review of the literature. International Journal of Nursing Studies, 35, 1-12. Sitza, J., & Wood, N. (1998b). Study of patient satisfaction with chemotherapy nursing care. European Journal of Oncology Nursing, 2(3), 142-153. Skills for Health. (2005).http://www.skillsforhealth.org.uk. Slevin, M. L., Stubbs, L., Plant, H. J., Wilson, P., Gregory, W. M., Armes, P., et al. (1990). Attitudes to chemotherapy: comparing views of patients with cancer with those of doctors, nurses, and general public. British Medical Journal., 300, 1458- 1460. Soothill, K., Morris, S., & Thomas, C. (2003). The universal, situational, and personal needs of cancer patients and their main carers. European Journal of Oncology Nursing, 7(1), 5-16. Tanghe, A., Paridaens, R., Evers, G., Vantogelen, K., Aerts, R., Lejeune, M., et al. (1996). Case study of quality assurance in the administration of chemotherapy. Cancer Nursing, 19(6), 447-454. Tanghe, A., Vantongelen, K., Paridaens, R., Van De Schueren, E., Aerts, R., Lejeune, M., et al. (1994). Role of nurses in cancer chemotherapy administration. Retrospective record analysis to improve role performance. European Journal. of Cancer Care, 3, 169-174. Taylor, L., & Birch, J. (2004). Chemotherapy support worker role - a one year pilot. Cancer Nursing Practice, 3(10), 23-27. Valanis, B., & Browne, M. (1985). Use of Protection by Nurses during Occupational Handling of Antineoplastic Drugs. National Intravenous Therapy Association, 8, 218-223. Valanis, B., Vollmer, W., Labuhn, K., & Glass, A. (1997). Occupational Exposure to Antineoplastic Agents and Self-reported Infertility among Nurses and Pharmacists. Journal of Occupation Environmental Medicine, 39(6), 574-580. Verity, R. (2002). Administering Cytotoxic Chemotherapy: The Nurse's Perspective:Unpublished MSc Dissertation, University of Surrey. Verity, R., & Bloomfield, J. (2005). Mastering Chemotherapy. Cancer Nursing Practice, 4(3), 14. Wallis, M., & Tyson, S. (2003). Improving the Nursing Management of Patients in a Haematology/Oncology Day Unit: An Action Research Project. Cancer Nursing, 26(1), 75-82. Wherney-Tedder, M. (1997). A positive approach to chemotherapy. Nursing Times, 93(23), 52-53.

70
Wilkinson, S. (1990). Nursing patients with cancer: satisfaction and stresses. In Faulkner A. (ed.) Oncology, excellence in nursing, the research route.London: Scutari press. Wilkinson, S. (1991). Factors which influence how nurses communicate with cancer patients. Journal of Advanced Nursing, 16, 677-688. Wiseman, T. (2002). An ethnographic study of empathy in clinical practice. Unpublished PhD thesis. University of Manchester. Wolcott, H. (1999). Ethnography - a way of seeing.California: Alta Mira Press. Wood, M., Hyde, L., & Salter, M. (2005). Management of the adult patient with cancer receiving chemotherapy. In Brighton D and Wood M (eds) The Royal Marsden Hospital Handbook of Cancer Chemotherapy.Edinburgh: Elsevier Churchill Livingstone.
71
7 Appendices Appendix 1 Appendix 2 Appendix 3 Appendix 4 Appendix 5 Appendix 6
Questionnaire Revisions to Questions Questions Added Information for Lead Cancer Nurses Cover letter to participants Nurse Information Sheet

I
Appendix 1: Questionnaire To be added manually

II
Appendix 2: Revisions to Questions Original Question Revision
Looking back do you feel the amount of teaching
you received was adequate?
Yes �
No �
Uncertain �
Q7. How adequate was the amount of teaching you
received on chemotherapy in pre-registration training?
Comprehensive �
Adequate �
Uncertain �
Inadequate �
Are there times when you think it is not
appropriate to handle chemotherapy?
Yes �
No �
Uncertain �
Q17. Are there times when you think it is NOT safe to
administer/handle chemotherapy?
Never �
Occasionally �
Often �
Always �
Have there been times when you didn’t want to
administer chemotherapy to a patient?
Yes �
No �
Q18. Have there been times when you didn’t want to
administer chemotherapy to a patient?
Never �
Occasionally �
Often �
Always �
Do any of the following WORRY you with regards
to your chemotherapy role?
Yes �
No �
Sometimes �
Q19. How often do you WORRY with regards to the
following aspects of your chemotherapy role?
Never �
Occasionally �
Often �
Always �
The next set of questions ask about YOUR
ATTITUDES to how YOU FEEL about your role
in administering chemotherapy
Strongly agree �
Agree �
Uncertain �
Disagree �
Strongly Disagree �
Q20. The next set of questions ask about YOUR
ATTITUDES to how YOU FEEL about your role in
administering chemotherapy
Strongly agree �
Agree �
Disagree �
Strongly Disagree �
Question relating to attitudes – split into two
Administering chemotherapy is a satisfying and
challenging part of my role
Question 20
Q20.t. Administering/handling chemotherapy is a
satisfying part of my role
Q20.u. Administering/handling chemotherapy is a
challenging part of my role.

III
Appendix 3: Questions Added 2. In which clinical area do you administer chemotherapy? (please tick all that apply)
Outpatients �
Ward �
Community �
Other �
Q6. Have you received formal education in any of the following?
(question l. added onto list)
Ql. – Appropriate use of pumps/equipment
Yes � No � Unsure �
Q9. Would you benefit from more education/information in any of the following?
(question l. added onto list)
Ql. - Appropriate use of pumps/equipment
Yes � No � Unsure �
Q20. The next set of questions ask about YOUR ATTITUDES to how you feel about
your role in administering/handling chemotherapy
(questions e, d, o, were added onto list of attitude statements)
Q20.
e Chemotherapy causes more harm than good
d. When presented with emergencies caused by chemotherapy I do NOT feel
confident in my competency
o. I focus entirely on the practical aspects of the task when giving/handling
chemotherapy

IV
Appendix 4: Information for Lead Cancer Nurses
Florence Nightingale
School of Nursing
and Midwifery
Professor Alison Richardson Chair of Cancer and Palliative Nursing Care Tel 020 7848 3503 Fax 020 7848 3506
Dear Colleague
Re: Exploring the work of nurses who administer chemotherapy
As you may already be aware, the Florence Nightingale School of Nursing and Midwifery at King’s College London (in collaboration with the South East London Cancer Network Nursing Research and Development Group) have been awarded a grant from the European Oncology Nursing Society to explore the work of nurses who administer chemotherapy. The purpose of this project is to gain knowledge of nurses’ beliefs, knowledge and attitudes towards chemotherapy administration, in order to enhance practice and develop educational programmes. The study aims to include all nurses who administer chemotherapy in hospitals throughout the London Cancer Networks. In order to ensure that all nurses who administer chemotherapy have the opportunity to be included in this study we need your help to compile a list of the nurses who fulfil the eligibility criteria to whom we can then send a questionnaire. However, to fulfil the requirements of the Data Protection Act we would like you, if possible, to give the attached letter to all nurses in permanent positions who currently administer chemotherapy in your Trust. This letter asks them to let you know if they do not wish their name to be forwarded to the research team. Following this exercise we ask that you compile a list of nurses’ names along with the department where they work so we might forward them information about the study along with a questionnaire. This study has been given ethical approval from an NHS Multi Research Ethics Committee, Project Number 04/Q0603/51. Permission has also been sought from your Trust’s Research and Development Committee to involve nurses in this study. We realise this will create extra work for you but hope, like us, you can see that the information this study will provide will help to better understand the concerns of this group of nurses and inform future education, training and support initiatives. If you would like to discuss this study and your involvement, Rebecca Verity, Lecturer in Nursing at King’s and a member of the research team, would be happy to meet you on an individual basis. Rebecca may be contacted via email: [email protected] or by phone 020 7848 3671. If you are willing to help us with this research please could you kindly email Rebecca to confirm this as soon as possible. Your contribution to this study will be greatly appreciated. We look forward to hearing from you. Yours sincerely Professor Alison Richardson Professor of Cancer and Palliative Nursing Care Chief Investigator

V
Appendix 5: Cover letter to participants
Florence Nightingale
School of Nursing
and Midwifery
Professor Alison Richardson Chair of Cancer and Palliative Nursing Care Tel 020 7848 3503 Fax 020 7848 3506
Dear Colleague
Exploring the work of nurses who administer chemotherapy The Florence Nightingale School of Nursing and Midwifery at King’s College London have been awarded a grant from the European Oncology Nursing Society to explore the work of nurses who administer chemotherapy. The purpose of this project is to gain knowledge of nurses’ beliefs, knowledge and attitudes towards chemotherapy administration in order to enhance practice and develop educational programmes. The study aims to include all nurses who administer chemotherapy in hospitals throughout the London Cancer Networks.
We would like you to consider taking part in this study. It will involve you completing a questionnaire that we will send to you via your hospital address. In order to give an opportunity to all the nurses in the London Cancer Networks to participate, we have asked the Lead Nurses of each cancer network to forward us the names of all nurses who administer chemotherapy in the hospitals/trusts within their particular network. If you do not want your name forwarded to the research team so that we can send you further information and a questionnaire, please return the “tear off” slip to your Manager/Lead Nurse.
Please be assured that the research team will not use your name for any other purpose and will not forward you any other material other than the questionnaire. Thank you for your time. Yours faithfully Professor Alison Richardson Chief Investigator
………………………………………………………………………………………………………………… To <<insert the name of the Lead Nurse for the Network >> I do not wish my name to be forwarded to the Research Team at Kings College London in connection with the study entitled “Exploring the work of nurses who administer chemotherapy”. Please return this by: <<insert date>> My Name:………………………………………………………………………………………………….. My signature………………………………………………………………………………………………

VI
Appendix 6: Nurse Information Sheet
NURSE INFORMATION SHEET
Study title: Exploring the work of nurses who administer chemotherapy
You are being invited to take part in a research study. Before you decide it is important for you to
understand why the research is being done and what it will involve. Please take time to read the
following information carefully and discuss it with others if you wish. Take time to decide whether
or not you wish to take part.
Thank you for reading this.
What is the purpose of the study? The study aims to:
To determine the knowledge, attitudes and beliefs of nurses who administer chemotherapy
Explore how nurses’ view their role in the process of chemotherapy administration.
To ascertain the nature and extent of educational preparation that nurses who administer
chemotherapy have received
To determine whether nurses who administer chemotherapy think this educational preparation is
sufficient.
Why have I been chosen?
This study will include up to 450 trained nurses who are administering chemotherapy in the
hospitals/trusts within the 5 Cancer Networks in London. Lead Nurses have been requested to
provide contact details for all nurses working in their trusts. To take part individuals have to be:
Registered general nurses
Employed by the trust
Administering chemotherapy to patients in one of the London Cancer Networks
Do I have to take part?
It is up to you whether or not to take part. This information sheet tells you all about the study and
will help you decide. If you do decide to take part, please complete the enclosed questionnaire and
return it to me in the next 4 weeks. Please post the completed questionnaire in the stamped
addressed envelope enclosed. If you do decide to take part, it is important that you know you can
withdraw at any time by contacting the research team up to the point when the data are analysed.
You do not have to give a reason for this.
What will happen to me if I take part? Around 450 nurses are being invited to take part in this study. Each person will be sent a
questionnaire. Your involvement will last the time it takes to complete the questionnaire
(approximately 30 minutes). By filling in the questionnaire, you will be confirming that you are
happy to take part in the research. However, as stated earlier you are free to withdraw at any time.
What do I have to do? Through taking part you will be asked to fill in a questionnaire and post it back to the research team
in the envelope provided.
What is being researched? We are exploring the knowledge, beliefs and attitudes of nurses who administer chemotherapy. The
information gained from the study will help to enhance practice and develop education
programmes.
What are the possible disadvantages of taking part?

VII
The questionnaire may take up to half an hour to complete. So there will be costs in terms of your
time. For the questionnaire you will need to think about your practice and management of patients
with cancer having chemotherapy. These questions are not intended to be upsetting, but may raise
issues for you.
What are the possible benefits of taking part? Through taking part you will help the London Cancer Networks to find out how best to provide
education and support to nurses providing care to patients having chemotherapy. Whilst this may
not directly benefit you, the information we get from this study may help us shape future education
and support services.
What happens when the research study stops?
Your usual working life will continue both during the study and after it is completed. Once the
study is complete you will not be requested for further information.
What if something goes wrong? The chief investigator is indemnified through the general Kings College London Liability
Insurance, with the principle of “No Fault” compensation in operation for subjects of clinical
research.
Will my taking part in this study be confidential? All responses you give will be confidential. Any information about you, which you provide, will
have your name and work address removed so that you cannot be recognised from it. You will be
identified solely by an identification number on the questionnaire. All study information will be
stored in accordance with the Data Protection Act (1998) in a locked filing cabinet to which only
the researchers will have access.
What will happen to the results of this study? The researchers will work with the London Cancer Networks to determine how best to disseminate
the findings from this research. Feedback will be provided to each of the Cancer Networks where
data has been collected. The researchers will also present findings at the European Oncology
Nursing Society (EONS) conference and publish findings in selected journals. Findings may also be
posted on the Kings College London website.
Who is organising and funding the research?
The research is being funded by the EONS Roche grant 2004 and conducted by researchers based at
the Florence Nightingale School of Nursing and Midwifery at King’s College London University.
The research is being monitored and overseen by a Steering Group who will advise on its conduct.
This Steering Group is made up of healthcare experts.
Who has reviewed this study? The South East London Cancer Network Research and Development group have reviewed and
commented on the study. The study has also been reviewed by the EONS grant review group and a
Multisite Research Ethics Committee.
Contact for further information
Ms Rebecca Verity
Lecturer in Cancer and Palliative Care
James Clerk Maxwell Building
57 Waterloo Road
London SE1 8WA
Email: [email protected] Direct telephone line: 020 7848 3671