med monthly june 2012
DESCRIPTION
The innovative medicine issue of Med Monthly MagazineTRANSCRIPT

Med Monthly the
innovative
medicine issue
GAME CHANGER
Say "Hello" to heart surgery's new transformation
CONCIERGE MEDICINEAre you available for the right price?
ALSOINNOVATING
OURSELVESEmbracing technology
resources for your practice
JUNE 2012
LEVERAGING THE CLOUDUsing technology for real results

contents
34 CONCIERGE MEDICINEThe doctor is always in for the right price
40 PATIENT BULLYINGDamaging behavior among doctors and patients
42 LEVERAGING THE CLOUD FOR REAL RESULTSUsing technology resources in your practice
44 INNOVATING OURSELVESThe move toward a better future begins with you
research and technology
10 eDEVICE ANNOUNCES HEALTHGO MONITOR
12 A GAME CHANGER FOR OPEN HEART SURGERYHow cardiologists are bypassing invasive surgery
16 UNC CDTR COLLABORATION FOR DIABETES
practice tips18 HIDDEN ADVANTAGES OF ONLINE REVIEWS20 TRANSITIONING FROM VOLUME TO VALUE22 ANSWERING SERVICES IMPROVE EXPERIENCES
legal26 BEST PRACTICES FOR PHI BREACHES 30 STRIKE FORCES MEDICARE FRAUD CHARGES
the arts48 BRIDGING THE GAP the kitchen51 LEMON BERRY SLUSHY
features
in every issue
4 editor’s letter8 news briefs
58 resource guide74 top 9 list
COVER PHOTO COURTESY ISTOCKPHOTO
48
34Concierge Medicine
Bridging the Gap

P.O. Box 98313, Raleigh, NC 27624
phone: 919.845.0054 fax: 919.845.1947e-mail: [email protected]
www.physiciansolutions.com
Physician Solutions MD STAFFING Locum tenens Permanent placement
When your physician can’t work tomorrow do you have a plan B?
With an extensive network of health care providers and over 20 years of ex-perience in physician staffing, Physi-cian Solutions is a leader in the indus-try. We specialize in primary care and place doctors in facilities such as famil-ly practices, urgent cares, pediatrics of-fices and occupational health.
Short-term or long-term, Physician Solutions has you covered
Scan this QR code with your smartphone to learn more.

Managing Editor
Leigh Ann Simpson
4 | JUNE 2012
editor’s letter
Innovation has been the cornerstone of health care for as long as hu-man beings have existed. Each generation has brought new scientific understanding and technological breakthroughs that have revolutionized the way we care for the sick and the injured. The pace of medical discov-ery has always been very rapid; however the 21st century has pushed this speed into overdrive. The results of this accelerated progression are re-markable; we’ve saved and improved the quality of life for millions. How-ever, as our level of knowledge continues to sky rocket, so does the cost of treating patients, especially here in the U.S. Fortunately, the country as a whole has recognized this tremendous problem and is now addressing the growing concern. Today health care professionals, government officials and other opinion leaders are innovating health care beyond the research lab and searching for more efficient and cost-effective, quality care.
Technology is being utilized in the administrative side of medicine today just as much as it is being used in clinical care. Physicians and administrators everywhere are finding great success using technology to streamline operations and attract more patients, and if you haven’t jumped on this bandwagon by now, you will likely be left behind. Amanda Kanaan explains how some doctors are taking a new perspective on the dreaded online patient review, and leveraging it to actually boost their internet visibility. Mary Pat Whaley shows us how medical practices and health systems are utilizing “the Cloud” to achieve greater financial success and save money in your practice. This issue is packed with clinical trial results, collaboration projects, and product launch announcements that are begin-ning to change the practice of medicine as we know it – for the better. All of these innovations have the potential to bring even greater achievement to those working in the health care profession, but there is still one very large obstacle that we must first overcome and that is innovating our-selves. Robert Tennant, our health IT solutions expert, points out a valid and very real-world argument that our progress will never happen unless we allow it.
Med Monthly also celebrates innovation this month as we welcome our new Creative Director, Bethany Houston. We are looking forward to the new heights that the magazine will take guided by her talent and creativ-ity. I’m very excited about our future collaborations to bring you even better coverage of the most essential medical news to keep you successful. I would also like to invite any of our forward-thinking readers in health care today to send us information or articles on how you are making a difference. As always, thank you for your continued support. I hope you enjoy our June issue.
Sincerely,
Greetings Medical Professionals!

Med Monthly
Publisher
Managing Editor
Creative Director
Marketing & Advertising
Contributors
Philip Driver
Leigh Ann Simpson
Bethany Houston
Jenna Cameron
Robert TennantLisa Shock, MHS, PA-CMary Pat Whaley, FACMPE Taylor ArnoldAshley Acornley, MS, RD, LDNElizabeth WitherspoonPaula RappMike CynarMichael FreudmanAmanda KanaanFrank J. Rosello
Med Monthly is a national monthly magazine committed to providing
insights about the health care profession, current events, what’s
working and what’s not in the health care industry, as well as practical
advice for physicians and practices. We are currently accepting articles to
be considered for publication. For more information on writing for Med Monthly,
check out our writer’s guidelines at medmonthly.com/writers-guidelines
June 2012
P.O. Box 99488Raleigh, NC 27624
Online 24/7 at medmonthly.com
MEDMONTHLY.COM |5
Amanda Kanaan is the owner/founder of WhiteCoat Designs – an online marketing agency committed to growing doctors’ prac-tices through cost-effective and power-ful online marketing solutions. Amanda regularly speaks at medical association meetings and conventions and is a published expert in the field of medical marketing. To learn more or for a free
website evaluation, contact her at [email protected] or www.whitecoat-designs.com
Paula Rapp is a strong activist and promoter of patients’ rights and advocacy issues. Paula established Green Pear Health in 2010 after recognizing that a vast majority of patients lack basic em-powerment tools and the requisite communication skills that can lead to healthier and more rewarding medical outcomes.
contributors
Ashley Acornley, RD, LDNholds a BS in Nutritional Sciences with a minor in Kinesiology from Penn State University. She com-pleted her Dietetic Internship at Meredith College and recently completed her Master’s Degree in Nutrition. She is also an AFAA certi-fied personal trainer. Her blog can
be found at: ashleyfreshfromthefarm.wordpress.com
Mary Pat Whaley, FACMPE is board certified in health care management and a Fellow in the American College of Medical Practice Executives. She has worked in health care and health care management for 25 years. She can be contacted at [email protected]
Lisa P. Shock, MHS, PA-Cis a PA who has practiced in primary care and geriatrics. She enjoys part-time clinical practice and is the President and CEO of Utilization Solutions in Healthcare – a specialty consultant company for physician practices and hospitals, offering services to help implement and im-prove the utilization of PAs and NPs
in the health care system. Contact her with questions at [email protected]

THINKING ABOUT SELLING YOUR PRACTICE?
Medical Practice Listings can help you sell your practice online!
919.848.4202 | medicalpracticelistings.com
The Standard Listing offers you the opportunity to gain national exposure by posting your listing on our website which is viewed daily by our network of professionals. This option also includes a brief practice consultation to explain the benefits of marketing through the Medical Practice Listings website.
In addtion to the benefits in the standard listing our Professional Listing affords you access to services provided by our expert legal and marketing team and a Bizscore Practice Valuation. This valuation compares your practice with other practices in your area, provides projections and determines what your practice is worth.
Now offering two types of listings to better serve all practice specialties and budgets.
Standard Listing Professional Listing
Visit us today at www.medicalpracticelistings.com to learn more.

American Council on Exercise®
4 8 5 1 P A R A M O U N T D R I V E , S A N D I E G O , C A 9 2 1 2 3 U S A
( 8 0 0 ) 8 2 5 - 3 6 3 6 X 6 5 3 | W W W . A C E F I T N E S S . O R G
A Public Service Message brought to you by the American Council on Exercise,
a not-for-profit organization committed to the promotion of safe and effective exercise
A M E R I C A ’ S A U T H O R I T Y O N F I T N E S STM
ACE Certified: The Mark of QualityLook for the ACE symbol of excellence
in fitness training and education.For more information, visit our website:
www.ACEfitness.org
Kids spend several hours a day playing video games and
less than 15 minutes in P.E. Most can’t do two push-ups.
Many are obese, and nearly half exhibit risk factors of
heart disease. The American Council on Exercise and
major medical organizations consider this situation a
national health risk. Continuing budget cutbacks have
forced many schools to drop P.E.—in fact, 49 states no
longer even require it daily.
You can help. Dust off that bike. Get out the skates.
Swim with your kids. Play catch. Show them exercise is
fun and promotes a long, healthy life. And call ACE. Find
out more on how you can get these young engines fired
up. Then maybe the video games will get dusty.
Unfortunately, its motor is inside playing video games.

8 | JUNE 2012
news briefs
Cohera Treats First Patient Using TissuGlu Surgical Adhesive
Cohera Medical announced that the first patient has been treated in a U.S. prospective multicentre randomized clinical trial of its TissuGlu surgical adhesive.
The TissuGlu surgical adhesive is an internal, lysine-derived urethane adhesive which serves the needs of plastic and aesthetic surgeons who perform abdominoplasty and other procedures that require the creation of large planar flaps of tissue. The chemical composition of the adhesive is resorbable, non-toxic and it forms a strong bond between tissue layers and allows for natural healing, which could ultimately enable faster recovery.
In the study, the effectiveness of TissuGlu on the reduction of wound drainage and post-surgical complications in abdominoplasty surgeries will be evaluated in 150 patients at six sites in the U.S. The surgical adhesive, which helps to eliminate or reduce fluid ac-cumulation and the need for post surgical drains, has been used successfully in over 350 surgical procedures in Germany.
Cohera Medical president and chief execu-tive officer Patrick Daly said: "We are hon-ored to be working with such a distinguished group of surgeons who share our vision for excellent clinical outcomes. We look forward to working with the United States Food and Drug Administration (FDA) to bring this breakthrough technology to patients and clinicians here in the United States."
Cleveland Clinic Innovation Collaboration
The Cleveland Clinic is pairing with New York's North Shore-Long Island Jewish Health System (North Shore-LIJ) to share its expertise in developing and marketing medical in-novations.
The deal, the value of which is not being disclosed, is the second such collaboration the Clinic has formed and pos-sibly the beginning of a "national innovation alliance," said Chris Coburn, executive director of Cleveland Clinic Inno-vations. "These providers are working together based on competencies and not on geographic proximity," Coburn said. The goal is for North Shore-LIJ, a 15-hospital system that has more than 200 facilities across the New York area, to gain expertise in how to turn ideas into marketable inven-tions just as the Clinic has.
Last year, the Clinic formed a collaboration with MedStar Health – a 9-hospital system that serves Maryland and the Washington, D.C. area. The Clinic placed two people on site at MedStar, and that system has since reported more than 100 new inventions, Coburn said. North Shore could have two to four Clinic staff members on site, according to Clinic officials.
Coburn said the collaboration also will mean that North Shore, MedStar and the Clinic work together, sharing ideas and sharpening innovations. Long-term, the partnership also could bring together doctors and other employees to solve medical problems, improve treatment and advance medical education. Since its founding in 2000, the Clinic In-novations had reported 35 active spin-off companies, ac-cording to the Clinic. This year, Global Corporate Ventur-ing magazine named Clinic Innovations among the top five most influential health care corporate venturing division in the world.Courtsey Cohera Medical Inc.

MEDMONTHLY.COM |9
Affordable Care Act Saved People on Medicare Over $3.4 Billion on Prescription Drugs
Thanks to the Affordable Care Act, seniors and people with disabilities on Medicare have saved a total of $3.4 billion on prescription drugs. The Cen-ters for Medicare & Medicaid Services (CMS) released data showing that, in the first three months of 2012 alone, more than 220,000 people saved an average of $837 on the pre-scription drugs they purchased after they hit the prescription drug donut hole, for a total of $184.5 million in savings.
In addition, CMS announced that from January through March 8.9 million people on traditional Medicare received at least one preventive service at no cost to them – including over 560,000 who have taken advantage of the new Annual Wellness Visit. Prior to 2011, peo-ple on Medicare faced cost-sharing for many preventive benefits like cancer screenings and smoking cessation coun-seling. Now, these benefits are offered free of charge to ben-eficiaries, with no deductible or co-pay.
“The Affordable Care Act is helping millions on Medi-care save billions of dollars on care and prescription drugs,” said CMS Acting Administrator Marilyn Tavenner. The Afford-able Care Act gives people on Medicare the relief they need from medical costs and more resources to stay healthy.”
New Zealand Lauded for Model Health IT Solutions
During a ConhIT Workshop of the European Health Telematics Association (EH-TEL), the New Zealand perspective was outlined by Chai Chuah, national director of New Zealand’s Ministry of Health. “New Zealand’s geography and population structure were a good driver to develop new care concepts that integrate innovative health care IT solutions,” Chuah said. “New Zealand is striving towards a sustain-able improvement of its health care system. We have realized that a cost-effective increase in quality of care is only possible when we apply new concepts.”
Per capita health care spending in New Zealand is lower than in many other industrial countries. According to the Organization for Economic Cooperation and Development (OECD) figures, people in New Zealand spend on average U.S.-$ 2,983 on health care. This compares with Germany at U.S.-$ 4,348 per capita, while France is also close to U.S.-$ 4,000. And the U.S. tops all others with U.S.-$ 7,960.
These big differences might at least partly be explained by a far more comprehen-sive implementation of health care IT solutions. This, according to Chuah, was dem-onstrated time and again by international comparisons. For example, 97 percent of doctors in private practice routinely send re-
minders concerning prevention and follow-up care measures. Another 97 percent
of doctors say that they use electronic patient records. And 99 percent of
pharmacies are computerized.Currently, New Zealand is focus-
ing on electronic online commu-nication between different medical institutions. Nationwide electronic
referrals are in the pipeline. Hospi-tals are on the verge of being granted
digital access to electronic patient records of primary care physicians in
emergency situations. A summary of recent healthcare IT development
in New Zealand can be downloaded at www.newzealand.com/business
COMING SOON
IN MED MONTHLY
In the July 2012 issue, Med
Monthly investigates the
transition of specialized
internal medicine to a
broader spectrum.

research & technology
10 | JUNE 2012
eDevice Announces HealthGO MonitorThe industry's first fully customizable technology platform for remote patient monitoring
By Michael Freudman
EDevice recently introduced HealthGO, a complete technol-ogy platform for Remote Patient Monitoring based on Freescale
Semiconductor’s Home Health Hub (HHH) reference platform.
“eDevice is providing the remote monitoring market a standard, flex-ible and affordable platform to fulfill patients’ needs. Together with our experience in embedded, sensing, and wireless technologies and eDevices market expertise, we will help improve the lives of patients worldwide”
HealthGO is a remote patient moni-toring technology platform designed for medical device and health care monitoring companies seeking to quickly roll‐out an end‐to‐end innova-tive, customized and reliable solution. HealthGO‐based telehealth solutions increase patient quality of life and quality of care through accurate and focused medical home‐based monitor-ing.
The need for connected health care is growing and the increase in life expectancy, the cost of the chronic diseases and the finan-cial pressure on the health care system will further accelerate this growth. At the end of 2011, according to Berg Insight, only 2.2 million patients worldwide were using a home monitoring service based on equipment with integrated connectivity, while more than 200 million people in the
European Union and the United States suffer from one or several diseases where home monitoring can become a treatment option. The number of home monitoring systems with cellular connectivity integrated is projected to grow at a compound annual growth rate (CAGR) of 34.6 percent during the next five years.
With the HHH and its team of application specific experts, eDevice has built a range of “universal medi-cal gateways.” The HealthGO will be branded and marketed by home moni-toring companies, whose quality and regulatory constraints are very impor-tant. Internally specifying, designing, developing and testing the hardware
products would drain an important part of their financial resources and skilled staff. eDevice allows them to focus on their core business and offers the possibility to launch a complete so-lution without going through the long, expensive and risky process of creating a new monitor.
The HealthGO monitors are com-plete and customizable. They come with vital sign monitoring, USB and Bluetooth peripheral interfaces, embedded blood pressure monitor (optional on HealthGO+), touch‐screen, embedded microphone and speaker, disease management possibili-ties, capability to display information, messages, weather and heath education
Courtesy of eDevice

tutorials. Both the firmware and the hardware of the HealthGO are cus-tomizable by the client. An application programming interface (API) is avail-able for in‐house development of the client applications and graphical user interface and the casing can be modi-fied to fit client requirements.
The HealthGo is part of eDevice’s complete remote monitoring offer, which also includes worldwide cel-lular connectivity and services & logistics portal. “With the Freescale HHH reference platform, we created a solution designed to securely connect millions of patients to their caregivers. We will now offer the only customiz-able technology platform for remote patient monitoring. We are proud to partner with Freescale because they are committed to help people live a better
life by driving innovation and enabling medical device manufacturers to lever-age the latest technology available to use for their products,” said Marc Ber-rebi, CEO of eDevice.
“eDevice is providing the remote monitoring market a standard, flex-ible and affordable platform to fulfill
patients’ needs. Together with our experience in embedded, sensing, and wireless technologies and eDevices market expertise, we will help improve the lives of patients worldwide,” said Steven Dean, Freescale’s Director of Medical Marketing.
Job: ADC-ART-M84812BDocument name: 1G66354_ADC_b2.1_crc.indd
Description: Walking Magazine AdbleeD: None
trim: 7” x 4.625”safety: NoneGutter: None
publication: TBDart Director: Cliff Skeete 8-3726
copyWriter: Bruce Jacobson 8-3119acct. mGr.: Tara Boras 8-4682
art proDucer: Bill Gastinger 8-3727print proD.: Jack Hughes 8-3504proJ. mnGr.: Elena Brady 8-4104
this advertisement prepared by young & rubicam, n.y.
1G66354_aDc_b2.1_crc.indd
client: ADC tmG #: 1G66354 HanDle #: 2 Job #: ADC-ART-M84812B billinG#: ADC-ART-M84581Document name: 1G66354_ADC_b2.1_crc.indd paGe count: 1 of 1 print scale: 100% inDesiGn Version: CS5stuDio artist: Sc last saVe Date: 7-11-2011 2:14 PM creator: Kris creation Date: 6-28-2011 12:01 PM
Document patH: TMG:Volumes:TMG:Clients:YR:Ad Council:Jobs:2011:1G:1G66354_ADC-ART-M84812:Mechanicals:1G66354_ADC_b2.1_crc.inddfont family: Gotham (Bold, Black)link name: 1f66261_aDc_a3_v.tif, 1f66261_aDc_m1_r.tif, arthritisf_4cblueblack_no_rule_yr.eps, aDcouncil_100c56m23k_yr1.epsink name: Cyan, Magenta, Yellow, Black
T:7”
T:4.625”
What’s your weapon? Visit FightArthritisPain.org
arthritismy weapon against
Courtesy of eDevice

12 | JUNE 2012
research & technology
W ith obesity levels and type II diabetes on the rise in America, it comes as no sur-
prise that more and more patients are battling a range of cardiovas-cular issues. And while the best remedy is often a healthy diet and regular exercise regimen, there are some cases where this simply isn’t enough. When patients don’t respond to beta-blockers or blood-thinning medications, or worse, when they have other high-risk conditions that won’t allow for open heart surgery, their options grow limited. Fortunately a number of technological advances are keep-ing the country’s top cardiologists on the cutting edge of heart health, and more importantly, helping pa-tients avoid the operating table.
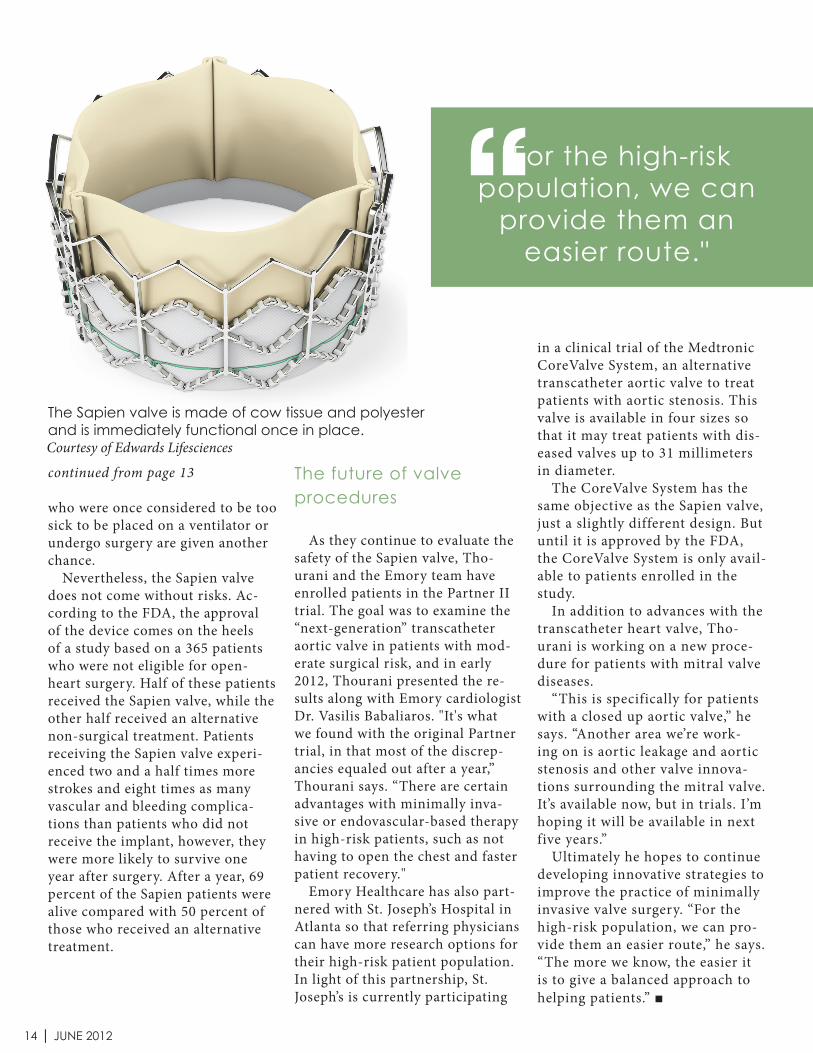
The Sapien valve
In November of 2011, The United States Food and Drug Administra-tion (FDA) approved a new trans-catheter heart valve that is expected to revolutionize the treatment of cardiovascular issues. The device – called the Sapien valve – offers a new, non-surgical option for indi-
viduals experiencing failing aortic valves. With this approach, doctors create a small incision in the groin or chest wall, and then feed the wire-mesh valve through a catheter and guide it up to the heart. The valve is then wedged into the aortic opening by an inflatable balloon, replacing the natural heart valve. This way, they can avoid opening the chest or stopping the heart.
“The impact of the Sapien valve is huge,” says Vinod H. Thourani, MD, Associate Professor of Cardio-thoracic Surgery at Emory Univer-sity School of Medicine in Atlanta, Ga. “It’s allowed us to take care of patients we couldn’t otherwise take care of. For the high-risk patient population, it provides a much easier route.”
This high-risk patient population includes approximately 300,000 Americans who currently suffer from deterioration of the aortic valve, the gateway to the heart. This condition forces the heart to work harder to pump blood, often leading to heart failure, blood clots and sudden death. The result is aortic stenosis, and according to the FDA, more than half of patients diagnosed with the condition die within two years.
Each year, about 50,000 people in the U.S. will undergo open-heart surgery to replace this valve, but the procedure is anything but easy. The surgeon must saw the breastbone in half, stop the heart, cut out the old valve and sew a new one into place. And until last
A Game Changer for Open Heart SurgeryHow cardiologists are helping patients avoid the operating table with a minimally invasive approach
By Taylor Arnold

MEDMONTHLY.COM |13
year, thousands of other patients were turned away, deemed too old or ill to survive the operation. But thanks to the Sapien valve, more of this high-risk patient population can avoid going under the knife. The tiny cardiac device, manu-factured by Edwards Lifesciences in Irvine, Cali., is made from cow tissue and polyester supported by a steel frame. Once surgeons put the Sapien valve in place, it is immedi-ately functional.
The learning curve of transcatheter aortic valve replacement
Today Thourani performs mul-tiple valve procedures a week, rang-
ing from transcatheter aortic valve replacement (TAVR) to surgical aortic valve replacement (SAVR). But he admits there was a learn-ing curve with the transcatheter valve, which he has been under study at Emory since 2007. “At first it was a novel procedure, and we were doing about two a month,” he explains. “Now we do about five to six procedures a week because our team can handle different patients in a more uniform fashion. It is operator dependent, so of course those who have done it more have more experience with it.”
The results of this extensive study at Emory, as well as the Part-ner I trial in 2007 led by Thourani and his team, were instrumental in the FDA’s approval of the Sapien
valve in late 2011. To date, the Em-ory Heart & Vascular Center team have completed over 260 TAVR procedures, and while the Sapien device is currently only approved for patients who cannot undergo open-heart surgery, about 20,000 new patients in the U.S. should be eligible to receive a heart valve each year moving forward.
The FDA is expected to clear the Sapien valve for patients who are healthy enough to undergo surgery, but still fall under the high-risk population. Once this group is cleared, anywhere from 50,000 to 80,000 new patients will be eligible for the procedure each year in the U.S.
The safety of a TAVR procedure
Thourani has found the safety of a TAVR procedure to be the same as open surgery, although TAVR patients recover much faster. In fact, it’s not uncommon to go home two to three days after surgery. “Inoperative patients for SAVR are good candidates for TAVR,” he says. “They’re super high-risk based on objective patient charac-teristics such as previous opera-tions, lung issues, severe chronic obstructive pulmonary disease (COPD) and poor heart function.”
When compared to open heart surgery, the most significant ben-efit of minimally invasive pro-cedures is avoiding the risks and complications associated with the heart and lung bypass machine. Less invasive procedures also have a significantly shorter recovery time and require a shorter hospital stay. And in some cases, patients continued on page 14
The Sapien valve offers a solution to patients who are
not eligible for open heart surgery.
Courtesy of Edwards Lifesciences
14 | JUNE 2012
continued from page 13 who were once considered to be too sick to be placed on a ventilator or undergo surgery are given another chance.
Nevertheless, the Sapien valve does not come without risks. Ac-cording to the FDA, the approval of the device comes on the heels of a study based on a 365 patients who were not eligible for open-heart surgery. Half of these patients received the Sapien valve, while the other half received an alternative non-surgical treatment. Patients receiving the Sapien valve experi-enced two and a half times more strokes and eight times as many vascular and bleeding complica-tions than patients who did not receive the implant, however, they were more likely to survive one year after surgery. After a year, 69 percent of the Sapien patients were alive compared with 50 percent of those who received an alternative treatment.
The future of valve procedures
As they continue to evaluate the safety of the Sapien valve, Tho-urani and the Emory team have enrolled patients in the Partner II trial. The goal was to examine the “next-generation” transcatheter aortic valve in patients with mod-erate surgical risk, and in early 2012, Thourani presented the re-sults along with Emory cardiologist Dr. Vasilis Babaliaros. "It's what we found with the original Partner trial, in that most of the discrep-ancies equaled out after a year,” Thourani says. “There are certain advantages with minimally inva-sive or endovascular-based therapy in high-risk patients, such as not having to open the chest and faster patient recovery."
Emory Healthcare has also part-nered with St. Joseph’s Hospital in Atlanta so that referring physicians can have more research options for their high-risk patient population. In light of this partnership, St. Joseph’s is currently participating
in a clinical trial of the Medtronic CoreValve System, an alternative transcatheter aortic valve to treat patients with aortic stenosis. This valve is available in four sizes so that it may treat patients with dis-eased valves up to 31 millimeters in diameter.
The CoreValve System has the same objective as the Sapien valve, just a slightly different design. But until it is approved by the FDA, the CoreValve System is only avail-able to patients enrolled in the study.
In addition to advances with the transcatheter heart valve, Tho-urani is working on a new proce-dure for patients with mitral valve diseases.
“This is specifically for patients with a closed up aortic valve,” he says. “Another area we’re work-ing on is aortic leakage and aortic stenosis and other valve innova-tions surrounding the mitral valve. It’s available now, but in trials. I’m hoping it will be available in next five years.”
Ultimately he hopes to continue developing innovative strategies to improve the practice of minimally invasive valve surgery. “For the high-risk population, we can pro-vide them an easier route,” he says. “The more we know, the easier it is to give a balanced approach to helping patients.”
"For the high-risk population, we can
provide them an easier route."‘‘
The Sapien valve is made of cow tissue and polyester and is immediately functional once in place.Courtesy of Edwards Lifesciences

What’s your practice worth?When most doctors are asked what their practice is worth, the answer is usually, “I don’t know.” Doctors can tell you what their practices made or lost last year, but few actually know what it’s worth.
In today’s world, expenses are rising and profits are being squeezed. A BizScore Performance Review will provide details regarding liquidity, profits & profit margins, sales, borrowing and assets.
Out three signature sections include: Performance review Valuation Projections
919.846.4747bizscorevaluation.com
Scan this QR code with your smart phone to learn more.

16 | JUNE 2012
The newly established Univer-sity of North Carolina (UNC) Center for Diabetes Transla-tion Research to Reduce Health
Disparities (CDTR) recently brought together institutional partners and diabetes researchers to foster collabo-ration during its first annual meeting. One of seven such centers established nationally, it began in September 2011 with a $3 million, 5-year grant from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The CDTR’s mission is to facilitate research about diabetes and move discoveries more quickly into practice, treatments and the commu-nity.
Partnering with UNC-Chapel Hill are institutions that can most directly move this research forward to im-
prove health: Wake Forest University (WFU), East Carolina University (ECU), UNC-Pembroke (UNC-P) and the Robeson County, N.C. Health Department, all of which had repre-sentatives presenting at the meeting.
Currently, 1 in 9 adults in the U.S. (about 26.4 million) has Type 2 diabetes. Projections suggest that 1 in 3 people may have the condition by 2050. Diabetes-related annual costs are currently $174 billion and may increase to $336 billion by 2034. Unfortunately, poor, minority and rural populations with limited access to health care suffer disproportion-ately. Especially in North Carolina, African-American, Hispanic and Native-American populations have a higher rate of diabetes and related complications.
Each partner provided updates on diabetes research at their institu-tion and suggested ways in which to work with one another. Ronny Bell, PhD, represented WFU; Doyle “Skip” Cummings, PharmD, ECU; and Frankie Powell, PhD, and Cherry Beasley, PhD, RN, UNC-Pembroke. “It was very affirming to have a face-to-face meeting with colleagues who are not only impressive ‘on paper’ but who are also very dedicated hu-man beings,” said Powell. “I think the contributions that we will make, collectively, to this state will be great. Given the newly released county health rankings, ours – Robeson County at 99th – will benefit much from our team efforts in address-ing the challenges of diabetes in our community.”
Each of the four CDTR leaders presented about their core areas as well. Rich Davis, MD, leader of the Access with Technology Core and co-director, led discussion about the CDTR’s intent to compile a library of emerging technologies useful to diabetes researchers. The core also provides training and consultation to researchers for using technology in
UNC CDTR Collaboration for Diabetes ResearchAddressing the challenges of treating the country’s most at-risk populations
By Elizabeth Witherspoon
research & technology

Lindsay Driver EmployeeSync Specialist
Consolidate Payroll, Benefits Administration, Time & Attendance and Personnel Management in one single database Available in IN, KY, NC, OH, PA, TN, VA Designed for employers with 25+ employees
www.Jones‐Insurance.com/EmployeeSync
their work.Mike Pignone, MD, MPH, co-director
and leader of the Literacy and Nu-meracy Core, a nationwide resource for investigators who want to study or use low-literacy materials in research, said approximately 10.3 million people are struggling with basic or below-basic literacy. Because of the heavy burden of monitoring, calculations and self-man-agement in diabetes, studies have shown that inadequate literacy increases the risk of adverse outcomes.
Alice Ammerman, DrPH, leader of the Community Connections Core, de-scribed ways in which the core can help investigators navigate community-based research, with the following admonition:“Vulnerable communities are often researched, but nothing is left behind. We need to give back and have a positive effect on the community.”
Finally, Beth Mayer-Davis, PhD, leader of the Pilots and Feasibility Core, described the qualifications and process to apply for pilot funding for diabetes research.Small groups of participants discussed: ways to foster cross-institutional collab-orations, ways to promote core resources and programs, institutional challenges to diabetes translational research and possible solutions and suggestions for CDTR consortium projects.
The CDTR also introduced new staff members: Kelley Cardone, Jim Mah-aney and Barbara Moeykens, project manager/literacy and numeracy core; Alexandra Lightfoot, EdD, director of community partnerships; and unveiled its new website. “I’m very encouraged by what we’ve been able to accomplish,” said Pignone as he asked participants to build on the momentum of the meeting.
The CDTR leverages existing adminis-trative and other resources at the North Carolina Translational and Clinical Sciences (NC TraCS) Institute, which is home for the UNC’s Clinical and Translational Sciences Awards (CTSA) from the National Institutes of Health. “Without those extensive resources at the CTSA, this center would look very different,” said Davis.
* Article previously published by NCTraCs

L ook no further than online patient reviews to discover what is good, bad and down-right ugly about your prac-
tice. It’s important to monitor these reviews in order to improve patient care and manage your online repu-tation, but there’s another hidden advantage that is perhaps the most valuable of all in attracting new patients – to boost your website’s search engine rankings.
By participating in free review websites such as Healthgrades, Vitals, and even Yelp, you can help
there is also an algorithm associ-ated with Google Places. Google relies on factors such as, how many reviews you have and how exten-sively you fill out your Google Plac-es listing to rank local businesses, such as medical practices and in a particular order.
Since the Google Places listings are merged with Google’s organic search engine results, you have an even greater chance of ranking on page one just by optimizing your Google Places listing. Unlike some review sites, Google actually al-lows you to respond to reviews by Google users. Use this opportunity to demonstrate your customer ser-vice skills by promptly responding to negative reviews to show patients you are listening. You can’t delete negative reviews but what you can do is encourage your happy pa-tients to dilute negative comments with positive ones.
One or two bad reviews will not significantly harm your reputa-tion as long as there are three or four positive ones as well. Posting a request through a link on your website or Facebook page are great ways to ask satisfied patients to post reviews. Google recognizes when you keep your profile up to date and are an active participant in your listing, and uses this as a major part of their algorithm when calculating rankings.
There are many reasons to monitor and manage your online patients reviews, but perhaps most beneficial of all is the opportunity to improve your website rankings in Google. For good or for bad, online patient reviews are an effec-tive way to promote and grow your practice.
maximize your website’s rankings and ultimately increase the num-ber of new patients visiting your site. It’s beneficial to optimize your listings on as many review sites as possible, but arguably the most valuable review source of all, due to its popularity, is Google Places.
Google Places (the section of Google search results that lists local businesses) collects ratings from various sites and provides a comprehensive list of patient re-views. Similar to how Google uses a special algorithm to rank websites,
The Hidden Advantages of Online Patient Reviews
Even bad ratings are good for both you and your patients
By Amanda Kanaan
practice tips
18 | JUNE 2012

Here’s how you can use online patient reviews to boost your rankings in Google Places.
1. Claim your listing: Google Places retrieves information from vari-ous online directories to create listings. Therefore, your practice may already exist in Google Places. Start by searching Google Places by your tele-phone number and then claim your listing(s) if you haven’t already. All you need for this is a Google account (simply sign up for a free Gmail account if you don’t already have one). Delete any dupli-cate listings as this may harm your rankings and do not use the same phone number for multiple loca-tions.
2. Complete your listing: After you claim your Google Places account, you will want to fill out your profile as completely as possible. That includes adding a link to your web-site, images and a description of your practice. Be sure to use keywords that relate to your practice or specialty. Your Google Places page will show your profile’s completion rate and it is most effective when it reaches 100 percent.
3. Use reviews to your advantage: Some physicians are hesitant to get involved in online resources such as Facebook and patient review websites, but the truth is the conversation is happening with or without you so take advantage of the opportunity to positively brand your prac-tice.

20| JUNE 2012
practice tips
A ccepting responsibil-ity to care for a given patient population with chronic disease (diabetes
for example) involves a transforma-tional shift from counting numbers of patients served to managing a population with a given chronic condition. As teams begin working to improve the quality of care and patient service to such a designated population, a shift in care delivery is
occurring. Accountable Care Orga-nizations (ACOS) are developing, organizing and experimenting with different ways to adjust reimburse-ment in primary care to reward im-provements in efficiency, and care coordination & delivery.
Many successful ACO models are embracing a shift from volume-based reimbursement to value based reimbursement and the formation of population health management
hubs. With the devel-opment of these new structured organiza-tions, PAs and NPs will also act as extenders to support the primary care physician within the medical home model.
Consumers are more actively shopping for health care provid-ers. Transparency is being demanded to enable comparison-shopping. The 2011 U.S. and Global Survey of Health Care Con-sumers performed by Deloitte showed that consumers remain largely confused about the health care system although they were highly opinionated about their interactions with doctors, hospitals, health insurers and in
their views of prescription drugs. As a result, they concluded that con-sumers judge the U.S. health care system based on their prior personal experience rather than by a systemic view, perhaps due to its magnitude and complexity.
Patient satisfaction is becoming more central to patient care, espe-cially in the primary care sector. With the advent of social media and online reputation management,
Transitioning from Volume to Value Cutting edge management of care delivery to populations with chronic diseases
By Lisa P. Shock, MHS, PA-C

‘‘"Many successful ACO models are embracing a shift from volume-based
reimbursement to value based reimbursement and the formation of
population health management hubs."
MEDMONTHLY.COM |21
DR. EDWAR D
DENTAL PRACTICE ADVISOR
Available at: DentistrysBusinessSecrets.com
Practice Management CD SeriesHighly effective practice management resources, fundamental
office documents and marketing campaigns to help grow and
promote your dental practice.
More tools for building and growing your dental practice
Learn more & get the practice management CD series at DentistrysBusinessSecrets.com
patients are increasingly rating and comparing all providers on their health care delivery team. Often customer service oriented met-rics including wait times; provider responsiveness and communication of test results in a timely fashion define a successful patient interac-tion experience.
Benefits for population manage-ment are based on a primary hy-pothesis for quality. Third party payors are incentivizing primary care providers to meet quality metrics through improved reim-bursement programs such as the Blue Cross Blue Shield Blue Quality Physician Program (BQPP). Improved reimbursement models also plan to utilize methodologies such as bundled payments to in-centivize quality. Under a system of bundled payments, reimbursements for multiple providers are bundled into a single, comprehensive pay-ment that covers all of the services involved in a patient’s care. The goal of the bundled payment approach is to improve population health, improve the patient care experience and reduce overall health care costs.
Health reform efforts are tar-geting development of improved bundled payment systems. The Ac-countable Care Act calls for estab-
lishing a national pilot program on payment bundling for Medicare by 2013 and for a Medicaid bundling demonstration program by 2012. The new Center for Medicare and Medicaid Innovation (CMI) will recruit and enroll patients into a voluntary, 5-year pilot program that will test bundled payments. These pilots may include hospitals,
long term care facilities, inpatient rehabilitation facilities, physician groups, skilled nursing centers and home health agencies. They will address episodes of care that begin three days prior to a hospitaliza-tion and span up to 30 days post-discharge. The trial pilot will test improved coordination, quality and efficiency of care services around a
given hospitalization for a patient with one or more of eight medical conditions to be determined and selected by the Secretary of Health and Human Services.
By integrating the care delivery system and restructuring the deliv-ery of primary care services across settings from outpatient to hospital, populations and conditions may be
managed more efficiently. A team approach to care delivery will help to improve patient satisfaction and improve quality care for chronic diseases. Transformation of care delivery teams and utilization of an interprofessional team approach will then lead to improved outcomes overall for patients.

practice tips
Most companies go through an agonizing yearly ritual of vetting which insurance companies will
provide the best medical options for the lowest cost to the company, while never taking the individual practice into account. As many patients choose their doctors from a list in a book, it is imperative that medical practices dif-ferentiate themselves from the practice down the road or across the hall. How do they make themselves stand out? Great customer service from initial contact is the single most important aspect affecting practices today. What impression does your practice make? Is voicemail the first thing a patient
hears? A recent survey asked, "What is the biggest complaint you have with your medical professional?" Most of those surveyed said, "leaving a voice-mail message and never getting a call back."
Have your patients voiced their discontent? Is your office staff com-plaining that they feel as if they are at the circus performing like jugglers on a tight rope? What about first thing in the morning, just as the doors are opening? The phones are already ringing but before these calls can be answered, the staff has to go through voicemails that came in overnight. These calls are for all different aspects of the practice – appointment calls,
insurance and billing questions, lab results and prescriptions just to name a few. They are being hand written and forwarded to the appropriate depart-ment. Consider how much time that takes your staff to accomplish. During that time, the staff member is unable to handle their own job responsibilities.
There are many solutions that can help staff become a welcomed friend rather than the enemy. One option is hiring a professional medical an-swering service to handle your calls. A good business answering service can handle inbound calls, overflow, appointment scheduling and many other scenarios that will free up office staff. This allows them to concentrate on taking care of the patients in the office. Any good answering service can separate calls and forward them to the appropriate staff member as complete messages. The staff can then return calls in a quick and professional manner because they already know what the caller requires. An answering service that also provides web-based documentation and creates a manage-ment tool that ensures all calls have been handled and nothing can slip through the cracks.
Everywhere from shopping malls to hospitals, companies want feedback. How are we doing? Did you have a good experience? Will you recommend us to friends, family and on your social network? The medical community is no different, they must remain engaged or they will stop being profitable.Remember, outsourcing calls to a professional virtual secretary will pro-vide patients with a better experience. Those patients will refer the practice to their family and friends, and your staff will have more time to concentrate on the things that are important to the practice and profitability. Everyone wins.For more information visit http://www.profilesandreviews.comArticle Source: http://EzineArticles.com/?expert=Mike_Cynar
Medical Answering Services Improve Patient ExperiencesOutsourcing calls can create a win-win situation for you and your patients
By Mike Cynar
practice tips
22| JUNE 2012

22| MAY 2012
practice tips

Trust patient education from the leading names in heart and stroke health.Krames is your source for American Heart Association and American Stroke Association patient
education. Built on an 80-year foundation of research and science, these resources help healthcare
professionals reach patients, caregivers, and at-risk groups to promote disease management and
prevention, create awareness, and inspire change.
Call 800-333-3032 or visit www.krames.com/aha
for our complete collection of patient education!
Turnkey kits
Education and awareness products Caregiver resources
And more…
Ask us about custom publishing opportunities!
7072
17359_full page ad 1/17/08 4:49 PM Page 1

CLIENT: BBDO InternalPRODUCT: Tommy FPJOB#: P25248SPACE: Full Page: 4CBLEED: NoneTRIM: 8.4375” x 10.375”SAFETY: NoneGUTTER: NonePUBS: NoneISSUE: NoneTRAFFIC: Donna MendietaART BUYER: NoneACCOUNT: NoneRETOUCH: NonePRODUCTION: Michael MusanoART DIRECTOR: NoneCOPYWRITER: None
This advertisement was prepared by BBDO New York
FontsArial Black (Regular), Helvetica (Regular, Bold), TheSansLight (Plain)Graphic Name Color Space Eff. Res.Tommy1.psd (CMYK; 438 ppi), Stitched_Type.psd (CMYK; 741 ppi), Linen_logos.psd (CMYK; 476 ppi), Autism Speaks Logo_4C_2010.ai
Filename: P25248_BBD_GEN_V2.inddProof #: 16 Path: Studio:Volumes:Studio:MECHANIC...Mechanicals:P25248_BBD_GEN_V2.indd Operators: Robison, Blane / Young, Michael
Ink Names Cyan Magenta Yellow Black
Created: 12-2-2011 4:31 PM Saved: 2-8-2012 4:01 PMPrinted: 2-8-2012 4:01 PMPrint Scale: 100%
T:8.4375”T:10.375”
Final Art
Photo by Jade Albert
Learn more at
autismspeaks.org/signsSome signs to look for:
No big smiles or other joyfulexpressions by 6 months
No babbling by12 months
No words by16 months
© 2012 Autism Speaks Inc. "Autism Speaks" and "It's time to listen" & design are trademarks owned by Autism Speaks Inc. All rights reserved. The person depicted is a model and is used for illustrative purposes only.
x1a

legal
26 | JUNE 2012
Health Care IT: Five Best Practices to Protect Against PHI BreachesDecrease non-compliance ramifications in your practice with a fool-proof planBy Frank J. Rosello
Health care information technology continues to be acquired and implemented by medical organizations
throughout the United States at his-toric levels. This significant trend in health care IT adoption can be at-tributed to the myriad of government initiatives and polices currently in place to promote the use of health care IT. As accessibility to patient informa-tion continues to increase, so does the risk of protected health information breaches.
Protected health information (PHI), also referred to as personal health information, can include demographic information, test and laboratory re-sults, medical history, insurance infor-mation and any other data collected by clinicians to identify an individual or determine appropriate care. As a result, the Health Information Portability and Accountability Act of 1996 (HIPAA) was established to create national stan-dards to protect a patient's electronic PHI. HIPAA requires appropriate administrative, physical and technical safeguards to ensure the confidential-ity, integrity, and security of electronic protected health information. The Of-fice for Civil Rights (OCR), a depart-ment within the U.S. Department of Health and Human Services (HHS), is responsible for enforcing the HIPAA
Privacy and Security Rules.Further, under the Health Informa-
tion Technology for Economic and Clinical Health Act (HITECH) Breach Notification Rule, notification to OCR of breaches involving five hundred or more individuals must occur contem-poraneously with notice to affected individuals. According to a HHS report to the U.S. Congress of PHI data breaches since 2009, 252 incidents oc-curred that went on to affect more than 10 million patients. The breach reports submitted to OCR for the reporting period described the five common causes of incidents in rank order:
1. theft 2. loss of electronic media or paper
records containing PHI 3. unauthorized access to, use, or
disclosure of PHI 4. human error 5. improper disposal
The largest PHI breach reported to date involved a covered entity that had 57 unencrypted computer hard drives stolen from a leased facility. The hard drives contained the PHI of more than 1 million individuals, including member names, social security num-bers, diagnosis codes, dates of birth and health plan identification num-bers. The OCR investigation found the
entity failed to implement appropriate administrative safeguards to adequate-ly protect information remaining at the leased facility by not performing the required security evaluation in re-sponse to operational changes. In addi-tion, the investigation showed a failure to implement appropriate physical safeguards by not having adequate facility access controls. Both of these safeguards are required by the HIPAA Security Rule. The lack of compliance resulted in the entity agreeing to pay HHS $1.5 million dollars for violations of HIPAA privacy and security provi-sions. This was the first enforcement action resulting from the HITECH Breach Notification Rule. Interestingly, the second largest breach occurred not because of a hacked password, but when computer back-up tapes were stolen from the back of a truck.
Security within the health care industry is changing and PHI data breaches are a significant issue. At risk are not just a patient's privacy and personal information, but also the reputation and financial well being of the medical organization. Health care administrators have a clear choice – either maintain internal staffing levels to effectively mitigate the risk of PHI data breaches or hire an outside health IT vendor that can help develop and manage their security policies and

MEDMONTHLY.COM |27
procedures.To help medical organizations and
providers effectively plan for, mitigate and protect against PHI data breaches, consider the following five best prac-tices:
1. Perform an enterprise-wide PHI risk assessment
Performing a risk assessment is the most effective way to understand where the threats and vulnerabili-ties are within the organization with regards to patients and their PHI. In many instances, risk assessments and mitigation plans are being discussed only at the executive level within an organization. The discussions are typi-cally about risk transfer and mitiga-tion, but should also include processes for securing patients PHI in the wake of new emerging threats. Deploying the latest security technology alone will not reduce the risk of PHI breach-es, as that's not where the vulnerabili-ties lie. Understanding when, who and how patient information is accessed are critical components that should be included in a comprehensive risk assessment.
2. Develop a PHI security strategy
A sound PHI security strategy involves not only understanding where PHI information resides, but also de-veloping a strategy to protect it. Once this understanding is achieved, it's essential to communicate it to employ-ees and other associates who are part of the organization. It is highly recom-mended to have a third party come in to bring a fresh perspective during the assessment stages and to help with developing a strategy. There has been a tendency for internal IT teams to look at security strategy and develop
a check-the-box solution. To prevent this situation, it can be very helpful for organizations to consider select-ing an outsourced health IT vendor who can be a trusted partner and can provide an organization a fresh and objective view of its PHI security vulnerabilities.
3. Implement PHI processes, technologies and polices
Once the risk assessment is com-plete and all potential issues are identified, it is important to leverage the tools and technologies in place, making it easy for employees and doctors to secure patient information. Establishing random inspection rou-tines is essential to insure compliance with internal PHI policies and proce-dures. Fortunately, there are effective techniques for implementing these routines with virtually no disruption to the primary focus of health care professionals, which is patient care.
4. Conduct impactful training sessions with employees
When it comes to protecting pa-tient information, it's about getting employees to understand how to best protect it and what to do if there is a data breach. Training is essential and should include not only administra-tive employees, but also doctors, nurs-es and other clinicians throughout the organization. All employees with access to patient information need to have the understanding of how to maintain security protocols when it comes to patient care. Many clinicians tend to look at PHI breaches as simply an IT issue. The HHS report to Con-gress validates that the risk of PHI breaches is far greater than a failure of technology alone.
5. Have a PHI breach re-sponse plan ready
Medical organizations should always be prepared in advance for a PHI breach. Many organizations oper-ate their facilities as if unauthorized disclosure of health information could never happen to them. Organizations that assume this posture often believe that they have effectively addressed all PHI security risks. However, there are thousands of unauthorized disclo-sures happening on a monthly basis all throughout the U.S. It is of critical importance for medical organizations to take a proactive approach in being prepared for a PHI breach. A reactive posture could be devastating, both on a reputational and economic level. The PHI breach response plan should be a living document within the orga-nization and should include specific procedures along with clearly defined roles and responsibilities in case of a PHI breach.
As medical organizations imple-ment health care IT systems that offer greater portability, interoperability and electronic data exchange capabil-ity, the development and execution of data security policies and procedures should be a key priority included in all health care IT strategic plans. Medical organizations and physicians that take preventative action by putting controls in place to safeguard sensitive patient information will be ahead of the game. Information security is not just a regulatory matter for providers; it's the right thing to do for their patients.
To learn more about our Physician Focused - Patient Driven approach to EHR & Health IT Visit our website: http://www.goeillc.com Article Source: http://EzineArticles.com/?expert=Frank_J_Rosello

26| MAY 2012

MEDMONTHLY.COM |29
Med Monthly
Medvertisingcompound noun: 1. The action of calling attention to medical goods or services for sale. Exclusively refers to advertising in Med Monthly.
Scan this code with your smartphone or visit medmonthly.com
Come see why we’re not your father’s medical journal
919.747.9031 | [email protected] | medmonthly.com
your practice website
MedMedia9 provides exceptional advertising, graphic design, mar-keting and publishing services in the health care industry. Promote your practice, hospital, medical service or product company on a large stage with MedMedia9.
$500OFF
To claim your discount, call 919.747.9031 and mention MM9 as your referral code to receive
$500 off of your personalized practice website!
Visit www.MedMedia9.com for more details on services and pricing.
www.MedMedia9.com
- Doctor bags- Briefcases- Handbags- Attachés- Luggage- Computer cases- And more!- And more!
Give your office something they’ve never seen.
&Rare SkinsCurrency
www.rareskins.com
Rare and Vintage Investment-Grade Skins and Currency

30 | JUNE 2012
legal
Medicare Fraud Strike Force Charges 107 Individuals for False BillingNation-wide stand reveals schemes involving approximately $452 million
H ealth and Human Services (HHS) Secretary Kathleen Sebelius and Attorney General Eric Holder re-
cently announced that a nationwide takedown by Medicare Fraud Strike Force operations in seven cities has resulted in charges against 107 in-dividuals, including doctors, nurses
and other licensed medical profes-sionals, for their alleged participa-tion in Medicare fraud schemes in-volving approximately $452 million in false billing.
Attorney General Holder and Secretary Sebelius were joined in the announcement by Assistant At-torney General Lanny A. Breuer of
the Justice Department’s Criminal Division, Federal Bureau of Investi-gations (FBI) Deputy Director Sean Joyce, Deputy Inspector General for Investigations Gary Cantrell of the HHS Office of Inspector General (HHS-OIG) and Peter Budetti, MD, Deputy Administrator for Program Integrity of the Centers for Medi-care & Medicaid Services (CMS). This coordinated takedown involved the highest amount of false Medi-care billings in a single takedown in Strike Force history. HHS also suspended or took other adminis-trative action against 52 providers following a data-driven analysis and credible allegations of fraud. The new health care law, the Affordable Care Act, significantly increased HHS’ ability to suspend payments until an investigation is complete.
The joint Department of Justice and HHS Medicare Fraud Strike Force is a multi-agency team of federal, state and local investigators designed to combat Medicare fraud through the use of Medicare data analysis techniques. More than 500 law enforcement agents from the FBI, HHS-OIG, multiple Medicaid Fraud Control Units, and other state and local law enforcement agencies participated in the takedown. In ad-dition to making arrests, agents also executed 20 search warrants in con-nection with ongoing Strike Force

‘‘
MEDMONTHLY.COM |31
investigations. “The results are at the heart of
an administration-wide commit-ment to protect American taxpay-ers from health care fraud, which can drive up costs and threaten the strength and integrity of our health care system,” said Attorney General Holder. “We are determined to bring to justice those who violate our laws
care fraud, violations of the anti-kickback statutes and money laun-dering. The charges are based on a variety of alleged fraud schemes in-volving various medical treatments and services such as home health care, mental health services, psycho-therapy, physical and occupational therapy, durable medical equipment (DME) and ambulance services.
According to court documents, the defendants allegedly partici-pated in schemes to submit claims to Medicare for treatments that were medically unnecessary and oftentimes never provided. In many cases, court documents allege that patient recruiters, Medicare ben-eficiaries and other co-conspirators were paid cash kickbacks in return for supplying beneficiary informa-tion to providers, so that the provid-ers could submit fraudulent billing to Medicare for services that were medically unnecessary or never provided. Collectively, the doctors, nurses, licensed medical profession-als, health care company owners and others charged are accused of conspiring to submit a total of ap-proximately $452 million in fraudu-lent billing.
“As charged in the indictments, continued on page 32
"These arrests send a strong message to criminals that the consequences of committing Medicare fraud are serious."
these fraud schemes were com-mitted by people up and down the chain of health care providers,” said Assistant Attorney General Breuer. “Today’s operations mark the fourth in a series of historic Medicare fraud takedowns over the past two years. These indictments remind us that Medicare is an attractive target for criminals. But it should also re-mind those criminals that they risk prosecution and prison time every time they submit a false claim.”
“Health care fraud is not a vic-timless crime,” said FBI Deputy Director Joyce. “Every person who pays for health care benefits, every business that pays higher insur-ance costs to cover their employees, every taxpayer who funds Medi-care—all are victims. The FBI will continue to work closely with our federal, state and local law enforce-ment partners to address health care vulnerabilities, fraud and abuse. We will use every tool we have to en-sure our health care dollars are used to care for the sick—not to line the pockets of criminals.”
In Miami, a total of 59 defen-dants, including three nurses and two therapists, were charged for their participation in various fraud schemes involving a total of $137 million in false billings for home health care, mental health services, occupational and physical therapy, DME and HIV infusion. In one case, 10 defendants were charged for participating in a fraud scheme at Health Care Solutions Network, which led to approximately $63 million in fraudulent billing for community mental health center (CMHC) services. Court documents allege that therapists at Health Care Solutions Network were instructed
and defraud the Medicare program for personal gain. As the takedown reflects, our ongoing fight against health care fraud has never been more coordinated and effective.”
“These arrests send a strong mes-sage to criminals that the conse-quences of committing Medicare fraud are serious,” said HHS Secre-tary Sebelius. “In addition to these arrests, we used new authority from the health care law to stop all future payments to 52 health care provid-ers suspected of fraud before they are ever made. Today’s actions are another example of how the Afford-able Care Act is helping the Obama administration fight fraud and strengthen Medicare.”
The defendants charged are ac-cused of various health care fraud-related crimes, including conspiracy to commit health care fraud, health

32 | JUNE 2012
Visit www.codinginstitute.com or Call us at 800-508-2582 and mention the promo code AN1IS011!
The Coding Institute LLC, 2222 Sedwick Drive, Durham, NC 27713
Start your ICD-10 Training Today with ICD-10 Coding Alert!
Your Monthly Guide to ICD-10 Coding, Training, and Reimbursement
12 monthly issues to get you ready for 2013.
Secure your coding arena with latest ICD-10 articles across all specialties.
Up to 18 CEUs per year!
Sweeping ICD-10 Changes Are in Sight - Will You Be Ready?
to alter notes and other medical documents to justify CMHC ser-vices for beneficiaries who did not need the services.
Seven individuals were charged in Baton Rouge, La., for participating in a fraud scheme involving $225 million in false claims for CMHC services. The case represents the largest CMHC-related scheme ever prosecuted by the Strike Force. Ac-cording to court documents, the defendants recruited beneficiaries from nursing homes and homeless shelters, some of whom were drug addicted or mentally ill, and provid-ed them with no services or medi-cally inappropriate services.
Eight defendants, including two doctors, were charged in Los An-geles for their roles in schemes to defraud Medicare of approximately $14 million. In one case, two indi-viduals allegedly billed Medicare for more than $8 million in fraudulent billing for DME.
In Detroit, 22 defendants, includ-ing four licensed social workers, were charged for their roles in fraud schemes involving approximately
$58 million in false claims for medi-cally unnecessary services, includ-ing home health, psychotherapy and infusion therapy.
The Strike Force operations are part of the Health Care Fraud Prevention & Enforcement Action Team (HEAT), a joint initiative an-nounced in May 2009 between the Department of Justice and HHS to focus their efforts to prevent and deter fraud and enforce current anti-fraud laws around the country.Since their inception in March 2007, Strike Force operations in nine loca-tions have charged more than 1,330 defendants who collectively have falsely billed Medicare for more than $4 billion. In addition, the CMS, working in conjunction with the HHS-OIG, are taking steps to increase accountability and decrease the presence of fraudulent provid-ers.
These cases are being prosecuted and investigated by Strike Force teams comprised of attorneys from the Fraud Section of the Justice Department’s Criminal Division and from the U.S. Attorneys’ Offices for the Southern District of Florida,
the Eastern District of Michigan, the Southern District of Texas, the Central District of California, the Middle District of Louisiana, the Northern District of Illinois, and the Middle District of Florida, and agents from the FBI, HHS-OIG and state Medicaid Fraud Control Units.
An indictment is merely a charge and defendants are presumed inno-cent until proven guilty.
To learn more about HEAT, go to: www.stopmedicarefraud.gov
continued from page 31
The Strike Force operations are a part of the Health Care
Fraud Prevention & Enforcement Action Team:
HEAT

National Provider IdentifierA National Provider Identifier (NPI) is a 10-digit
identification number issued to health care providers in the United States. The number is issued by Centers for Medicare and Medicaid Services (CMS).
The NPI began replacing the unique provider identification number (UPIN) in 2006 as the required identifier for Medicare services and other payers, including commercial health care insurers. The change to the NPI was mandated as part of the Administrative Simplifications portion of the Health Insurance Por-tability and Accountability Act of 1996 (HIPAA), and the first numbers were issued in October of 2006.
The NPI was proposed as an eight-position al-phanumeric identifier. However, many stakeholders preferred a 10-position numeric identifier with a check digit in the last position to help detect keying errors. The NPI contains no embedded intelligence; that is it contains no information about the health care pro-vider, such as the type or location.
All individual HIPAA covered health care providers (physicians, physician assistants, nurse practitioners, dentists, chiropractors, physical therapist, athletic trainers, etc.) or organizations (hospitals, home health care agencies, nursing homes, residential treatment centers, group practices, laboratories, pharmacies, medical equipment companies, etc.) must obtain an NPI for use in all HIPAA standard transactions, even if a billing agency prepares the transaction. Once assigned, a provider’s NPI is permanent and remains with the provider regardless of job or location changes.
More information regarding NPI numbers can be found at http://nppes.cms.hhs.gov
DEA NumberThe Drug Enforcement Administration (DEA) is a
U.S. Department of Justice law enforcement agency tasked with enforcing the Controlled Substances Act of 1970. It shares concurrent jurisdiction with the Federal Bureau of Investigation (FBI) in narcotics enforcement matters.
A DEA number is a series of numbers assigned to a health care provider allowing them to write prescriptions for controlled substances. Legally the DEA number is sup-posed to only be used for tracking controlled substances, however, the DEA number is often used by the industry as a general “prescriber” number that is a unique identifier for anyone who can prescribe medication.
A valid DEA number consists of two letters, six num-bers and a one check digit.
More information regarding DEA numbers can be found at www.deanumber.com
NPI and DEA numbersBy the numbers...
What you need to know about the National Provider Identifier and the Drug Enforcement Administration numbers
MEDMONTHLY.COM |33

Concierge Medicine The Doctor is Always in (for the right price)
features

‘‘
MEDMONTHLY.COM |35
F or anyone who has ever waited days or weeks to see the doctor, concierge medi-cine sounds appealing: For
an additional fee, patients typically enjoy same-day appointments and 24-hour access, more face time with the doctor and extra preventative care. Doctors who offer concierge medicine say the practice frees them from the constraints imposed by insurance providers and al-lows them time to give patients the individualized attention they need. Skeptics argue that concierge medi-cine promotes a two-tiered system, improving health care for a few but worsening it for everyone else.
“It's an attempt to formalize a two-class medical system,” says Wharton University professor of health care management Mark V. Pauly, PhD. “Those who can pay will get better treatment with a smile, and those who can't will have to wait.”
Sometimes called boutique medicine, retainer-based medicine or direct care, concierge medicine is a small but growing practice model. Concierge doctors in the United States serve almost a million patients, according to the Ameri-can Academy of Private Physicians (AAPP), a national association of physicians who provide concierge medicine and fee-for-service health care. The Academy estimates there are about 3,500 concierge doctors nationwide, up from about 2,400 just 18 months ago. It expects the number to double every 12 to 18 months for the next three years.
Concierge medicine comes in many different forms, according to Tom Blue, the Academy's executive director. About 75 percent of con-
cierge physicians hold on to their traditional practice, but take addi-tional fees from a small number of patients who receive special perks, priority treatment and services not covered by traditional insurance. On the other end of the spectrum, doctors forgo relationships with Medicare, Medicaid and insurance carriers entirely, building their
practice exclusively on patients
willing to pay annual retainer fees for care. Depending upon the ser-vices, fees range from as little as $60 per year up to $30,000 per year. The majority of patients still carry health insurance to pay for specialized services that their concierge doctor is unable to provide.
For doctors, concierge medicine isn't necessarily less work, but more satisfying work that allows them to build a more profitable prac-tice. Unlike traditional doctors, a concierge physician builds up an income stream from patient con-tracts, much like the business of an insurance agent or retainer-based financial planner. That makes the practice potentially more profitable when it is finally sold.
For patients, the much-touted benefit of concierge medicine is
that the doctor has more time and can provide them greater access. Concierge doctors “have 80 percent to 90 percent fewer patients, so they can do other things that other physicians simply can't,” Blue adds, such as house calls, email consulta-tions, and more extensive exams and preventative tests that insurance won't cover.
Prevention is concierge medi-
cine's most important benefit, ac-cording to Randy Baggesen, MD, a concierge physician in Richmond, Va., who says he often catches disease in early stages because his practice focuses on cutting-edge preventative care. Baggesen charges $3,300 annually for his services, which on top of routine care also in-clude tests such as a carotid intima-media thickness (CIMT) measure-ment, a type of ultrasound to detect plaque in artery walls. Sometimes described as a mammogram for the heart, the test is usually not covered by insurance if a patient is deemed low-risk, so most people don't get it. The problem, according to Baggesen, is that using current national guidelines, 88 percent of heart attack victims would have
continued on page 36
"Those who can pay will get better
treatment with a smile, and those who can't will
have to wait."

been deemed low to moderate risk on the day before their heart attack, 75 percent of all heart attack victims have normal cholesterol, and 86 percent would have passed a stress test. “Heart attack and stroke should be a preventable issue,” he says. “We catch subclinical vascular disease all the time.”
Concierge medicine could grow as the country's population ages and wealthy baby boomers demand more extensive care, notes Wharton health care management professor Jonathan Kolstad, PhD. Physicians, constrained by mounting paper-work, may also find the concierge option increasingly appealing. A study published in Health Affairs in 2011 found that the average physi-cian in the United States spends $82,975 per year to process insur-ance claims, coverage and billing, and that a physician's staff spends 20.6 hours per physician per week interacting with health plans. “The amount of time spent coding and documenting purposes is quite stag-gering,” Kolstad says. “The growth of concierge medicine reflects both a demand and supply effect. As more people want this kind of ac-cess, physicians see it as a way to gain autonomy.”
Off the grid
One of those physicians is Steven D. Knope, MD, a concierge physi-cian in Tucson, Ariz., who runs a full-retainer practice that is “com-pletely off the grid” of third-party payers such as Medicare, Medicaid and insurers. He charges an an-nual fee of $6,000 per individual or
$10,000 per couple for full services. He began his practice in 2000 after spending 10 years in a traditional practice and becoming increasingly frustrated with insurance companies. “When HMOs dominate the practice, for all intents and purposes, you work for them. They set the rates; they tell you what to order,” he says. “They owned 55 percent of my income stream... It just really demoral-ized me.” When a few of his patients approached him and suggested he shift to concierge medicine, he said, “No, this sounds elitist. It sounds unethical.” Over time, he changed his mind. “What was unethical was managing this third party system of companies rationing care.”
Today, Knope sees 12 to 15 patients per day instead of 30 or 40, giving him time for pro-bono work with veterans and the elderly. His practice consists of about 300 patients – half of whom pay the fee, and half “who either pay nothing, or sometimes give me a chicken.” A few of his long-time patients, in their 90s or older, cannot afford the an-nual fee but insist on paying him $5 per visit. “There's nothing unethical about taking care of the rich because all of us who do this take care of the poor as well,” he notes. “I have this amazing commodity called time.”
Knope believes concierge medi-cine holds part of the answer to the country's growing shortage of
primary care physicians. “I think the only way you can make primary care attractive is to do some sort of fee-for-service medicine,” he
states. “The bottom line is, people are not
going to make an investment
in medical school and their train-ing to make a terrible living at it...
It's logical to me that we
go back to our roots and we act
like any other pro-fessional – like a dentist
or a lawyer and say, ‘These are my rates; this is what I cost’.”
Arnold “Skip” Rosoff, a Whar-ton professor of legal studies and business ethics, disagrees. He says the spread of concierge medicine could numb people to the problems in the country's health care system. Patients who can afford concierge medicine and doctors who choose to offer it will naturally become less interested in finding a solution that benefits the country as a whole, he suggests. “It's going to devolve into a two-class system of care. If we don't address the fact that we don't have primary care physicians and all we do is put a band-aid on it for people who have concierge medicine... You have just shifted the problem.”
A "gun to the head" model?
Concerns about concierge medi-cine have grown as it has spread.
continued from page 35
36 | JUNE 2012
Concierge doctors see
an average of 12 to 15
patients per day, instead
of the industy average
of 30 to 40 patients.
FACT

‘‘With over 30 years of experience,
Additional Staffing Group can provide your practice with an exceptionally
talented staff that will streamline operations in your health care facility.
OUR SERVICES INCLUDE: Short/Long Term Temporary Placement Direct Hire and Executive Permanent Placement Payroll Services HR Consultant Services
WE STAFF: Receptionists Medical Records Technicians Accounting and Medical Billing Specialists
919-844-6601www.astaffinggroup.com
WORKFORCE EXPANSION SOLUTIONS
EMPLOYING PEOPLE THAT FIT
Some insurance companies have dropped concierge doctors, say-ing the model violates insurance contracts. Several states have ques-tioned whether concierge medicine goes against their insurance laws. The Office of Inspector General (OIG) of the U.S. Department of Health and Human Services (HHS) has warned concierge doctors that charging Medicare patients “an ‘access fee’ or ‘administrative fee’ that simply allows them to obtain Medicare-covered services” could be considered double billing.
Pauly worries about what will happen if increasing numbers of doctors see concierge medicine as an alternative to taking Medicare patients. Medicare is in financial trouble and is reducing its payments to physicians, making Medicare pa-tients less desirable. A survey by the American Medical Association of more than 9,000 physicians in May 2010 found that 17 percent were restricting the number of Medicare patients in their practice. Among the top reasons: 85 percent said Medicare payment rates were too low, and 78 percent said the ongoing threat of future payment cuts makes Medicare an unreliable payer.
“The great majority of doc-tors still take Medicare patients, but more are refusing to take new Medicare patients,” Pauly says. “If Medicare continues to tighten the screws on doctors some will react by saying, ‘I'm just fed up with the whole thing.’” And if more doctors shift away from traditional prac-tices to concierge medicine, it could exacerbate the physician shortage because there will be fewer doctors to go around, he adds. That could make it increasingly difficult for
non-concierge patients to find a physician.
The hybrid model of concierge medicine may offer a solution, says Wayne Lipton, founder of Concierge Choice Physicians. The private company, based in Rockville Cen-tre, N.Y., helps physicians incorpo-rate both concierge and traditional medicine under a single practice. Physicians usually keep about 2,000 patients but transition 75 to 100 patients into a concierge class that pays $150 to $200 per month ex-tra for enhanced care. That is far less drastic than shifting an entire practice of 2,000 to 3,000 patients to the full concierge model, which accommodates about 350 patients
continued on page 38
on average.Lipton calls the full-fledged
concierge practice the “gun-to-the-head” model for patients, who must choose between having to pay the concierge fee and losing their doctor. “To me, that's inherently troubling,” says Lipton. “If we were to promote that as a solution, it be-comes a have and have-not environ-ment.” The hybrid model, Lipton notes, “rebalances the system.” Pa-tients have the option to try out the concierge service without having to change doctors, and physicians are
"The hybrid model,
Lipton notes, 'rebalances the system.'"

38 | JUNE 2012
Does your Practice Accept
Insurance?
We Can Help!
Also, ask us about Affordable Medical Billing!
Call us at
1-855-4-THRIVE
Visit us at
MedicalCredentialing.org
able to create a new revenue stream and ease into a less hectic practice without turning patients away. Pa-tients also have a choice to stop pay-ing for the concierge service if they can no longer afford it or decided they don't want it anymore. “They're not hooked in forever,” Lipton says. “They can go back to being a regular patient.”
Wharton health care management professor Guy David, PhD is skep-tical. While models that trim fees down to $100 or $200 per month may make concierge medicine af-fordable for the middle class (that's less than what many people shell out every month for Starbucks cof-fee, he points out), it's unclear how much better care a physician could offer concierge patients on top of a full practice. It's simple mathemat-ics, David says. “What can a physi-
cian who has a very full clinic do for those priority patients?” David speculates that becoming a con-cierge patient in a hybrid practice might be like moving to zone 2 from zone 5 on an airplane – rather than upgrading from coach to first class. “If the effect on the non-concierge patient isn't big, the effect on the concierge patient isn't big.”
Another possible outcome: Non-concierge patients in the practice might suffer. Sometimes when firms try to differentiate services, instead of making higher-priced service better, they simply make the lower priced services worse. David points out a classic case from 18th cen-tury France, when a train company ripped the roofs off its low-priced cars to encourage customers to buy more expensive tickets. Might concierge doctors begin to resent
patients who don't pay for the extra service and skimp on health care as a result? David wonders: “Once you have this class system in your practice, what's going to stop (such) behavior?”
David emphasizes that concierge medicine is neither good nor bad, but a natural response to prob-lems in the health care system. He does not consider it a solution for the country. “I don't see concierge medicine being the new model for 300 million Americans,” he notes. Most people can't afford to pay retainer fees on top of taxes and health insurance premiums. “When you think about something that is sustainable at the national level, it's very clear that concierge medicine will not work,” David says, return-ing to his airline analogy: “You can't have everybody sit in zone 2.”
continued from page 37


Damaging behavior that is destroying the patient-
doctor relationshipBy Paula Rapp
features
Patient Bullying

A young friend of mine re-cently experienced minor chest pain. Not the kind that made her want to call 911
immediately, but worrisome enough to land her before a triage nurse at the local emergency room reviewing her symptoms. The patient, a nurse herself, was promptly seen by the ER physi-cian and after completing the requisite battery of chest pain examinations and blood work was discharged. The tests ruled out a heart attack and she was told to follow-up with her primary physician to determine other possible causes of the discomfort.
Of course as the pain persisted, she did what any well-informed health care consumer would do, she Googled the symptoms to find out what was ailing her. Within several clicks, she found the elusive diagnosis of which the ER doctor failed to provide: costochondri-tis, inflammation of the cartilage in the chest wall that can cause pain during breathing. Dutifully, she followed-up with her primary doctor and pro-claimed the diagnosis within minutes of their interaction. Silently she scoffed at the need for further testing that included x-rays, echocardiograms and blood work, and (although she politely listened to the recommendations) she left with what she had gone to receive: a prescription in hand for pain relief. When the symptoms eventually faded, she felt reassured that her diagnosis had been correct and was relieved not to have been subject to a further bat-tery of tests.
The traditional doctor-patient re-lationship is central to the practice of medicine and cornerstone to a thera-
peutic bedside interaction. The quality of this intricate bond is based on shared trust, mutual respect and knowledge. If these qualities exist, the doctor and patient will be able to communicate clearly and will likely lead to a more accurate diagnosis and outcome. If this rela-tionship is poor however, and either party distrusts the other’s judgment, de-creased compliance with the treatment will often occur. Decreased compliance leads to frustration, aggravation and further erosion of the relationship.
There is another phenomenon how-ever, emerging in the doctor-patient relationship: patient bullying. This is not to suggest a physical or name-calling type of bullying but rather a more passive, subliminal form. In light of the Internet era, it has become easier to instantly review symptoms and self diagnose, thereby making the doctor seem more of a “middleman,” rather than the voice of diagnosis determina-tion. The situation is often exacerbated by the fact that that the doctor has limited time with each patient and will often comply with a patient’s strong request.
The doctor’s knowledge and experi-ence has been demystified by the age of modern technology. Patients present to their doctor’s office with the expec-tation of the antibiotic prescription or the desired test or the clinical trial re-ferral and often won’t relent until their “demands” are upheld. If these requests
are ignored, patients feel as if they are being slighted or their symptoms mini-mized – all before the stethoscope has heard its first heartbeat.
Patient bullying behavior is seldom aggressive in nature; in fact it is often so subtle that it may seem more like the patient is just taking an active role in their own health care. After all, pa-tients are indeed savvier when it comes to their health and want to showcase to their doctor that they also have some medical insight. However, this type of rapport can become toxic when the patient’s strong arm requests outweigh the physician’s judgment.
A population of educated and inter-active patients would certainly be ideal, but some of these behaviors may lead to over-demanding pa-tients. The goal of patient education is to make knowledgeable health care decisions that are evidence-based and – more importantly – considered within a positive, recip-rocal patient-doctor partnership.
Don’t be pushed around!
Are you being pushed around? If there is evidence of any of the following behaviors in your practice, you are facing patient bullying.
Do your patients always expect a prescription when they are seen?
2 Are your patients always unsatisfied with your wait and see approach?
3 Do your patients quote web-sites, research trials & diagnosis before they have even been
examined?
4 Do your patients always insist on getting a second, third or fourth opinion when you do not agree
with them?
MEDMONTHLY.COM |41
1

42 | JUNE 2012
Three technology trends are creat-ing big opportunities for health care providers and managers to improve their bottom line,
drive savings, and empower a mobile workforce with “The Cloud”: improved cellular and network access to the Internet at all times, from all devices, and more powerful, less expensive smartphones and mobile devices to harness this improved access.The move to deliver computing services to these mobile devices, as well as traditional personal computers through these ubiquitous, powerful Internet con-nections, so that most of the work is actually done “In the Cloud” – saving a
lot of resources.The Cloud is more than just a fash-
ionable concept – this is a real change in the way people work – and leading organizations are looking past the buzz into the substantive improvements that technology can offer in work flow and cash flow.NOTE: For those who have not heard the term before, you can always substi-tute “the Internet” for the Cloud.
Do you get your email in a web browser? Cloud-based email! Do you like to stream your movies to your TV? Media in the Cloud! Do you have any-where you save important stuff online for either security or posterity? Yep –
this is Cloud-based storage!By relying on off-site computing
power and a constant high-speed Internet connection, the Cloud has all sorts of advantages over a traditional, on-premise model.
How can the Cloud change your practice today?
The Cloud can actually pro-tect things better than you can – for less money
If you have your valuable documents stored in on-site servers, or on person-al desktops, you are at risk. Cloud ser-vices offer auditability, encryption and redundancy, and with strong end-user security practices in place, can provide health care organizations with absolute top of the line data security AND put the replacement and maintenance back on the vendor. You pay for access, and pay only for what you need.
Moving documents to the Cloud not only protects them physically, but keeps them at your fingertips and the fingertips of permissioned users. Sepa-rated data facilities, redundant storage, and professional grade encryption are all more secure than the traditional, “server in the closet” model.
The Cloud can mobilize your practice, but keep everyone on the same page
The modern medical practice employs providers and administrative & clinical staff that bring powerful mo-bile devices to work every day – and take them home too. By giving your key decision makers access to their work files outside of the office, you give them the tools of a work com-puter anywhere they go. Physicians can handle office tasks on their own schedule, and in their own setting. Ad-ministrators can access critical docu-ments from a phone, or a home laptop
Leveraging the Cloud for Real ResultsUsing technology to increase revenue, drive savings and protect information
By Mary Pat Whaley
features

as easily as they would their desktop. The access you pay for is everywhere: if you have a web or wireless connection, you can access your files.
Tedious, in-house file transfer protocol (FTP) setups, or using virtual private networking (VPN) to access the network can be complex and costly solutions; work-arounds like emailing yourself the work files you need, or loading USB flash drives can introduce security risks. And, how can you be sure you remembered to send the latest version? If your work data is hosted in the Cloud, the availability of what you are working on is as much of an afterthought as the lights and water at your office. Updates to files are pushed to everyone immediately too, so you know your team always has the latest. With mobile applications and network access, employees can not only work from home – they can work from anywhere they have a mobile device and service.
The Cloud turns computing power into a utility
In terms of your practice cash flow, cloud computing enables you to flatten IT spending into a much more predict-able outlay. If you own your server, you are very familiar with the “update cycle.” Determining the right time for updates, upgrades, replacements and expansion to keep up with your needs, comply with new regulations, ease pain points for the staff, or improve security can be an endless loop of spending lots of time and money. In effect, a practice is never out of the upgrade cycle, they are only on the easier end of one for a while. The Cloud allows you to simply pay your monthly access and storage fees to your providers, and change plans as soon as you need more or less. Upgrades are pushed automati-cally, and built into monthly fees. You “pay as you go” for what you use – and only that. Scaling your IT resources up
and down as needed lets you fine tune your budget, and allows you turn your upgrade cycle into a predictable fixed expense. Employees can “B.Y.O.D.” or
How many of the things on this list are taking up space in your office and are at risk of being misplaced? How many can you locate and share with your employees, physicians and stakehold-ers right now?
• Physician credentials, privileges, re-appointments, continuing medical education (CME)
• Monthly and quarterly financials• Daily work – deposit slips, explanation of benefits (EOB),
checks, superbills• Practice management reports• Accounts payable invoices• Contracts• Partial or full paper charts that will not be included in the elec-
tronic medical records (EMR)• Personnel files• Personnel policies and employee handbook• PTO requests• Board agendas and minutes• Applicant resumes and paperwork• Benefit plan books• Retirement plan documents• Tax documents• Agendas and minutes of staff and board meetings• Policy changes and reviews• Templates and forms• Equipment user manuals• Referring physician holiday card or gift list• Anything else stored offsite or in your office that doesn’t need
to be taking space and costing money.
Where do I start?
Manage My Practice thinks leveraging the Cloud is an important way for medical offices to achieve efficiency and reduce costs. In fact, we think it is so important that we have partnered with Cloud leader Box to bring you MMP Fileconnect – a product specific to health care that allows you to manage your practice documents from anywhere. Box has installations in more than 70 percent of the Fortune 500 companies, and we think it’s the right product for you. Contact us to learn how Fileconnect can start helping your prac-tice today!
To find out more about Fileconnect contact Mary Pat at [email protected] or visit her website: www.managemy-practice.com
“Bring Your Own Device” – to give them a familiar hardware and software interface, and to give employers lower hardware costs.
MEDMONTHLY.COM |43

features

INNOVATING OURSELVESTechnologies exist to improve health care well beyond today’s standards. The move toward a better future begins with self innovation.
By Robert C. Tennant

In the United States we have access to unparalleled medical innovations. Laser eye surgery restores 20/20 vision. Infertile couples have means
to become biological parents. Robotics enable a doctor in California to per-form surgery on a patient in Florida. We may even be close to the day when a patient’s gene code will predictably inform an individualized treatment plan.
Unfortunately, even with all of these advancements, studies show that our avoidable death rate is still around 100,000 patients per year. This same study shows that we are not improving significantly in that the rate of avoid-able deaths has dropped only slightly (4.4 percent) in the 5 years between 1997 and 1998 & 2002 and 2003. On the financial front, hospital CEOs are struggling to keep their organizations prosperous and physicians (many worried about making ends meet) are scrambling to align with these larger health systems so that they have a safe haven.
Medical advancements touch many lives directly and indirectly, yet basic problems, such as the inability to pro-vide affordable health care to all, frus-trate consumers as costs continue to rise and more uncertainty surrounds the future of health care. Clearly, as many have pointed out, the business of medicine needs to change but where do we start? And why the seeming innovation paradox with health care being so advanced medically yet so lacking in other areas?
Outpaced by technology
Scientists and medical professionals have extensive knowledge of the hu-man body and medical technology has been developed to repair complex is-sues, so the lack of medical technology is not the problem. Could it be that the lack of non-medical technology, which enables the ‘business’ side of medicine
(medical processes and information management) is the cause? If we look at these medical processes and infor-mation management as it applies to health care, it all boils down to com-mon generic processes that exist in other industries, such as:
• Collecting usable data at the point of care
• Ordering things and making sure the order is filled
• Measuring operations and taking action if results are out of line
• Securely passing information between business partners
• Coordinating delivery of services between partners
• Combining and analyzing data to look for efficiencies and opportunities
Health care is uniquely complex in that it deals with caring for the human condition on all levels and it requires, on a regular basis, delivery of services to individuals with no ability to pay. Notwithstanding, other industries have found ways to innovate the above processes and leverage that innovation toward customer satisfaction and high profitability.
Regardless of the complexities, the fact of the matter is that health care is not effectively leveraging these non-medical technologies and this creates the innovation paradox. Statistics show that of the approximately 500,000 Eligible Professional (EP) physicians, only 31,000 or 6 percent have attested and received payment for Meaning-ful Use of an electronic health record (EHR) system. Meaningful Use mea-sures include the percentage of physi-cians who use an EHR system to:
• warn them if a patient is allergic to a medication.
• keep track of patients medications and problems.
• enter orders electronically (Note: receipt of order does not need to be
tracked).• electronically communicate with
other physicians and patients.• give their patients educational
material related to their condition and a summary of their visit.
• generate a list of patients with a certain condition such as diabetes or obesity.
Like most industries, health care couldn’t survive without the technolo-gy-enabled systems that perform their day-to-day operations. The technology is available but lack of adoption (and market driven improvement) of these technologies is a big part of the reason the U.S. health care system is strug-gling. The bottom line is that the inno-vators (you and I), not the technology, have become the limiting factor.
Behavior drives markets
A recent Wall Street Journal article titled “The Wireless Revolution Hits Medicine” points out that “…while medicine is one of the globe’s premier drivers of innovation, it is also a con-servative culture that now finds itself buffeted by transformational change.”
As health care professionals we find ourselves in the throws of transfor-mation and it is our reaction to this transformational wave that will define the new horizons of health care. How we behave when our comfort zone is challenged or “buffeted” will de-termine how and where innovation happens. We have the power to drive or squelch innovation and we have dis-played this power time and time again. Our willingness to adopt innovations has driven technologies such as the personal video recorder, fax machine, personal computer, flat screen TV and cell phones from the point of unafford-ability to ultimate ubiquity. Likewise, we need to adopt innovations that will drive affordable health care to the point of ubiquity.
What would it take for this kind of
46 | JUNE 2012

MEDMONTHLY.COM |47
market-driven transformation to hap-pen in health care? What would it take to drive the cost of a routine physical to $25 or less? How can we make rou-tine imaging, laser eye surgery or an emergency room visit more affordable to all? It would take a lot of willing-ness to (and to stop resisting) change. While none of us are individually to blame for the issues, the willingness to change is ours to own. It’s going to take courage, intention and sacrifice from all of us.
The barriers of fear, discomfort and short-term thinking
Unfortunately, too much of the health care system is driven by mis-aligned objectives. Some days it may seem as if the major players in health care (governmental bodies, payers, pharmaceutical, lawyers, physicians and hospitals) all want something different. These misaligned objectives create pressure and forces seemingly outside of our control driving the costs and complexities of delivering health care higher and higher.
Our resistance to these opposing forces instead of finding ways to align objectives can kill innovation. A strong desire to avoid conflict, fear of the un-known and to seek immediate payback often drives our resistance. These are a few examples of postures that we can easily find ourselves taking:
• “But we’ve always done it this way,” as opposed to objectively evaluat-ing the short and long-term merits of the new way.
• “Don’t bother me, I’m too busy,” instead of mustering the courage to step off and evaluate options.
• “This will never work,” and instead of articulating why, we are closed-minded and refuse to give it a chance.
• “But I can’t give that up, it’s what I do,” rather than evaluate how we might change our role to
contribute even more.• “They are out to get me,” rather
than considering the situation from the other parties perspec-tive, and explaining your position objectively so that you can work together to create a compromise.
We can also find ourselves wanting to avoid change for seemingly valid reasons with a short-term perspec-tive. For example, it is very rational for a physician to substantiate how much they stand to gain or lose by the reimbursement for achieving Mean-ingful Use. A physician may rationally determine that it will cost them more than the $44,000 payback and, thereby, decide not to pursue it. However, look-ing at the $44,000 as an item on the short term profit and loss statement is taking a short-term view. A long-term view of Meaningful Use would point to the idea that, in a few years, physicians who cannot perform certain basic functions with their EHR will be of much less value to the health care sys-tem and therefore receive much lower compensation for their work. In fact, they may eventually have a difficult
time finding work at all, depending on their specialty and geographic region.
We can’t afford to let fear, discom-fort and short-term thinking drive our decisions with regard to health care innovation.
An opportunity, not a burdenThere are definitely a lot of hurdles,
and the challenge to innovate the health care delivery system is not for the faint. It may seem like the system has taken away a lot of our indepen-dence and maybe it has, but the truth still remains that we are not slaves or prisoners. We have choices and the free will to exercise them. We can decide to be innovative or we can refuse. We can speak up on what we feel passionate about. There may be seemingly unpleasant consequences to our decisions, but we do have the abil-ity to choose and decide for ourselves. The technology exists and we have the freedom and opportunity to choose how we will hinder or promote inno-vation. In the end, the future of health care is up to us.

When Gutenberg invented the printing press in the 15th century he set a social revolution in motion that continues to gain momentum today: the increased
speed and availability of communication. Although his innovation underwent countless refinements and mechanism increases, the same simple principles were used up until the 20th century. Brian Allen is an expert on the history of printing and a master of the craft. He is truly an artisan printer and a pioneer, bringing together his wealth of knowledge, years of experience and his imagination in hopes of bridging the gap between modern and ancient printing tech-niques with his art.
Step inside his studio and you’ll find his intense dedication to the craft quite obvious. Every nook is occupied by printing equipment from various days in time, walls of books, large antique printers cabi-nets filled with type letters and several computers;
however you won’t find a desk or chairs on which to sit. One of the room’s most notable items is a 19th century Albion hand press from circa 1850. Origi-nally designed and manufactured in London, Allen found what he calls his “pride and joy” through an online auction from a seller in Atlanta. Allen uses his treasured press along with other printing mediums from his collection to create fine art spawned from an interesting blend of hand-set metal and wood type and computer generated designs. His experience in the field covers the gamut of print making technique, and he pulls inspiration from every facet, incorporat-ing modern digital typesetting with centuries old, tedious and even obsolete techniques. This pecu-liar marriage results in unique monotypes set onto exquisite paper (some even handmade) and then embellishing them with original brushstrokes and calligraphy. In addition to his art, Allen prints invita-tions, announcements, book covers and marketing
the arts
48 | JUNE 2012

MEDMONTHLY.COM |49
Bridging the Gap
Printing with the quality of ancient craftsmanship and modern technique
By Leigh Ann Simpson
materials. The quality of his letterpress printing is tactile and provides warmth that is rarely found today and widely sought after. Allen works with graphic designers and wedding consultants to make exotic invitations for his high-end clients. “They have to look more original in the wedding world so
that people don’t think that their invitations were done at Kinko’s,” he jokes.
Allen has an enormous library comprised of over 500 rare books on typeset-ting and printing as well as calligraphy, art and ceram-ics. “This is where I get my inspiration,” says Allen. “The shape of a letter is utilitarian and beautiful and that just fascinates me.
Look at the letter S, it’s both utilitarian and sen-sual – I’m just fascinated by that.” Allen also derives inspiration from early Venetian Renaissance printers like Nicholas Jenson. “Italian Renaissance forms are stately but not obtrusive,” he says. “They carried a message without being ostentatious.”
Allen was always a reader but he didn’t discover
Allen's 19th century Albion printing press. "
I always say I have one foot in the 15th
century and the other foot in the
20th century.
"

his passion for letters until after he graduated from college. He obtained a degree in geography and had planned on going into academia, but he took a posi-tion as a typesetter with a mapping company, a move that ultimately sparked his passion. Allen worked as a typesetter for nearly a decade from the mid 1970s to the early 80s before making a career shift during the time that the printing industry was being trans-formed into the digital age. He spent many years at the heart of the movement as a productionist making digital fonts for computer systems. “My career has been on the forefront and I’m very proud of the huge contributions that I made during the transition to today’s printing world,” he says. “And this was done before Photoshop!”
In addition to his list of impressive accomplish-ments, Allen is also a survivor of tongue cancer, a lesser-known type of cancer that is associated with extremely unpleasant radiation treatments that leave permanent, problematic effects such as constant dry
mouth and difficulty swallowing. “It was very dif-ficult but I made it,” he explains. “Now I know more about the medical world than I ever care to know.” Despite the challenge, he has managed to keep his sense of humor and can now laugh about one of the most painful experiences his life. “The protocol for head and neck radiation treatment must have gotten their ideas from the Spanish Inquision – at the end I would have told them anything,” he jokes. Allen admits he doesn’t have the stamina that he did before he was diagnosed. He says that he has downsized to a life that is much more simple and modest, which has allowed him to focus more on what is really impor-tant to him – his art. He also has moved into teaching his “bridging the gap” methods of letterpress printing to small groups of students. His inspiring story is a tribute to a fading art that he hopes to keep alive. “I want to leave a legacy,” he says. “That’s why I always say I have one foot in the 15th century and the other foot in the 20th century.”
Allen's St. Jerome letterpress and printmaking
50 | JUNE 2012

the kitchen
Summer Sips!
Summer is the season of hanging out by the pool, relaxing at the beach, or grilling out with friends and family. Many times, the drinks that we choose to accompany our summer
activities are full of calories, especially coming from sugar and/or alcohol. Here is a light and refreshing summer drink to quench your thirst! Each glass is filled with antioxidant rich strawberries and Vitamin C loaded lemon juice to keep you rejuvenated and hydrated. Enjoy!
Lemon Berry SlushyPreprep Time: 15 minutes | Servings: 2Ingredients:1/3 cup lemon juice (fresh squeezed juice is preferred)1 cup water1 cup frozen strawberries, thawed, with juice1/8 cup sugar (or Splenda)1 tray ice cubes
Directions:In a blender, blend the lemon juice, water, strawberries with juice, sugar and ice cubes until slushy. Serve in a tall glass with
a straw.
Nutritional Information per Serving: Calories: 130 Total Fat: 0.1gCholesterol: 0mg
By Ashley Acornley MS, RD, LDN
MEDMONTHLY.COM |51

SOMETIMES, THE GAME THEY LOVEDOESN’T LOVE THEM BACK.More and more, young athletes are focusing on a single sport and training for that sport year-round — a practice that’s led to an increase in Overuse Injuries. Left untreated, overuse traumato young shoulders, elbows, knees and wrists may require surgery and have lifelong consequences. For information on preventing and treating Overuse Injuries, visit these sites:
orthoinfo.org stopsportsinjuries.org
overuse8.5x11.indd 1 12/1/11 8:47 AM
MEDMONTHLY.COM |53
U.S. OPTICAL BOARDSAlaskaP.O. Box 110806Juneau, AK 99811(907)465-5470http://www.dced.state.ak.us/occ/pdop.htm
Arizona1400 W. Washington, Rm. 230Phoenix, AZ 85007(602)542-3095http://www.do.az.gov
ArkansasP.O. Box 627Helena, AR 72342(870)572-2847
California2005 Evergreen St., Ste. 1200Sacramento, CA 95815(916)263-2382www.medbd.ca.gov
Colorado1560 Broadway St. #1310Denver, CO 80202(303)894-7750www.dph.state.ct.us
Connecticut410 Capitol Ave., MS #12APPP.O. Box 340308Hartford, CT 06134(860)509-7603 ext. 4http://www.dph.state.ct.us/
Florida4052 Bald Cypress Way, Bin C08Tallahassee, FL 32399(850)245-4474doh.state.fl.us
Georgia237 Coliseum Dr.Macon, GA 31217(478)207-1671www.sos.state.ga.us
HawaiiP.O. Box 3469Honolulu, HI 96801(808)[email protected]
Idaho450 W. State St., 10th FloorBoise , ID 83720(208)334-5500 www2.state.id.us/dhw
KentuckyP.O. Box 1360Frankfurt, KY 40602(502)564-3296http://1.usa.gov/xMFQAK
Massachusetts239 Causeway St.Boston, MA 02114(617)727-5339http://1.usa.gov/zbJVt7
NevadaP.O. Box 70503Reno, NV 89570(775)853-1421http://nvbdo.state.nv.us/
New Hampshire129 Pleasant St.Concord, NH 03301(603)271-5590www.state.nh.us
New JerseyP.O. Box 45011Newark, NJ 07101(973)504-6435http://bit.ly/wLM20Y
New York89 Washington Ave., 2nd Floor W.Albany, NY 12234(518)[email protected]
North CarolinaP.O. Box 25336Raleigh, NC 27611(919)733-9321http://www.ncoptometry.org/
Ohio77 S. High St.Columbus, OH 43266(614)466-9707http://optical.ohio.gov/
Oregon3218 Pringle Rd. SE Ste. 270Salem, OR 97302(503)373-7721 www.obo.state.or.us
Rhode Island3 Capitol Hill, Rm 104Providence, RI 02908(401)222-7883www.health.state.ri.us
South CarolinaP.O. Box 11329Columbia, SC 29211(803)896-4665www.llr.state.sc.us
TennesseeHeritage Place Metro Center227 French Landing, Ste. 300Nashville, TN 37243(615)253-6061 www2.state.tn.us/health
TexasP.O. Box 149347Austin, TX 78714(512)834-6661www.roatx.org
Vermont National Life Bldg N FL. 2 Montpelier, VT 05620(802)828-2191www.vtprofessionals.org
Virginia3600 W. Broad St.Richmond, VA 23230(804)367-8500www.state.va.us/licenses
Washington300 SE Quince P.O. Box 47870Olympia, WA 98504(360)236-4947www.doh.wa.gov

U.S. DENTAL BOARDSAlabamaAlabama Board of Dental Examiners 5346 Stadium Trace Pkwy., Ste. 112 Hoover, AL 35244(205) 985-7267http://www.dentalboard.org/
AlaskaP.O. Box 110806Juneau, AK 99811-0806(907)465-2542http://bit.ly/uaqEO8
Arizona4205 N. 7th Ave. Suite 300Phoenix, AZ 85103(602)242-1492http://azdentalboard.us/ Arkansas101 E. Capitol Ave., Suite 111Little Rock, AR 72201(501)682-2085http://www.asbde.org/
California2005 Evergreen Street, Suite 1550 Sacramento, CA 95815877-729-7789http://www.dbc.ca.gov/
Colorado1560 Broadway, Suite 1350Denver, CO 80202(303)894-7800http://www.dora.state.co.us/dental/
Connecticut410 Capitol Ave. Hartford, CT 06134(860)509-8000http://www.ct.gov/dph/site/default.asp
DelawareCannon Building, Suite 203861 Solver Lake Blvd.Dover, DE 19904(302)744-4500http://1.usa.gov/t0mbWZ
Florida4052 Bald Cypress WayBin C-08Tallahassee, FL 32399 (850)245-4474http://bit.ly/w1m4MI
Georgia237 Coliseum DriveMacon, GA 31217(478)207-2440http://sos.georgia.gov/plb/dentistry/
HawaiiDCCA-PVLAtt: DentalP.O. Box 3469Honolulu, HI 96801(808)586-3000http://1.usa.gov/s5Ry9i
IdahoP.O. Box 83720Boise, ID 83720(208)334-2369http://isbd.idaho.gov/
Illinois320 W. Washington St.Springfield, IL 62786(217)785-0820http://bit.ly/svi6Od
Indiana402 W. Washington St., Room W072Indianapolis, IN 46204(317)232-2980http://www.in.gov/pla/dental.htm
Iowa400 SW 8th St. Suite DDes Moines, IA 50309(515)281-5157http://www.state.ia.us/dentalboard/
Kansas900 SW Jackson Room 564-STopeka, KS 66612(785)296-6400http://www.accesskansas.org/kdb/
Kentucky312 Whittington Parkway, Suite 101Louisville, KY 40222(502)429-7280http://dentistry.ky.gov/
Louisiana365 Canal St., Suite 2680New Orleans, LA 70130(504)568-8574http://www.lsbd.org/
Maine143 State House Station161 Capitol St.Augusta, ME 04333(207)287-3333http://www.mainedental.org/
Maryland55 Wade Ave.Catonsville, Maryland 21228(410)402-8500http://dhmh.state.md.us/dental/
Massachusetts1000 Washington St., Suite 710Boston, MA 02118(617)727-1944www.mass.gov
MichiganP.O. Box 30664Lansing, MI 48909(517)241-2650www.michigan.gov
Minnesota2829 University Ave., SE. Suite 450Minneapolis, MN 55414(612)617-2250http://www.dentalboard.state.mn.us/
Mississippi600 E. Amite St., Suite 100Jackson, MS 39201(601)944-9622http://bit.ly/uuXKxl
Missouri3605 Missouri Blvd.P.O. Box 1367Jefferson City, MO 65102(573)751-0040http://pr.mo.gov/dental.asp
MontanaP.O. Box 200113Helena, MT 59620(406)444-2511http://mt.gov/
Nebraska301 Centennial Mall SouthLincoln, NE 68509(402)471-3121http://bit.ly/uBEqwK
54 | JUNE 2012

Oklahoma201 N.E. 38th Terr., #2Oklahoma City, OK 73105(405)524-9037http://www.dentist.state.ok.us/
Oregon1600 SW 4th Ave. Suite 770Portland, OR 97201(971)673-3200http://www.oregon.gov/Dentistry/
PennsylvaniaP.O. Box 2649Harrisburg, PA 17105(717)783-7162http://bit.ly/s5oYiS
Rhode IslandDept. of HealthThree Capitol Hill, Room 104Providence, RI 02908(401)222-2828http://1.usa.gov/u66MaB
South CarolinaP.O. Box 11329Columbia, SC 29211(803)896-4599http://www.llr.state.sc.us/POL/Dentistry/ South DakotaP.O. Box 1079105. S. Euclid Ave. Suite CPierre, SC 57501(605)224-1282https://www.sdboardofdentistry.com/
Tennessee 227 French Landing, Suite 300Nashville, TN 37243(615)532-3202http://health.state.tn.us/boards/dentistry/
Texas333 Guadeloupe St. Suite 3-800Austin, TX 78701(512)463-6400http://www.tsbde.state.tx.us/
Utah160 E. 300 SouthSalt Lake City, UT 84111(801)530-6628http://1.usa.gov/xMVXWm
VermontNational Life BuildingNorth FL2Montpelier, VT 05620(802)828-1505http://bit.ly/zSHgpa
VirginiaPerimeter Center9960 Maryland Dr., Suite 300Henrico, VA 23233(804)367-4538http://bit.ly/zDkIU2
Washington310 Israel Rd. SEP.O. Box 47865Olympia, WA 98504(360)236-4700http://1.usa.gov/tKBFHT West Virginia1319 Robert C. Byrd Dr.P.O. Box 1447Crab Orchard, WV 258271-877-914-8266http://www.wvdentalboard.org/
WisconsinP.O. Box 8935Madison, WI 537081(877)617-1565http://bit.ly/sEhr0Q Wyoming1800 Carey Ave., 4th FloorCheyenne, WY 82002(307)777-6529http://plboards.state.wy.us/dental/index.asp
MEDMONTHLY.COM |55
Nevada6010 S. Rainbow Blvd. Suite A-1Las Vegas, NV 89118(702)486-7044http://www.nvdentalboard.nv.gov/
New Hampshire2 Industrial Park Dr. Concord, NH 03301(603)271-4561http://www.nh.gov/dental/
New JerseyP.O Box 45005Newark, NJ 07101(973)504-6405http://bit.ly/uO2tLg New MexicoToney Anaya Building2550 Cerrillos Rd.Santa Fe, NM 87505(505)476-4680http://bit.ly/vCnCP4
New York89 Washington Ave.Albany, NY 12234(518)474-3817http://www.op.nysed.gov/prof/dent/
North Carolina507 Airport Blvd., Suite 105Morrisville, NC 27560(919)678-8223http://www.ncdentalboard.org/
North DakotaP.O. Box 7246Bismark, ND 58507(701)258-8600http://www.nddentalboard.org/
OhioRiffe Center77 S. High St.,17th FloorColumbus, OH 43215(614)466-2580http://www.dental.ohio.gov/

AlabamaP.O. Box 946 Montgomery, AL 36101 (334)242-4116http://www.albme.org/
Alaska550 West 7th Ave., Suite 1500Anchorage, AK 99501(907)269-8163http://bit.ly/zZ455T
Arizona9545 E. Doubletree Ranch Rd. Scottsdale, AZ 85258(480)551-2700http://www.azmd.gov
Arkansas1401 West Capitol Ave., Suite 340Little Rock, AR 72201(501)296-1802http://www.armedicalboard.org/
California2005 Evergreen St., Suite 1200Sacramento, CA 95815(916)263-2382 http://www.mbc.ca.gov/
Colorado1560 Broadway, Suite 1350Denver, CO 80202(303)894-7690http://www.dora.state.co.us/medical/
Connecticut401 Capitol Ave. Hartford, CT 06134(860)509-8000http://www.ct.gov/dph/site/default.asp
DelawareDivision of Professional Regulation Cannon Building 861 Silver Lake Blvd., Suite 203 Dover, DE 19904(302)744-4500http://dpr.delaware.gov/
District of Columbia899 North Capitol St., NE Washington, DC 20002 (202)442-5955http://www.dchealth.dc.gov/doh
Florida2585 Merchants Row Blvd.Tallahassee, FL 32399(850)245-4444http://www.doh.state.fl.us/
Georgia2 Peachtree Street NW, 36th Floor Atlanta, GA 30303 (404)656-3913http://bit.ly/vPJQyG
HawaiiDCCA-PVL P.O. Box 3469 Honolulu, HI 96801(808)587-3295http://hawaii.gov/dcca/pvl/boards/medical/
IdahoIdaho Board of Medicine P.O. Box 83720 Boise, Idaho 83720(208)327-7000http://bit.ly/orPmFU
Illinois 320 West Washington St. Springfield, IL 62786(217)785 -0820http://www.idfpr.com/
Indiana402 W. Washington St. #W072Indianapolis, IN 46204(317)233-0800http://www.in.gov/pla/
Iowa400 SW 8th St., Suite C Des Moines, IA 50309(515)281-6641http://medicalboard.iowa.gov/
Kansas800 SW Jackson, Lower Level, Suite ATopeka, KS 66612(785)296-7413http://www.ksbha.org/
Kentucky310 Whittington Pkwy., Suite 1B Louisville, KY 40222(502)429-7150http://kbml.ky.gov/default.htm
LouisianaLSBMEP.O. Box 30250New Orleans, LA 70190(504)568-6820http://www.lsbme.la.gov/
Maine161 Capitol Street 137 State House Station Augusta, ME 04333 (207)287-3601http://bit.ly/hnrzp
Maryland4201 Patterson Ave.Baltimore, MD 21215(410)764-4777http://www.mbp.state.md.us/
Massachusetts200 Harvard Mill Sq., Suite 330 Wakefield, MA 01880 (781)876-8200http://www.mass.gov
MichiganBureau of Health Professions P.O. Box 30670 Lansing, MI 48909(517)335-0918http://www.michigan.gov/lara
MinnesotaUniversity Park Plaza 2829 University Ave. SE, Suite 500 Minneapolis, MN 55414 (612)617-2130 http://bit.ly/pAFXGq
Mississippi1867 Crane Ridge Drive, Suite 200-B Jackson, MS 39216(601)987-3079http://www.msbml.state.ms.us/
MissouriMissouri Division of Professional Registration 3605 Missouri Blvd. P.O. Box 1335 Jefferson City, MO 65102 (573)751-0293 http://pr.mo.gov/
U.S. MEDICAL BOARDS
56 | JUNE 2012

Montana301 S. Park Ave. #430Helena, MT 59601(406)841-2300http://bit.ly/obJm7J p
NebraskaNebraska Department of Health and Human ServicesP.O. Box 95026Lincoln, NE 68509(402)471-3121http://www.hhs.state.ne.us/
NevadaBoard of Medical ExaminersP.O. Box 7238Reno, NV 89510 (775)688-2559 http://www.medboard.nv.gov/
New HampshireNew Hampshire State Board of Medicine 2 Industrial Park Dr. #8 Concord, NH 03301 (603)271-1203http://www.nh.gov/medicine/
New JerseyP. O. Box 360Trenton, NJ 08625 (609)292-7837http://bit.ly/w5rc8J
New Mexico2055 S. Pacheco St. Building 400 Santa Fe, NM 87505 (505)476-7220http://www.nmmb.state.nm.us/
New YorkOffice of the ProfessionsState Education Building, 2nd FloorAlbany, NY 12234(518)474-3817http://www.op.nysed.gov/
North CarolinaP.O. Box 20007Raleigh, NC 27619(919)326-1100http://www.ncmedboard.org/
North Dakota418 E. Broadway Ave., Suite 12Bismarck, ND 58501(701)328-6500http://www.ndbomex.com/
Ohio30 E. Broad St., 3rd FloorColumbus, OH 43215(614)466-3934http://med.ohio.gov/
OklahomaP.O. Box 18256 Oklahoma City, OK 73154(405)962-1400http://www.okmedicalboard.org/
Oregon1500 SW 1st Ave., Suite 620Portland, OR 97201(971)673-2700http://www.oregon.gov/OMB/
Pennsylvania P.O. Box 2649 Harrisburg, PA 17105 (717)787-8503 http://bit.ly/havKVj
Rhode Island3 Capitol HillProvidence, RI 02908(401)222-5960http://1.usa.gov/xgocXV
South CarolinaP.O. Box 11289Columbia, SC 29211(803)896-4500http://www.llr.state.sc.us/pol/medical/
South Dakota101 N. Main Ave. Suite 301Sioux Falls, SD 57104(605)367-7781http://www.sdbmoe.gov/
Tennessee425 5th Ave. NorthCordell Hull Bldg. 3rd FloorNashville, TN 37243(615)741-3111http://health.state.tn.us/
TexasP.O. Box 2018Austin, TX 78768(512)305-7010http://bit.ly/rFyCEW
UtahP.O. Box 146741 Salt Lake City, UT 84114(801)530-6628http://www.dopl.utah.gov/
VermontP.O. Box 70Burlington, VT 05402(802)657-4220http://1.usa.gov/wMdnxh
VirginiaVirginia Dept. of Health ProfessionsPerimeter Center9960 Maryland Dr., Suite 300Henrico, VA 23233(804)367-4400http://1.usa.gov/xjfJXK
WashingtonPublic Health Systems DevelopmentWashington State Department of Health101 Israel Rd. SE, MS 47890Tumwater, WA 98501(360)236-4085http://www.doh.wa.gov/PHIP/default.htm
West Virginia101 Dee Dr., Suite 103Charleston, WV 25311(304)558-2921http://www.wvbom.wv.gov/
WisconsinP.O. Box 8935Madison, WI 53708(877)617-1565http://drl.wi.gov/section.asp?linkid=6&locid=0
Wyoming320 W. 25th St., Suite 200Cheyenne, WY 82002(307)778-7053http://wyomedboard.state.wy.us/
MEDMONTHLY.COM |57

medical resource guide
1-800-Urgent-Care6881 Maple Creek Blvd, Suite 100West Bloomfield, MI 48322-4559(248)819-6838
www.ringringllc.com
Find Urgent CarePO Box 15130Scottsdale, AZ 85267(602)370-0303
www.findurgentcare.com
MedMedia9PO Box 98313Raleigh, NC 27624(919)747-9031
www.medmedia9.com
Ring Ring LLC6881 Maple Creek Blvd, Suite 100West Bloomfield, MI 48322-4559(248)819-6838
www.ringringllc.com
ADVERTISING
BILLING & COLLECTION
Advanced Physician Billing, LLCPO Box 730Fishers, IN 46038(866)459-4579
www.advancedphysicianbillingllc.com
58| JUNE 2012
ANSWERING SERVICES
Corridor Medical Answering Service3088 Route 27, Suite 7Kendall Park, NJ 08824(866)447-5154
www.corridoranswering.net
Docs on Hold14849 West 95th St. Lenexa, KS 66285(913)559-3666
www.soundproductsinc.com
CODING SPECIALISTS
The Coding Institute LLC2222 Sedwick DriveDurham, NC 27713(800)508-2582
http://www.codinginstitute.com/
CAREER CONSULTING
Doctor’s Crossing4107 Medical Parkway, Suite 104 Austin, Texas 78756 (512)517-8545
http://doctorscrossing.com/
COMPUTER, SOFTWARE
American Medical Software1180 Illinois 157Edwardsville, IL 62025(618) 692-1300
www.americanmedical.com
CDWG300 N. Milwaukee AveVernon Hills, IL 60061(866)782-4239
www.cdwg.com/
Instant Medical History4840 Forest Drive #349Columbia, SC 29206(803)796-7980
www.medicalhistory.com
SEAK Non-Clinical Careers ConferenceOct. 21-22, 2012 in Chicago, IL(508)457-1111
www.nonclinicalcareers.com
ACCOUNTING
Boyle CPA, PLLC3716 National Drive, Suite 206Raleigh, NC 27612(919) 720-4970
www.boyle-cpa.com
Ajishra Technology Support3562 Habersham at Northlake, Bldg JTucker, GA 30084(866)473-0011
www.ajishra.com
Applied Medical Services4220 NC Hwy 55, Suite 130BDurham, NC 27713(919)477-5152
www.ams-nc.com
Axiom Business Solutions4704 E. Trindle Rd.Mechanicsburg, PA 17050(866)517-0466
www.axiom-biz.com
Frost Arnett480 James Robertson ParkwayNashville, TN 37219(800)264-7156
www.frostarnett.com
Gold Key Credit, Inc.PO Box 15670Brooksville, FL 34604888-717-9615
www.goldkeycreditinc.com
Horizon Billing Specialists4635 44th St., Suite C150Kentwood, MI 49512(800)378-9991
www.horizonbilling.com
Management Services On-Call200 Timber Hill Place, Suite 221Chapel Hill, NC 27514(866)347-0001
www.msocgroup.com
Marina Medical Billing Service18000 Studebaker Road4th FloorCerritos, CA 90703(800)287-8166
www.marinabilling.com
Mediserv6451 Brentwood Stair Rd.Ft. Worth, TX 76112(800)378-4134
www.mediservltd.com
Practice Velocity1673 Belvidere RoadBelvidere, IL 61008(888)357-4209
www.practicevelocity.com
Sweans Technologies501 Silverside Rd.Wilmington, DE 19809(302)351-3690
www.medisweans.com
VIP BillingPO Box 1350Forney, TX 75126(214)499-3440
www.vipbilling.com

ELECTRONIC MED. RECORDSINSURANCE, MED. LIABILITY
medical resource guide
FINANCIAL CONSULTANTS
Sigmon Daknis Wealth Management701 Town Center Dr. , Ste. #104Newport News, VA 23606(757)223-5902
www.sigmondaknis.com
Sigmon & DaknisWilliamsburg, VA Office325 McLaws Circle, Suite 2Williamsburg, VA 23185 (757)258-1063
http://www.sigmondaknis.com/
MEDMONTHLY.COM |59
Biomet 3i4555 Riverside Dr.Palm Beach Gardens, FL 33410(800)342-5454
www.biomet3i.com
Dental Management Club4924 Balboa Blvd #460Encino, CA 91316
www.dentalmanagementclub.com
ABELSoft1207 Delaware Ave. #433Buffalo, NY 14209(800)267-2235
www.abelmedicalsoftware.com
Acentec, Inc17815 Sky Park Circle , Suite JIrvine, CA 92614(949)474-7774
www.acentec.com
AdvanceMD 10011 S. Centennial PkwySandy, UT 84070(800) 825-0224
www.amdsoftware.com
CollaborateMD201 E. Pine St. #1310Orlando, FL 32801(888)348-8457
www.collaboratemd.com
DocuTAP4701 W. Research Dr. #102Sioux Falls, SD 57107-1312(877)697-4696
www.docutap.com
Integritas, Inc.2600 Garden Rd. #112Monterey, CA 93940(800)458-2486
www.integritas.com
Aquesta Insurance Services, Inc.Michael W. Robertson3807 Peachtree Avenue, #103Wilmington, NC 28403Work: (910) 794-6103Cell: (910) 777-8918
www.aquestainsurance.com
Jones Insurance 820 Benson Rd. Garner, North Carolina 27529 (919) 772-0233
www.Jones-insurance.com
Medical Protective5814 Reed Rd.Fort Wayne, In 46835(800)463-3776
MGIS, Inc.1849 W. North TempleSalt Lake City, UT 84116(800)969-6447
www.mgis.com
Professional Medical Insurance Services16800 Greenspoint Park DriveHouston, TX 77060(877)583-5510
www.promedins.com
Wood Insurance Group4835 East Cactus Rd., #440Scottsdale, AZ 85254-3544(602)230-8200
www.woodinsurancegroup.com
Manage My Practice103 Carpenter Brook Dr.Cary, NC 27519(919)370-0504
www.managemypractice.com
myEMRchoice.com24 Cherry LaneDoylestown, PA 18901(888)348-1170
www.myemrchoice.com
Urgent Care America17595 S. Tamiami TrailFort Meyers, FL 33908(239)415-3222
www.urgentcareamerica.com
Medical Practice Listings8317 Six Forks Rd. Suite #205Raleigh, NC 27624(919)848-4202
www.medicalpracticelistings.com
Utilization [email protected](919) 289-9126
www.pushpa.bizMedical Credentialing(800) 4-THRIVE
www.medicalcredentially.org
Synapse Medical Management18436 Hawthorne Blvd. #201Torrance, CA 90504(310)895-7143
www.synapsemgmt.com
DENTAL
The Dental Box Company, Inc.PO Box 101430Pittsburgh, PA 15237(412)364-8712
www.thedentalbox.com
Dentistry’s Business Secrets9016 Phoenix ParkwayO’Fallon, MO 63368(636)561-5445
www.dentistrysbusinesssecrets.com
Modern Dental Marketing Practices504 N. Oak St. #6Roanoke, TX 76262(940)395-5115
www.moderndentalmarketing.com
CONSULTING SERVICES,PRACTICE MANAGEMENT

60| JUNE 2012
medical resource guide
LOCUM TENENS
MEDICAL ART
Brian Allenwww.artisanprinter.com
Deborah Brenner877 Island Ave #315San Diego, CA 92101(619)818-4714
www.deborahbrenner.com
Martha Petty316 Burlage CircleChapel Hill, NC 27514(919)933-4920
www.marthapetty.com
Julie Jennings(678)[email protected]
http://silksynergy.com/http://www.coroflot.com/naddie09
Eduardo Lapetina318 North Estes DriveChapel Hill, NC 27514(919)960-3400
eduardolapetina.com/index.shtml
Marianne Mitchell(215)704-3188
http://www.mariannemitchell.comhttp://www.colordrop.blogspot.com
Nicholas Downhttp://bit.ly/yHwxb0
Barry Hanshaw 18 Bay Path DriveBoylston MA 01505508 - 869 - [email protected]
www.barryhanshaw.com
Pia De Girolamowww.piadegirolamo.com
MEDICAL EQUIPMENT
ALLPRO Imaging1295 Walt Whitman RoadMelville, NY 11747(888)862-4050
www.allproimaging.com
Biosite, Inc9975 Summers Ridge RoadSan Diego, CA 92121(858)805-8378
www.biosite.com
Cryopen800 Shoreline, #900Corpus Christi, TX 78401(888)246-3928
www.cryopen.com
Carolina Liquid Chemistries, Inc.391 Technology WayWinston Salem, NC 27101(336)722-8910
www.carolinachemistries.com
Dicom Solutions548 WaldIrvine, CA 92618(800)377-2617
www.dicomsolutions.com
Tarheel Physicians Supply1934 Colwell Ave. Wilmington, NC 28403 (800)672-0441
www.thetps.com
MEDICAL PRACTICE SALES
Medical Practice Listings8317 Six Forks Rd. Ste #205Raleigh, NC 27624(919)848-4202
www.medicalpracticelistings.com
MEDICAL RESEARCH
BizScorePO Box 99488Raleigh, NC 27624(919)846-4747
www.bizscorevaluation.com
Arup Laboratories500 Chipeta WaySalt Lake City, UT 84108(800)242-2787
www.aruplab.com
Chimerix, Inc.2505 Meridian Parkway, Suite 340Durham, NC 27713(919) 806-1074
www.chimerix.com
Clinical Reference Laboratory8433 Quivira Rd.Lenexa, KS 66215(800)445-6917
www.crlcorp.comPeters Medical Research507 N. Lindsay St., 2nd FloorHigh Point, NC 27262
www.Petersmedicalresearch.com
Sanofi US55 Corporate DriveBridgewater, NJ 08807(800) 981-2491
www.sanofi.us
Scynexis, Inc.3501 C Tricenter Blvd.Durham, NC 27713(919) 933-4990
www.scynexis.com
MEDICAL PRACTICE VALUATIONS
MEDICAL MARKETING
MedMedia9PO Box 98313Raleigh, NC 27624(919)747-9031
www.medmedia9.com
WhiteCoat DesignsWeb, Print & Marketing Solutions for Doctors(919)714-9885
www.whitecoat-designs.com
Physician SolutionsPO Box 98313Raleigh, NC 27624(919)845-0054
www.physiciansolutions.com

Triangle Nutrition Therapy6200 Falls of Neuse Road, Suite 200Raleigh, NC 27609(919)876-9779
http://trianglediet.com/
NUTRITION THERAPIST
medical resource guide
Additional Staffing Group, Inc.8319 Six Forks Rd, Suite 103Raleigh, NC 27615(919) 844-6601
Astaffinggroup.com
SUPPLIES, GENERAL
BSN Medical5825 Carnegie BoulevardCharlotte, NC 28209(800)552-1157
www.bsnmedical.us CNF Medical1100 Patterson AvenueWinston Salem, NC 27101(877)631-3077
www.cnfmedical.com
STAFFING COMPANIESDermabondEthicon, Route 22 WestSomerville, NJ 08876(877)984-4266
www.dermabond.com DJO1430 Decision St.Vista, CA 92081(760)727-1280
www.djoglobal.com ExpertMed31778 Enterprise Dr.Livonia, MI 48150(800)447-5050
www.expertmed.com
Gebauer Company4444 East 153rd St. Cleveland, OH 44128-2955(216)581-3030
www.gebauerspainease.comScarguard15 Barstow Rd.Great Neck, NY 11021(877)566-5935
www.scarguard.com
MEDMONTHLY.COM |61
Is Your Practice Well Managed?Take the Test and Find out...
Manage My Practice is the go-to online source of technology, information and resources for
practice management professionals, and it is visited by over 20,000 medical-practice
managers and medical providers each month.
❏ Yes ❏ No Are your foundation documents in place & reviewed bi-annually?
❏ Yes ❏ No Do owners & management have monthly meetings?
❏ Yes ❏ No Do management & staff have monthly meetings?
❏ Yes ❏ No Do you have a compliance plan?
❏ Yes ❏ No Is your net collection percentage greater than 95%?
❏ Yes ❏ No Are your budget variances addressed monthly?
❏ Yes ❏ No Is your unfilled/no-show appointment percentage less than 5%?
❏ Yes ❏ No Do you have a written marketing plan?
❏ Yes ❏ No Is employee turnover rate is less than 10%?
❏ Yes ❏ No Do your management reports track and trend key performance indicators?
❏ Yes ❏ No Do you use Process Improvement (PI) to address negative trends?
❏ Yes ❏ No Is patient satisfaction measured and prioritized for improvement of the practice?
If you’ve answered “No” to one or more of these questions, then you need to...
❏ Call Manage My Practice(919) 370-0504or go online at ManageMyPractice.com
✔
Careers | Customer Service | Day-to-Day Operations | Electronic Medical Records | Finance | Human Resources | Innovation | Leadership | Marketing | Medicare & Reimbursement | Social Media
REAL ESTATE
York Properties, Inc.Headquarters & Property Management 1900 Cameron StreetRaleigh, NC 27605(919) 821-1350
Commercial Sales & Leasing (919) 821-7177
www.yorkproperties.com

Buying Bene�tsAccurate practice pricingDetailed reports and �nancialsLargest selection of health care facilitiesWork one-on-one with an experienced team of quali�ed professionals
medicalpracticelistings.comA Philip Driver Company
Maintain con�dentialityProfessional representationNational and regional marketingMaximize your practice valueBizScore Valuation assessment
Listing Bene�ts
Medical Practice Listings
•
•
••
•
•
••
•
Buying or selling? We can help!
Scan this QR code with your smartphone to learn more

North Carolina North Carolina (cont.)Occupational Health Care Practice in Fayetteville North Carolina has two to five days of locums work per week. Send copies of your CV, NC medical license, DEA certifi-cate and NPI certificate with number to Physician Solu-tions for immediate consideration. Physician Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054, email: [email protected]
Occupation Health Care Practice located in Greensboro, NC has an immediate opening for a primary care physi-cian. This is 40 hours per week opportunity with a base salary of $135,000 plus incentives, professional liability insurance and an excellent CME, vacation and sick leave package. Send copies of your CV, NC medical license, DEA certificate and NPI certificate with number to Physi-cian Solutions for immediate consideration. Physician Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054, email: [email protected] Family Practice physician opportunity in Raleigh, NC This is a locum’s position with three to four shifts per week require-ment that will last for several months. You must be BC/BE and comfortable treating patients from one year of age to geriatrics. You will be surrounded by an exceptional, experienced staff with beautiful offices and accommoda-tions. No call or hospital rounds. Send copies of your CV, NC medical license, DEA certificate and NPI certificate with number to Physician Solutions for immediate consideration. Physician Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054, email: [email protected] Methadone Treatment Center located near Charlotte, NC has an opening for an experienced physician. You must be comfortable in the evaluation and treatment within the guidelines of a highly regulated environment. Practice operating hours are 6 a.m. till 3 p.m. Monday through Friday. Send copies of your CV, NC medical license, DEA certificate and NPI certificate with number to Physician Solutions for immediate consideration. Physi-cian Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054,email: [email protected] Immediate Full-Time Opportunity for Board Certified occupational health care MD in Greensboro, NC. Excel-lent working environment, wage and professional liability insurance provided. Send copies of your CV, NC medical license, DEA certificate and NPI certificate with number to Physician Solutions for immediate consideration. Physician Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054, email: [email protected]
Physicians needed Physicians needed
To place a classified ad, call 919.747.9031
classified listings
Classified
MEDMONTHLY.COM |63
Cardiology Practice located in High Point, NC has an opening for a board certified cardiovascular physi-cian. This established and beautiful facility offers the ideal setting for an enhanced lifestyle. There is no hospital call or invasive procedures. Look into join-ing this three physician facility and live the good life in one of North Carolina’s most beautiful cities. Send copies of your CV, NC medical license, DEA certificate and NPI certificate with number to Physician Solutions for immediate consideration. Physician Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054, email: [email protected]
Board Certified Internal Medicine physician position is available in the Greensboro, NC area. This is an out-pa-tient opportunity within a large established practice. The employment package contains salary plus incentives. Please send a copy of your current CV, NC medical license, DEA certificate and NPI certificate with number along with your detailed work history and CME courses completed to: Physician Solutions, P.O. Box 98313, Ra-leigh, NC 27624. email: [email protected] or phone with any questions, PH: (919) 845-0054.
Family Practice physician is needed to cover several shifts per week in Rocky Mount, NC. This high profile practice treats pediatrics, women’s health and primary care patients of all ages. If you are available for 30 plus hours per week for the remainder of the year, this could be the perfect opportunity. Send copies of your CV, NC medical license, DEA certificate and NPI certificate with number to Physician Solutions for immediate con-sideration. Physician Solutions, P.O. Box 98313, Raleigh, N.C. 27624, and PH: (919) 845-0054, email: [email protected]
Locum Tenens opportunity for primary care MD in the Triad Area NC. This is a 40 hour per week on-going as-signment in a fast pace established practice. You must be comfortable treating pediatrics to geriatrics. We pay top wages, provide professional liability insurance, lodging when necessary, mileage and exceptional op-portunities. Please send a copy of your current CV, NC medical license, DEA certificate and NPI certificate with number along with your detailed work history and CME courses completed to: Physician Solutions, P.O. Box 98313, Raleigh, NC 27624. email: [email protected] or phone with any questions, PH: (919) 845-0054.
Buying Bene�tsAccurate practice pricingDetailed reports and �nancialsLargest selection of health care facilitiesWork one-on-one with an experienced team of quali�ed professionals
medicalpracticelistings.comA Philip Driver Company
Maintain con�dentialityProfessional representationNational and regional marketingMaximize your practice valueBizScore Valuation assessment
Listing Bene�ts
Medical Practice Listings
•
•
••
•
•
••
•
Buying or selling? We can help!
Scan this QR code with your smartphone to learn more

Primary Care Practice for SaleHickory, North Carolina
The owning physician is retiring, creating an excellent opportunity for a progressive buyer.
There are two full-time physician assistants that see the majority of the patients which averages
between 45 to 65 per day.
There is lots of room to grow this already solid practice that has a yearly gross of $1,500,00.
You will be impressed with this modern and highly visible
practice.
Call for pricing and details.
Call Medical Practice Listings at (919) 848-4202 for details and to view our other listings vist www.medicalpracticelistings.com
Established primary care practice in the beautiful foothills of North Carolina
Ophthalmic and Neuro-Ophthalmic PracticeRaleigh North Carolina
This is a great opportunity to purchase an established ophthalmic practice in the heart of Raleigh. Locate on a major road with established clients and plenty of room for growth; you will appreciate the upside this practice offers. This practice performs comprehensive ophthalmic and neuro-ophthalmic exams with diagnosis and treatment of eye disease of all ages.
Surgical procedures include no stitch cataract surgery, la-ser treatment for glaucoma and diabetic eye disease. This practice offers state-of-the-art equipment and offer you the finest quality optical products with contact lens fitting and follow-up care & frames for all ages.
List Price: $75,000 | Gross Yearly Income: $310,000
Contact Cara or Philip 919-848-4202 for more information or visit MedicalPracticeListings.com
64| JUNE 2012

Ask your patients about their health priorities at each visit. When you do, both you and your patient can make the most out of the time you have together, and they’ll feel more invested in their own care. Not only does that improve efficiencies, but it also helps improve health outcomes.
For tools and tips to share with your patients, visit www.ahrq.gov/questions
“WHAT ARE OUR GOALS FOR TODAY?”
A simple question can reveal as much as a test.

North Carolina family practice located 30 miles from Lake Norman has everything going for it.
Gross revenues in 2010 were 1.5 million, and there is even more upside. The retiring physician is willing to continue to practice for several months while the new owner gets established.
Excellent medical equipment, staff and hospital nearby, you will be hard-pressed to find a family practice achieving these numbers.
Listing price is $625,000.
Medical Practice Listings For more information call
(919) 848-4202. To view other practice listings visit medicalpracticelistings.com
EXCELLENT FAMILY PRACTICE FOR SALE
Urgent care practice wanted in North Carolina.
Qualified physician is seeking to purchase an established urgent care within 100 miles of Raleigh, North Carolina. If you are considering retiring, relocations or closing your practice for personal reasons, contact us for a confidential discussion regarding your urgent care. You will receive cash at closing and not be required to carry a note.
Wanted:Urgent Care Practice
Call 919-848-4202 or e-mail [email protected]
Medical Practice ListingsBuying and selling made easy
Wanted:
To view our national listings visitwww.medicalpracticelistings.com
Hospice Practice in Dallas, TX
We have a qualified buyer that is looking for an established hospice practice in the Dallas,Texas area. To review your hospice practice options confidentially, contact
Medical Practice Listings at 919-848-4202 or e-mail us at
Pediatrics practice wanted in NCConsidering your options regarding your pediatric prac-tice? We can help. Medical Practice Listings has a well qualified buyer for a pediatric practice anywhere in central North Carolina.
Contact us today to discuss your options confidentially.
Pediatrics Practice Wanted
Medical Practice ListingsCall 919-848-4202 or e-mail [email protected]
www.medicalpracticelistings.com
66| JUNE 2012

MEDMONTHLY.COM |67
Wilmington, NC
Established primary care on the coast of North Carolina’s beautiful beaches. Fully staffed with MD’s and PA’s to treat both appointment and walk-in patients. Excellent exam room layout, equipment and visibility.
Contact Medical Practice Listings for more information.
Primary Care Practice For Sale
Medical Practice Listings919.848.4202 | [email protected]
www.medicalpracticelistings.com
Established North Carolina Primary Care practice only 15 minutes from Fayetteville, 30 minutes from Pinehurst, 1 hour from Ra-leigh, 15 minutes from Lumberton and about an hour from Wilm-ington. The population within 1 hour of this beautiful practice is over one million. The owning physician is retiring and the new owner will benefit from his exceptional health care, loyal patient following, professional decorating, beautiful and modern free standing medical building with experienced staff. The gross revenue for 2010 is $856,000, and the practice is very profitable. We have this practice listed for $415,000. Call today for more details and information regarding the medical building. Our Services:• Primary Health• Well Child Health Exams• Sport Physical• Adult Health Exams• Women’s Health Exams• Management of Contraception• DOT Health Exam• Treatment & Management of Medical Conditions• Counseling on Prevention of Preventable Diseases• Counseling on Mental Health• Minor surgical Procedures
Exceptional North Carolina Primary Care Practice for Sale
For more information call Medical Practice Listing at (919) 848-4202. To view our other listings, visit medicalpracticelistings.com.
We understand that most physicians cannot take valuable time away from seeing patients and managing their day-to-day operations of their practice to think about real estate. For over 100 years we have been helping clients find the best real estate solutions in the Triangle. Our combination of energetic young leaders, wisdom of established team members, and full range of real estate services have provided our healthcare clients with peace of mind, ideas and solutions.
RALEIGHHeadquarters & Property Management (919) 821-1350
Commercial Sales & Leasing (919) 821-7177
MOREHEAD CITY(252) 247-5772
www.yorkproperties.com
York Properties Broker Team
BROKERAGE LEASING PROPERTY MANAGEMENT INVESTMENT SECURITY MAINTENANCE LANDSCAPING
HELPING YOU WITH REAL ESTATE, SO YOU CAN FOCUS ON HELPING OTHERS.

Modern, well-appointed med spa is available in a picturesque part of the state. This practice is positioned in a highly traveled area with positive demographics adding to the business appeal and revenue stream. A sampling of the services and procedures offered are: BOTOX, facial therapy and treatments, laser hair removal, eye lash extensions and body waxing as well as a menu of anti-aging options.
If you are currently a med spa owner and looking to expand or considering this high profile med business, this is the perfect opportunity.
Highly profitable and organized, you will find this spa poised for success. The qualified buyer can obtain detailed information by contacting Medical Practice Listings at 919-848-4202.
MODERN MED SPA AVAILABLELocated in beautiful coastal North Carolina
MedicalPracticeListings.com | [email protected] | 919.848.4202
68| JUNE 2012
Located in South Denver, Colorado, this practice features high patient volume and high visibility on the internet. Established referral sources, owner (psychologist) has excellent reputa-tion based on 30 years experience in Denver. Private pay and insurances, high-density traffic, beautifully decorated and furnished offices, 378 active and inactive clients, corporate clients, $14,000 physical assets, good parking, near bus and rapid transit housed in a well-maintained medical building. Live and work in one of the most healthy cities in the U.S.
List Price: $150,000 | Established: 2007 | Location: Colorado
Practice for Sale in South Denver
For more information contact Dr. Jack McInroy at 303-929-2598 or [email protected]
Neurofeedback and Psychological Practice
Med MonthlyMed Monthly is the premier health care
magazine for medical professionals.
By placing an ad in Med Monthly you’ll reach: family medicine, internal
medicine, physician assistants and more!
Call us today to place your classified!
919.747.9031
Also available online 24/7medmonthly.com

Pediatric Locums Physician needed in Harrisonburg, Danville and Lynchburg, VA. These locum positions require 30 to 40 hours per week, on-going. If you are seeking a beautiful cli-mate and flexibility with your schedule, please consider one of these opportunities. Send copies of your CV, VA. medical license, DEA certificate and NPI certificate with number to Physician Solutions for immediate consideration. Physician Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054, email: [email protected]
Urgent Care opportunities throughout Virginia. We have contracts with numerous facilities and eight to 14-hour shifts are available. If you have experience treating patients from pediatrics to geriatrics, we welcome your inquires. Send copies of your CV, VA medical license, DEA certificate and NPI certificate with number to Physician Solutions for im-mediate consideration. Physician Solutions, P.O. Box 98313, Raleigh, NC 27624, and PH: (919) 845-0054, E-mail: [email protected]
Physicians needed
North Carolina (cont.)
MEDICAL PRACTICE LISTINGSAre you looking to sell or buy a practice?
View national practice listings by visiting our website orcontact us for a confidential discussion regarding your prac-
tice options. We are always ready to assist you.
[email protected] | medicalpracticelistings.com
We have in-house practice experts and an attorney ready to assist.
To place a classified ad, call 919.747.9031
Classified
MEDMONTHLY.COM | 69
Practice wantedPediatric Practice Wanted in Raleigh, NCMedical Practice Listings has a qualified buyer for a pediatric practice in Raleigh, Cary or surrounding area. If you are retiring, relocating or considering your options as a pediatric practice owner, contact us and review your options. Medical Practice Listings is the leading seller of practices in the US. When you list with us, your practice receives exceptional national, regional and local exposure. Contact us today at (919) 848-4202.
Virginia
Internal Medicine Practice located in High Point, NC, has two full-time positions available. This well-established practice treats private pay as well as Medicare/Medicaid patients. There is no call or rounds associated with this opportunity. If you con-sider yourself a well-rounded IM physician and en-joy a team environment, this could be your job. You would be required to live in or around High Point and if relocating is required, a moving package will be extended as part of your salary and incentive package. BC/BE MD should forward your CV, and copy of your NC medical license to [email protected] - View this and other exceptional physician opportunities at www.physiciansolutions.com or call (919) 845-0054 to discuss your availabil-ity and options.
Locum Tenens Primary Care Physicians Needed If you would like the flexibility and exceptional pay associated with locums, we have immediate oppor-tunities in family, urgent care, pediatric, occupa-tional health and county health departments in NC and VA. Call today to discuss your options and see why Physician Solutions has been the premier physi-cian staffing company on the eastern seaboard. Call (919) 845-0054 or review our corporate capa-bilities at www.physiciansolutions.com
Pediatricians Needed Well established Pediatric office in Harnett County & Wake County, North Carolina seeks ongoing coverage for locum tenen opportunity. Pediatrician will see about 20 patients daily, hours are 9 a.m. - 5 p.m. No call or hospital duties. Please send a current CV to [email protected] or call (919) 845-0054 for details on this and other opportunities across the state.
Physicians Needed Immediately We have several immediate needs for physician coverage for various facilities in North Carolina for addiction medicine. For immediate consideration please call or email us at [email protected] or call (919) 845-0054. We can put you to work tomorrow! We have very competitive salaries, we pay for mileage, your accommodations if necessary. We look forward to hearing back from you.
Physicians needed

70| JUNE 2012
Practice for sale
Lucrative ENT Practice with room for growth, located three miles from the beach. Physician’s assistant, audiolo-gist, esthetician and well-trained staff. Electronic medical records, mirror imaging system, established patient and referral base, hearing aids and balance testing, esthetic services and Candela laser. All aspects of otolaryngology, busy skin cancer practice, established referral base for re-constructive eyelid surgery, Botox and facial fillers. All new surgical equipment, image-guidance sinus surgery, balloon sinuplasty, nerve monitor for ear/parotid/thyroid surgery. Room for establishing allergy, cosmetics, laryngology and trans-nasal esophagoscopy. All the organization is done; walk into a ready-made practice as your own boss and make the changes you want, when you want. Physician will to stay on for a smooth transition. Hospital support is also an option for up to a year. The listing price is $395,000 for the practice, charts, equipment and good will. Contact Medical Practice Listings for additional information. Medi-cal Practice Listings, P.O. Box 99488, Raleigh, NC 27624. PH: (919) 848-4202 or email: [email protected]
Practice for sale
South Carolina
To place a classified ad, call 919.747.9031
North Carolina
Classified
Family Practice located in Bainbridge Island, WA has recent-ly been listed. Solid patient following and cash flow makes this 17-year-old practice very attractive. Contact Medical Practice Listings for more details. email: [email protected] or (919) 848-4202.
Washington
Family Practice located in Hickory, NC. Well-established and a solid 40 to 55 patients split between an MD and physician assistant. Experienced staff and outstanding medical equipment. Gross revenues average $1,500,000 with strong profits. Monthly practice rent is only $3,000 and the utilities are very reasonable. The practice with all equipment, charts and good will are priced at $625,000. Contact Medical Practice Listings for additional informa-tion. Medical Practice Listings, P.O. Box 99488, Raleigh, NC 27624. PH: (919) 848-4202 or email: [email protected]
Impressive Internal Medicine Practice in Durham, NC: The City of Medicine. Over 20 years serving the community, this practice is now listed for sale. There are four well-equipped exam rooms, new computer equipment and a solid pa-tient following. The owner is retiring and willing to con-tinue with the new owner for a few months to assist with a smooth transition. Contact Medical Practice Listings at (919) 848-4202 for more information. View additional listings at: www.medicalpracticelistings.com
Modern Vein Care Practice located in the mountains of NC. Booking seven to 10 procedures per day, you will find this impressive vein practice attractive in many ways. Housed in the same practice building with an internal medicine, you will enjoy the referrals from this as well as other primary care and specialties in the community. We have this practice listed for $295,000 which includes charts, equipment and good will. Contact Medical Practice List-ings at (919) 848-4202 for more information. View addition-al listings at www.medicalpracticelistings.com
Primary Care Practice specializing in women’s care. The owning female physician is willing to continue with the practice for a reasonable time to assist with smooth own-ership transfer. The patient load is 35 to 40 patients per day, however that could double with a second provider. Exceptional cash flow and profitable practice that will surprise even the most optimistic practice seeker. This is a remarkable opportunity to purchase a well-established woman’s practice. Spacious practice with several well-appointed exam rooms throughout. New computers and medical management software add to this modern front desk environment. This practice is being offered for $435,000. Contact Medical Practice Listings for additional information. Medical Practice Listings, P.O. Box 99488, Raleigh, NC 27624. PH: (919) 848-4202 or send an email to [email protected]
Internal Medicine Practice located just outside Fayette-ville, NC is now being offered. The owning physician is retiring and is willing to continue working for the new owner for a month or two assisting with a smooth trans-action. The practice treats patients four and a half days per week with no call or hospital rounds. The schedule accommodates 35 patients per day. You will be hard pressed to find a more beautiful practice that is modern, tastefully decorated and well appointed with vibrant art work. The practice, patient charts, equipment and good will is being offered for $415,000 while the free standing building is being offered for $635,000. Contact Medical Practice Listings for additional information. Medical Prac-tice Listings, P.O. Box 99488, Raleigh, NC 27624. PH: (919) 848-4202 or email: [email protected]
North Carolina (con't)

MEDMONTHLY.COM |71
This upscale primary care practice has a boutique look and feel while realizing consistent revenues and patient flow. You will be impressed with the well appointed layout, functionality as well as the organization of this true gem of a practice. Currently accepting over 20 insurance carriers including Aetna, Blue Cross and Blue Shield, Cigna, City of Seattle, Great West and United Healthcare. The astute physician considering this practice will be impressed with the comprehensive collection of computers, office furniture and medical equipment such as Welch Allyn Otoscope, Ritter Autoclave, Spirometer and Moore Medical Exam table.
Physician compensation is consistently in the $200,000 range with upside as you wish. Do not procrastinate; this practice will not be available for long.
List price: $255,000 | Year Established: 2007 | Gross Yearly Income: $380,000
FAMILY PRACTICE FOR SALEA beautiful practice located in Seattle, Washington
MedicalPracticeListings.com | [email protected] | 919.848.4202
Medical Practice ListingsSelling and buying made easy
Please direct all correspondence to [email protected] serious, qualified inquirers.
One of the oldest Locums companies Large client list Dozens of MDs under contract Executive office setting Modern computers and equipment Revenue over a million per year Owner retiring List price is over $2 million
MD STAFFING AGENCY FOR SALE
Great opportunity for anyone who wants to purchase an established business.
OCCUPATIONAL HEALTH CARE PRACTICE FOR SALEGreensboro, North Carolina
Well-established practice serving the Greensboro and High Point areas for over 15 years. Five exam rooms that are fully equipped, plus digital X-Ray. Extensive corporate accounts as well as walk-in traffic. Lab equip-ment includes CBC. The owning MD is retiring, creat-ing an excellent opportunity for a MD to take over an existing patient base and treat 25 plus patients per day from day one. The practice space is 2,375 sq. feet. This is an exceptionally opportunity. Leased equipment in-cludes: X-Ray $835 per month, copier $127 per month, and CBC $200 per month. Call Medical Practice Listings at (919) 848-4202 for more information.
PRACTICE FOR SALE
Asking price: $385,000
To view more listings visit us online at medicalpracticelistings.com

72| JUNE 2012
Established private internal medicine practice treating general as well as adolescent patients and licensed clinical psychologist’s combine for a high profile multi-disciplinary practice. The staff includes a medical doctor, physician assistant, three licensed clinical psychologists, and a complement of nurses and administrators. The internal medicine practice also uses locum physicians to treat primary care patients as needed. Excellent gross income with solid profits are enjoyed in this ever-growing practice located in a bustling community with handsome demographics. Two all brick condominiums house these practices which are offered for lease or purchase.This expanded services private health care facility has a solid following and all the tools necessary for enhanced services, income and expan-sion. For more details which include a BizScore Practice Valuation, finan-cial statements, patient demographics and furniture and equipment details, contact one of our professionals.
Private Medical and Mental Health Care Practice for SaleCoastal North Carolina, minutes from Atlantic Beach
Medical Practice ListingsPH: (919) 848-4202 Email: [email protected]
www.medicalpracticelistings.com
By placing a professional ad in Med Monthly, you're spending smart money and directing your marketing efforts toward qualified clients. Contact one of our advertising agents and find out how inexpensive yet powerful your ad in Med Monthly can be.
medmonthly.com | 919.747.9031
ADVERTISE YOUR PRACTICE BUILDING IN MED MONTHLY
Hospice Practice wanted in Raleigh/Durham area of North Carolina.
Medical Practice Listings has a qualified physician buyer that is ready to purchase. If you are considering your hospice practice options, contact us for a confidential discussion regarding your practice.
Hospice Practice Wanted
To find out more information call 919-848-4202 or e-mail [email protected]
www.medicalpracticelistings.com

MEDMONTHLY.COM |73
MedSpa Located in North Carolina
We have recently listed a MedSpa in NC
This established practice has staff MDs, PAs and nurses to assist patients. Some of the procedures performed include: Botox, Dysport, Restylane, Perian, Juvederm, Radiesse, IPL Photoreju Venation, fractional laser resurfacing as well as customized facials. There are too many procedures to mention in this very upscale practice. The qualified buyer will be impressed with the $900,000 gross revenue. This is a new listing, and we are in the valuation process.
Contact Medical Practice Listings today to discuss the practice details.
NC MedSpa For Sale
For more information call Medical Practice Listings at919-848-4202 or e-mail [email protected]
www.medicalpracticelistings.com
Plastic Surgery practice for sale with lucrative ENT specialty
Myrtle Beach, South Carolina
Practice for sale with room for growth, located only three miles from the beach. Physician’s assistant, audiologist, esthetician and well-trained staff. Electronic medical records, Mirror imaging system, established patient and referral base, hearing aids and balance test-ing, esthetic services and Candela laser. All aspects of Otolaryngology, busy skin cancer practice, established referral base for reconstructive eyelid surgery, Botox and facial fillers. All new surgical equipment, image-guidance sinus surgery, balloon sinuplasty, nerve monitor for ear/parotid/thyroid surgery. Room for establishing allergy, cosmetics, laryngology & trans-nasal esophagoscopy. Walk into a ready made practice as your own boss and make the changes you want, when you want. Physician will stay on for smooth transition. Hospital sup-port also an option for up to a year. The listing price is $395,000.
For more information call Medical Practice Listing at (919) 848-4202. To view our other listings, visit medicalpracticelistings.com
Practice at the beach
Physician Solutions has immediate opportunities for psychiatrists throughout NC. Top wages, professional liability insurance and
accommodations provided.
Call us today if you are available for a few days a month, on-going or for permanent placement.
Please contact Physican Solutions at 919-845-0054 or [email protected]
NC OPPORTUNITIES LOCUMS OR PERMANENT
For more information about Physician Solutions or to see all of our locums and permanent listings,
please visit physiciansolutions.com
Primary care practice specializing in women’s careRaleigh, North Carolina
The owning physician is willing to continue with the practice for a reasonable time to assist with smooth ownership trans-fer. The patient load is 35 to 40 patients per day, however, that could double with a second provider. Exceptional cash flow and profit will surprise even the most optimistic prac-tice seeker. This is a remarkable opportunity to purchase a well-established woman’s practice. Spacious practice with several well-appointed exam rooms and beautifully decorat-ed throughout. New computers and medical management software add to this modern front desk environment.
List price: $435,000
Practice for Sale in Raleigh, NC
Call Medical Practice Listings at (919) 848-4202 for details and to view our other listings visit
www.medicalpracticelistings.com

the top
74| JUNE 2012
3
Most Innovative
Medical Breakthroughs of 2012
2
June’s Top 9 list names some of the nomi-nations selected for the Cleveland Clinic’s most innovative medical breakthroughs of 2012. These innovations qualified based on the criteria of having signifi-cation potential for short-term clinical success, a high probability of success, already being on the market (or close to being introduced), and sufficient data to support the nomination.
Compiled by Leigh Ann Simpson
Concussion Management System for Athletes
This system instantly detects brain inju-ries at contact, and provides patient-spe-cific return to play guidance. The novel system includes an assessment tool that establishes an athlete’s baseline cognitive and motor skills at the begin-ning of his or her athletic season.
CT Scans for Early Detection of Lung CancerWith low-radiation-dose spiral
computed tomography (spiral CT), this scan can generate a detailed cross-sectional images of the lungs that cre-ate a three-dimensional image. These scans identify tumors earlier and also spot them when they are smaller and more treatable by surgery. Novel Diabetes Therapy:
SGLT2 InhibitorsMost diabetes medications work by affecting the supply or use of insulin, which helps move glucose into the
cells. But now there is a new class of drugs called sodium-glucose co-transporter 2 protein inhibitors, or SGLT2 inhibitors that represent a paradigm shift in diabetes treatment – reducing blood sugar by excreting it during urination.
Active Bionic Prosthesis: Wear-able Robotic DevicesThanks to remarkable advances in
prosthetics research, space-age plastics and carbon-fiber composites have been engineered to help restore function. Now the computer-ized bionic leg, with its microprocessors and computer chips, can rival the functionality of biological limbs.
Medical Apps for Mobile DevicesThese apps provide doctor’s with several advantages: access to reli-able, up-to-date medical informa-tion, the ability to answer patient queries quickly without leaving the patient’s bedside, and interactive features that help select appropri-ate screening tests and calculate a patient’s risk of developing diseases.
Catheter-Based Renal Denervation to Control Resistant HypertensionThis 40-minute procedure is approach-ing resistant hypertension in a new way – by targeting the renal sympathetic system. Clinical trial results have shown improved blood pressure levels, and also show promise in treating chronic kidney disease, insulin resistance and heart failure.
Genetically Modified Mosquitoes to Reduce Disease Threat
Researchers are exploring new avenues to fight mosquitoes, starting in the laboratory where sci-entists manipulate the DNA of the insects so that they are not capable of reproducing.
Increasing Discovery with Next-Generation Gene SequencingLeading Geneticists envi-
sion a day soon when everyone’s genome will be sequenced and included in their medical records. These next-generation sequencing machines, now faster and more af-fordable, can help achieve this goal in the near future.
Implantable Device to Treat Complex Brain AneurysmsThis minimally-invasive proce-dure can treat
brain aneurysms without open surgery by implanting a device directly into the artery. Consist-ing of a flexible braided mesh tube made of platinum and nickel-cobalt chromium alloy, this device can
be delivered by catheter to block off aneurysms in the damaged internal carotid artery. 9
75
8

Save a life. Don’t Drive HoMe buzzeD. BUZZED DRIVING IS DRUNK DRIVING.

GROW YOUR PRACTICELet MedMedia9’s expert designers create a website
for your practce. Need more? We can also create print collateral to help your practice grow.
IMAGINE THAT!MEDMEDIA9.COM | 919-747-9031Scan this QR code with your smartphone to learn more.