medical case studies acnp boot camp 2013. case study #1
TRANSCRIPT

Medical Case Studies
ACNP Boot Camp 2013

Case Study #1

Mr. Allen is a 62 y/o male, PMH HTN and DM2, admitted to MICU with hypoxia related to newly diagnosed community acquired pneumonia. He was given azithromycin by his PCP 2 days ago, however this morning awoke short of breath and feeling worse. He has an allergy to sulfa drugs.
In the ED, SpO2 was 89% on RA. Vitals on arrival to MICU: HR 115, BP 101/58, RR 38, SpO2 92% on 50% venti-mask. His CXR is as follows:


ABG on admission: 7.49 / 25 / 65 / 24
Na 138, K 4.2, Cl 102, C02 24, BUN 12 , Cr 0.8 ,AG 12
What is the acid-base disturbance?
A. Mixed metabolic acidosis and respiratory alkalosis
B. Respiratory alkalosis with compensation
C. Respiratory alkalosis without compensation
D. Respiratory acidosis

What antibiotic changes should be made?
A. Discontinue Azithro then start Vancomycin and Zosyn
B. Add Bactrim to regimen
C. Start Clindamycin and discontinue Azithro
D. None of the above
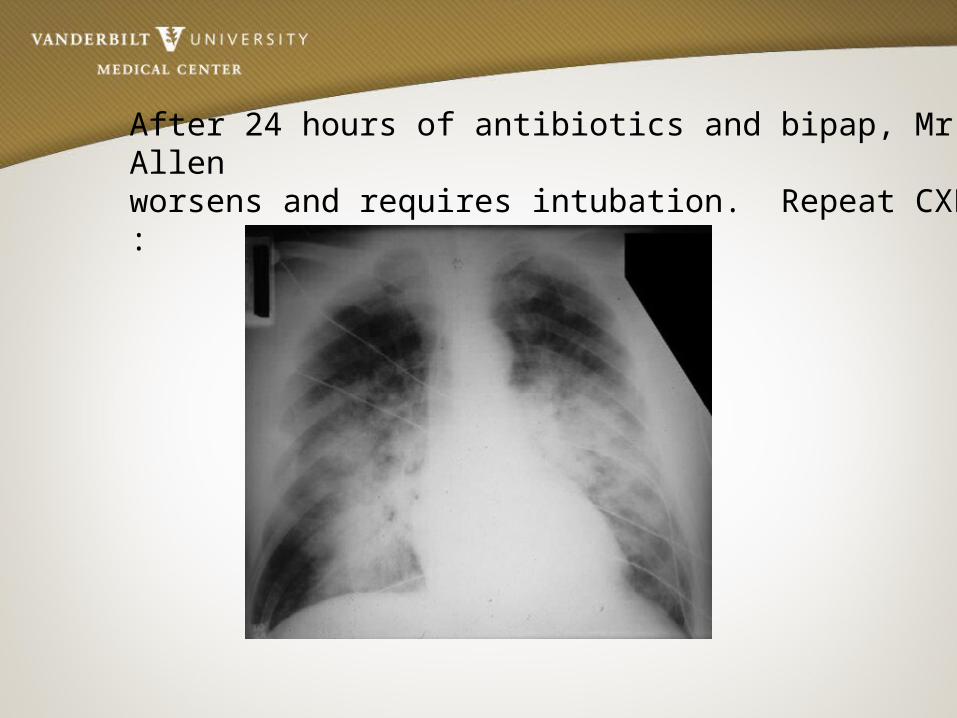
After 24 hours of antibiotics and bipap, Mr. Allen worsens and requires intubation. Repeat CXR :
ABG prior to intubation7.2 / 50 / 53 / 20
Na 136, K 4.5, Cl 100, C02 21, BUN _ , Cr _ , AG 15Lactate 3.9

What is the acid-base disturbance?
A. Metabolic acidosisB. Respiratory acidosisC. Respiratory acidosis
with metabolic acidosis
D. None of the above
With a pH of 7.2, what can you do to correct the acidosis?
A. Increase minute ventilation (RR up to 35)
B. Start a paralytic infusion
C. Give crystalloid fluidsD. Do nothing

He now has ARDS and is now requiring 70% FiO2. For maximizing alveolar recruitment, what should his PEEP setting be?
A. 5 mmHgB. 18 mmHgC. 22 mmHgD. 12 mmHg

Mr. Allen is 73 inches in height and weighs 105kg. Calculate his set tidal volume (predicted body weight x 6)
A. 480 mlB. 340 mlC. 920 mlD. 220 ml

After 3 days of supportive care, Mr. Allen continues to decompensate and a bronchoscopy is performed. Preliminary results reveal a gram positive organism. What changes should be made to the antibiotic regimen?
A. Discontinue vancomycin and start linezolid
B. Discontinue vancomycin and start daptomycin
C. Add coverage for atypical organisms
D. Both A and C

Unfortunately, the next day, Mr. Allen starts having melena stools. His PCV has been downtrending from 3833 27. After further review of his medication list, he was never started on stress ulcer prevention. Which is the best treatment option?
A. IV H2 BlockerB. PO H2 BlockerC. High dose IV PPID. PO PPI
Aggressive red blood cell transfusion would be the next best course of action.
A. TrueB. False
Mr. Allen’s condition is improving. Which factor is not required to start vent weaning:
A. Make unassisted breathing efforts
B. No pressors requiredC. FiO2 <.40 and PEEP <8D. Awake and following
all commands

Questions?

Case Study #2
Mr. Commodore is a 43 yo M with a hx of alcoholic cirrhosis and CAD on daily ASA who presents to the MICU with c/o melena, fatigue, and weakness.
Pertinent labs on admission include WBC 15, PCV 26, and platelets 100K. His initial VS are: BP 120/80, HR 110, RR 18, afebrile.
Physical exam is negative except for abdominal distention with positive fluid wave.
What would you do next?
A.Begin Pepcid 20 mg IVP BIDB.Transfuse 1 unit of PRBCC.Begin esomeprazole 40 mg IVP BIDD.Prep for colonoscopy

You should begin an octreotide drip at 50 mcg/hr after a 50 mcg bolus dose.
A. TrueB. False

SBP prophylaxis should be initiated.
A. TrueB. False
Which antibiotic would you start for SBP prophylaxis?
A. VancomycinB. CeftriaxoneC. MetronidazoleD. Caspofungin

Within 1 hour of arrival, the patient develops large volume hematemesis and becomes hemodynamically unstable. His vital signs are as follows: HR 135, BP 80/44, RR 26, O2 sat 89% on 2L NC.

Which of the following is the most important next step:
A. Intubate the patient and obtain 2 large bore PIVs
B. Insert CVC and begin levophed drip
C. Order STAT PT/INRD. Consult EGS
Once the patient is intubated and the airway is stabilized, you consult the GI team STAT for endoscopy and intervention. While waiting for the team to arrive, how can you optimize the patient for endoscopy and attempt to stabilize him?
A. Transfuse 1 pack of platelets
B. Give 10 mg Reglan IVP now
C. Transfuse 1 unit of PRBCD. All of the above

The patient undergoes endoscopy and is noted to have large esophageal varices. Five bands are placed and hemostasis is achieved. Incidentally, the patient is noted to also have esophageal candidiasis.

Which antibiotic should be initiated in this patient?
A. FluconazoleB. MicafunginC. Amphotericin BD. None of the above; pt is asymptomatic

The patient remains in the MICU overnight for close observation. He remains hemodynamically stable and has no further bleeding. However, this morning’s labs reveal a PCV of 20 and platelet count of 92K.

Which of the following is the next best course of action?
A. Nothing. The patient is stable without evidence of recurrent bleeding.
B. Transfuse 1 unit of PRBCC. Discharge the patient homeD. Transfuse FFP

Questions?
Case Study #3

Mr. Smith is a 67 yo male who resides in a SNF, with a history of CVA, COPD on 2L 02 who was treated 6 weeks ago for CAP. He is admitted to the MICU with SOB, AMS, and a 5 day history of diarrhea.
VS: BP 88/52, HR 116, RR 22, 02 sat 92% on 6L 02
ABG: 7.22 / 30 / 65 / 10

What acid base disturbance is present?
A. Metabolic acidosisB. Acute Respiratory
acidosisC. Chronic Respiratory
acidosisD. Respiratory alkalosis

Winter’s formula1.5 x 10 + 8 = 23
What does this tell us?
A. Respiratory compensation is incomplete
B. Pt. has a secondary respiratory acidosis
C. Both 1 and 2D. Neither 1 or 2
Delta / Delta ratio is 7/14This indicates the following:
A. There is an additional non-gap metabolic acidosis
B. There is an additional metabolic alkalosis
C. Neither of the aboveD. Not sure
Mr. Smith’s diarrhea becomes severe and he tests positive for clostridium difficile.

What is the best antibiotic treatment for this patient?
A. Metronidazole POB. Vancomycin IVC. Fluconazole IVD. Vancomycin PO

Questions?

Case Study #4
55 y/o male presented to ED with 3 day hx of malaise, fever, and poor PO intake. PMH significant for HTN, DM, and ESRD s/p renal transplant March 2013. Admitted to MICU for septic shock. Admission labs showed WBC 0.4, creatinine 5.0, increased from baseline of 1.8, and lactate 6. Patient received 1500mg IV Vancomycin, Zosyn, and 2L IVF in the emergency department.
When should the Vancomycin level be checked and what type of level should it be (peak, trough, random)?
A. Trough level 30 min before 5th doseB. Peak level 12 hours after initial doseC. Peak level after the 5th doseD. Random level 12-24 hours after the initial dose
Patient arrived in MICU hypotensive. An additional 3L IVF given with no improvement and vasopressors started. Patient rapidly became hypoxic (SpO2 in the 70’s) and required intubation. Vent settings: Volume control, 100% FiO2, 12 PEEP, rate 15. Fentanyl drip started. Patient remains hypoxic on the current vent settings. Peak pressure is 23.

This patient’s peak pressure is within acceptable range.
A. TrueB. False
ABG: pH 7.22 / 30 / 65 / 10Na 136, Cl 102, C02 10What is the acid-base disturbance?
A. Respiratory acidosisB. Non-anion gap
metabolic acidosisC. Anion gap metabolic
acidosisD. Compensated
metabolic acidosis

What are the next steps to improve oxygenation?
A. Paralyze the patientB. Increase PEEPC. Prone positioningD. Inhaled Flolan
Hospital day #2: Patient without improvement. Remains ventilated and on vasopressors. Creatinine up to 5.5 and WBC holding at 0.4. Current antibiotics include Vancomycin, Zosyn, and Levaquin. Blood cultures pending. Urine culture pending.

What additional organisms should be considered as a source of infection?
A. MRSAB. ESBLsC. CandidaD. Candida and ESBLs

Which is the best antibiotic to treat an ESBL in this patient?
A. ZosynB. AztreonamC. ClindamycinD. Meropenem
Which antibiotic would best treat Candida in this patient?
A. FluconazoleB. CaspofunginC. Fluconazole and CaspofunginD. None of the above
Patient’s shock is resolved and he is no longer requiring pressors. What should your next action be?
A. Continue fluid infusionsB. Daily CPAP breathing trialsC. Attempt diuresisD. Both B and C

Questions?
References
Acute Respiratory Distress Syndrome Network: Ventilation with Tidal Volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New Engl J Med. 2000; 342: 1302-1308.
ARDSNet: Higher versus lower Positive End-Expiratory Pressures in patients with the acute respiratory distress syndrome. New Engl J Med. 2004; 351: 327-336.
CDC websiteGarcia-Pagan et al, NEJM 2010; 362:2370-9Halperin, Mitchell L., Kamel, Kamel S. and Goldstein, Marc B. (2010) Fluid, Electrolyte and Acid- Base Physiology: A
Problem Based Approach, Fourth Edition. Philadelphia, PA. Saunders Elsevier. Infectious Disease Society of America websiteLau JY, Sung JJ, Lee KKC, et al, NEJM 2000; 343: 310–316Marini, J.J., Wheeler, A.W. (2010). Critical care medicine: The essentials (4th ed.). Philadelphia, PA: Lippincott Williams &
Wilkins.Rivkins, K., Lyakhovetskiy, A AJHP 2005; 62: 1164-1165Sucher, A.J., Chahine, E.B., Balcer, H.E. Echinocandins: The Newest Class of Antifungals. The Annals of
Pharmacotherapy. 2009, (43), pp. 1647 - 1657. Villaneuva, C et al NEJM 2013; 368:11-21