pathophysiology of adrenal insufficiency insufficiency...
TRANSCRIPT
Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing
� Pathophysiology of sepsis and septic shock� How sepsis affects the endocrine system� Pathophysiology of adrenal insufficiency� Clinical manifestations of relative adrenal
insufficiency� History of treatment for relative adrenal insufficiency,
use of corticosteroids and the cosyntropin stim test� Current treatment of adrenal insufficiency� Pathophysiology and clinical manifestations of
hyperglycemia� Treatment of hyperglycemia and how insulin
protocols have changed and why
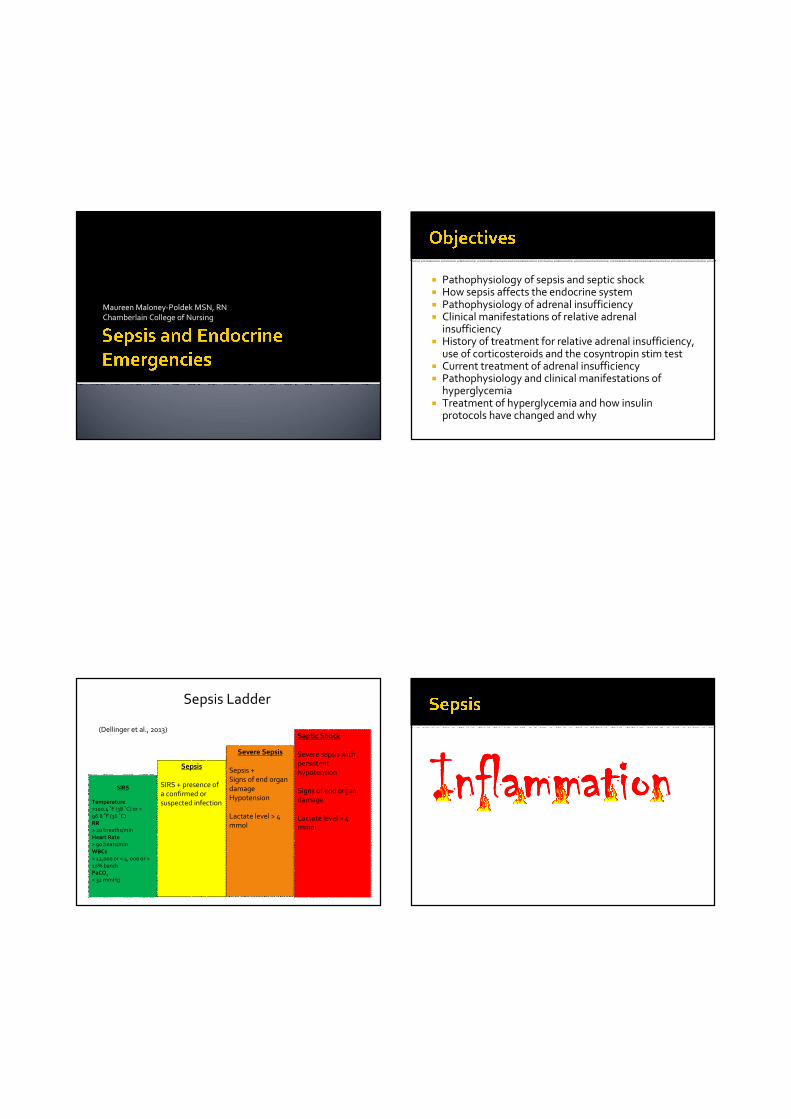
SIRS
Temperature
>100.4 ˚F (38 ˚C) or <
96.8 ˚F (36 ˚C)RR
> 20 breaths/min
Heart Rate
> 90 beats/min
WBCs
> 12,000 or < 4, 000 or >
10% bandsPaCO2
< 32 mmHg
Sepsis
SIRS + presence of a confirmed or suspected infection
Severe Sepsis
Sepsis + Signs of end organ
damageHypotension
Lactate level > 4 mmol
Septic Shock
Severe sepsis with persistent hypotension
Signs of end organ damage
Lactate level > 4 mmol
(Dellinger et al., 2013)
Sepsis Ladder
InflammationInflammationInflammationInflammation
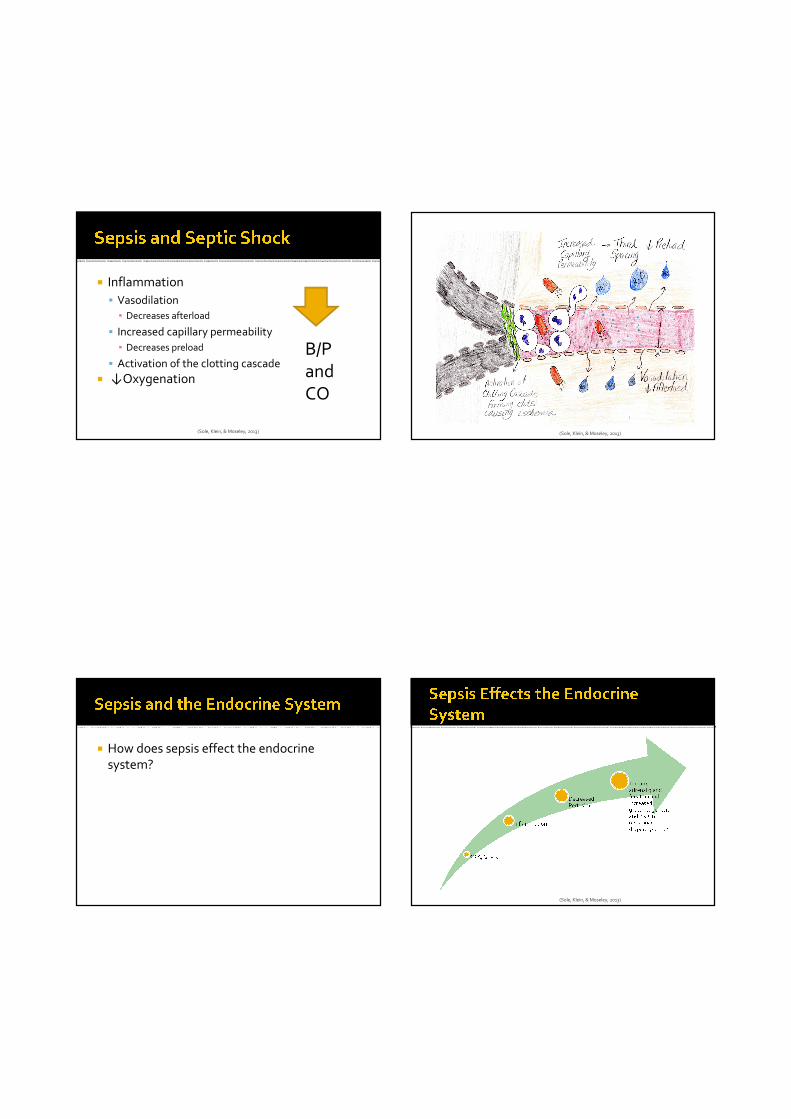
� Inflammation
� Vasodilation
▪ Decreases afterload
� Increased capillary permeability
▪ Decreases preload
� Activation of the clotting cascade
� ↓Oxygenation
B/P and CO
(Sole, Klein, & Moseley, 2013) (Sole, Klein, & Moseley, 2013)
� How does sepsis effect the endocrine system?
(Sole, Klein, & Moseley, 2013)

(Lewis et al., 2011).(Sole, Klein, & Moseley, 2013)
� Inflammation from sepsis suppresses the HPA axis altering the feedback loop
� Resistance to steroids related to altered
feedback loop
� Thrombotic necrosis of the adrenal gland
(Sole, Klein, & Moseley, 2013)
� Circulatory collapse
� Refractory hypotension
� Tachycardia
� Dehydration
� Fever
� A/N/V/D/abdominal pain
� Fatigue and muscle weakness
Very vague in critically ill patients!!!
(Whiteman, 2009)

� Baseline cortisol level, cosyntropin administration and repeat cortisol level
(Whiteman, 2009)
� No longer recommended to assess for
relative adrenal insufficiency
(Dellinger et al., 2013)
� Why steroids?� Originally thought to reduce inflammation
� Currently– treats relative adrenal insufficiency
� History of steroid use in sepsis� High doses increased mortality rate (Bone et al., 1987)
� Low doses improved mortality rates (Annane et al., 2002)
� CORTICUS –reduction in organ failure rates but not mortality (Moreno et al., 2011)
� Patients with refractory hypotension despite vasopressor administration
� Recommend a dose of 200 mg/day
� Recommend a continuous infusion
(Dellinger et al., 2013)
� Can occur in critically ill patients without a history of diabetes
� Due to increased stress response
� Can lead to complications
� Abnormal immune function
� ↑ Infection rates
� Hemodynamic instability
� Dysrhythmias
(Schiffner, 2014)
� What is a normal blood glucose?
� What should the target blood glucose be?
� Blood glucose goal of < 180 mg/dL� Van Den Berghe et al., (2001)
� 80-110 mg/dL
� Used to be <150 mg/dL (2008 guidelines)
� NICE SUGAR Trial
▪ Hypoglycemia = ↑mortality rates
(NICE SUGAR TRIAL, 2008, Dellinger et al., 2008 & Dellinger et al., 2013)
� Treat two consecutive BG readings of > 180 mg/dL
� Insulin infusion goal BG of < 180 mg/dL
� Monitor BG every 1-2 hrs until stable, then
every 4 hours
� Caution with Point of care testing
(Dellinger et al., 2013 & Kleinpell, Aitken, & Schorr, 2013)
� Nurse controlled protocols
� Safe
� Better target outcomes
(Kleinpell, Aitken, & Schorr, 2013)

Case Study� G.S. is a 46 year-old female with a past
medical history of HTN and an acute
appendicitis. She developed septic shock
after her appendix ruptured…
� She is currently intubated, ventilated and sedated and receiving antibiotics.
� After receiving multiple fluid boluses, she also
has a continuous infusion of norepinephrine
at 20 mcg/min and vasopressin of 0.03
units/min� Despite this, her MAP is at 65mmHg
� Is she a candidate for corticosteroids?
� Yes
� She has received multiple fluid boluses to correct
volume loss and she is currently on multiple
pressors for a MAP of 65mmHg
� What is the recommended daily dose?
� Her morning blood glucose is 200 mg/dL and her afternoon blood glucose is 192 mg/dL
� What should the nurse anticipate?
� An insulin infusion is started, what is the target glucose level?
� How should the insulin infusion be managed?
� G.S. is started on hydrocortisone at 200 mg/day and an insulin infusion
� Gradually, she was weaned off
norepinephrine and vasopressin
� Eventually she was weaned off mechanical
ventilation and extubated
� She eventually made a complete recovery
The End

Annane, D., Sebille, V., Charpentier, C., Bollaert, P.E., Francois, B., Korach, J.M., …Bellissant, E. (2002). Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. Journal of the American Medical Association 288(7) 862-871.
Bone, R.C., Fishers, C. J., Clemmer, T. P., Slotman, G.J. , Metz. C.A., & Balk, R.A. (1987). A controlled clinical trial of high-dose methylprednisolone in the treatment of severe sepsis and septic shock. The New England Journal of Medicine 317(11), 653-658.
Dellinger, R.P. et al. (2013). Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Critical Care Medicine 41(2), 580-637.
Dellinger, R.P. et al. (2008). Surviving sepsis campaign: International guidelines for the management of severe sepsis and septic shock: 2008. Critical Care Medicine 36(1), 296-327.
Kleinpell, R., Aitken, L. & Schorr, C. (2013). Implications of the new international sepsis guidelines for nursing care. American Journal of Critical Care 22(3), 212-222.
Lewis, S. L., Dirksen, S. R., Heitkemper, M. M., & Bucher, L. (2014). Medical surgical nursing: Assessment and management of clinical problems (9th ed.). St. Louis, MO: Mosby Elsevier
Moreno, R., Sprung, C.L., Annane, D., Chevret, S. Briegel, J., Keh, D., …Vincent, J.L. (2011). Time course of organ failure in patients with septic shock treated with corticosteroids: Results of the corticus study. Intensive Care Medicine 37(11) 1765-1772.
The NICE-SUGAR Study Investigators. (2009). Intensive versus conventional glucose control in critically ill patients. The New England Journal of Medicine 360(13), 1283-1297.
Schiffner, L. (2014). Glucose management in critically ill medical and surgical patients. Dimensions of Critical Care Nursing 33(2), 70-77.
Sole, M.L. , Klein, D.G., & Moseley, M.J. (2013). Introduction to critical care nursing (6th ed.). St. Louis: MO, Elsevier.
Van Den Berghe, G., Wouters, P., Weekers, F., Verwaest, C., Bruyninckx, F., Schetz, M. … Bouillon, R. (2001). Intensive insulin therapy in
critically ill patients. The New England Journal of Medicine 345(19),
1359-1367. Whiteman, K. (2009). ACTH stimulation: Testing the adrenals. Nursing 2009
Critical Care 4(1), 56.