prof gergely péter vascularitis. active necrotizing vasculitis
TRANSCRIPT
Prof Gergely Péter

Active necrotizing vasculitis

Vasculitic scars
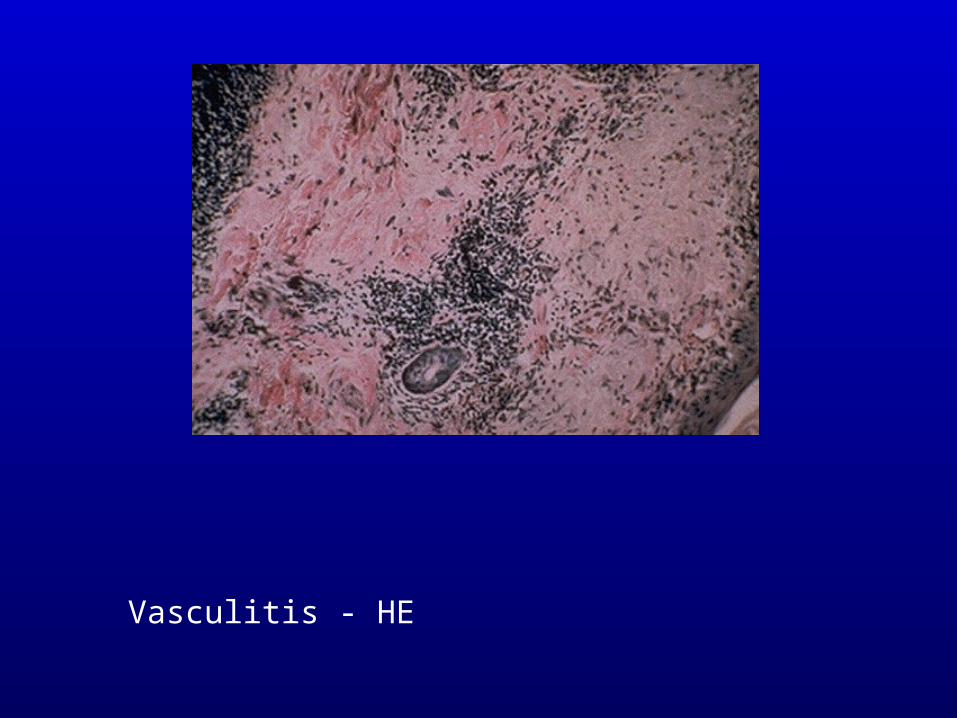
Vasculitis - HE
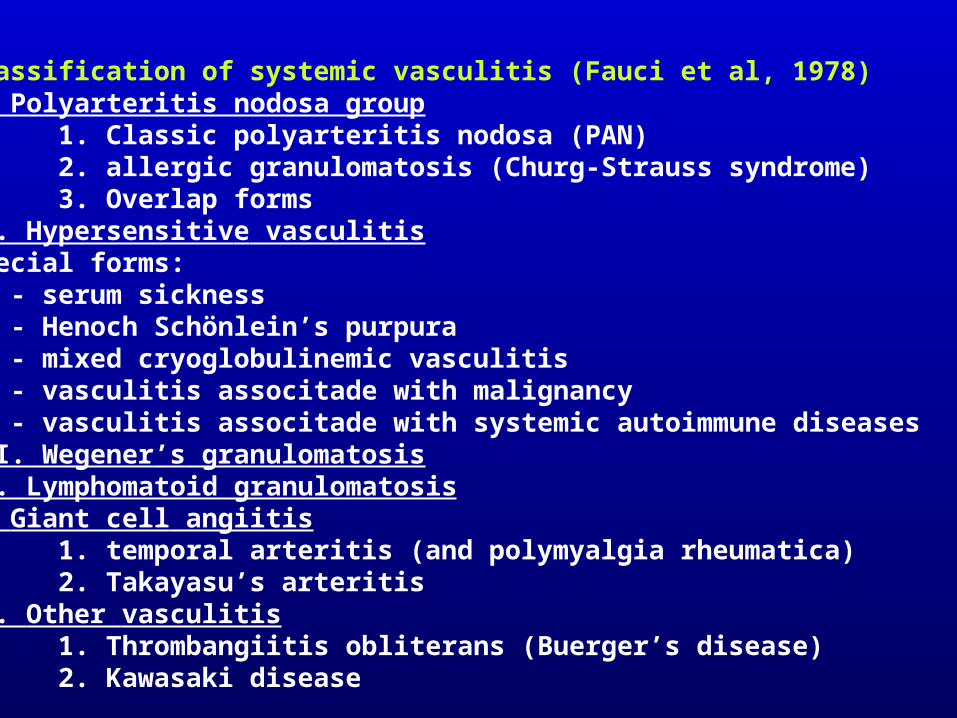
Classification of systemic vasculitis (Fauci et al, 1978)I. Polyarteritis nodosa group
1. Classic polyarteritis nodosa (PAN)2. allergic granulomatosis (Churg-Strauss syndrome)3. Overlap forms
II. Hypersensitive vasculitis Special forms: - serum sickness - Henoch Schönlein’s purpura - mixed cryoglobulinemic vasculitis - vasculitis associtade with malignancy - vasculitis associtade with systemic autoimmune diseasesIII. Wegener’s granulomatosisIV. Lymphomatoid granulomatosisV. Giant cell angiitis
1. temporal arteritis (and polymyalgia rheumatica)2. Takayasu’s arteritis
VI. Other vasculitis1. Thrombangiitis obliterans (Buerger’s disease)2. Kawasaki disease
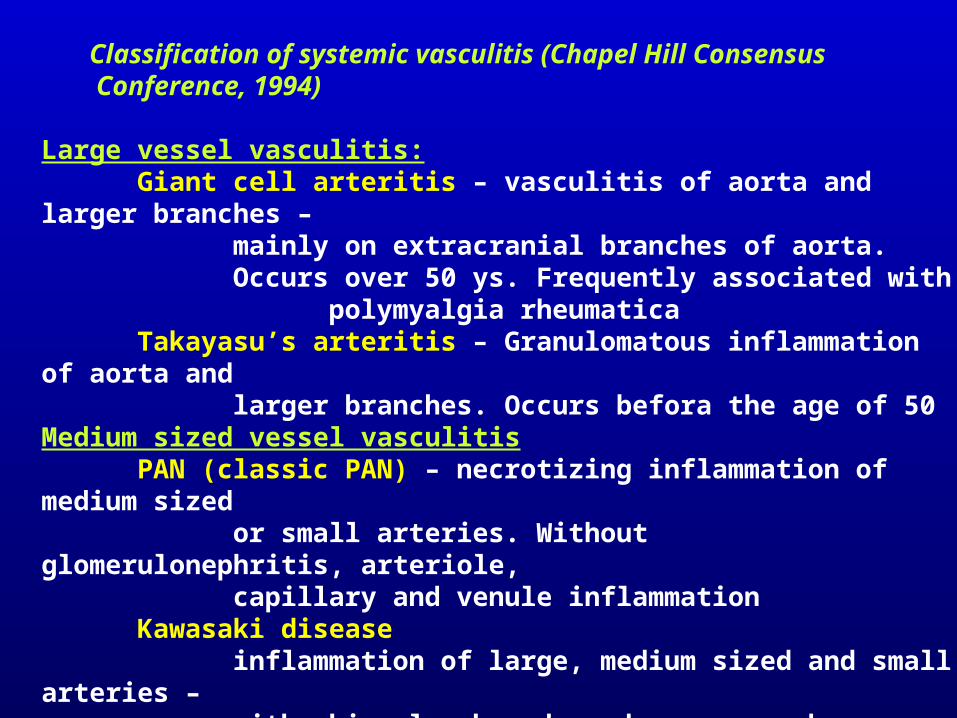
Classification of systemic vasculitis (Chapel Hill Consensus Conference, 1994)
Large vessel vasculitis:Giant cell arteritis – vasculitis of aorta and larger branches –
mainly on extracranial branches of aorta.Occurs over 50 ys. Frequently associated with polymyalgia rheumatica
Takayasu’s arteritis – Granulomatous inflammation of aorta and larger branches. Occurs befora the age of 50
Medium sized vessel vasculitisPAN (classic PAN) – necrotizing inflammation of medium sized
or small arteries. Without glomerulonephritis, arteriole, capillary and venule inflammation
Kawasaki diseaseinflammation of large, medium sized and small arteries –with skin, lymph node and mucous membrane symptoms. Frequently affects coronaries, occurs mainly in smallchildren
Small cell vasculitis:Wegener’s granulomatosis
necrotizing inflammation primarily of airway vessels, frequently with necrotizing glomerulonephritis
Churg-Strauss syndrome - eosinophile granulocytic necrotizing vasculitis, involving vessels of airways
microscopic polyangiitis (microscopic polyarteritis)necrotizing inflammation of arterioles, capillaries, venules (may involve also medium sized arteries) pauci-immune (i.e. no IC deposit)frequent necrotizing glomerulonephritis and capillaritisof lungs
Henoch-Schönlein’s purpuravasculitis localized to capillaries, venules, arterioles, with IgA deposition, with skin, intestinal andglomerular involvement
essential cryoglobulinemic vasculitiscryoglobulin and cryoglobulin deposition
cutaneous-leukocytoclastic vasculitiswithout visceral involvement
Classification criteria of polyarteritis nodosa (ACR, 1990)
1 Weight loss 4 kg (since illness began, not due to dieting or other factors)
2 Livedo reticularis (mottled reticular pattern over the skin of portions of extremities or torso)
3 Testicular pain or tenderness (not due to infection, trauma or other causes)
4 Myalgias, weakness, or leg tenderness (diffuse myalgias, excludingshoulder and hip girdle, or weakness of muscles or tenderness of leg muscles)
5 Mono- or polyneuropathy6 Hypertension (diastolic blood pressure >90 Hgmm)7 Elevated BUN or creatinine8 Hepatitis B virus (presence of virus antigen or antibody)9 Arteriographic abnormality (aneurysms or occlusions of the visceral
arteries, not due to other causes, e.g. arteriosclerosis, etc.)10 Biopsy (granulocytes and/or granulocytes and mononuclear
leukocytes in the artery wall)Diagnosis is based on the presence of at least 3 criteria.

Livedo reticularis

Livedo vasculitis

Livedo reticularis (racemosa)
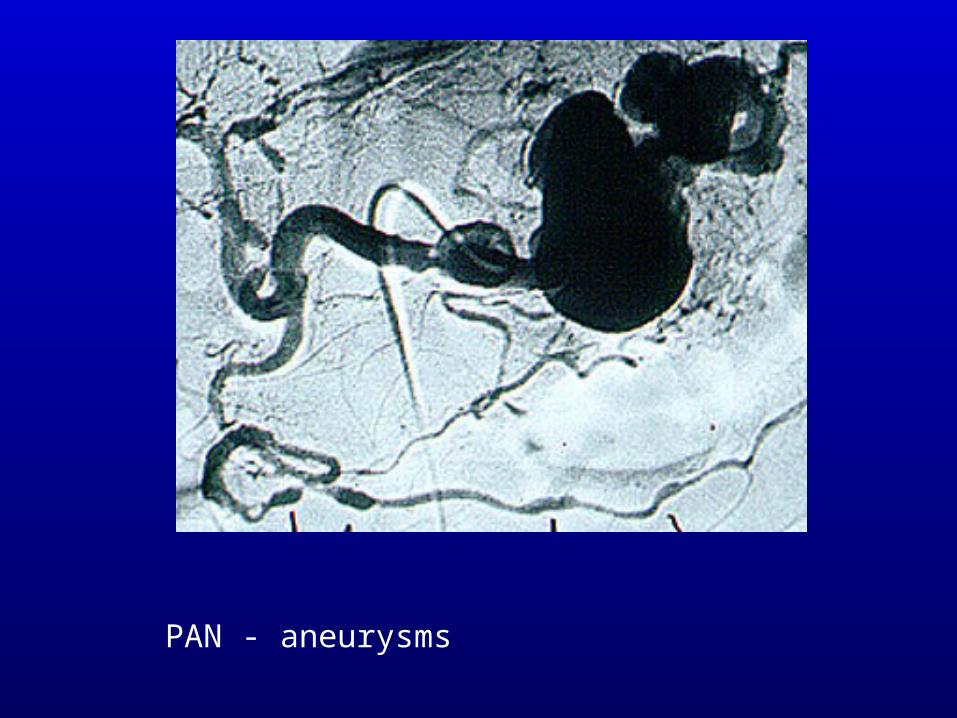
PAN - aneurysms
Classification criteria of allergic granulomatosis (Churg-Strauss syndrome) (ACR, 1990)
1 Asthma (in the history)2 Eosinophilia in WBC count (>10%)3 Mono- or polyneuropathy4 Non-fixed pulmonary infiltrates (migratory or transitory infiltrates
on radiographs)5 Paranasal sinus abnormality (history of acute or chronic paranasal
sinus pain or tenderness or radiographic opacification)6 Biopsy (artery, arteriole or venule, showing accumulation of
eosinophils in extravascular area)
Diagnosis is based on the presence of at least 4 criteria.
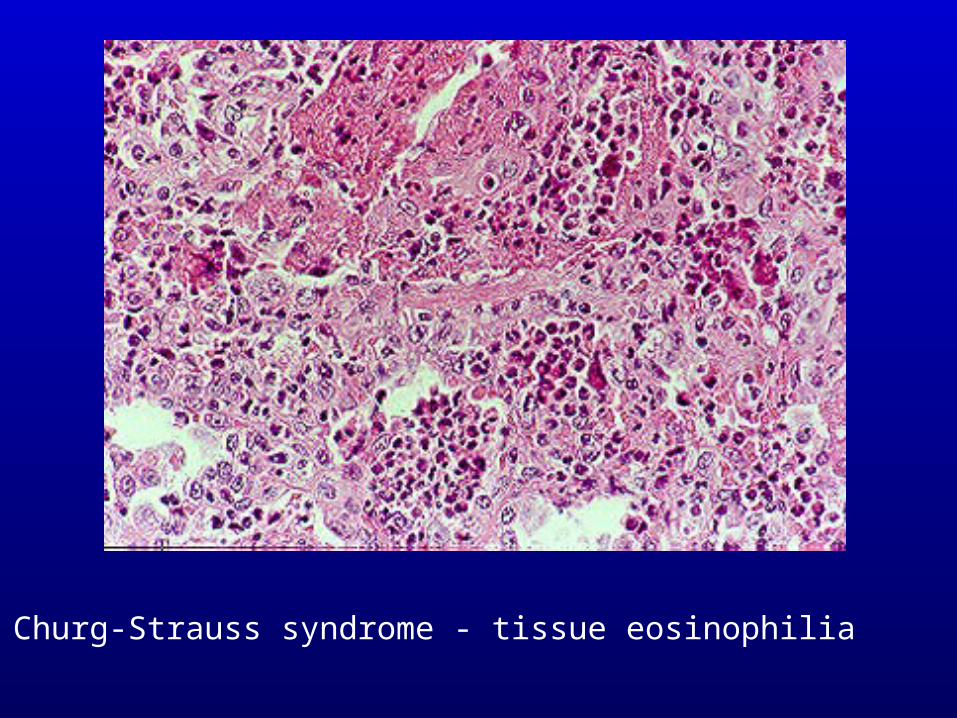
Churg-Strauss syndrome - tissue eosinophilia
Classification criteria of Wegener’s granulomatosis (ACR, 1990)
1 Nasal or oral inflammation (painful or painless oral ulcers or purulent or bloody nasal discharge)
2 Abnormal chest radiograph (presence of nodules, fixed infiltrates, or cavities)
3 Urinary sediment (microhematuria , i.e. >5 red blood cell per high power field, or red cell casts in sediment)
4 Biopsy (granulomatous inflammation within the wall of an artery or in the peri- or extravascular area of artery or arteriole)
Diagnosis is based on the presence of at least 2 criteria. In the absence of specific biopsy finding, hemoptysis can be used as a surrogate variable.
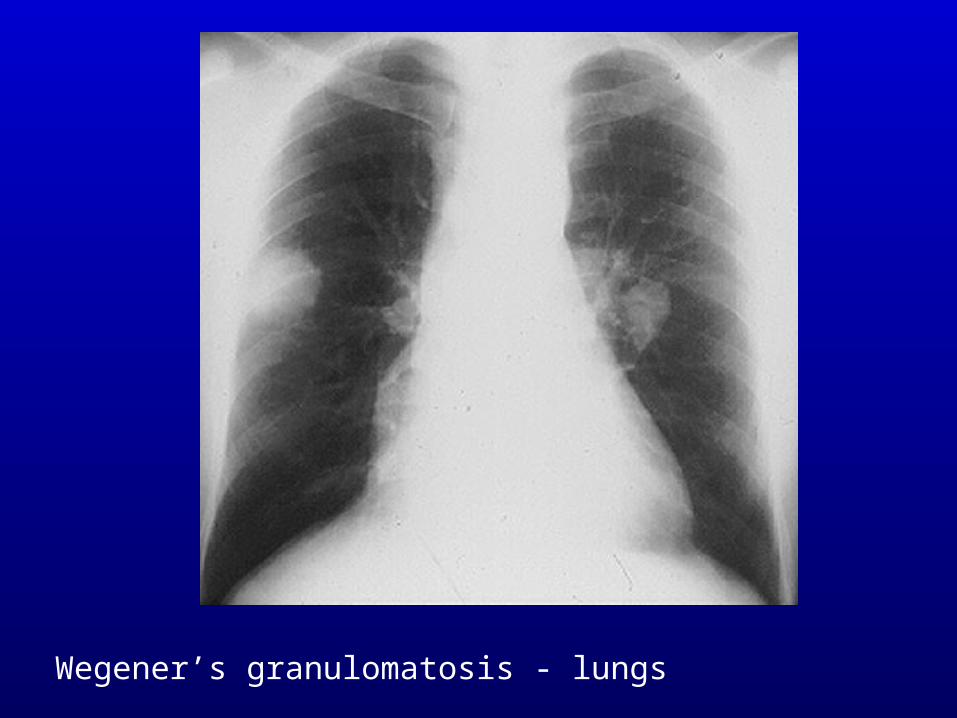
Wegener’s granulomatosis - lungs
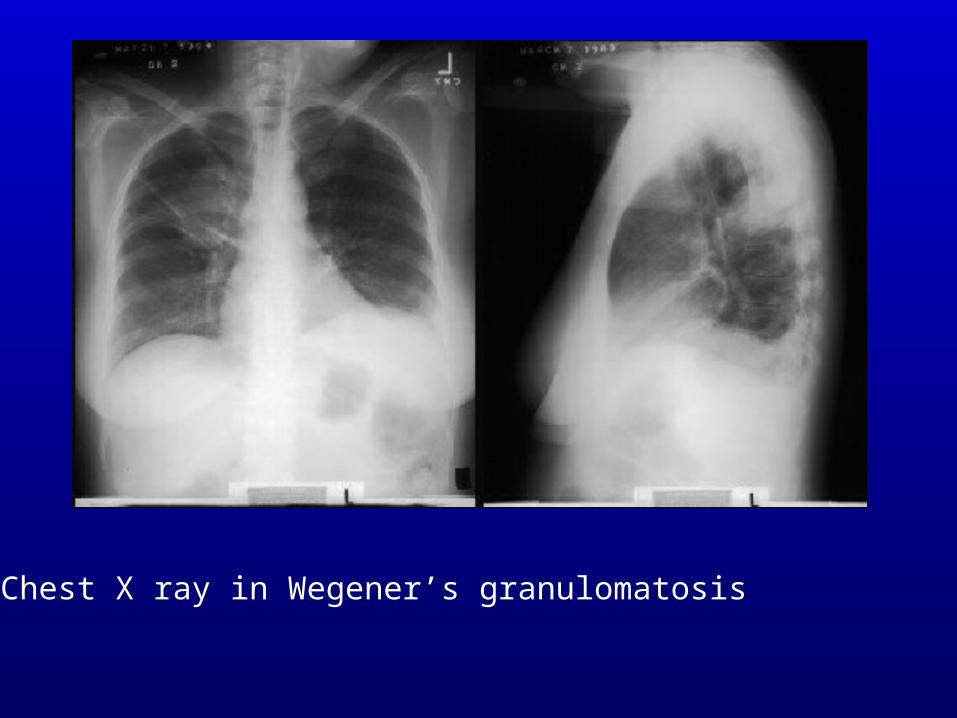
Chest X ray in Wegener’s granulomatosis
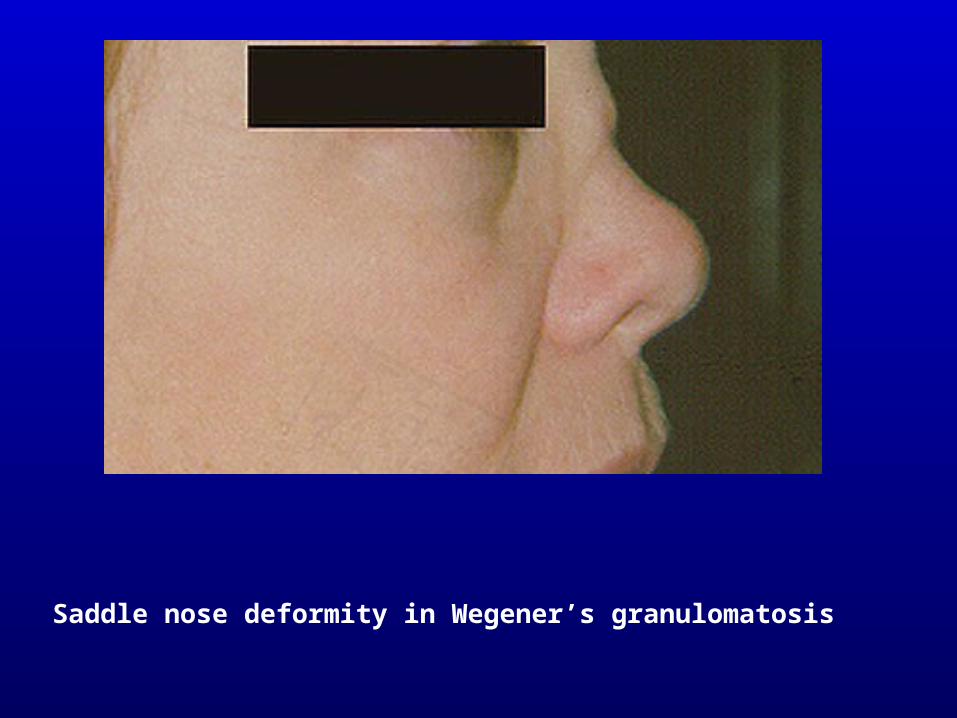
Saddle nose deformity in Wegener’s granulomatosis
Classification criteria of hypersensitivity vasculitis (ACR, 1990)
1 Age at onset over 16 years2 Medication at disease onset3 Palpable purpura (slightly elevated purpuric rash over one or more
areas of the skin; does not blench with pressure and is not related to thrombocytopenia)
4 Maculopapular rash (flat or raised lesions of various sizes over one or more areas of the skin)
5 Biopsy (granulocytes in a peri- or extravascular localisation)
Diagnosis is based on the presence of at least 3 criteria.
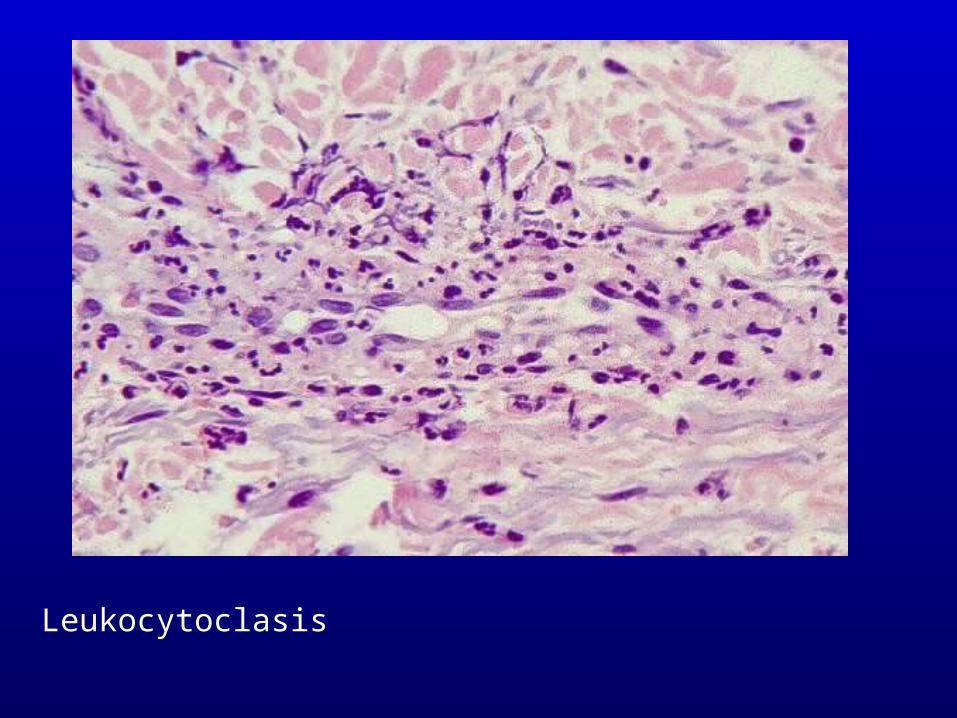
Leukocytoclasis

Cutaneous leukocytoclastic vasculitis

Cryoglobulinemia

Cyoglobulinemia - HBsAg+

Vasculitis in RA
Classification criteria of Henoch-Schönlein purpura (ACR, 1990)
1 Palpable purpura2 Age 20 years at disease onset3 Bowel angina (diffuse abdominal pain, worse after meals, or
bloody diarrhea)4 Biopsy (granulocytes in the walls of arterioles and venules)
Diagnosis is based on the presence of at least 2 criteria.

H-S purpura – palpable purpura

H-S purpura
Classification criteria of giant cell arteritis (temporal arteritis) (ACR, 1990)
1 Age at onset 50 years2 "New" headache (new onset or new type of localized pain)3 Temporal artery abnormality (tenderness to palpation or decreased
pulsation, unrelated to other causes, e.g. arteriosclerosis)4 Elevated ESR (50 mm/hr)5 Abnormal artery biopsy (vasculitis with mononuclear cell infiltration
or granulomatous inflammation with multinucleated giant cells)
Diagnosis is based on the presence of at least 3 criteria.
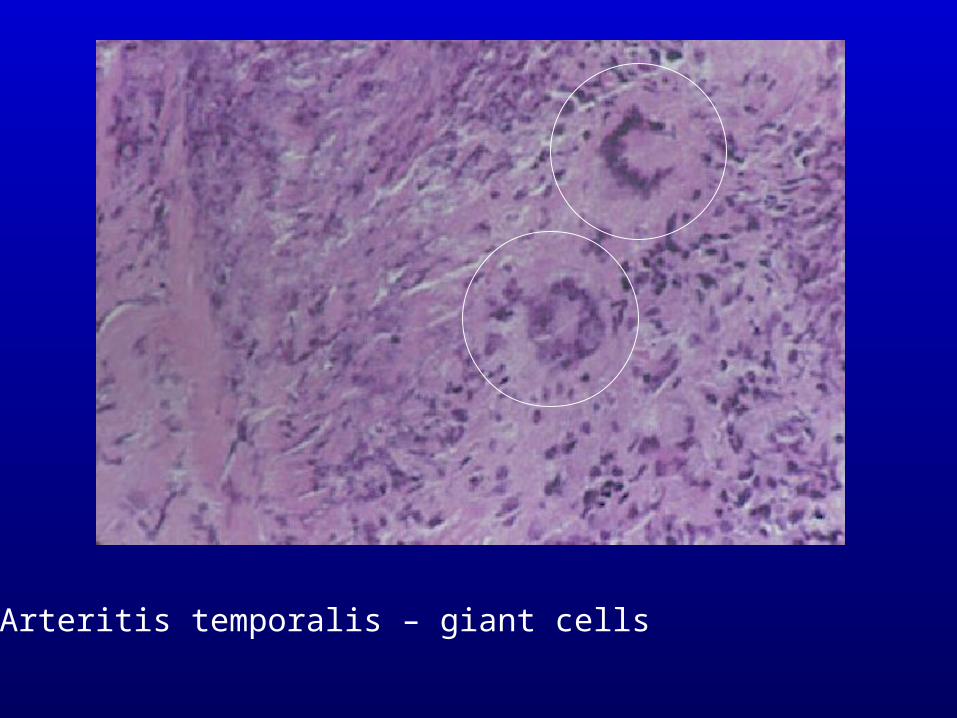
Arteritis temporalis – giant cells

Inflamed, painful arteria temporalis
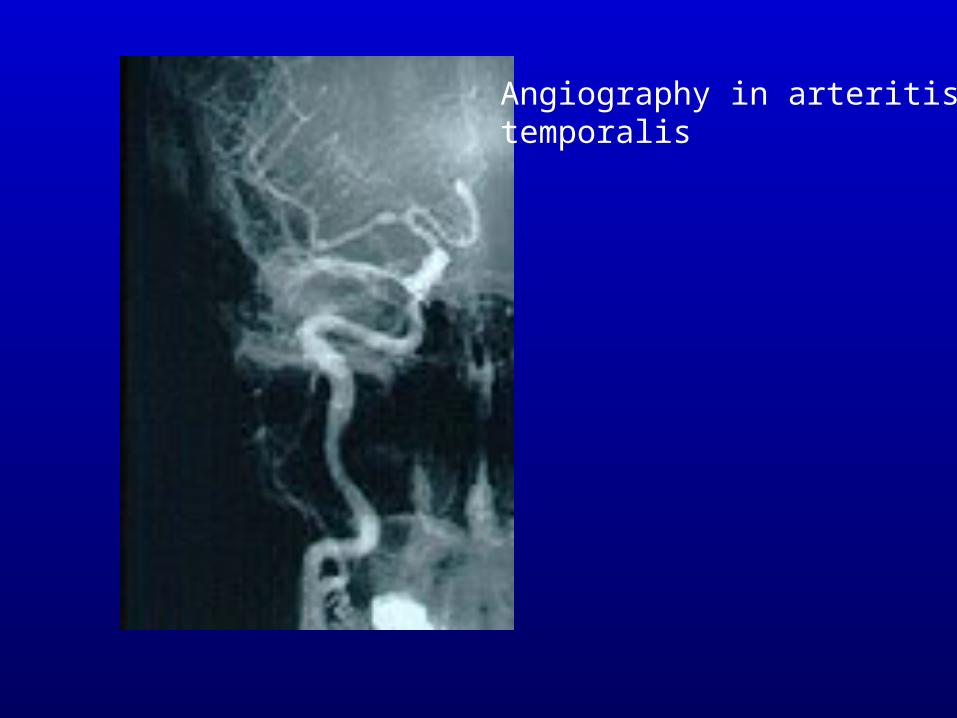
Angiography in arteritistemporalis
Diagnostic criteria of polymyalgia rheumatica (Healey, 1984)
Absolute criterium: onset after 50 ys of age
Other criteria: 1 Neck, shoulder or hip pain 2. Morning stiffness for at least 2 hrs 3 Elevated ESR (>40 mm/hr) 4 Rapid response to low dose corticosteroid
<20 mg prednisolone/day)
Diagnosis is based on the absolute criteria + 3 others
Classification criteria of Takayasu’s arteritis (ACR, 1990)
1 Onset before 40 ys of age2 Claudication of extremities (pain or dyscomfort on movement,
mostly in upper extremities)3 Decreased brachial artery pulse (decreased pulsation of one or both
brachial arteries)4 More than 10 mm Hg difference in systolic blood pressure between
arms5 Bruit over subclavian arteri(es) or (abdominal) aorta6 Arteriogram abnormality (occlusion or narrowing of the aorta,
its branches or large arteries, not due to other cause, e.g. arteriosclerosis, etc.)
At least 3 criteria are required for a definite diagnosis.
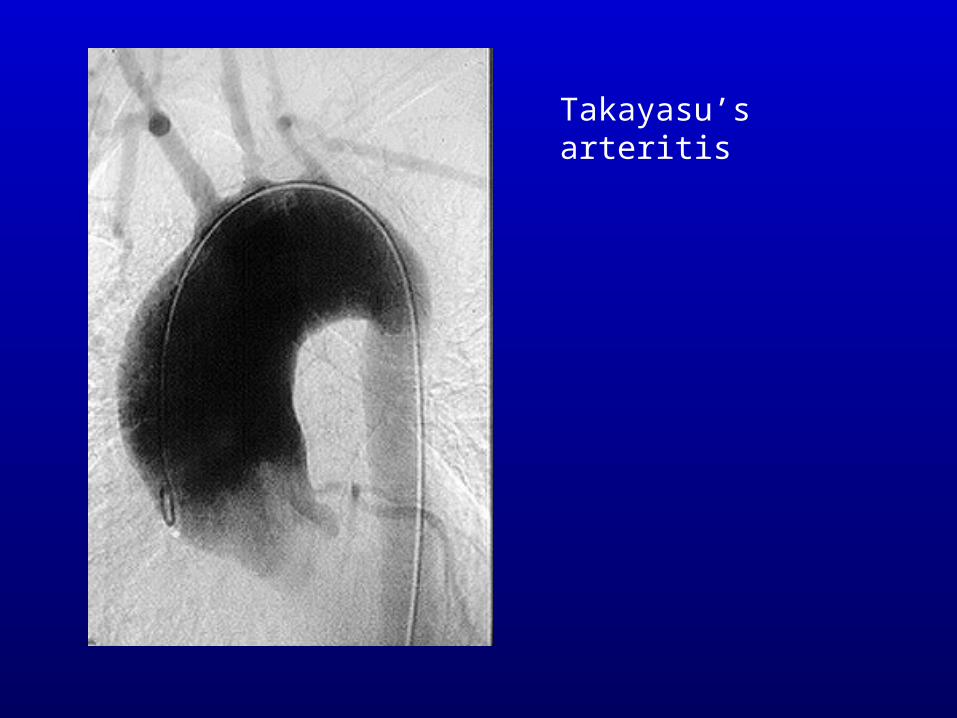
Takayasu’sarteritis
Diagnostic criteria of Kawasaki disease (American Heart Association, 1990):
1. Fever, persisting 5 days or more (with no other cause)2. At least four of the followings:
a) Non exudative conjunctival congestionb) Oropharyngeal signs: mucosal erythema, or
reddening of lips, orstrawberry tongue
c) Peripheral extremities: reddening of palms and soles, in-durative edema, membranous desquamation of fingertips
d) Polymorphous exanthemae) Acute nonpurulent cervical lymphadenopathy (one or more
lymph nodes with at least 1.5 cm diameter)
Diagnosis requires at least 4 criteria. In case of coronary involvement and less than 4 criteria, atypical Kawasaki disease diagnosis may be made.
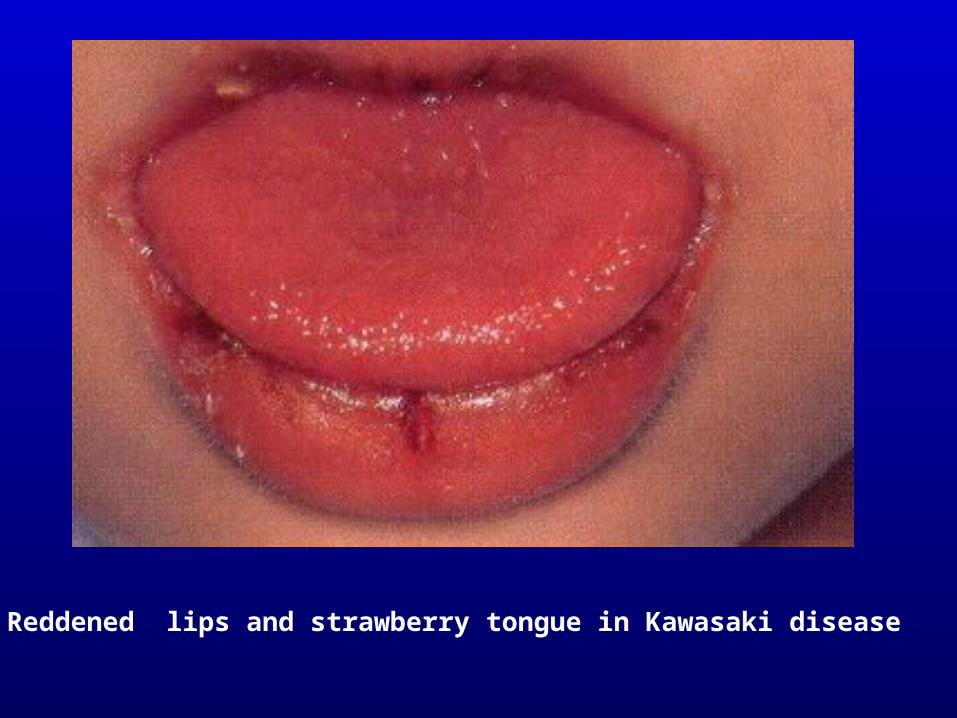
Reddened lips and strawberry tongue in Kawasaki disease
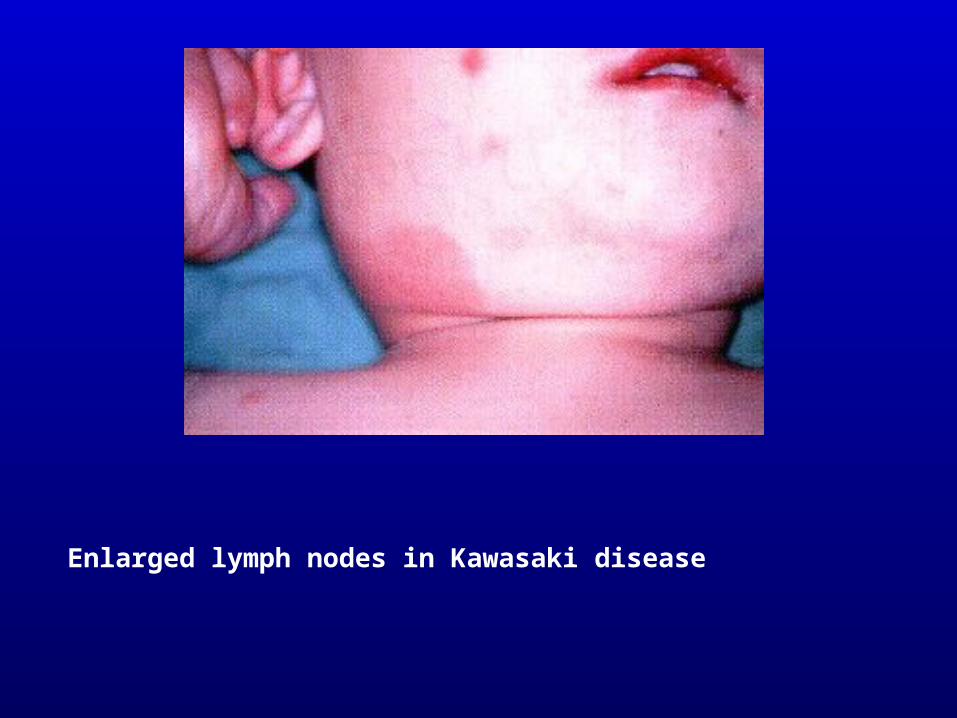
Enlarged lymph nodes in Kawasaki disease

Membranous desquamation of fingertips in Kawasaki disease
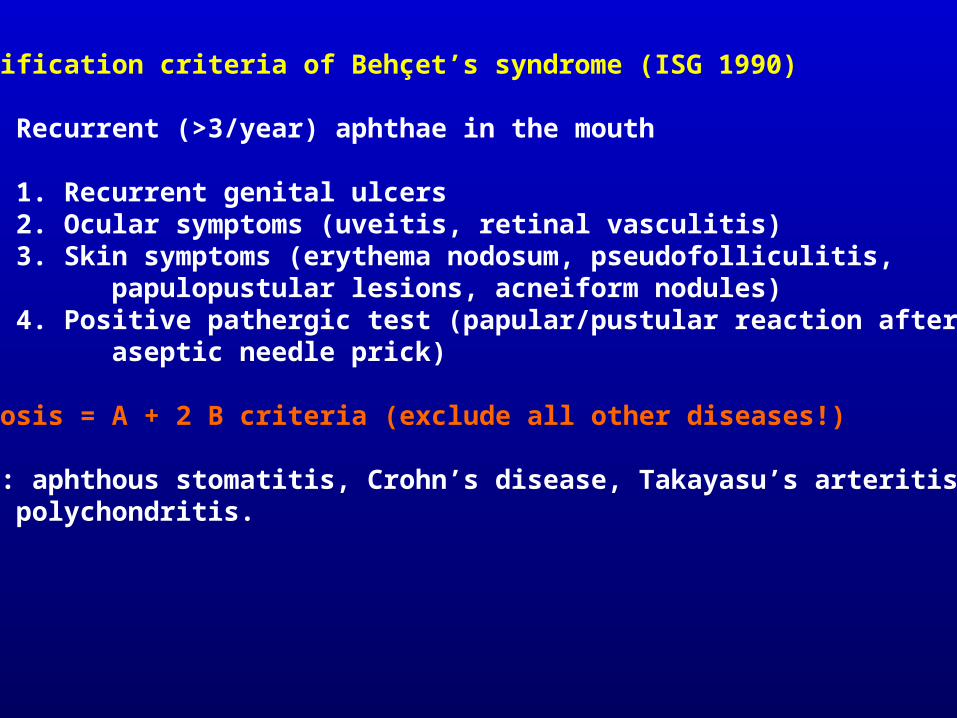
Classification criteria of Behçet’s syndrome (ISG 1990)
A Recurrent (>3/year) aphthae in the mouth
B 1. Recurrent genital ulcers2. Ocular symptoms (uveitis, retinal vasculitis)3. Skin symptoms (erythema nodosum, pseudofolliculitis,
papulopustular lesions, acneiform nodules)4. Positive pathergic test (papular/pustular reaction after an
aseptic needle prick)
Diagnosis = A + 2 B criteria (exclude all other diseases!)
Other: aphthous stomatitis, Crohn’s disease, Takayasu’s arteritis,polychondritis.
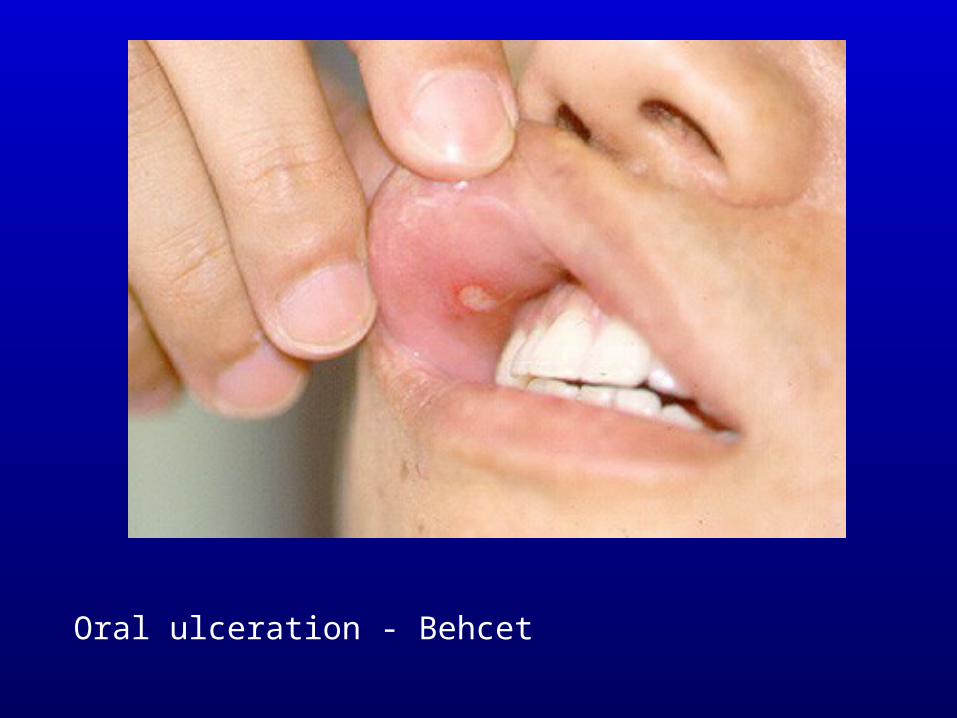
Oral ulceration - Behcet
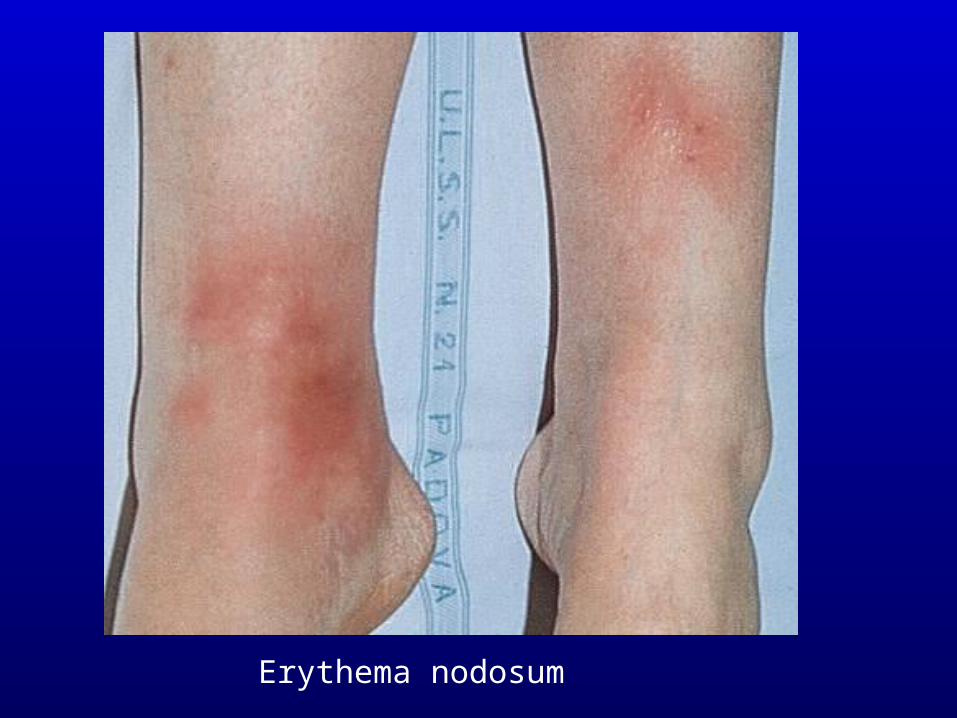
Erythema nodosum
Therapy
1. Periarteritis (PAN), Wegener’s granulomatosis, and microscopic polyangiitis:
Starting with 1-4 mg/kg/day corticosteroid (CS) + 100 mg/day p.o. cyclophospgamide (CTX), followed by CTX monotherapy (generally for 2 years). In case of intolerance, azathioprine (100 mg/day) or methotrexate (MTX) (25 mg/week) adható. In mild Wegener’s co-trimoxazol (Sumetrolim) therapy may be sufficient.
2. Schönlein-Henoch purpura: 0.5-1 mg/kg/day CS. Arthritis will respond to NSAID, long-term prognosis is determined by kidney disease.
3. Cryoglobulinemia: in “idiopathic”, hepatitis C virus positive cases, complex antiviral treatment (interferon-alpha + ribavirin) is required, CS, or CS+azathioprine therapy affects only arthritis and purpura, but not glomerulonephritis.
Therapy (cont’d)
4. Temporal arteritis: in mild cases 0.5 mg/kg/day CS, or NSAID may be sufficient. In more severe cases 1-2 mg/kg/day CS is recommended. If inflammation last for longer, azathioprine may be added to CS.
5. Polymyalgia rheumatica: In general 0.5 mg/kg/day CS (25 mg/day prednisolon or 20 mg methylprednisolon) is sufficient.
6. Takayasu’s arteritis: only in early active stage: 1 mg/kg/day CS and/or CTX for ½-1 year. In later stage: surgery.
7. Kawasaki betegség: in mild cases NSAID, in case of coronaritis high dose intravenous immune globulin (IVIG) (0.4 mg/kg/dose).
8. Behçet’s syndrome. In skin and mucous membrane involvation: 1-2 mg/kg/day CS, or colchicin, NSAID. In case of uveitis, retina vasculitis 1-2 mg/kg/day CS + 5-6 mg/kg/day cyclosporine! In arthritis NSAID, 1 mg/kg/day CS, azathioprine, or CTX may be required. In thrombophlebitis esetén: heparin, or warfarin.