vasculitis board review: 2019reviews.berlinpharm.com/20190316/vasculitis.pdf · 2. exclude...
TRANSCRIPT
3/6/2019
1
Vasculitis Board Review: 2019
Asso. Prof. Sumapa Chaiamnuay Rheumatic Disease Unit
Department of Medicine Phramongkutklao Hospital and College of Medicine
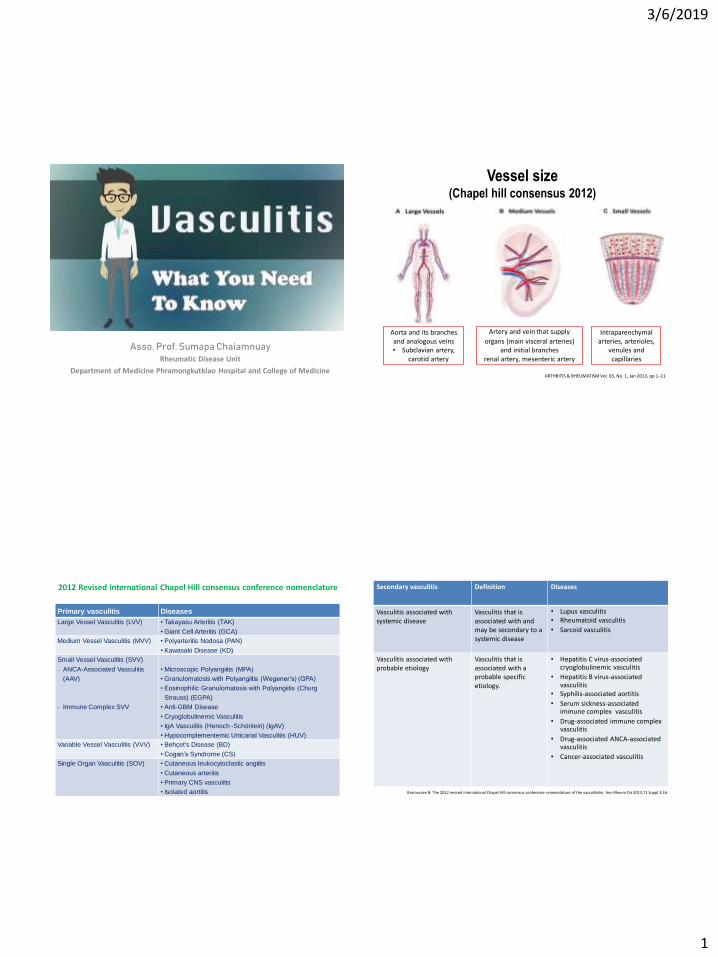
Vessel size (Chapel hill consensus 2012)
ARTHRITIS & RHEUMATISM Vol. 65, No. 1, Jan 2013, pp 1–11
Aorta and its branches and analogous veins • Subclavian artery,
carotid artery
Artery and vein that supply
organs (main visceral arteries) and initial branches
renal artery, mesenteric artery
Intraparenchymal arteries, arterioles,
venules and capillaries
2012 Revised international Chapel Hill consensus conference nomenclature
Primary vasculitis Diseases
Large Vessel Vasculitis (LVV) • Takayasu Arteritis (TAK)
• Giant Cell Arteritis (GCA)
Medium Vessel Vasculitis (MVV) • Polyarteritis Nodosa (PAN)
• Kawasaki Disease (KD)
Small Vessel Vasculitis (SVV)
ANCA-Associated Vasculitis
(AAV)
Immune Complex SVV
• Microscopic Polyangiitis (MPA)
• Granulomatosis with Polyangiitis (Wegener’s) (GPA)
• Eosinophilic Granulomatosis with Polyangiitis (Churg
Strauss) (EGPA)
• Anti-GBM Disease
• Cryoglobulinemic Vasculitis
• IgA Vasculitis (Henoch -Schönlein) (IgAV)
• Hypocomplementemic Urticarial Vasculitis (HUV)
Variable Vessel Vasculitis (VVV) • Behçet's Disease (BD)
• Cogan’s Syndrome (CS)
Single Organ Vasculitis (SOV) • Cutaneous leukocytoclastic angiitis
• Cutaneous arteritis
• Primary CNS vasculitis
• Isolated aortitis
Secondary vasculitis Definition Diseases
Vasculitis associated with systemic disease
Vasculitis that is associated with and may be secondary to a systemic disease
• Lupus vasculitis • Rheumatoid vasculitis • Sarcoid vasculitis
Vasculitis associated with probable etiology
Vasculitis that is associated with a probable specific etiology.
• Hepatitis C virus-associated cryoglobulinemic vasculitis
• Hepatitis B virus-associated vasculitis
• Syphilis-associated aortitis • Serum sickness-associated
immune complex vasculitis • Drug-associated immune complex
vasculitis • Drug-associated ANCA-associated
vasculitis • Cancer-associated vasculitis
Rasmussen N. The 2012 revised international Chapel Hill consensus conference nomenclature of the vasculitides. Ann Rheum Dis 2012;71 Suppl 3:16.
3/6/2019
2
Clinical approach
1. Suspected vasculitis
• Constitutional symptom
• Multiple organ involvement
• Sign& symptom
2. Exclude vasculitis mimics
3. secondary vasculitis
4. Defining primary systemic vasculitis 5. Principal of treatment
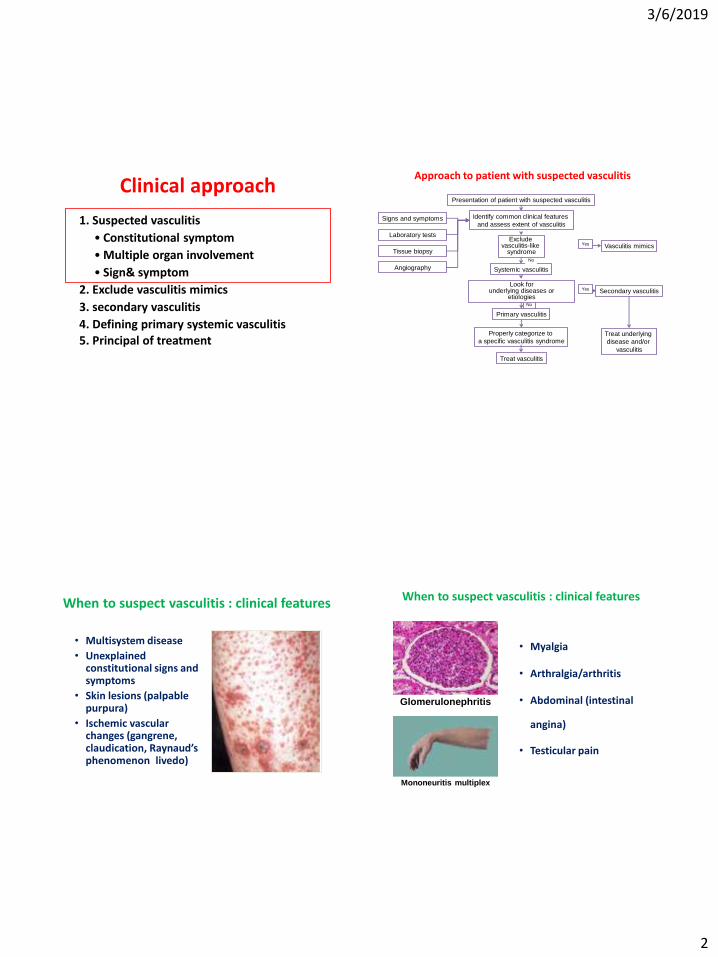
Approach to patient with suspected vasculitis
Presentation of patient with suspected vasculitis
Identify common clinical features
and assess extent of vasculitis
Systemic vasculitis
Vasculitis mimics
Primary vasculitis
Secondary vasculitis
Properly categorize to
a specific vasculitis syndrome
Signs and symptoms
Laboratory tests
Tissue biopsy
Angiography
Treat vasculitis
Treat underlying
disease and/or
vasculitis
Yes
Yes
No
No
Look for underlying diseases or
etiologies
Exclude vasculitis-like
syndrome
When to suspect vasculitis : clinical features
• Multisystem disease
• Unexplained constitutional signs and symptoms
• Skin lesions (palpable purpura)
• Ischemic vascular changes (gangrene, claudication, Raynaud’s phenomenon, livedo)
• Myalgia
• Arthralgia/arthritis
• Abdominal (intestinal
angina)
• Testicular pain
When to suspect vasculitis : clinical features
Glomerulonephritis
Mononeuritis multiplex
3/6/2019
3
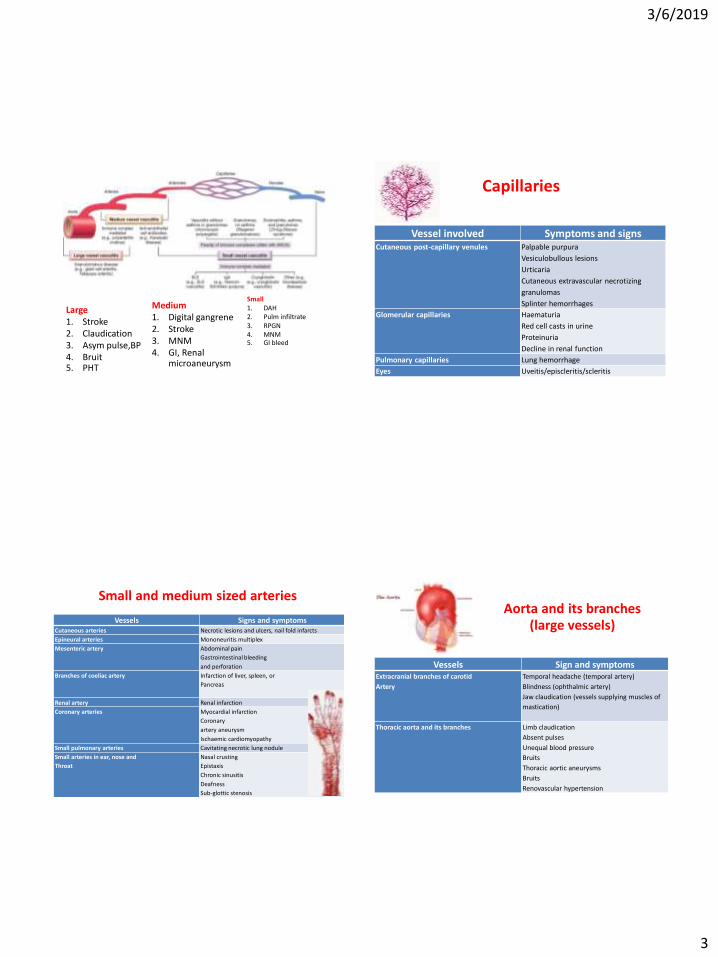
Large 1. Stroke 2. Claudication 3. Asym pulse,BP 4. Bruit 5. PHT
Medium 1. Digital gangrene 2. Stroke 3. MNM 4. GI, Renal
microaneurysm
Small 1. DAH 2. Pulm infiltrate 3. RPGN 4. MNM 5. GI bleed
Capillaries
Vessel involved Symptoms and signs Cutaneous post-capillary venules Palpable purpura
Vesiculobullous lesions
Urticaria
Cutaneous extravascular necrotizing
granulomas
Splinter hemorrhages
Glomerular capillaries Haematuria
Red cell casts in urine
Proteinuria
Decline in renal function
Pulmonary capillaries Lung hemorrhage
Eyes Uveitis/episcleritis/scleritis
Small and medium sized arteries
Vessels Signs and symptoms Cutaneous arteries Necrotic lesions and ulcers, nail fold infarcts
Epineural arteries Mononeuritis multiplex
Mesenteric artery Abdominal pain
Gastrointestinal bleeding
and perforation
Branches of coeliac artery
Infarction of liver, spleen, or
Pancreas
Renal artery Renal infarction
Coronary arteries Myocardial infarction
Coronary
artery aneurysm
Ischaemic cardiomyopathy
Small pulmonary arteries Cavitating necrotic lung nodule
Small arteries in ear, nose and
Throat
Nasal crusting
Epistaxis
Chronic sinusitis
Deafness
Sub-glottic stenosis
Vessels Sign and symptoms Extracranial branches of carotid
Artery
Temporal headache (temporal artery)
Blindness (ophthalmic artery)
Jaw claudication (vessels supplying muscles of
mastication)
Thoracic aorta and its branches Limb claudication
Absent pulses
Unequal blood pressure
Bruits
Thoracic aortic aneurysms
Bruits
Renovascular hypertension
Aorta and its branches (large vessels)

3/6/2019
4
UV, PP (HSP,CLA)
Venule/cap/arterioles Arterioles/small artery Small-artery
skin ulcer (ANCA) LVR, panniculitis, EN like, nodule, (PAN)
Clinical approach
1. Suspected vasculitis
• Constitutional symptom
• Multiple organ involvement
• Sign& symptom
2. Exclude vasculitis mimics
3. secondary vasculitis
4. Defining primary systemic vasculitis 5. Principal of treatment
Vasculitis: exclude mimics
• Emboli – Crystal
– Endocarditis
• Thrombosis – Anti-phospholipid syndrome
– Thrombocytopenic purpura
• Infection – Gonococcal
– Sepsis
Vasculitis Mimics (1) Diseases
Infectious diseases Bacterial endocarditis
Coccidioidomycosis
Disseminated gonococcal infection
Lyme disease
Rocky Mountain spotted fever
Syphilis
Whipple's disease
Drug-related Amphetamines
Arsenic
Cocaine
Ergot alkaloids
Methysergide

3/6/2019
5
Vasculitis Mimics (2) Diseases
Coagulopathy / microangiopathy Antiphospholipid syndrome
Cryofibrinogenemia
Thrombotic thrombocytopenic purpura
Neoplasms Atrial myxoma
Paraneoplastic syndrome
Miscellaneous Amyloidosis
Atherosclerosis, calciphylaxis
Cholesterol crystal emboli
Coarctation of aorta
Fibromuscular dysplasia
Migraine
Neurofibromatosis
Sarcoidosis
Sickle cell disease
Clinical approach
1. Suspected vasculitis
• Constitutional symptom
• Multiple organ involvement
• Sign& symptom
2. Exclude vasculitis mimics
3. secondary vasculitis
4. Defining primary systemic vasculitis 5. Principal of treatment
Secondary causes of vasculitis 1. Autoimmune diseases
Systemic lupus erythematosus
Sjögren's syndrome
Behçet disease
Rheumatoid vasculitis
Ulcerative colitis
Crohn's disease
Sarcoidosis
2. Infectious diseases Viruses (HIV, CMV)
Bacteria (spirochaetales, mycobacteria, streptococci, tropheryma
whippeli)
Parasites (e.g. Ascaris etc.)
Fungi (e.g. Aspergillus)
3. Neoplasia Non‐Hodgkin lymphoma
Myeloproliferative diseases
Solid tumours
Atrial myxomas
4. Drug abuse (intoxication) Opioids (cocaine, morphine)
5. Drug‐induced Antihypertensive (hydralazine)
Antithyroid drugs (propylthiouracil, methimazole, carbamizole)
Antibiotics (azithromycin, minocycline)
Antifibrotic (penicillamine)
Leukotriene receptor antagonist (zafirlukast, montelukast, pranlukast)
Infection mimics vasculitis
Vessel size Organism
Large Bacterial
Spirochete
Fungus
Staphylococcus, Salmonella, mycobacteria, Streptococcus
Treponema pallidum
Coccidiomycosis
Medium Bacteria
Virus
Group A Streptoccus, mycobacteria
HBV, HCV, HIV, parvovirus B19
Small and
medium
Bacteria
Virus
Streptococcus
HBV, HCV, HIV, CMV
Small
Bacteria
Virus
Staphylococcus, Salmonella, mycobacteria,
Streptococcus, Yersinia, Neisseria, Rickettsia
HIV, CMV, herpes zoster, parvovirus B19, HBV, HCV
Somer T, et al. Vasculitides associated with infections, immunization, and antimicrobial drugs. Clin Infect Dis 1995;20:1010-36.
3/6/2019
6
Secondary vasculitis/mimicker Vessel size Secondary vasculitis Mimicker
Large Syphilis ,TB, RA FMD, radiation fibrosis, NF, coarctation of aorta, APS
Medium RA, SLE, SS, drug Cholesterol emboli, atrial myxoma, thromboembolic disease, ergotism, APS,MPD, ED IV
Small SLE, SS, RA, DM, drug GC, meningococemia, pseudomonase, HIV,HBV,HCV,CMV, EBV Lymphomatoid granulomatosis
IE, mycotic aneurysm, cholesterol emboli, APS, TTP calciphylaxis
Drug : penicillin, sulfonamide, pill, allopurinol, PTU, Hydralazine
Clinical approach
1. Suspected vasculitis
• Constitutional symptom
• Multiple organ involvement
• Sign& symptom
2. Exclude vasculitis mimics
3. secondary vasculitis
4. Defining primary systemic vasculitis 5. Principal of treatment
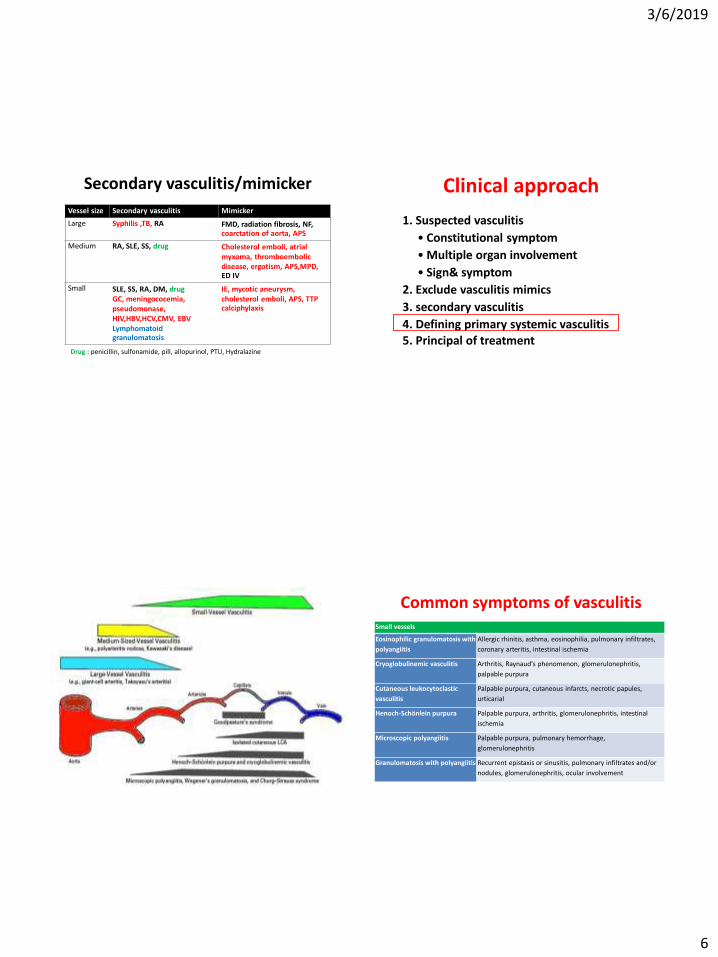
Common symptoms of vasculitis Small vessels
Eosinophilic granulomatosis with
polyangiitis
Allergic rhinitis, asthma, eosinophilia, pulmonary infiltrates,
coronary arteritis, intestinal ischemia
Cryoglobulinemic vasculitis Arthritis, Raynaud's phenomenon, glomerulonephritis,
palpable purpura
Cutaneous leukocytoclastic
vasculitis
Palpable purpura, cutaneous infarcts, necrotic papules,
urticarial
Henoch-Schönlein purpura Palpable purpura, arthritis, glomerulonephritis, intestinal
ischemia
Microscopic polyangiitis Palpable purpura, pulmonary hemorrhage,
glomerulonephritis
Granulomatosis with polyangiitis Recurrent epistaxis or sinusitis, pulmonary infiltrates and/or
nodules, glomerulonephritis, ocular involvement
3/6/2019
7
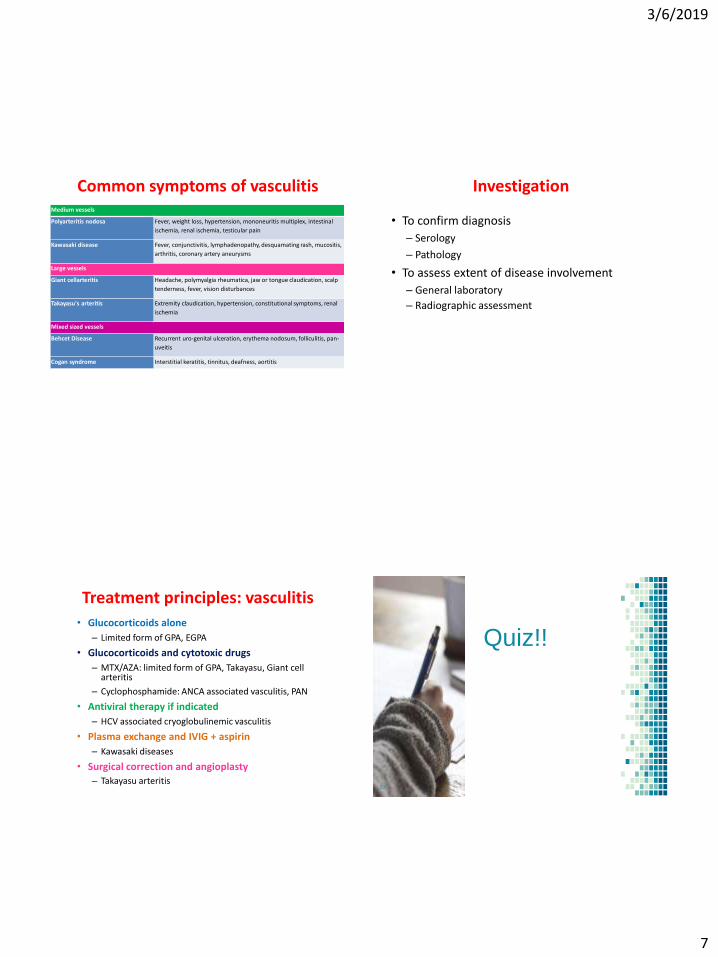
Medium vessels
Polyarteritis nodosa Fever, weight loss, hypertension, mononeuritis multiplex, intestinal
ischemia, renal ischemia, testicular pain
Kawasaki disease Fever, conjunctivitis, lymphadenopathy, desquamating rash, mucositis,
arthritis, coronary artery aneurysms
Large vessels
Giant cellarteritis Headache, polymyalgia rheumatica, jaw or tongue claudication, scalp
tenderness, fever, vision disturbances
Takayasu's arteritis Extremity claudication, hypertension, constitutional symptoms, renal
ischemia
Mixed sized vessels
Behcet Disease Recurrent uro-genital ulceration, erythema nodosum, folliculitis, pan-
uveitis
Cogan syndrome Interstitial keratitis, tinnitus, deafness, aortitis
Common symptoms of vasculitis Investigation
• To confirm diagnosis
– Serology
– Pathology
• To assess extent of disease involvement
– General laboratory
– Radiographic assessment
Treatment principles: vasculitis • Glucocorticoids alone
– Limited form of GPA, EGPA
• Glucocorticoids and cytotoxic drugs
– MTX/AZA: limited form of GPA, Takayasu, Giant cell arteritis
– Cyclophosphamide: ANCA associated vasculitis, PAN
• Antiviral therapy if indicated
– HCV associated cryoglobulinemic vasculitis
• Plasma exchange and IVIG + aspirin
– Kawasaki diseases
• Surgical correction and angioplasty
– Takayasu arteritis
Quiz!!
29
3/6/2019
8
Q62 MKSAP18
A 26 years old woman is evaluated for a 4 weeks history of progressive dyspnea on exertion. She has malaise myalgia and arms ache with activity for the past 6 months.
No rash, jaw claudication, GI or neuro symptoms
PE: Rt arm 120/60 Lt arm 95/50
↓Radial pulse Lt arm
Heart: grade 2/6 diastolic murmur at LPSB
Lab: Hct 30% WBC 11,000 Plt 439k ESR 90 Cr 1.1
What is the following is the most likely diagnosis?
A. Takayasu arteritis
B. Polyarteritis nodosa
C. Giant cell arteritis
D. Kawasaki disease
MKSAP18 Q77
A 28 years old woman presented with 3 weeks history of progressive
worsening pain in the left arm which was worsen with the use of it.
Fatigue, malaise, low-grade fever, inability to walk long distance.
BT 38.1 BP right 166/95 left 115/60 PR 72/min
↓left radial and both dorsalis pedis pulses
+ abdominal bruit
No rash
LAB:
ESR 115 Cr 1.4 mg/dL Hct 32% WBC 10,500 PMK 70% Plt 510k
Which of the following is the most appropriate next diagnostic test?
A. Anti-phospholipid antibodies B. Anti-myeloperoxidase antibody
C. Temporal artery biopsy D. Aortic arteriography
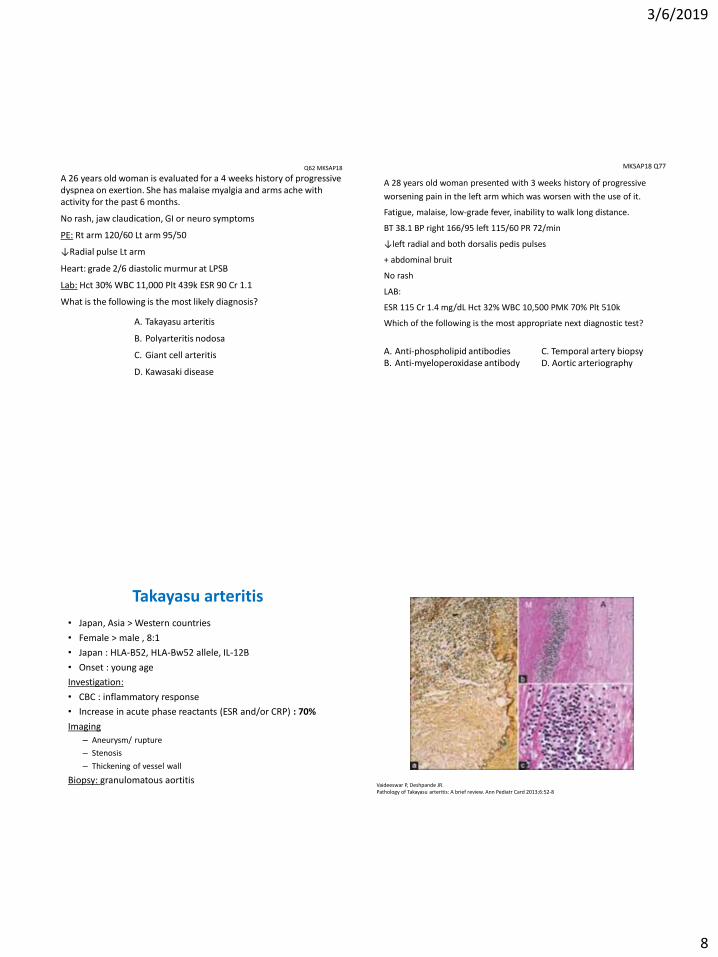
Takayasu arteritis
• Japan, Asia > Western countries
• Female > male , 8:1
• Japan : HLA-B52, HLA-Bw52 allele, IL-12B
• Onset : young age
Investigation:
• CBC : inflammatory response
• Increase in acute phase reactants (ESR and/or CRP) : 70%
Imaging
– Aneurysm/ rupture
– Stenosis
– Thickening of vessel wall
Biopsy: granulomatous aortitis
Vaideeswar P, Deshpande JR. Pathology of Takayasu arteritis: A brief review. Ann Pediatr Card 2013;6:52-8

3/6/2019
9
E17 Q17 GCA
An 82 years old woman is evaluated for a 2-wk history of left-sided headaches with pain on chewing, shoulders and hip achiness.
U/D: HTN, dyslipid
PE: BP 130/80 BT 38.1c
Tenderness and swelling over left temporal area
Limit ROM of shoulders and hips due to pain
Lab: CBC, cr, LFT -normal. ESR 85
What is the most helpful investigation to establish diagnosis?
A. Temporal artery biopsy B. Lumbar puncture C. MRI brain with gadolinium D. hs-CRP E. Rheumatoid factor
Clinical manifestations of GCA
• Onset: gradual >> abrupt
• Systemic symptoms
– Fever (50%), usually low grade
– Fatigue
– Weight loss
• Headache (60-70%): new onset
– Pain over the temporal areas (may be frontal, occipital or generalise)
– Variable course
– Tender temporal or occipital arteries (30%)
• Jaw claudication (50%)
– Most specific sign of GCA
– Occur with repeated swallowing and in the tongue with eating
Clinical manifestations of GCA • Polymyalgia rheumatica
– Aching and morning stiffness in the shoulder and hip girdles, in the neck, and in the torso.
– PMR occurs in about 40 – 50% of GCA patients
– GCA occurs in about 15 % of PMR patients
• Joint pain and arthritis
• Arm claudication 3 – 15%
– Subclavian and axillary arteries involvement
– Gradual tapering
• Central nervous system involvement
– Documented involvement of intracranial vessels in GCA is rare
– When transient ischemic attacks, vertigo, hearing loss, and stroke occur in GCA, they are most often due to vertebral artery involvement or to internal carotid lesions that are extradural in location
Polymyalgia rheumatica
• Age > 50 years
• Constitutional symptoms
• Aching and stiffness of shoulder, axial musculature and tendinous attachments, often bilaterally
• Elevated ESR/CRP
• 10-15% have positive of temporal arteries biopsy
• PMR itself does not appear to cause vision loss
• Responds to low doses of GC (pred 20-30 mg/day)
3/6/2019
10
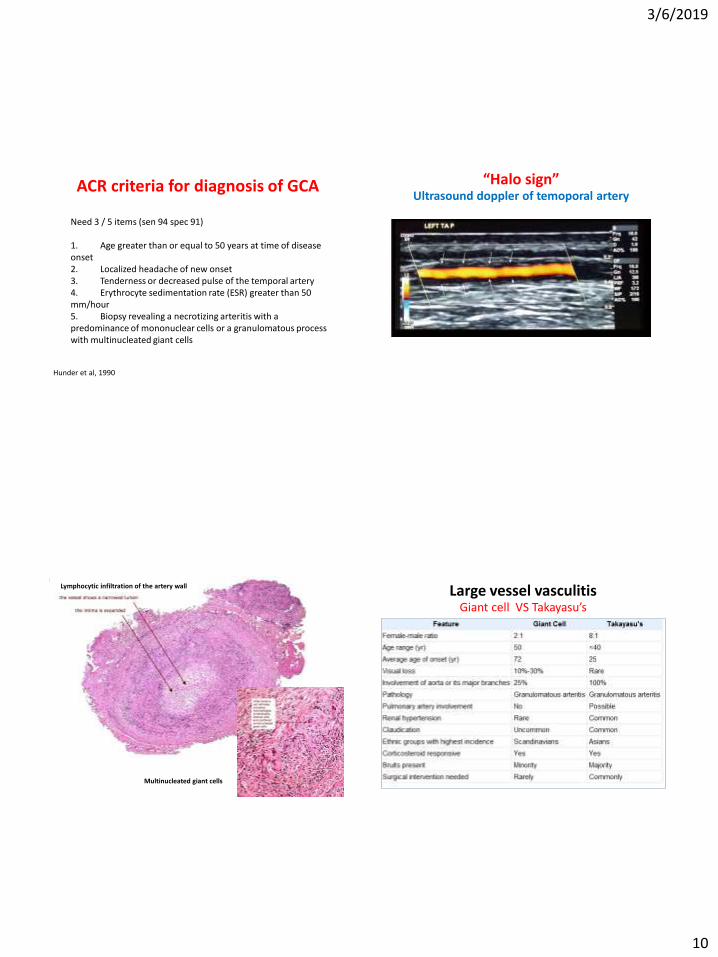
ACR criteria for diagnosis of GCA
Need 3 / 5 items (sen 94 spec 91) 1. Age greater than or equal to 50 years at time of disease onset 2. Localized headache of new onset 3. Tenderness or decreased pulse of the temporal artery 4. Erythrocyte sedimentation rate (ESR) greater than 50 mm/hour 5. Biopsy revealing a necrotizing arteritis with a predominance of mononuclear cells or a granulomatous process with multinucleated giant cells
Hunder et al, 1990
“Halo sign” Ultrasound doppler of temoporal artery
Lymphocytic infiltration of the artery wall
Multinucleated giant cells
Large vessel vasculitis Giant cell VS Takayasu’s

3/6/2019
11
What is the most appropriate immediate next step management?
A. Initiate prednisolone 15 mg/day
B. Initiate prednisolone 60 mg/day
C. Obtain MRI brain
D. Obtain temporal artery biopsy
E. Lumbar puncture
What is the most appropriate treatment?
A. Prednisolone 15 mg/day
B. Prednisolone 60 mg/day
C. Pulse methylprednisolone 1 gm iv x 3 day
D. Aspirin 81 mg/day
E. B + D
Treatment of GCA • Induction
– High dose steroid
• Pred 1 mkd (avoid alternate dosing)
• Pulse methylprednisolone 500-1000 mg iv x 3 d for patients with visual loss or a history of amaurosis fugax
– Give until complete resolution of symptoms and inflammatory markers
• Maintenance
– ↓ 10 mg of pred q 2 wk to 20 mg then
– ↓2.5 mg q 2-4 wk to 10 mg then
– ↓1 mg q 1-2 mo
• Early methotrexate or other alternative immunosuppressant
therapy following a relapse
• Add aspirin + bone protection + GI protection
Ponte C 2015 Current management of giant cell arteritis

3/6/2019
12
A 69 years old woman with severe headache and right eye blindness
CC: Sudden visual loss in her left eye 1 hour
HPI:
She had several episodes of transient loss of vision in her left eye in the previous weeks which resolved spontaneously. Eye examination as normal.
ROS: She had temporal headaches and jaw claudication for a few weeks. She did not show weight loss or systemic fever
PE:
Left scalp tenderness with nodular and pulseless temporal artery was noted.
Visual acuity was no light perception
Fundoscopy: a pale and edematous optic disk and ischemia of the papillomacular bundle area which was also noticed on fluorescein angiography
What is the most appropriate treatment?
A. Prednisolone 15 mg/day
B. Prednisolone 60 mg/day
C. Pulse methylprednisolone 1 gm iv x 3 day
D. Aspirin 81 mg/day
E. C + D
A 41 years old man with acute severe abdominal pain
The pain was excruciating and sudden in onset, originating in his right lower quadrant and radiating to his right groin and flank
Two weeks PTA:
A less severe episode of similar pain but in his left lower quadrant, with radiation to his left flank, which subsequently resolved
Fatigue for several months preceding these episodes
BP 180/100
Abdomen: soft, generalized tender, no guarding or rebound tenderness, normal BS, bilateral CVA tenderness
Laboratory test:
WBC 14,280 78% PMN. Hb12.6 g/dL, plt 215,000
BUN 8 mg/dL, Cr 1.5 mg/dL
CRP 181 mg/dL (normal < 3)
PT, INR, PTT, electrolyte, LFT, amylase, lipase-normal
UA: 1+ protein, rbc 10-20, no cast
Echocardiogram: normal
N Engl J Med 2014;370:70-5

3/6/2019
13
CT abdomen: infarcts in both kidneys, with focal volume loss in the left kidney that was suggestive of scarring
N Engl J Med 2014;370:70-5
Problem lists
1. HTN
2. Bilateral renal infarcts
3. Fatigue
What is the most likely diagnosis?
Echocardiogram: normal Hypercoagulable: neg
N Engl J Med 2014;370:70-5
↑CRP vasculitis
Drug screening: neg
A. Atrial myxoma
B. Antiphospholipid syndrome with renal vein thrombosis
C. Fibromuscular dysplasia
D. Polyarteritis nodosa
E. Ergot induced vasospasm
Vasculitis • Renal infarcts small VS medium vessel
• Urine: no sediments, HTN renal artery medium vessel
• ANCA, C3, C4 normal
• Angiograms
Left Renal angiogram Superior mesenteric artery angiogram
A 52 years old man is evaluated for fever, malaise, arthralgia, left foot drop,
abdominal pain that is worse after eating, weight loss 2 kgs over 2 mo.
PE: BT 38.4c BP 154/92
Sinus and lung: normal
Abdominal bruit +
Testicles are tender to palpitation.
Joints are tender, but no swelling.
Weakness of left foot dorsiflexion.
Lab: ESR 72 C3, C4-normal Cr 2.2
UA: rbc 3-5, no proteinuria, no red cell cast
ANCA-negative, HBsAg +
3/6/2019
14
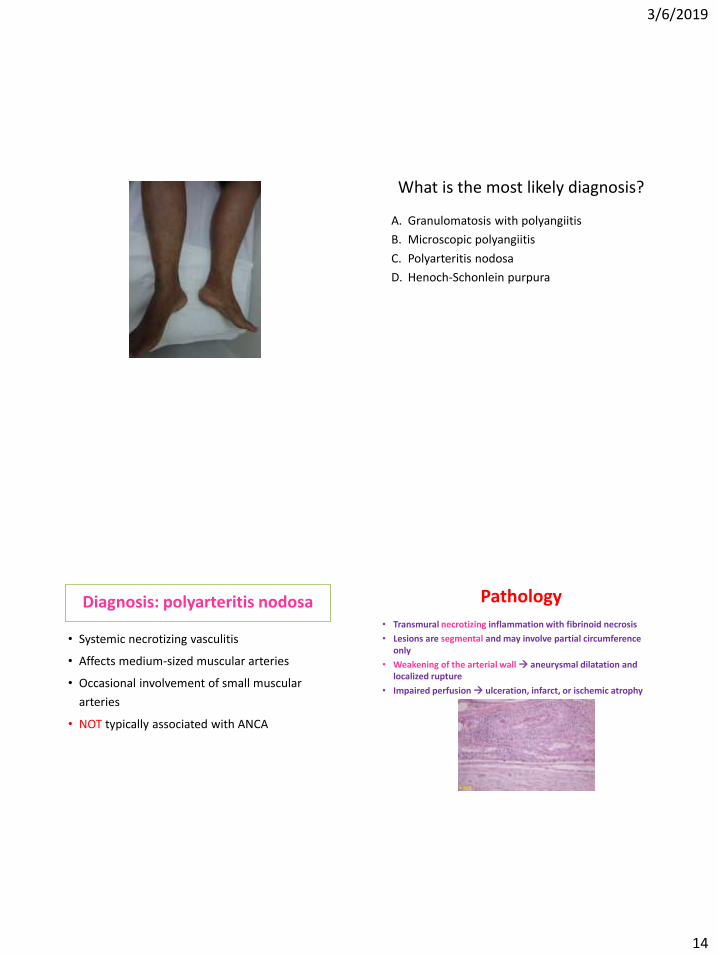
What is the most likely diagnosis?
A. Granulomatosis with polyangiitis
B. Microscopic polyangiitis
C. Polyarteritis nodosa
D. Henoch-Schonlein purpura
Diagnosis: polyarteritis nodosa
• Systemic necrotizing vasculitis
• Affects medium-sized muscular arteries
• Occasional involvement of small muscular
arteries
• NOT typically associated with ANCA
Pathology
• Transmural necrotizing inflammation with fibrinoid necrosis
• Lesions are segmental and may involve partial circumference only
• Weakening of the arterial wall aneurysmal dilatation and localized rupture
• Impaired perfusion ulceration, infarct, or ischemic atrophy

3/6/2019
15
Clinical manifestations: PAN
Constitutional symptoms • Fever
• Malaise
• myalgia
• Weight loss, Anorexia
Musculoskeletal • Arthralgia
• Episodic, nondeforming, asymmetrical polyarthritis
• Predominant: large joints , especially the lower extremities
• Myalgia
Clinical manifestations: PAN
Cutaneous manifestations • Livedo reticularis, skin ulcers, bullous or vesicular
eruption, subcutaneous nodule
• Palpable petechial or purpuric lesions
• Frequent sites : fingers, ankles around the malleoli, and pretibial area, often marked over the lower extremities
• Digital gangrene
• Splinter hemorrhage
Clinical manifestations: PAN Palpable purpura Livedo reticularis

3/6/2019
16
Subcutaneous nodules
Reddish, painful, tender, subcutaneous nodule
Nervous system (Peripheral disease) • Mononeuritis multiplex :frequently affected
peroneal, median, ulnar, sural nerve.
• Distal sensorimotor polyneuropathy
• Cranial nerve palsy less common
• Noted early in 50-70% of patients
• Direct result of occlusion of the vasa vasorum
Clinical manifestations: PAN
Polyarteritis nodosa: wrist drop
This neuropathy is due to ischemia of the vasa nervorum.
Nervous system (Central disease) • Rare
• occur late
• Ischemic stroke, intracerebral hemorrhage small vessel strokes
• Diffuse encephalopathy
• Seizure
Clinical manifestations: PAN

3/6/2019
17
Renal involvement • Vascular nephropathy common manifestation
• HTN renal artery involvement
• Renal failure Multiple infarcts
• Intrarenal, perirenal, or retroperitoneal hemorrhage rupture of microaneurysm
• Urinalysis :normal or near normal
• No glomerulonephritis
Clinical manifestations: PAN Clinical manifestations
Gastrointestinal involvement • Abdominal pain :mesenteric arteritis
– dull and constant, worse by eating, rapid wt loss
• GI bleeding and bowel perforation • Malabsorption , pancreatitis ,or vasculitis of appendix or gall
bladder
• Liver frequently involved at autopsy; but clinical involvement uncommon
: infarct or hematoma
: hepatomegaly with or without jaundice
Clinical manifestations: PAN
Genitourinary involvement
• Testicular pain : Orchitis
• Prostatitis
Cardiac involvement
• Coronary artery involvement myocardial ischemia
• Heart failure
• Pericarditis
Clinical manifestations Clinical manifestations: PAN * PAN key points
• General confinement to medium sized vessels
• Exclusive involvement of arteries, with sparing of veins except by contiguous spread
• Lack of granuloma formation
• Tendency to form microaneurysm
• Absence of lung involvement
• Absence of renal glomerular involvement
• Absence of associated autoantibodies(ANCA, anti GBM)

3/6/2019
18
ACR 1990 criteria of PAN (3/10)
Criteria Remarks
1.Unexplained wt. loss > 4 kg at the onset
2.Livedo reticularis Mottled reticulate pattern
3.Testicular pain Exclude infection and trauma
4.Myalgia, weakness or leg tenderness Exclude shoulder and hip girdle
5.Mono-polyneuropathy
6.DBP > 90 mmHg
7.Elevated BUN or Cr BUN > 40 mg/dl or Cr>1.5 mg/dl (exclude dehydration or postrenal)
8.Hepatitis B virus HBs Ag+ or anti-HBs +
9.Arteriographic abnormality Aneurysms or occlusion at visceral a.
10. Abnormality of small or medium sized a. PMN or Mononuclear cell infiltrate at the vessel wall
Treatment
• Non-hepatitis associated PAN
• PAN with hepatitis B infection
Clin Exp Rheumatol 2011; 29 (Suppl. 64):S110-S116.
FFS ≥ 1
Prognosis Revisited 2009 Five-factor scores
Presence of each = +1 point
1. Age >65 years
2. Cardiac symptoms
3. Gastrointestinal involvement
4. Renal insufficiency (stabilized peak creatinine ≥ 1.7 mg/dL)
Presence of each = -1 point
1. Ear, nose, and throat (ENT) symptoms
• FFS : 0,1,>2
• 5 yr mortality rate: 9, 21, 40%

3/6/2019
19
MKSAP18 Q/2
A 55 years old man previously healthy is hospitalized for acute
respiratory failure. He noted leg swelling and non-healing skin ulcers
and joint pain in wrists, MCPs and PIPs 4 weeks ago.
+ tobacco 20 pack-year
PE: BP 150/95 BT 37.2c on mechanical ventilator
CXR: diffuse bilateral infiltrates
Skin bx: non-granulomatous, small vss vasculitis, no immune cpx
deposits by immune fluorescence.
Which of the following is the most likely diagnosis?
A. Systemic lupus erythematosus
B. Microscopic polyangiitis
C. Granulomatous polyangiitis
D. Polyarteritis nodosa
E. Thromboangiitis obliterans
Which of the following is likely to found in this patient?
A. Anti-myeloperoxidase antibody
B. Anti-PR3 antibody
C. Anti-nuclear antibody
D. Low C3 C4 levels
E. Abnormal angiogram: cockscrew collaterol vss.
MKSAP17 Q27
A 32 years old woman admitted for 2 weeks of progressive SOB and 48 hours of hemoptysis.
She also noted rash and weakness of left foot.
Previously healthy except for mild asthma (as needed albuterol MDI)
PE: BT 37.5c RR 26/min BP 146/87
Lab:
ESR 98 Hct 26% WBC 16,000 eo 42% Plt 450k Cr 0.8
ANCA and ANA: neg
UA: negative
What is the most likely diagnosis?
A. Microscopic polyangiitis
B. Eosinophilic granulomatosis with polyangiitis
C. Granulomatosis with polyangiitis
D. Goodpasture's syndrome
E. Systemic lupus erythematosus
3/6/2019
20
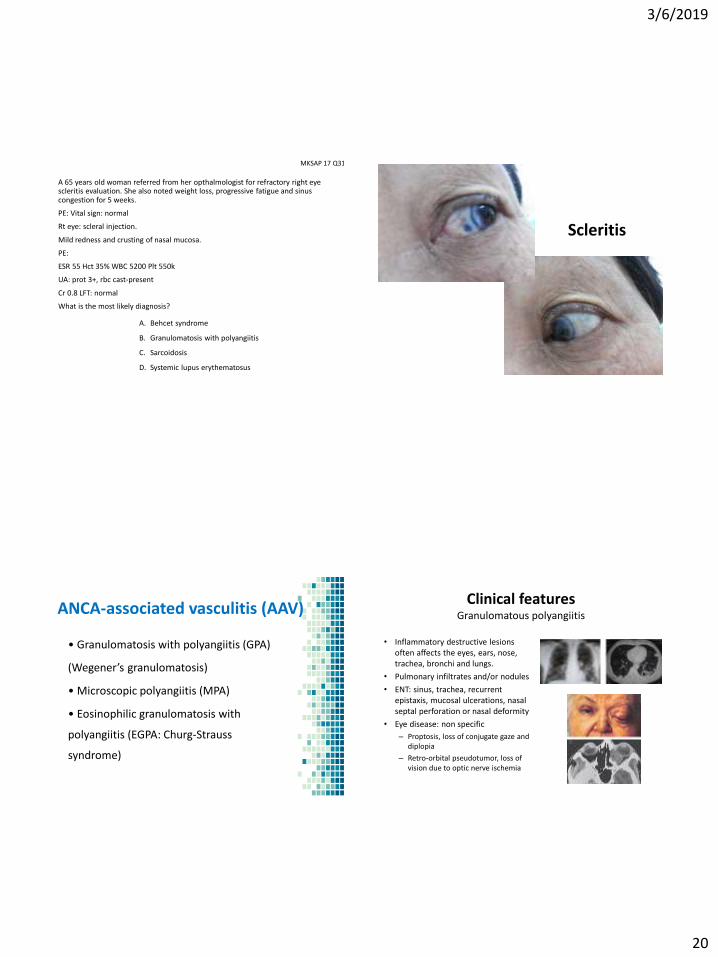
MKSAP 17 Q31
A 65 years old woman referred from her opthalmologist for refractory right eye scleritis evaluation. She also noted weight loss, progressive fatigue and sinus congestion for 5 weeks.
PE: Vital sign: normal
Rt eye: scleral injection.
Mild redness and crusting of nasal mucosa.
PE:
ESR 55 Hct 35% WBC 5200 Plt 550k
UA: prot 3+, rbc cast-present
Cr 0.8 LFT: normal
What is the most likely diagnosis?
A. Behcet syndrome
B. Granulomatosis with polyangiitis
C. Sarcoidosis
D. Systemic lupus erythematosus
Scleritis
ANCA-associated vasculitis (AAV)
• Granulomatosis with polyangiitis (GPA)
(Wegener’s granulomatosis)
• Microscopic polyangiitis (MPA)
• Eosinophilic granulomatosis with
polyangiitis (EGPA: Churg-Strauss
syndrome)
Clinical features Granulomatous polyangiitis
• Inflammatory destructive lesions often affects the eyes, ears, nose, trachea, bronchi and lungs.
• Pulmonary infiltrates and/or nodules
• ENT: sinus, trachea, recurrent epistaxis, mucosal ulcerations, nasal septal perforation or nasal deformity
• Eye disease: non specific
– Proptosis, loss of conjugate gaze and diplopia
– Retro-orbital pseudotumor, loss of vision due to optic nerve ischemia

3/6/2019
21
Clinical features Granulomatous polyangiitis
• Pauci-immune glomerulonephritis
• Musculoskeletal features are common (arthralgia not frank arthritis)
• 25 % neuro involvement: peripheral or CNS
Biopsy
– Lung : highest diagnostic yield
– Upper airway tissue : may not show vasculitis
– Renal : pauci-immune glomerulonephritis
•Necrotizing
granulomanous vasculitis
•Neutrophilic infiltrates
Kidney
• Glomerulonephritis
• NO GRANULOMA
• PAUCI-IMMUNE = NO IMMUNE COMPLEX DEPOSITION
– Acute renal failure, RPGN
– Active urinary sediment
Definition of disease stages according to EULAR
Rheum Dis Clin N Am 36 (2010) 507–526

3/6/2019
22
MICROSCOPIC POLYANGIITIS
Clinical manifestation : – Common cause of pulmonary-renal
syndrome
– Constitutional symptom
– Pulmonary : Cough , Dyspnea, Pulmonary hemorrhage
– Kidney : Glomerulonephritis
– Joint : Arthalgia , Arthritis
– Skin : rash, palpable purpura, livido reticularis
– Neuro: mononeuritis multiplex
Microscopic Polyangiitis
• Age of onset 40-50 yrs
• Necrotizing vasculitis
• No granuloma !!!!
• Over 80% positive for ANCA, mostly P-ANCA
• Anti-MPO antibodies
• P-ANCA, anti MPO
• Frequent pulmonary and renal inv
• Negative Hep B serology
DDx from WG
DDx from PAN
Eosinophilic granulomatosis with polyangiitis (EGPA)
• M = F , mean age 50 years
• Asthma (esp. late onset, refractory)
• Eosinophilia > 10%
• Mono/polyneuropathy
• Migratory/transient pulmonary opacities on radiography
• Paranasal abnormality: sinusitis, nasal polyp, rhinitis
• Biopsy containing a blood vessel show eosinophils in extravascular area
• Skin : purpura, nodule, urticaria, ulcer
• ANCA : pANCA > cANCA
Clinical features: EGPA
• Prodromal phase – Characterized by atopic disease, allergic rhinitis,
and asthma
• Eosinophilic phase – eosinophilia and eosinophilic infiltration of multiple
organs, esp the lung and gastrointestinal tract
• Vasculitic phase

3/6/2019
23
Churg-Strauss syndrome
• Compared with WG and MPA
– CSS involves much less frequent and less severe renal disease
– more frequent neuropathy and cardiac disease
A 52 years old man is admitted for several episodes of hemoptysis for 2 days.
3 weeks ago: myalgia, arthralgia, low-grade fever, nasal fullness, ↓hearing in left ear, rash both legs and weakness of right hand
PE: 150/90 BT 38c – Tender bilateral maxillary sinus
– Chest: diffuse rhonchi
– Palpable purpura
– Right wrist drop
CBC: Hct 35% WBC 12,300 PMN 70% L23% eo2% Plt 580K
UA: prot 3+, RBC cast +
Which of the following is most likely to establish the diagnosis?
A. Anti-ds-DNA antibody B. Anti-myeloperoxidase antibody
C. Anti-proteinase 3 antibody D. Serum cryoglobuline
Cytoplasmic ANCA
Diffuse granular
cytoplasmic staining
pattern
Anti-preteinase-3
Perinuclear ANCA
Perinuclear or nuclear
staining pattern
Anti-myeloperoxidase
0
20
40
60
80
100
WG MPA idiopathic
RPGN
CSS
p-ANCA
c-ANCA
Frequency of ANCA reactivity

3/6/2019
24
ANCA in other diseases
• Non-specific esp P-ANCA
• Autoimmune disease
• Systemic vasculitis : HSP, Kawasaki’s disease
• Other rheumatic disease: RA, SLE, Sjögren syndrome
• Inflammatory bowel disease
• Infections
• Endocarditis, respiratory tract infection, cystic fibrosis, chromomycosis, HIV, amoebiasis
• Drugs
• Propylthiouracil, hydralazine, minocycline
Sign and symptoms GPA (%) MPA (%) EGPA (%)
Upper airways disease 95 - 50-60
Pulmonary disease
Asthma - - 90-100
Radiographic
nodule/infiltrates
70-85 15-70 40-70
Alveolar hemorrhage 5-15 10-50 < 5
Glomerulonephritis 70-80 75-90 10-40
Gastrointestinal system < 5 30 30-50
Nervous system
Peripheral 40-50 60-70 70-80
Central 5-10 10-15 5-30
Cardiac 10-25 10-15 10-40
Ocular 50-60 < 5 < 5
Arthralgia/arthritis 60-70 40-60 40-50
Genitourinary system < 2 < 5 < 2
Skin 40-50 50-65 50-55
ANCA
PR3-cANCA 75-90 10-50 3-35
MPO-pANCA 5-20 50-80 2-50
Pathology Granulomatous
necrotizing vasculitis
Necrotizing vasculitis
without granuloma
Granulomatous
necrotizing vasculitis
with abundant of
eosinophils J ALLERGY CLIN IMMUNOL Feb 2010
Treatment ANCA-associated vasculitis
Induction
• Limited form: methotrexate + pred 1 mkd
• Generalised form:
– Pulse cyclophosphamide iv monthly
– Oral daily cyclophosphomide
– Rituximab 375 mg/m2 x 4 doses
– Pulse methylpred 500 -1000 mg iv x 3 days
– Prednisolone 1 mkd
• Severe generalised form: add plasmapheresis in
– DAH
– Severe renal disease
– Concurrent anti-GBM disease
• PCP prophylaxis: trimethoprim-sulfamethoxazole
– 1 single strength (80 mg/400 mg) daily
– 1 double strength (160 mg/800 mg) 3 times per week
Oral: more leukopenia, less relapse
RTX=CYC Only more remission in relapse pt
ANCA vasculitis. EULAR 2016 guideline
Maintenance after achieved remission: 24 months
– Glucocorticoid can be discontinued
– Methotrexate = Azathioprine (WEGENT)
– Methotrexate 0.3 mkw 20-25 mkw (NORAM)
– Azathioprine 2 mkd (CYCAZAREM)
– Rituximab* 500 mg D1, 14 at months 6, 12, and 18 (better than aza)
Treatment ANCA-associated vasculitis
ANCA vasculitis. EULAR 2016 guideline

3/6/2019
25
A 39 year old woman is
evaluated for a lower
extremities rash and joint
pain for 8 weeks. She takes
no medication.
PE: BT 37.4c
• Wrist drop on the right
• Joint tenderness with mild
synovitis at MCPs, PIPs,
wrists
• Rash: as shown
Small vascular infarction on the ears Scatter palpable purpuric lesions
Lab: ESR 66 C3: normal, C4:↓, Cr 2.1 RF +, anti-HCV + UA: prot 3+, RBC 5-10, RBC cast +
Which of the following is most likely to establish diagnosis?
A. Anti-CCP antibodies
B. Anti-dsDNA antibody
C. Cryoglobulin
D. Anti-myeloperoxidase antibody
Clinical manifestations of HCV associated mixed cryoglobulinemia

3/6/2019
26
Investigation Cryoglobunemic vasculitis
• Low early complement C1, C2, C4 but normal C3
– Often seen in mixed cryoglobulinemia
– Not correlate with disease activity
• RF is detected in 2/3 of patients (50% having levels of 3-4x UNL)
– Negative anti-CCP antibody
• Other nonspecific features:↑ESR, ↑CRP, and anemia of inflammation
– ↑↑ESR in type I cryoglobulinemia because of the presence of large concentrations of paraproteins
– CBC
• Pseudothrombocytosis
• Formation of erythrocyte rouleaux
How to detect cryoglobulin??
Warm collecting tube at 37c
No anti-coagulant
Draw 10 cc of blood
Blood transport at 37C
Blood clot at 37C > 1 hr
Centrifuge at 2500 RPM for 10 mins
Incubate serum at 4C for 3-7 days
Centrifuged to measure at 4C
Washing
Rewarm at 37C for resolubility
Characterization of immuno-precipitate by immunofixation
Collected, stored, and centrifuged at 37 ⁰C
Lancet 2012
Arthralgia/arthritis Non-inflammatory musculoskeletal pain General features (malaise, fever)
MKSAP17 Q40
A 32 years old woman presented with new rash on both legs for 4 days. She has had cystitis and was given a 7 day-plan of trimethoprim-sulfamethoxazole.
PMH: Hashimoto thyroiditis
Med: levothyroxine
Which of the following is the most appropriate next step in management?
A. Discontinue trimethoprim-sulfamethoxazole
B. Discontinue levothyroxine
C. Initiate prednisolone
D. Measure anti-histone antibody
E. Obtain skin biopsy
3/6/2019
27
Hypersensitivity vasculitis
• Hypersensitivity reaction to antigens ex medication or infection
• Resolve after removing offending agents
• Immune complex deposition
• Small vss: capillaries, venules, arterioles
E18 Q65
A 35 years old woman presented with severe abdominal pain, palpable purpura rash both legs, arthralgia and myalgia for 2 days.
Lab: CBC, UA, Cr, LFT: normal
ANA, ANCA: neg
Stool exam: occult blood +
CT abdomen: short segment of small bowel thickening and edema.
Which of the following is the most appropriate test to establish the diagnosis?
A. Kidney biopsy
B. Mesenteric angiography
C. Skin biopsy with immunogfluoresence
D. Complement level
IgA vasculitis (IgAV) Henoch-Scholein Purpura
• Common in children
• Occur after URI 10-14 days
– 90 % purpura
– 75 % arthralgias
– 60 % colicky abdominal pain
– 50 % renal, < ESRD 5%
• Patho: vascular IgA-dominant immune complexes
• Rx: supportive, unless nephritis is present
1. Allergic rhinitis, asthma, eosinophilia, pulmonary infiltrates, coronary arteritis, intestinal ischemia, mononeuritis multiplex
2. Arthritis, Raynaud's phenomenon, glomerulonephritis, palpable purpura, mononeuritis multiplex ,↓C3, C4
3. Recurrent epistaxis or sinusitis, pulmonary infiltrates and/or nodules, glomerulonephritis, ocular involvement, granulomatous necrotizing vasculitis
QUIZ

3/6/2019
28
4. Fever, weight loss, hypertension, mononeuritis multiplex, intestinal ischemia, renal ischemia, testicular pain, ANCA-negative
5. Headache, polymyalgia rheumatica, jaw or tongue claudication, scalp tenderness, fever, vision disturbances
6. Extremity claudication, hypertension in the young, constitutional symptoms, renal ischemia
QUIZ
117