protocollo diagnostico: gestione della steatosi epatica ... ranucci... · minute gocce di grasso...
TRANSCRIPT

Università degli Studi di Napoli “Federico II”
Scuola di Specializzazione in Pediatria
Dire:ore: Prof. Riccardo Troncone
GLI INCONTRI DEL MERCOLEDI’ 16 Gennaio 2013
Pablo Picasso, “Pesca di notte a Antibes” (1939)
Protocollo diagnostico: GESTIONE DELLA STEATOSI EPATICA PEDIATRICA
A cura di G. Ranucci- I. Bracale Tutor: R.Iorio

DEFINIZIONE STEATOSI EPATICA Accumulo di lipidi all’interno dell’epatocita (>5%).
Più comunemente di si tratta di accumulo di trigliceridi
DIAGNOSI ISTOLOGICA
MICROVESCICOLARE MACROVESCICOLARE
Un singolo e voluminoso vacuolo di grasso disloca lateralmente il nucleo centrale.
Minute gocce di grasso circondano il nucleo centrale dell’epatocita.
Schwimmer JB, in “Liver disease in children” 2007 by Suchy et al

DEFINIZIONE DI STEATOSI Ev idenza i s to log ica d i s t e a t o s i c o n o s e n z a infiammazione e fibrosi
Kleiner DE et al, Hepatology 2005; 41:1313-21
• Fegato brillante all’ecografia con o senza ipertransaminasemia
STEATOSI EPATICA PROBABILE
ECOGRAFIA:
BRIGHT LIVER PATTERN
La steatosi epaEca è obesità-‐ correlata (cosidde:a NAFLD primaria) se associata ad almeno 1 dei 3 seguenE fa:ori: obesità, diabete mellito, ipertrigliceridemia

STEATOSI NON SOLO OBESITA’…
POSITION PAPER OF ESPGHAN; JPGN 2012; 54
Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Clinical Features
Clinically, most pediatric patients with NAFLD/NASHhave nonspecific symptoms. Some complain of fatigue, malaise,or vague abdominal pain (42%–59% of cases), especially in theright upper quadrant, which has been associated with the moreprogressive form of NASH (2). Acanthosis nigricans is a clinicalmarker of hyperinsulinemia and has been observed in one-third tohalf of the children with biopsy-proven NAFLD (23). Hepatome-galy can be frequently detected (up to 50% of cases) (21,22).
Anthropometric Features
Visceral adiposity, which may be related to a state of insulinresistance, is a major contributor to fatty liver, representing a moreinfluential component than BMI in predicting liver steatosis.Unfortunately, indirect measurements of visceral adiposity usedin adult studies such as waist-to-hip ratio are not appropriate forchildhood because they change with age and have poor correlationwith measures of adiposity measured by DEXA (32,33). In children,waist circumference alone represents a practical anthropometricparameter to identify central adiposity and it may predict increased
risk for insulin resistance and the metabolic syndrome (34). Specificpercentiles have been developed for children ages 5 to 16 years (35)and 11 to 18 years (36). The importance of waist circumferencemeasurement in childhood NAFLD is well established (37).Lin et al (37) showed that in obese children and adolescents, forevery 5-cm increase in waist circumference, there was an odds ratioof 1.4 for predicting ultrasonographic liver steatosis, but no detailson percentiles were given. Increased waist circumference is alsoassociated with increased hepatic fibrosis (38). There is a need forstandard international waist circumference charts.
Laboratory Tests
In clinical practice the diagnosis of NAFLD is usuallysuggested by finding elevated serum hepatobiliary enzymes(mostly ALT and g-glutamyl transpeptidase [GGT]), and/or evi-dence of a bright liver on ultrasound (US), most frequently amongoverweight/obese children (27,39,40).
SerumALT activity is a widely available and inexpensive testfor the screening and initial evaluation of NAFLD. The sensitivity ofthis biochemical marker, however, remains low because a number ofadult and pediatric patients may present ALT values in the normal
TABLE 2. Causes of fatty liver disease in children
General or systemic Genetic-metabolic causesOther rare hereditarygenetic disorders Drugs’ hepatotoxicity
Acute systemic disease Cystic fibrosis and Shwachmansyndrome
Alstrom syndrome Ethanol
Acute starvation Wilson disease Bardet-Biedl syndrome Ecstasy, cocaineProtein energy malnutrition a1-Antitrypsin deficiency Prader-Willi syndrome NifedipineTotal parenteral nutrition Galactosemia Cohen syndrome DiltiazemObesity/metabolic syndrome Fructosemia Cantu syndrome (1p36 deletion) EstrogensPolycystic ovary syndrome Cholesteryl ester storage disease Weber-Christian disease CorticosteroidsObstructive sleep apnea Glycogen storage disease
(types I and VI)Amiodarone
Rapid weight loss Mitochondrial and peroxisomaldefects of fatty acid oxidation
Perhexiline
Anorexia nervosa Madelung lipomatosis CoralgilCachexia Lipodystrophies TamoxifenInflammatory bowel disease Dorfman-Chanarin syndrome MethotrexateCeliac disease Abeta or hypobetalipoproteinemia PrednisoloneHepatitis C a- and b-oxidation defects ValproateNephrotic syndrome Porphyria cutanea tarda VitaminType 1 diabetes mellitusand Mauriac syndrome
Homocystinuria L-asparaginase
Thyroid disorders Familial hyperlipoproteinemias Zidovudine andHIV treatments
Hypothalamo-pituitary disorders Tyrosinemia type 1 SolventsBlind loop (bacterial overgrowth) Bile acids synthesis defects Pesticides
Congenital disorders of glycosylationTurner syndromeOrganic acidosisCitrin deficiencyHFE (hemochromatosis)
Modified from (7,19,20). Exclusions should be adjusted to age and clinical presentation. In infants and young children, NAFLD is hardly to be expected,whereas genetic, metabolic, syndromic, and systemic causes should be primarily considered guided by clinical signs and symptoms. In children older than10 years, NAFLD is expected when!1 features of the metabolic syndrome are present; still, Wilson disease and a1-antitrypsin deficiency should be excludedand autoimmune hepatitis should be considered.
Vajro et al JPGN " Volume 54, Number 5, May 2012
702 www.jpgn.org

Come viene reclutato il bambino con steatosi epatica?
ü Pazienti obesi
ü Pazienti asintomatici con ipertransaminasemia e/o epatomegalia
ü Pazienti con quadro clinico di epatopatia conclamata
ü Riscontro occasionale in pazienti che praticano l’ecografia dell’addome per altri motivi
E’ opportuno ricercarla sistema0camente in tu1 gli obesi? … sopra6u6o dal punto di vista dei cos0 e dell’impa6o sulla ges0one?
In questo contesto è alto il rischio di una malaPa geneEco-‐metabolica so:ostante!!!

APPROCCIO AL BAMBINO CON STEATOSI
BAMBINO SOVRAPPESO/ OBESO
BAMBINO NORMOPESO
LATTANTE
BAMBINO/ADOLESCENTE

COSA RICERCARE ALL’ANAMNESI? Familiare -‐ Obesità, sindr. metabolica (diabete 7po 2, iperlipidemia,
ipertensione arteriosa, etc) -‐ Consanguineità, provenienza di entrambi i genitori da un piccolo centro. Presenza di epatopa7e gene7co-‐metaboliche nel gen7lizio.
Personale -‐ Storia gravidica (IUGR, -‐ Recente e rapido incremento ponderale -‐ Dimagrimento -‐ Sviluppo psicomotorio -‐ MalaIe sistemiche -‐ Ospedalizzazioni (NPT) -‐ Apnee ostruIve noMurne
Alimentare -‐ Comportamento bulimico o anoressico -‐ Intolleranza al digiuno prolungato nei primi mesi (glicogenosi) -‐ Avversione a fruMosio e saccarosio
Farmacologica -‐ Farmaci steatogeni
Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Clinical Features
Clinically, most pediatric patients with NAFLD/NASHhave nonspecific symptoms. Some complain of fatigue, malaise,or vague abdominal pain (42%–59% of cases), especially in theright upper quadrant, which has been associated with the moreprogressive form of NASH (2). Acanthosis nigricans is a clinicalmarker of hyperinsulinemia and has been observed in one-third tohalf of the children with biopsy-proven NAFLD (23). Hepatome-galy can be frequently detected (up to 50% of cases) (21,22).
Anthropometric Features
Visceral adiposity, which may be related to a state of insulinresistance, is a major contributor to fatty liver, representing a moreinfluential component than BMI in predicting liver steatosis.Unfortunately, indirect measurements of visceral adiposity usedin adult studies such as waist-to-hip ratio are not appropriate forchildhood because they change with age and have poor correlationwith measures of adiposity measured by DEXA (32,33). In children,waist circumference alone represents a practical anthropometricparameter to identify central adiposity and it may predict increased
risk for insulin resistance and the metabolic syndrome (34). Specificpercentiles have been developed for children ages 5 to 16 years (35)and 11 to 18 years (36). The importance of waist circumferencemeasurement in childhood NAFLD is well established (37).Lin et al (37) showed that in obese children and adolescents, forevery 5-cm increase in waist circumference, there was an odds ratioof 1.4 for predicting ultrasonographic liver steatosis, but no detailson percentiles were given. Increased waist circumference is alsoassociated with increased hepatic fibrosis (38). There is a need forstandard international waist circumference charts.
Laboratory Tests
In clinical practice the diagnosis of NAFLD is usuallysuggested by finding elevated serum hepatobiliary enzymes(mostly ALT and g-glutamyl transpeptidase [GGT]), and/or evi-dence of a bright liver on ultrasound (US), most frequently amongoverweight/obese children (27,39,40).
SerumALT activity is a widely available and inexpensive testfor the screening and initial evaluation of NAFLD. The sensitivity ofthis biochemical marker, however, remains low because a number ofadult and pediatric patients may present ALT values in the normal
TABLE 2. Causes of fatty liver disease in children
General or systemic Genetic-metabolic causesOther rare hereditarygenetic disorders Drugs’ hepatotoxicity
Acute systemic disease Cystic fibrosis and Shwachmansyndrome
Alstrom syndrome Ethanol
Acute starvation Wilson disease Bardet-Biedl syndrome Ecstasy, cocaineProtein energy malnutrition a1-Antitrypsin deficiency Prader-Willi syndrome NifedipineTotal parenteral nutrition Galactosemia Cohen syndrome DiltiazemObesity/metabolic syndrome Fructosemia Cantu syndrome (1p36 deletion) EstrogensPolycystic ovary syndrome Cholesteryl ester storage disease Weber-Christian disease CorticosteroidsObstructive sleep apnea Glycogen storage disease
(types I and VI)Amiodarone
Rapid weight loss Mitochondrial and peroxisomaldefects of fatty acid oxidation
Perhexiline
Anorexia nervosa Madelung lipomatosis CoralgilCachexia Lipodystrophies TamoxifenInflammatory bowel disease Dorfman-Chanarin syndrome MethotrexateCeliac disease Abeta or hypobetalipoproteinemia PrednisoloneHepatitis C a- and b-oxidation defects ValproateNephrotic syndrome Porphyria cutanea tarda VitaminType 1 diabetes mellitusand Mauriac syndrome
Homocystinuria L-asparaginase
Thyroid disorders Familial hyperlipoproteinemias Zidovudine andHIV treatments
Hypothalamo-pituitary disorders Tyrosinemia type 1 SolventsBlind loop (bacterial overgrowth) Bile acids synthesis defects Pesticides
Congenital disorders of glycosylationTurner syndromeOrganic acidosisCitrin deficiencyHFE (hemochromatosis)
Modified from (7,19,20). Exclusions should be adjusted to age and clinical presentation. In infants and young children, NAFLD is hardly to be expected,whereas genetic, metabolic, syndromic, and systemic causes should be primarily considered guided by clinical signs and symptoms. In children older than10 years, NAFLD is expected when!1 features of the metabolic syndrome are present; still, Wilson disease and a1-antitrypsin deficiency should be excludedand autoimmune hepatitis should be considered.
Vajro et al JPGN " Volume 54, Number 5, May 2012
702 www.jpgn.org

IUGR e SGA: *malattie genetico-metaboliche
* maggiore incidenza di steatosi e di malattie cardiovascolari Hindawi Publishing CorporationInternational Journal of EndocrinologyVolume 2011, Article ID 269853, 8 pagesdoi:10.1155/2011/269853
Review ArticleIntrauterine Growth Retardation and Nonalcoholic Fatty LiverDisease in Children
Anna Alisi,1 Nadia Panera,1 Carlo Agostoni,2 and Valerio Nobili1
1 Liver Research Unit, Bambino Gesu Children’s Hospital and Research Institute, 00165 Rome, Italy2 Department of Maternal and Pediatric Sciences, Fondazione IRCCS Ca’ Granda—Ospedale Maggiore Policlinico, University of Milan,20122 Milan, Italy
Correspondence should be addressed to Anna Alisi, [email protected]
Received 27 July 2011; Accepted 11 October 2011
Academic Editor: Daniela Jezova
Copyright © 2011 Anna Alisi et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Intrauterine growth retardation (IUGR), the most important cause of perinatal mortality and morbidity, is defined as a foetalgrowth less than normal for the population, often used as synonym of small for gestational age (SGA). Studies demonstrated therelationships between metabolic syndrome (MS) and birthweight. This study suggested that, in children, adolescents, and adultsborn SGA, insulin resistance could lead to other metabolic disorders: type 2 diabetes (DM2), dyslipidemia, and nonalcoholic fattyliver disease (NAFLD). NAFLD may evolve to nonalcoholic steatohepatitis (NASH), and it is related to the development of MS.Lifestyle intervention, physical activity, and weight reduction represent the mainstay of NAFLD therapy. In particular, a catch-upgrowth reduction could decrease the risk to develop MS and NAFLD. In this paper, we outline clinical and experimental evidencesof the association between IUGR, metabolic syndrome, insulin resistance, and NAFLD and discuss on a possible management toavoid the risk of MS in adulthood.
1. Introduction
Intrauterine growth retardation (IUGR) is one of the mostimportant causes of perinatal mortality and morbidity anda!ects approximately 7–15% of worldwide pregnancies [1].IUGR is commonly defined as foetal growth less than thatcharacterizing commonly healthy population. However, todate, there is no a clear internationally conventional clinicaldefinition for this term. In fact, although some studies useIUGR as synonym of small for gestational age (SGA), it is im-portant to remember that infants born with IUGR may ormay not be necessarily SGA and, similarly, infants who areSGA may be born without growth-restricting processes char-acterizing IUGR [2, 3].
Although several causes or risk factors have been sug-gested for development of IUGR, including those of mater-nal, placental, and foetus origin [4], it is very di"cult to esta-blish, in most situations, the real cause of this condition.
In addition to the high rates of perinatal mortality, IUGR,recently, has been often associated with the development ofseveral features of metabolic syndrome (MS) in adulthood,
increasing seriously the risk of mortality associated to cardio-vascular disease [5]. Features of MS classically associatedwith IUGR are insulin resistance, hypertension, dyslipide-mia, impaired glucose tolerance, and type 2 diabetes (DM2);but, very recently, also nonalcoholic fatty liver disease(NAFLD) has been included among the persistent IUGR-de-pendent metabolic dysfunctions [6, 7].
Furthermore, on the basis of numerous pieces of eviden-ces demonstrating that early improvement in growth appearsbeneficial for a number of important outcomes, the person-nel of neonatal follow-up clinics are encouraged to promoteearly catch-up growth for SGA subjects [8]. However, from2003, several controversial studies have forwarded the hypo-thesis that restricting postnatal catchup after prematuritycould prevent later metabolic abnormalities [9].
In this paper, we overview on several aspects associated toIUGR, discussing with a particular attention all correlationwith MS and NAFLD. In addition, here, we emphasize on thefact that an optimal nutritional management needs to achi-eve normal growth variables and a normal body compositionwithout increasing the risk of MS in adulthood.
4 International Journal of Endocrinology
Foetalgenetics
Intrauterineenvironment
IUGR
Insulin-resistant genotype Insulin-resistant phenotype
Insulin resistance
Dyslipidemia DM2 NAFLD Hypertension
MS
Figure 1: Possible hypotheses to explain the association between IUGR and MS. IUGR: intrauterine growth retardation; DM2: type 2 dia-betes; NAFLD: nonalcoholic fatty liver disease; MS: metabolic syndrome.
the MS later in life, comprising arterial hypertension, hyperc-holesterolemia, cardiovascular disease, impaired glucose tol-erance, and/or DM2, and many other diseases, includingosteoporosis. This association, described in various popula-tions, is unrelated to age, sex, and ethnicity and occurs indep-endently of weight and physical activity [5, 23].
From Barker et al. [2], who was the first to introduce theexisting correlation between birth size and later developmentof MS in adult life, several authors [24] showed a wide collec-tion of data highlighting that subjects born SGA are prone tocentral redistribution of adipose tissue and are at high risk fordeveloping insulin resistance, DM2, MS, and cardiovasculardisease. Although the mechanism able to induce MS in IUGRis still unclear in all observed cases, increased insulin resis-tance appeared to play a key role. Two theories have been pro-posed to explain the development of insulin resistance inIUGR: the first is the foetal reprogramming due to thriftyphenotype hypothesis; the second is the establishment of aninsulin-resistant genotype independently of intrauterine en-vironment (Figure 1).
According to “thrifty phenotype hypothesis,” maternalundernutrition during pregnancy modifies the programm-ing of biochemical mechanisms related to endocrine-meta-bolic control inducing permanent changes in glucose-insulinmetabolism. These changes include reduced capacity for in-sulin secretion and insulin resistance which, combined withthe e!ects of obesity, aging, and physical inactivity, may re-sult in cardiovascular and metabolic complications [25]. Fur-thermore, it has been suggested that, in condition of under-nutrition, a genotype conferring insulin resistance would bepreferentially selected during evolution because this geno-type would increase survival among small babies. This phen-omenon is called the “surviving small baby hypothesis” [26].This foetal programming of adaptation to an adverse intrau-terine environment results in increased sensitivity of the peri-pheral tissues to metabolic hormones, such as glucocorti-coids and insulin, this latter condition enhances survival andmaximizes growth and fuel deposition, as the nutritional pat-tern improves after birth. So a “thrifty phenotype” postulatesthat the intrauterine deprivation programs the fetus to in-crease appetite and obesity, hypertension, and diabetes [19].If postnatal nutrient availability is greater than prenatallypredicted, enhanced postnatal growth and fat deposition will
occur. In turn, this increased adiposity will lead to adultinsulin resistance. Certainly, the risk of developing adult MSis the greatest when poor prenatal growth is coupled withrapid catch-up growth during childhood [27].
The alternative hypothesis to development of insulin-re-sistant phenotype in IUGR individuals has suggested thatinsulin resistance might be genetically determined indepen-dently of unfavourable intrauterine environment; as conseq-uences, thus, also a genetic predisposition to metabolic con-sequences of IUGR. In particular, Hattersley and Tooke [3]proposed a “foetal insulin hypothesis,” suggesting the strongcontribution of genetic factors to alter either foetal insulinsecretion or sensitivity of foetal tissues. Polymorphisms ormutations in genes associated to insulin resistance couldresult in impaired foetal growth, low birthweight, and sub-sequent susceptibility to DM2 and cardiovascular disease inadult life. In fact, monogenic disorders a!ect foetal insulinsecretion and resistance causing retarded foetal growth inutero during the third trimester, just when the insulin in-crease should act as one of the major growth factors in foe-tal life. Some monogenic disorders and their e!ects on insu-lin and birth weight are reported in Table 2. For example,mutations in the gene encoding glycolytic enzyme glucoki-nase have been observed, this mutation results in beta-celldysfunction, low-birth-weight and DM2 susceptibility inchildhood and adulthood [28]. However, the monogenic dis-eases are rare and thus they cannot explain the low birthweight case normally seen. So it should be clear that bothgenetic and environmental factors and their possible interac-tions may contribute to the development of the MS in laterlife [29].
6. Evidence of Association between SGA and MS
There are several articles that demonstrated the associationbetween SGA and features of MS.
Interestingly, there are three relevant clinical trials de-monstrating a strong association between low birth weightand insulin resistance. In the first study, including 85 SGAsubjects and 23 AGA subjects, the authors found a close linkbetween insulin secretion/sensitivity, patterns of rapidity,and length of catch-up-growth process during early postnatallife [30]. In the second study, the authors found that mildly
Int J Endocrinol. 2011.
COSA RICERCARE ALL’ANAMNESI?

Svezzamento e vomito (ha assunto miele, zuccheri, tisane, ecc…):
presenza di vomito ricorrente: malattie metaboliche; soprattutto dopo ingestione di
zuccheri: IEF, galattosemia
PASTI FREQUENTI-PIANTO INCONSOLABILE-INTOLLERANZA AL DIGIUNO-EPISODI DI
IPOGLICEMIA: glicogenosi
ASSUME FRUTTA O DOLCI O BEVANDE
ZUCCHERATE
Rifiuto totale di sostanze contenenti zucchero:
IEF DIAGNOSI DI CELIACHIA A DIETA SENZA GLUTINE
Rifiuto totale di sostanze contenenti zucchero: IEF
Hereditary fructose Intolerance and Celiac Disease: a Novel Genetic Association
Clinical Gastroenterology and Hepatology 2006; 4:635-638
COSA RICERCARE ALL’ANAMNESI?

COSA RICERCARE ALL’ESAME OBIETTIVO?
VALUTAZIONE ANTROPOMETRICA Peso, Altezza, P/A, BMI Peso ideale Circonferenza addominale
2 to 20 years: GirlsBody mass index-for-age percentiles
NAME
RECORD #
SOURCE: Developed b(2000).
y the National Center for Health Statistics in collaboration withthe National Center for Chronic Disease Prevention and Health Promotionhttp://www.cdc.gov/growthcharts
2 543 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
26
24
22
20
18
16
14
12
kg/m2
28
26
24
22
20
18
16
14
12
kg/m2
30
32
34
BMI
BMI
AGE (YEARS)
13
15
17
19
21
23
25
27
13
15
17
19
21
23
25
27
29
31
33
35
Date Age Weight Stature BMI* Comments
95
90
85
75
50
10
25
5
Published May 30, 2000 (modified 10/16/00).
OBESITA’ CENTRALE
INSULINO RESISTENZA
Sovrappeso: BMI > 85° Obesità: BMI > 95° Magrezza: BMI < 5°
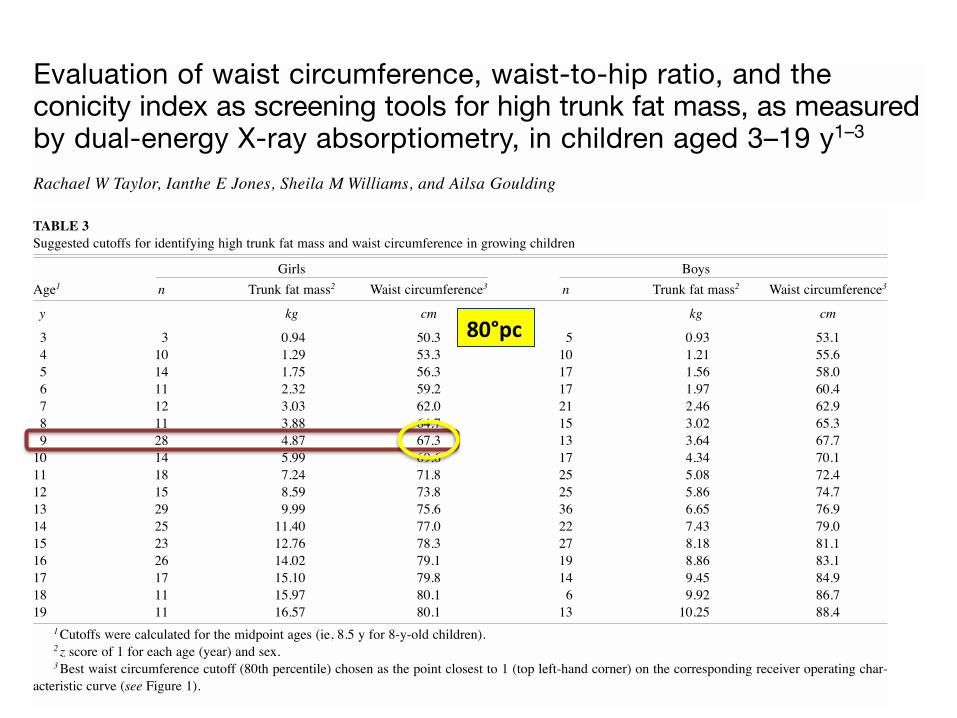
ABSTRACTBackground: A central fat pattern has adverse health implica-tions in both children and adults. Because adiposity tracks fromchildhood into adulthood, the ability of simple anthropometrictechniques to correctly measure truncal adiposity in childhoodneeds to be assessed.Objectives: We sought to assess the validity of waist circumfer-ence, waist-to-hip ratio (WHR), and the conicity index as indi-cators of trunk fat mass in children and adolescents.Design: Trunk fat mass (kg) was measured with dual-energy X-ray absorptiometry in 278 girls and 302 boys aged 3–19 y.Receiver operating characteristic (ROC) curves and areas underthe curves (AUCs) for the ROCs were calculated to compare therelative abilities of the anthropometric measures to correctlyidentify children with high trunk fat mass (z score for our studypopulation of !1).Results: The 80th percentile for waist circumference correctlyidentified 89% of girls and 87% of boys with high trunk fatmass (sensitivity) and 94% of girls and 92% of boys with lowtrunk fat mass (specificity). Waist circumference performedsignificantly better as an index of trunk fat mass than didWHR or the conicity index, as shown by the AUCs in girls andboys, respectively: waist circumference AUCs = 0.97 and 0.97,conicity index AUCs = 0.80 and 0.81, and WHR AUCs = 0.73and 0.71. Our cutoffs for high trunk fat mass and high waistcircumference are provided for both sexes for each year ofage.Conclusion: Waist circumference provides a simple yet effectivemeasure of truncal adiposity in children and adolescents. AmJ Clin Nutr 2000;72:490–5.
KEY WORDS Waist-to-hip ratio, conicity index, trunk fat,dual-energy X-ray absorptiometry, receiver operating characteristiccurve, children, adolescents, body fat, anthropometry
INTRODUCTIONIn adults, it is well established that a more central fat distri-
bution is associated with an increased risk of ill health (1).Recent studies in children also showed that a greater depositionof central fat is correlated with less favorable patterns of serumlipoprotein concentrations (2–5) and blood pressure (2). Because
adiposity (6, 7) and cardiovascular risk factors (7) track fromchildhood into adulthood, early identification of children withhigh central adiposity is important.
Although computed tomography (CT) and magnetic reso-nance imaging (MRI) are considered the gold standards forassessing central fat distribution, their high cost, radiation dose(with CT), and unsuitability for use in young children have oftenprecluded their use on a broad scale. In contrast, dual-energy X-ray absorptiometry (DXA) is a relatively simple technique forevaluating total and regional adiposity in children of all ages (8,9). Although DXA cannot distinguish between intraabdominaland subcutaneous fat, research in adults (10) and children (11)showed strong correlations between trunk fat mass measuredwith DXA and intraabdominal fat measured with CT or MRI.
Routine evaluation of regional fat distribution on a widescale requires methods that are simpler than DXA, CT, or MRI.However, studies on the efficacy of anthropometric techniquesfor identifying children with high central adiposity are scarce(11–13). The waist-to-hip ratio (WHR) has been used exten-sively in adults; however, studies published in the 1990s sug-gest that waist circumference alone may be a more useful andaccurate tool in adults (14–17) and children (11–13). The conic-ity index, which evaluates waist circumference in relation toheight and weight, appears to have a prognostic value similar tothat of WHR in adults (18), but its ability to assess truncal adi-posity has not been evaluated in children as far as we know.Therefore, the aim of our study was to assess the relative abil-ities of waist circumference, the WHR, and the conicity indexto correctly identify children with high trunk fat mass as meas-ured by DXA.
Am J Clin Nutr 2000;72:490–5. Printed in USA. © 2000 American Society for Clinical Nutrition
Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measuredby dual-energy X-ray absorptiometry, in children aged 3–19 y1–3
Rachael W Taylor, Ianthe E Jones, Sheila M Williams, and Ailsa Goulding
490
1 From the Departments of Human Nutrition, Medicine, and Preventiveand Social Medicine, University of Otago, Dunedin, New Zealand.
2 Supported by The Health Research Council of New Zealand and theOtago Medical Research Foundation.
3 Address reprint requests to RW Taylor, Department of Human Nutrition,University of Otago, PO Box 56, Dunedin, New Zealand. E-mail: [email protected].
Received November 16, 1999.Accepted for publication January 31, 2000.
by guest on January 13, 2013ajcn.nutrition.org
Dow
nloaded from
girls and boys, respectively). Negative likelihood ratios showedthat children with waist circumferences above the 80th per-centile for age were only approximately one-tenth (0.11 in girlsand 0.14 in boys) as likely to have low trunk fat mass as werechildren with low waist circumferences (below the 80th per-centile). Higher negative likelihood ratios were calculated forthe conicity index (0.48 and 0.45 in girls and boys, respectively)and WHR (0.62 and 0.64, respectively).
In Table 3 we show the 80th-percentile waist-circumferencecutoffs calculated for each 1-y age group in boys and girls.These were somewhat higher in boys, particularly in late ado-lescence. In Table 3 we also show the estimated cutoffs fortrunk fat mass (z score of 1) for each 1-y interval. In contrastwith waist circumference, these were higher in girls at allages, reflecting their higher total fat mass compared with boys(data not shown). This sex difference is further illustrated inFigure 2, which highlights the large variability in trunk fatmass observed in both sexes.
DISCUSSIONOur study showed that waist circumference performs well as an
index of central adiposity in children and adolescents of bothsexes over a wide age range. In contrast, we showed for the firsttime that the conicity index is not an accurate indicator of centralfat distribution in youths. Other researchers (11–13) suggestedpreviously that WHR correlates poorly with central adiposity.However, their studies were conducted in small samples of chil-dren with a limited age range. In contrast, we used more rigorousstatistical analyses in a large sample of both boys and girls rang-ing in age from 3 to 19 y. Our results showed clearly the superior-ity of waist circumference as an anthropometric indicator ofregional fat distribution. The use of ratios such as WHR to assessobesity may not be appropriate because they are highly age depen-dent (25) and may obscure stronger relations that may be presentwith separate circumference measurements (26). Furthermore, dif-ferences in skeletal structure may confound the results (27).
The conicity index was found to relate to atherogenic risk fac-tors to an extent similar to that of WHR in adults, but it has theadvantage of accounting for total adiposity without requiringmeasurement of hip circumference (18). This may contribute tothe superior performance of the conicity index compared withWHR for identifying children with high trunk fat in our study.However, our results show that the conicity index is not as accu-rate a measure of central adiposity as is waist circumference inchildren, in that it correctly identified fewer than two-thirds ofchildren with high trunk fat mass. This may be due in part to thereasons, discussed above, that ratios may not be appropriate forassessing obesity. It is also not known whether the relationsbetween cardiovascular risk factors and conicity that areobserved in adults also are present in children.
In contrast, waist circumference performed well in identifyingchildren with high trunk fat as measured with DXA. Waist cir-cumference correctly identified >90% of children as being truly
ANTHROPOMETRIC ESTIMATES OF TRUNK FAT IN CHILDREN 493
TABLE 2Areas under the receiver operating characteristic (ROC) curves1
ROC curve Area 95% CI
1: Waist girth and trunk fat mass in girls 0.97 0.95, 0.992: Conicity index and trunk fat mass in girls 0.80 0.72, 0.863: WHR and trunk fat mass in girls 0.73 0.64, 0.814: Waist girth and trunk fat mass in boys 0.97 0.95, 0.995: Conicity index and trunk fat mass in boys 0.81 0.74, 0.886: WHR and trunk fat mass in boys 0.71 0.62, 0.80
1WHR, waist-to-hip ratio. Differences between pairs of curves (95%CIs for the difference) were as follows: curves 1 and 2 = 0.18 (0.12, 0.25),curves 2 and 3 = 0.06 (0.01, 0.12), curves 1 and 3 = 0.24 (0.17, 0.32),curves 4 and 5 = 0.16 (0.10, 0.23), curves 5 and 6 = 0.10 (0.06, 0.14),curves 4 and 6 = 0.26 (0.18, 0.35).
TABLE 3Suggested cutoffs for identifying high trunk fat mass and waist circumference in growing children
Girls BoysAge1 n Trunk fat mass2 Waist circumference3 n Trunk fat mass2 Waist circumference3
y kg cm kg cm
03 3 0.94 50.3 5 0.93 53.104 10 1.29 53.3 10 1.21 55.605 14 1.75 56.3 17 1.56 58.006 11 2.32 59.2 17 1.97 60.407 12 3.03 62.0 21 2.46 62.908 11 3.88 64.7 15 3.02 65.309 28 4.87 67.3 13 3.64 67.710 14 5.99 69.6 17 4.34 70.111 18 7.24 71.8 25 5.08 72.412 15 8.59 73.8 25 5.86 74.713 29 9.99 75.6 36 6.65 76.914 25 11.40 77.0 22 7.43 79.015 23 12.76 78.3 27 8.18 81.116 26 14.02 79.1 19 8.86 83.117 17 15.10 79.8 14 9.45 84.918 11 15.97 80.1 6 9.92 86.719 11 16.57 80.1 13 10.25 88.4
1Cutoffs were calculated for the midpoint ages (ie, 8.5 y for 8-y-old children).2 z score of 1 for each age (year) and sex.3Best waist circumference cutoff (80th percentile) chosen as the point closest to 1 (top left-hand corner) on the corresponding receiver operating char-
acteristic curve (see Figure 1).
by guest on January 13, 2013ajcn.nutrition.org
Dow
nloaded from
80°pc

COME SI MISURA IL SOVRAPPESO ?
Ø Peso in kg x 100/ peso ideale* *Il peso ideale corrisponde al peso al 50° percentile rispetto alla statura reale
Esempio: Peso reale Kg 28, peso ideale Kg 22, Sovrappeso: 28 x 100/22= 127%

COSA RICERCARE ALL’ESAME OBIETTIVO?
VALUTAZIONE DELL’EPATOPATIA ricerca di epatomegalia
splenomegalia-ipertensione portale
Spider nevi, eritema palmare
Prurito
Ittero RICERCA DI SEGNI ORIENTATIVI DELLE PRINCIPALI CONDIZIONI ASSOCIATE A STEATOSI:
- Celiachia
- Fibrosi cistica
- MICI - Endocrinopatie (Cushing, distiroidismi, deficit di GH,…)


Dimensioni del fegato
Konus et al. AJR Roentgenol 1998;171:1693-8

Dimensioni della milza
Konus et al. AJR Roentgenol 1998;171:1693-8

COSA RICERCARE ALL’ESAME OBIETTIVO?
VALUTAZIONE DELL’INSULINO RESISTENZA Misurare PA (ipertensione arteriosa) Achantosis nigricans Ovaio policistico Acne Striae rubrae Irsutismo Necrosi lipoidea

COSA RICERCARE ALL’ESAME OBIETTIVO?
VALUTAZIONE DEI DISMORFISMI E RICERCA MALATTIA METABOLICA
BARDET-‐BIEDL
PRADER WILLI
SINDROME DI COHEN

COSA RICERCARE ALL’ESAME OBIETTIVO?
VALUTAZIONE DEI DISMORFISMI E RICERCA MALATTIA METABOLICA
Sindrome di DORFMAN-‐CHANARIAN
MUCOPOLISACCARIDOSI

I SCENARIO:
BAMBINO SOVRAPPESO/OBESO

COSA CERCARE IN LABORATORIO?
Laboratorio (Metabolic function and liver tests) • LFT’s (AST, ALT, GGT, ALP, albumina, PT, BT e BD,Quick)
• Profilo lipidico (colesterolo LDL, colesterolo HDL, trigliceridi)
• Tolleranza glucidica (Glicemia, insulinemia, OGTT, Hb glicosilata)
• Uricemia
• Profilo tiroideo
. Sierologia celiachia
. Ceruloplasmina
POSITION PAPER OF ESPGHAN; JPGN 2012; 54

Nat Clin Pract Endocrinol Metab. 2007 Jun;3:458-‐69
“NAFLD can be considered a liver manifestaEon of the metabolic syndrome”
NAFLD

Sì, Sì, è proprio grasso…e ora che si fa?

COME SI CALCOLA UNA DIETA IPOCALORICA IN UN BAMBINO
OBESO ? • Identificare il peso ideale (=quello corrispondente al 50° percentile per la
statura)
• Calcolare il fabbisogno calorico corrispondente al peso ideale con la seguente formula:
- tra 11 e 20 Kg: 1000 + [(Peso Ideale-10) x 50]
- >20 Kg: 1500 + [(Peso Ideale –20) x 20]
• Sottrarre il 20% al risultato ottenuto
Esempio:
Peso ideale = 25Kg; Fabbisogno =1600 Kcal/die;
Dieta da prescivere = 1300 kcal/die

Hepatology 2006;2:456-60

Quando il gatto non c’è….
COSA SUCCEDE NEL TEMPO?
Gut 2009; 58:1538-1544

Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Wilson disease (58), and autoimmune hepatitis (56,26). ALT serumlevels alone are a useful tool, but they are not adequate as a singlemarker for diagnosing NAFLD. The presence of hepatomegaly orsplenomegaly is suggestive of advanced liver disease, which callsfor a rapid and complete assessment, including early liver biopsy toexclude other etiologies (19).
The differential diagnosis of NAFLD/NASH is detailed inTable 2 and the proposed workup is outlined in Table 3. NAFLDusually does not occur in extremely young children (younger than3 years) and is rare in children younger than 10 years. Differentialdiagnosis should be based first on clinical features, then on bloodtests, and finally liver biopsy must be considered (Fig. 1).
Executive Summary
The panel indicates a high suspicion of metabolic disordersas cause of fatty liver in young children. NAFLD hardly occurs inchildren younger than 3 years and is rare in children younger than10 years. Thus, young children require a detailed diagnostic work-up to exclude other etiologies. In older children and teenagers, somemetabolic disorders should also be considered for differentialdiagnosis. Obesity per se does not justify making the diagnosisof NAFLD in patients with increased transaminase activity.
THE REFERENCE STANDARD: LIVER BIOPSYLiver biopsy is the test with the highest discrimination for
excluding other potentially treatable conditions. It is also the only
single test that can reliably distinguish between simple steatosis(NAFLD) and NASH. As summarized in Table 1, it providesimportant information regarding the degree of liver damage,changes in the liver architecture, and severity of inflammatoryactivity and fibrosis (59). Normal liver function tests do not excludeany degree of NAFLD-related liver injury (41). Furthermore,evaluation of liver biopsy may be essential for detecting coexistingdiseases (eg, for diagnosis of autoimmune hepatitis).
The principal histological features of NASH include thepresence of macrovesicular fatty changes of hepatocytes withdisplacement of the nucleus to the edge of the cell, ballooningdegeneration of hepatocytes, and a mixed lobular inflammation.Other features, such as perisinusoidal-pericellular fibrosis, Malloryhyaline, megamitochondria, acidophil bodies, and glycogenatednuclei, can be present but are not mandatory to establish thediagnosis of NASH (60).
In an effort to standardize the histological criteria, theNational Institute of Diabetes and Digestive and Kidney Diseasesponsored the NASH Clinical Research Network to developthe NAFLD activity score (NAS) (59). This score is based onthe classification proposed earlier by Brunt et al (61) and consistsof an unweighted sum for each of the following lesions: steatosis(0–3), lobular inflammation (0–3), and hepatocellular ballooning(0–2). A score!5 is strongly suggestive of NASH, whereas a score<3 is largely consistent with the absence of NASH; however, theNAS cannot replace a pathologist’s diagnosis of steatohepatitis.Furthermore, its utility in assessing the response to therapeuticintervention remains to be determined.
Obese children and adolescents
Perform LFTs and sonography in all
If US hyperechogenicity or increased AST/ALT
Consider age, history, and physical examination
Children >10 y(NAFLD more probable)
Children 3-10 y(NAFLD less probable)
Infants & children <3 y(NAFLD less probable)
NAFLD diagnosis should bebased after exclusions ofviral, toxic, metabolic (eg,
WD), systemic causes(eg, CD) workup
If central obesity, IR andno clinical signs of
progressive liver disease
Trial of weight reductionand lifestyle changes for
3-6 months
If persistenthypertransaminasemiaor hyperechogenicity at
US
Perform laboratoryworkup of exclusion of
other causes
If sustainedhypertransaminasemia orhyperechogenicity at US
If negative or inconclusive
Consider liver biopsy after completionof laboratory diagnostic workup Consider early liver biopsy Consider liver biopsy Consider early liver biopsy
Family histoty of NASHHepartosplenomegalyComorbiditiesHypothalamicExpansive processesMarkedhypertransaminaserniaElevated fibrosisserum markers
Suspect first other disease: genetic/metabolic, syndromic, systemic
causes workupNAFLD diagnosis must be critically
questioned
If normal
Follow for central obesity &consider fatty liver at MRI if clinical
signs of insulin resistance (IR)
Nonobese childrenadolescentswith hyper-
transaminasemiaand hyperechogenic
liver
FIGURE 1. Overall management algorithm for children with suspected nonalcoholic fatty liver disease (NAFLD). CD" celiacdisease; LFTs" liver function tests; MRI"magnetic resonance imaging; US"ultrasound; WD"Wilson disease.
Vajro et al JPGN # Volume 54, Number 5, May 2012
704 www.jpgn.org
POSITION PAPER OF ESPGHAN; JPGN 2012; 54

Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Diagnosis of Nonalcoholic Fatty Liver Disease in Childrenand Adolescents: Position Paper of the ESPGHAN
Hepatology Committee!Pietro Vajro, ySelvaggia Lenta, zPiotr Socha, §Anil Dhawan, jjPatrick McKiernan,
#Ulrich Baumann, !!Ozlem Durmaz, yyFlorence Lacaille, zzValerie McLin, and !Valerio Nobili
ABSTRACT
Nonalcoholic fatty liver disease (NAFLD) is the most common cause ofchronic liver disease in children and adolescents in the United States, andmost probably also in the rest of the industrialized world. As the prevalenceof NAFLD in childhood increases with the worldwide obesity epidemic,there is an urgent need for diagnostic standards that can be commonly usedby pediatricians and hepatologists. To this end, we performed a PubMedsearch of the adult and pediatric literature on NAFLD diagnosis throughMay2011 using Topics and/or relevant Authors as search words. According to thepresent literature, NAFLD is suspected based on the association of fatty livercombined with risk factors (mainly obesity), after the exclusion of othercauses of liver disease. The reference but imperfect standard for confirmingNAFLD is liver histology. The following surrogate markers are presentlyused to estimate degree of steatosis and liver fibrosis and risk of progressionto end-stage liver disease: imaging by ultrasonography or magneticresonance imaging, liver function tests, and serum markers of liver fibrosis.NAFLD should be suspected in all of the overweight or obese children andadolescents older than 3 years with increased waist circumference especiallyif there is a NAFLDhistory in relatives. The typical presentation, however, isin children ages 10 years and older. The first diagnostic step in these childrenshould be abdominal ultrasound and liver function tests, followed by
exclusion of other liver diseases. Overweight/obese children with normalultrasonographic imaging and normal liver function tests should still bemonitored due to the poor sensitivity of these tests at a single assessment.Indications for liver biopsy include the following: to rule out othertreatable diseases, in cases of clinically suspected advanced liver disease,before pharmacological/surgical treatment, and as part of a structuredintervention protocol or clinical research trial.
Key Words: children, histology, imaging, liver biopsy, nonalcoholic fatty
liver disease, nonalcoholic steatohepatitis, noninvasive biomarkers, obesity-
related liver disease
(JPGN 2012;54: 700–713)
O besity is a major public health concern. The rise in theincidence of obesity diffusion is paralleled by that of its
comorbidities, including nonalcoholic fatty liver disease (NAFLD)(1). The latter includes a spectrum of clinicopathological entitiesranging from simple steatosis through nonalcoholic steatohepatitis(NASH) to cirrhosis and end-stage liver disease (Table 1).The nomenclature is inconsistent, with NAFLD being both thesummarizing term for the entire spectrum of the condition and thedescriptor of the more benign forms of simple steatosis and mildinflammation in contrast to NASH. The histopathological definitionof steatohepatitis requires at least 5% of liver cells with micro- ormacrovesicular fatty infiltration. NAFLD has become the mostcommon chronic hepatopathy both in adults and children. Itshistologically proven prevalence in children in the United States(as revealed at autopsy after accidents) ranges from 9.6% in normal-weight individuals up to 38% in obese ones (2). Due to its tendencyto progress through this spectrum in childhood (3) or after transitioninto adulthood (4), early diagnosis and treatment are importantissues at all ages (5). Treatment should address not only the liverdisease itself but also the entire spectrum of comorbidities toimprove overall survival and quality of life (6).
Available diagnostic procedures include a set of clinicalsigns and symptoms, laboratory and radiological imaging tests,and a combination of clinical parameters and blood test results (7,8).Although several of these markers are commonly used for thediagnostic evaluation of a patient with suspected NAFLD, noneof them seems to have a high specificity and sensitivity capableof definitely excluding another underlying liver disease. With therising prevalence of childhood obesity, the proportion of childrenwith both an underlying primary liver disease, such as autoimmuneliver disease or Wilson disease, and additional NAFLD increases,so it becomes essential not to miss a treatable condition. Also,only liver histology can distinguish simple steatosis or mild inflam-matory changes from NASH and determine the presence and stage
Received December 6, 2011; accepted February 23, 2012.From the !Department of Pediatrics, Medical School, University of
Salerno, Salerno, Italy, the yDepartment of Pediatrics, University ofNaples ‘‘Federico II,’’ Naples, Italy, the zDepartment of Gastroenter-ology, Hepatology, and Eating Disorders, the Children’s MemorialHealth Institute, Warsaw, Poland, the §Liver Unit, King’s College,London, the jjLiver Unit, Birmingham Children’s Hospital, Birming-ham, UK, the !Hepatometabolic Unit, ‘‘Bambino Gesu’’ Children’sHospital, Rome, Italy, the #Division of Pediatric Gastroenterology andHepatology, Hannover Medical School, Hannover, Germany, the!!Department of Pediatrics, Istanbul Medical Faculty, University ofIstanbul, Turkey, the yyHopital Necker-Enfants Malades, Paris, France,and the zzDepartment of Pediatrics, University of Geneva Hospital,Geneva, Switzerland
Address correspondence and reprint requests to Pietro Vajro, MD, Chair ofPediatrics, University of Salerno, Via Allende, 84081 Baronissi(Salerno), Italy (e-mail: e-mail [email protected])
Drs Vajro, Socha, Dhawan, McKiernan, and Nobili are members of theNAFLD Group of the ESPGHAN Hepatology Committee. Drs Bau-mann, Durmaz, Lacaille, and McLin are other members of the ESP-GHAN Hepatology Committee. Dr Lenta is an invited expertparticipating in this ESPGHAN panel.
Conflicts of interest for the writing group appear on the ESPGHANWeb site(www.espghan.med.up.pt).
Copyright # 2012 by European Society for Pediatric Gastroenterology,Hepatology, and Nutrition and North American Society for PediatricGastroenterology, Hepatology, and Nutrition
DOI: 10.1097/MPG.0b013e318252a13f
CONSENSUS STATEMENT
700 JPGN " Volume 54, Number 5, May 2012
Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Diagnosis of Nonalcoholic Fatty Liver Disease in Childrenand Adolescents: Position Paper of the ESPGHAN
Hepatology Committee!Pietro Vajro, ySelvaggia Lenta, zPiotr Socha, §Anil Dhawan, jjPatrick McKiernan,
#Ulrich Baumann, !!Ozlem Durmaz, yyFlorence Lacaille, zzValerie McLin, and !Valerio Nobili
ABSTRACT
Nonalcoholic fatty liver disease (NAFLD) is the most common cause ofchronic liver disease in children and adolescents in the United States, andmost probably also in the rest of the industrialized world. As the prevalenceof NAFLD in childhood increases with the worldwide obesity epidemic,there is an urgent need for diagnostic standards that can be commonly usedby pediatricians and hepatologists. To this end, we performed a PubMedsearch of the adult and pediatric literature on NAFLD diagnosis throughMay2011 using Topics and/or relevant Authors as search words. According to thepresent literature, NAFLD is suspected based on the association of fatty livercombined with risk factors (mainly obesity), after the exclusion of othercauses of liver disease. The reference but imperfect standard for confirmingNAFLD is liver histology. The following surrogate markers are presentlyused to estimate degree of steatosis and liver fibrosis and risk of progressionto end-stage liver disease: imaging by ultrasonography or magneticresonance imaging, liver function tests, and serum markers of liver fibrosis.NAFLD should be suspected in all of the overweight or obese children andadolescents older than 3 years with increased waist circumference especiallyif there is a NAFLDhistory in relatives. The typical presentation, however, isin children ages 10 years and older. The first diagnostic step in these childrenshould be abdominal ultrasound and liver function tests, followed by
exclusion of other liver diseases. Overweight/obese children with normalultrasonographic imaging and normal liver function tests should still bemonitored due to the poor sensitivity of these tests at a single assessment.Indications for liver biopsy include the following: to rule out othertreatable diseases, in cases of clinically suspected advanced liver disease,before pharmacological/surgical treatment, and as part of a structuredintervention protocol or clinical research trial.
Key Words: children, histology, imaging, liver biopsy, nonalcoholic fatty
liver disease, nonalcoholic steatohepatitis, noninvasive biomarkers, obesity-
related liver disease
(JPGN 2012;54: 700–713)
O besity is a major public health concern. The rise in theincidence of obesity diffusion is paralleled by that of its
comorbidities, including nonalcoholic fatty liver disease (NAFLD)(1). The latter includes a spectrum of clinicopathological entitiesranging from simple steatosis through nonalcoholic steatohepatitis(NASH) to cirrhosis and end-stage liver disease (Table 1).The nomenclature is inconsistent, with NAFLD being both thesummarizing term for the entire spectrum of the condition and thedescriptor of the more benign forms of simple steatosis and mildinflammation in contrast to NASH. The histopathological definitionof steatohepatitis requires at least 5% of liver cells with micro- ormacrovesicular fatty infiltration. NAFLD has become the mostcommon chronic hepatopathy both in adults and children. Itshistologically proven prevalence in children in the United States(as revealed at autopsy after accidents) ranges from 9.6% in normal-weight individuals up to 38% in obese ones (2). Due to its tendencyto progress through this spectrum in childhood (3) or after transitioninto adulthood (4), early diagnosis and treatment are importantissues at all ages (5). Treatment should address not only the liverdisease itself but also the entire spectrum of comorbidities toimprove overall survival and quality of life (6).
Available diagnostic procedures include a set of clinicalsigns and symptoms, laboratory and radiological imaging tests,and a combination of clinical parameters and blood test results (7,8).Although several of these markers are commonly used for thediagnostic evaluation of a patient with suspected NAFLD, noneof them seems to have a high specificity and sensitivity capableof definitely excluding another underlying liver disease. With therising prevalence of childhood obesity, the proportion of childrenwith both an underlying primary liver disease, such as autoimmuneliver disease or Wilson disease, and additional NAFLD increases,so it becomes essential not to miss a treatable condition. Also,only liver histology can distinguish simple steatosis or mild inflam-matory changes from NASH and determine the presence and stage
Received December 6, 2011; accepted February 23, 2012.From the !Department of Pediatrics, Medical School, University of
Salerno, Salerno, Italy, the yDepartment of Pediatrics, University ofNaples ‘‘Federico II,’’ Naples, Italy, the zDepartment of Gastroenter-ology, Hepatology, and Eating Disorders, the Children’s MemorialHealth Institute, Warsaw, Poland, the §Liver Unit, King’s College,London, the jjLiver Unit, Birmingham Children’s Hospital, Birming-ham, UK, the !Hepatometabolic Unit, ‘‘Bambino Gesu’’ Children’sHospital, Rome, Italy, the #Division of Pediatric Gastroenterology andHepatology, Hannover Medical School, Hannover, Germany, the!!Department of Pediatrics, Istanbul Medical Faculty, University ofIstanbul, Turkey, the yyHopital Necker-Enfants Malades, Paris, France,and the zzDepartment of Pediatrics, University of Geneva Hospital,Geneva, Switzerland
Address correspondence and reprint requests to Pietro Vajro, MD, Chair ofPediatrics, University of Salerno, Via Allende, 84081 Baronissi(Salerno), Italy (e-mail: e-mail [email protected])
Drs Vajro, Socha, Dhawan, McKiernan, and Nobili are members of theNAFLD Group of the ESPGHAN Hepatology Committee. Drs Bau-mann, Durmaz, Lacaille, and McLin are other members of the ESP-GHAN Hepatology Committee. Dr Lenta is an invited expertparticipating in this ESPGHAN panel.
Conflicts of interest for the writing group appear on the ESPGHANWeb site(www.espghan.med.up.pt).
Copyright # 2012 by European Society for Pediatric Gastroenterology,Hepatology, and Nutrition and North American Society for PediatricGastroenterology, Hepatology, and Nutrition
DOI: 10.1097/MPG.0b013e318252a13f
CONSENSUS STATEMENT
700 JPGN " Volume 54, Number 5, May 2012
Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
range (41). In fact, determining an ALT cutoff for NAFLD has beenthe subject of some debate. In a study involving 72 obese childrenwith NAFLD, an ALT >35 IU/L had a sensitivity of 48% andspecificity of 94% for detecting steatosis >5% as measured bymagnetic resonance imaging (MRI) (42). More recently, the Screen-ingALT forElevation inToday’sYouth (SAFETY) study has shownthat in American laboratories conventional ALT cutoff values are settoo high for the reliable detection of pediatric chronic liver disease,includingNAFLD. In theNational Health andNutrition ExaminationSurvey (NHANES) study, the 95th percentile levels for ALT inhealthy weight, metabolically normal, liver disease–free patientswere 25.8 U/L (boys) and 22.1 U/L (girls) (43). Comparable con-clusions were also reached in the European pediatric population (44).
It is now widely accepted that the degree of ALT elevationdoes not correlate with the presence (42,45) or severity of histo-logical findings of NAFLD (40). A number of children with normalALT or minimal serum ALT elevation may have advanced fibrosison liver biopsy. The natural history of the disease is not yet welldetermined in children, but at times ALT tends to fluctuate and mayeven normalize (22,41). High serum levels of GGT represent a riskfactor for advanced fibrosis in NAFLD (46).
NAFLD may be considered the hepatic manifestation of themetabolic syndrome, which is defined by the presence of visceralobesity, hypertension, insulin resistance or diabetes, dyslipidemia,and hyperuricemia. Hyperinsulinemia, due to insulin resistance,most probably represents the first pathogenetic hit of NAFLD (47).It is a sensitive but nonspecific predictor of NAFLD (48), and henceunsuitable as a single indicator of NAFLD; however, it may be apredictor for progressive hepatic fibrosis (21,26). Abnormalities inthe oral glucose tolerance test also may suggest NAFLD (49).
Hypertriglyceridemia is another biochemical marker fre-quently reported in obese children with NAFLD (21). Oliveiraet al (50) showed a positive correlation between ALT and trigly-ceride values among pediatric patients. Others showed that amongpatients with suspected steatohepatitis, ALT concentration wassignificantly higher in subjects with elevated triglycerides (51).Finally, in children with NAFLD, an atherogenic lipid profilecorrelates with severity of liver injury (52). High levels of serumuric acid have been reported in the majority of subjects with the
metabolic syndrome, and has been proposed as an independentpredictor of NAFLD both in adults (53) and children (49), probablyas a marker of high fructose consumption that correlates with theprogression of fibrotic changes (30). Serum IgA level is elevatedin about 25% of cases of NAFLD-NASH, but its meaning anddiagnostic value are still not clear. High levels of IgA antibodiesagainst tissue transglutaminase have been reported in several chronicliver diseases, including NAFLD (54). Silent celiac disease and fattyliver have been reported to coexist in unrecognized obese children(55).
Increased titers of serum nonorgan-specific autoantibodies(particularly anti-nuclear antibody and anti-smooth muscle anti-body) have been reported in up to one-third of all of the investigatedpatients, both in adults (56) and children (26), and may requireimmediate definitive further investigation to rule out associatedautoimmune hepatitis. Table 3 summarizes the biochemicalmarkers routinely performed in clinical practice in suspectedpediatric NAFLD (7,8).
Executive Summary
The panel agreed that careful consideration of a series ofanthropometric, demographic, clinical, and laboratory featuresmay offer a clue to the identification of NAFLD risk. Acanthosisnigricans and increased waist circumference are warning signs forNAFLD. ALT in combination with liver ultrasound is an indicatorof NAFLD, but normal ALT does not exclude liver steatosis orits progression to severe fibrosis and cirrhosis. Insulin resistanceand increased triglyceride concentration are additional risk factorsof NAFLD. These factors were identified based on observationalstudies that associated NAFLD with clinical, anthropometric, andlaboratory parameters.
DIFFERENTIAL DIAGNOSISAbnormal serum aminotransferases in overweight or obese
patients are not diagnostic of NAFLD/NASH. Other causes ofmuscle (57) and treatable liver disease should be ruled out, withspecial emphasis on celiac disease–related hepatopathy (55),
TABLE 3. Laboratory workup in children with suspected NAFLD
Metabolic function and liver testsBasic profile: blood counts, standard liver function tests, fasting glucose and insulin, urea and electrolytes, coagulation, INR,ALT/AST ratio
Lipid profile (cholesterol, triglycerides, HDL-cholesterol, LDL-cholesterol), lipoproteinsGlucose tolerance test (OGTT), glycosylated hemoglobinCalculation of HOMA-IR, ISI-gly as markers for insulin resistanceThyroid function tests
Tests for exclusion of other main causes of hepatic steatosisSerum lactate, uric acid, iron, ferritin, pyruvateSerum copper, ceruloplasmin levels, 24-hour urinary copperSweat testAntibodies against tissue transglutaminase IgA and total IgAa1-Antitrypsin levels and phenotype when indicatedAmino and organic acidsPlasma-free fatty acids and acyl carnitine profileUrinary steroid metabolitesOther specific tests as suggested by history and examination (eg, viral hepatitis panel, serum immunoglobulins, liver autoantibodies)
Modified from (7,8). ALT! alanine aminotransferase; AST! aspartate aminotransferase; HDL! high-density lipoprotein; HOMA-IR! homeostaticmodel assessment; INR! international normalized ratio; ISI-gly! insulin sensitivity index; LDL! low-density lipoprotein; OGTT! oral glucosetolerance test.
JPGN " Volume 54, Number 5, May 2012 Diagnosis of NAFLD in Children and Adolescents
www.jpgn.org 703

Low serum titers of autoantibodies are often present in children with NAFLD, but higher titers, particularly in association with higher serum aminotransferases and high globulin should prompt a liver biopsy to evaluate for possible autoimmune hepatitis. (Strength – 2, Quality – B)
RecommendaEons

II SCENARIO:
BAMBINO NORMOPESO
III SCENARIO: LATTANTE
NORMOPESO

RecommendaEons Children with faDy liver who are very young or not overweight should be tested for monogenic causes of chronic liver disease such as faDy acid oxidaIon defects, lysosomal storage diseases and peroxisomal disorders, in addiIon to those causes considered for adults. (Strength – 2, Quality – C)

II SCENARIO:
BAMBINO NORMOPESO

QUALI ESAMI FARE?
LFTs (AST, ALT, GGT, albumina, PT, BT e BD, Quick, glicemia)
• Profilo 0roideo
• Sierologia per celiachia
• Colesterolo tot e LDL, Tgl, evt APO B
• Ceruloplasmina sierica, cupruria
• Ig tot, QPE, ANA, LKM1 (se ipertransaminasemia da 6 mesi)
• HCV-‐Ab
• Ele6roforesi delle glicoproteine (evnt dosaggio enzima0co leucicitario)
• Ammonio, acido la1co, EAB, clinitest su urine, amminoacidi sierici e urinari, acidi organici
urinari, acilcarni0ne, ele6roforesi delle glicoproteine
• Visita oculis0ca
• Funzionalità pancrea0ca-‐ test del sudore

STEATOSI NON SOLO OBESITA’…
POSITION PAPER OF ESPGHAN; JPGN 2012; 54
Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Clinical Features
Clinically, most pediatric patients with NAFLD/NASHhave nonspecific symptoms. Some complain of fatigue, malaise,or vague abdominal pain (42%–59% of cases), especially in theright upper quadrant, which has been associated with the moreprogressive form of NASH (2). Acanthosis nigricans is a clinicalmarker of hyperinsulinemia and has been observed in one-third tohalf of the children with biopsy-proven NAFLD (23). Hepatome-galy can be frequently detected (up to 50% of cases) (21,22).
Anthropometric Features
Visceral adiposity, which may be related to a state of insulinresistance, is a major contributor to fatty liver, representing a moreinfluential component than BMI in predicting liver steatosis.Unfortunately, indirect measurements of visceral adiposity usedin adult studies such as waist-to-hip ratio are not appropriate forchildhood because they change with age and have poor correlationwith measures of adiposity measured by DEXA (32,33). In children,waist circumference alone represents a practical anthropometricparameter to identify central adiposity and it may predict increased
risk for insulin resistance and the metabolic syndrome (34). Specificpercentiles have been developed for children ages 5 to 16 years (35)and 11 to 18 years (36). The importance of waist circumferencemeasurement in childhood NAFLD is well established (37).Lin et al (37) showed that in obese children and adolescents, forevery 5-cm increase in waist circumference, there was an odds ratioof 1.4 for predicting ultrasonographic liver steatosis, but no detailson percentiles were given. Increased waist circumference is alsoassociated with increased hepatic fibrosis (38). There is a need forstandard international waist circumference charts.
Laboratory Tests
In clinical practice the diagnosis of NAFLD is usuallysuggested by finding elevated serum hepatobiliary enzymes(mostly ALT and g-glutamyl transpeptidase [GGT]), and/or evi-dence of a bright liver on ultrasound (US), most frequently amongoverweight/obese children (27,39,40).
SerumALT activity is a widely available and inexpensive testfor the screening and initial evaluation of NAFLD. The sensitivity ofthis biochemical marker, however, remains low because a number ofadult and pediatric patients may present ALT values in the normal
TABLE 2. Causes of fatty liver disease in children
General or systemic Genetic-metabolic causesOther rare hereditarygenetic disorders Drugs’ hepatotoxicity
Acute systemic disease Cystic fibrosis and Shwachmansyndrome
Alstrom syndrome Ethanol
Acute starvation Wilson disease Bardet-Biedl syndrome Ecstasy, cocaineProtein energy malnutrition a1-Antitrypsin deficiency Prader-Willi syndrome NifedipineTotal parenteral nutrition Galactosemia Cohen syndrome DiltiazemObesity/metabolic syndrome Fructosemia Cantu syndrome (1p36 deletion) EstrogensPolycystic ovary syndrome Cholesteryl ester storage disease Weber-Christian disease CorticosteroidsObstructive sleep apnea Glycogen storage disease
(types I and VI)Amiodarone
Rapid weight loss Mitochondrial and peroxisomaldefects of fatty acid oxidation
Perhexiline
Anorexia nervosa Madelung lipomatosis CoralgilCachexia Lipodystrophies TamoxifenInflammatory bowel disease Dorfman-Chanarin syndrome MethotrexateCeliac disease Abeta or hypobetalipoproteinemia PrednisoloneHepatitis C a- and b-oxidation defects ValproateNephrotic syndrome Porphyria cutanea tarda VitaminType 1 diabetes mellitusand Mauriac syndrome
Homocystinuria L-asparaginase
Thyroid disorders Familial hyperlipoproteinemias Zidovudine andHIV treatments
Hypothalamo-pituitary disorders Tyrosinemia type 1 SolventsBlind loop (bacterial overgrowth) Bile acids synthesis defects Pesticides
Congenital disorders of glycosylationTurner syndromeOrganic acidosisCitrin deficiencyHFE (hemochromatosis)
Modified from (7,19,20). Exclusions should be adjusted to age and clinical presentation. In infants and young children, NAFLD is hardly to be expected,whereas genetic, metabolic, syndromic, and systemic causes should be primarily considered guided by clinical signs and symptoms. In children older than10 years, NAFLD is expected when!1 features of the metabolic syndrome are present; still, Wilson disease and a1-antitrypsin deficiency should be excludedand autoimmune hepatitis should be considered.
Vajro et al JPGN " Volume 54, Number 5, May 2012
702 www.jpgn.org

STEATOSI NON SOLO OBESITA’…
POSITION PAPER OF ESPGHAN; JPGN 2012; 54
Copyright 2012 by ESPGHAN and NASPGHAN. Unauthorized reproduction of this article is prohibited.
Clinical Features
Clinically, most pediatric patients with NAFLD/NASHhave nonspecific symptoms. Some complain of fatigue, malaise,or vague abdominal pain (42%–59% of cases), especially in theright upper quadrant, which has been associated with the moreprogressive form of NASH (2). Acanthosis nigricans is a clinicalmarker of hyperinsulinemia and has been observed in one-third tohalf of the children with biopsy-proven NAFLD (23). Hepatome-galy can be frequently detected (up to 50% of cases) (21,22).
Anthropometric Features
Visceral adiposity, which may be related to a state of insulinresistance, is a major contributor to fatty liver, representing a moreinfluential component than BMI in predicting liver steatosis.Unfortunately, indirect measurements of visceral adiposity usedin adult studies such as waist-to-hip ratio are not appropriate forchildhood because they change with age and have poor correlationwith measures of adiposity measured by DEXA (32,33). In children,waist circumference alone represents a practical anthropometricparameter to identify central adiposity and it may predict increased
risk for insulin resistance and the metabolic syndrome (34). Specificpercentiles have been developed for children ages 5 to 16 years (35)and 11 to 18 years (36). The importance of waist circumferencemeasurement in childhood NAFLD is well established (37).Lin et al (37) showed that in obese children and adolescents, forevery 5-cm increase in waist circumference, there was an odds ratioof 1.4 for predicting ultrasonographic liver steatosis, but no detailson percentiles were given. Increased waist circumference is alsoassociated with increased hepatic fibrosis (38). There is a need forstandard international waist circumference charts.
Laboratory Tests
In clinical practice the diagnosis of NAFLD is usuallysuggested by finding elevated serum hepatobiliary enzymes(mostly ALT and g-glutamyl transpeptidase [GGT]), and/or evi-dence of a bright liver on ultrasound (US), most frequently amongoverweight/obese children (27,39,40).
SerumALT activity is a widely available and inexpensive testfor the screening and initial evaluation of NAFLD. The sensitivity ofthis biochemical marker, however, remains low because a number ofadult and pediatric patients may present ALT values in the normal
TABLE 2. Causes of fatty liver disease in children
General or systemic Genetic-metabolic causesOther rare hereditarygenetic disorders Drugs’ hepatotoxicity
Acute systemic disease Cystic fibrosis and Shwachmansyndrome
Alstrom syndrome Ethanol
Acute starvation Wilson disease Bardet-Biedl syndrome Ecstasy, cocaineProtein energy malnutrition a1-Antitrypsin deficiency Prader-Willi syndrome NifedipineTotal parenteral nutrition Galactosemia Cohen syndrome DiltiazemObesity/metabolic syndrome Fructosemia Cantu syndrome (1p36 deletion) EstrogensPolycystic ovary syndrome Cholesteryl ester storage disease Weber-Christian disease CorticosteroidsObstructive sleep apnea Glycogen storage disease
(types I and VI)Amiodarone
Rapid weight loss Mitochondrial and peroxisomaldefects of fatty acid oxidation
Perhexiline
Anorexia nervosa Madelung lipomatosis CoralgilCachexia Lipodystrophies TamoxifenInflammatory bowel disease Dorfman-Chanarin syndrome MethotrexateCeliac disease Abeta or hypobetalipoproteinemia PrednisoloneHepatitis C a- and b-oxidation defects ValproateNephrotic syndrome Porphyria cutanea tarda VitaminType 1 diabetes mellitusand Mauriac syndrome
Homocystinuria L-asparaginase
Thyroid disorders Familial hyperlipoproteinemias Zidovudine andHIV treatments
Hypothalamo-pituitary disorders Tyrosinemia type 1 SolventsBlind loop (bacterial overgrowth) Bile acids synthesis defects Pesticides
Congenital disorders of glycosylationTurner syndromeOrganic acidosisCitrin deficiencyHFE (hemochromatosis)
Modified from (7,19,20). Exclusions should be adjusted to age and clinical presentation. In infants and young children, NAFLD is hardly to be expected,whereas genetic, metabolic, syndromic, and systemic causes should be primarily considered guided by clinical signs and symptoms. In children older than10 years, NAFLD is expected when!1 features of the metabolic syndrome are present; still, Wilson disease and a1-antitrypsin deficiency should be excludedand autoimmune hepatitis should be considered.
Vajro et al JPGN " Volume 54, Number 5, May 2012
702 www.jpgn.org

Recommendations Liver biopsy in children with suspected NAFLD should be performed in those where the diagnosis is unclear, where there is possibility of multiple diagnoses, or before starting therapy with potentially hepatotoxic medications. (Strength – 1, Quality – B) Liver biopsy to establish a diagnosis of NASH should be obtained prior to starting children on pharmacologic therapy for NASH. (Strength – 2, Quality – C).

STEATOSI EPATICA IN PEDIATRIA: TAKE HOME MESSAGES
§ Dis0nguere i pazien0 con steatosi in base alla presenza di obesità. Se l’obesità è
presente, è alta la probabilità di NAFLD. Consigliare dieta ipocalorica e incremento
a1vità fisica. Tener presen0 gli altri organi-‐bersaglio della sindrome metabolica
(complicanze cardiovascolari)
§ In assenza di obesità e negli obesi che rimangono steatosici nonostante il calo ponderale
considerare la possibilità di disordini gene0co-‐metabolici o di altre cause (celiachia,
farmaci, etc)
§ La steatosi epa0ca va sempre indagata nel bambino di età inferiore ai 3 anni con
l’obie1vo di escludere mala1e gene0co-‐metaboliche.

The Evolution of Man

The Evolution of ...liver