reentrant ventricular arrhythmias in the late myocardial infarction period: 17. correlation of...
TRANSCRIPT
Reentrant ventricular arrhythmias in the late myocardial infarction period: 17. Correlation of activation patterns of sinus and reentrant ventricular tachycardia
The relationship between myocardial sites with late activation during sinus rhythm and sites cr i t ica l for the initiation and sustentation of reentrant ventricular tachycardia was systematically examined in the 4-day-old postinfarcUon canine heart. The critical sites for prevention of the initiation of reentry and for termination of sustained figure-of-8 reentrant tachycardia by cryothermal techniques were correlated with the last 20 msec isochrone during sinus rhythm. In 12 exper iments , 20 cr i t ica l sites were examiend. The m e a n distance between sites critical for reentry and the latest isochrone during sinus rhythm was 26.7 -+ 13.3 mm. Only five sites (25%) were within a 12 mm distance, which corresponded to the diameter of the cryoprobe. Nine sites (45%) were within a 24 mm d is tance ( twice the diameter of the cryoprobe), while 11 si tes (55%) were separated by more than 24 ram. In three experiments the sites of latest activation during sinus rhythm represented areas showing Wenckebach period or 2:1 conduction block. These sites became dissociated and did not participate in the reentrant excitation induced by premature stimulation. Poor correlation was explained by the fact that sites critical for reentry were intimately related to the location and extent of the arcs of functional conduction block while sites of delayed activation during sinus rhythm were not. (AM HEART J 1990;119:1014. )
Mahsh id Assadi, MD, M a r k Restivo, PhD, Will iam B. Gough, PhD, and
Nabi l E1-Sherif, MD. Brooklyn, N.Y.
T h e re la t ionship be tween vent r icular myocard ia l zones with late ac t ivat ion dur ing sinus r h y t h m and myocard ia l zones providing the electrophysiologic subs t ra te for r e e n t r a n t r h y t h m s has not been sys- t emat ica l ly invest igated. These da ta could provide the answer to whe ther m a p p i n g of vent r icular acti- va t ion dur ing sinus r h y t h m could be used to guide surgical or abla t ive t h e r a p y of r een t r an t a r rhy thmias in the opera t ing room or in the electrophysiology laboratory .
T h e 4-day-old pos t infarc t ion canine hear t is a d o c u m e n t e d exper imen ta l model of r een t r an t ven- t r icular r h y t h m s and is an app rop r i a t e model to s t udy the above re la t ionship for the following tea-
From the Cardiology Division, Department of Medicine. State University of New York, Health Science Center and Veterans Administration Medical Center. Supported by National Institutes of Health Grants HL 36680 and HL 31341 and by the Veterans Administration Medical Research Funds. Received for publication Aug. 30, 1989; accepted Dec. 20, 1989. Reprint requests: Nabil E1-Sherif, MD, Cardiology Division, SUNY Health Science Center, 450 Clarkson Ave., P.O. Box 1199, Brooklyn, NY 11203. 4/1 / 1 9 0 8 5
sons. First , the r een t r an t circuits are located in the surviving electrophysiological ly abnorma l epicardial layer overlying the infarct ion and are therefore accessible to detai led m a p p i n g of ventr icular activation. 1-5 Second, the crit ical site for t e rmina t ion of r een t ry has been clearly identified. 5 T h e r een t r an t circuit has a figure-of-8 act ivat ion pa t t e rn in the form of clockwise and counterclockwise wave f ronts circu- lating a round two arcs of funct ional conduct ion block and coalescing into a slow common r een t r an t wave front. The common r een t r an t wave f ront was shown to represen t the critical and mos t vulnerable zone of the r e e n t r a n t circuit. 5 R e e n t r a n t exci tat ion could be consis tent ly in te r rup ted only when cooling or cryo- ablat ion was appl ied to this zone. 5, 6 T h e re la t ionship be tween this zone and myocard ia l zones wi th late ac- t ivat ion dur ing sinus r h y t h m w a s critically examined in this s tudy. A pre l iminary repor t was publ ished previously. 7
METHODS
In 20 mongrel dogs weighing 15 to 20 kg, the left anterior descending coronary artery was ligated just distal to the
1014
Volume 119 Number 5 Sinus versus reentrant activation patterns 1015
anterior septal branch. Details of the surgical technique have been described. 3 The dogs were reanesthetized with pentobarbital sodium (30 mg/kg intravenously) 4 days af- ter coronary artery ligation and received supplemental doses as required. Each animal was ventilated with room air through an endotracheal tube with a Harvard positive pressure pump (Harvard Apparatus Inc., S. Natick, Mass.), and in each dog a jugular vein was cannulated for the ad- ministration of. fluids. Electrocardiographic lead II and femoral blood pressure were continuously monitored on an Electronics for Medicine DR10 electrophysiologic recorder (PPG Biomedical Systems, Pleasantville, N.Y.). To slow the sinus rhythm, stimulation of the right and left vago- sympathetic trunks was accomplished by delivery of 0.5 msec square-wave pulses of I to 10 V intensity at a frequency of 10 to 20 Hz through two Teflon-insulated sil- ver wires (0.01 inch in diameter). The heart was exposed through a left thoracotomy and was cradled in the opened pericardium. Ventricular pacing was achieved via two fine Teflon-insulated stainless steel wires (0.005 inch in diam- eter) inserted by a 21-gauge hypodermic needle. Both reg- ular pacing and programmed stimulation were performed with a programmable digital stimulator (Model DTU-101 MVA, Bloom Associates, Ltd., Reading, Pa.). The stimula- tor delivered rectangular pulses of variable duration (usu- ally 2 to 5 msec) and twice diastolic threshold with an ac- curacy up to a 1 msec interval.
A stimulation protocol was selected that resulted in the induction of a reproducible monomorphic ventricular tachycardia. The latter was defined as having similar elec- trocardiographic and activation patterns during three con- secutive trials using the same stimulation protocol. In each experiment, at least two stimulation sites were tested for the induction of a reentrant rhythm. These were usually the right ventricular outflow tract on the septal side of the ischemic zone and a left ventricular site on the lateral bor- der of the ischemic zone. The stimulation protocol consists of $1S1 stimulation for eight beats at a cycle length of 380 msec, followed by the introduction of up to three extra- stimuli. Details of the stimulation protocol in this experi- mental model were previously published, s
Epicardial activation maps were constructed from 62 to 126 simultaneous bipolar electrode recordings obtained with a sock electrode. A higher density of electrodes (approximately 4 to 8 mm between pairs) covered the area of the infarction and the border zones, and a lower density (approximately 10 to 15 mm) covered the remaining surface of the heart. In some experiments a patch electrode was also used to obtain epicardial recordings at a closer in- terelectrode distance (3 to 4 mm). Details of the recording techniques, the mapping system, and the methods for con- struction of epicardial isochronal maps were previously reported.2, 4
Cryothermal techniques. The cryothermal system was a Spembly-Amoils BMS 401 cryo unit (Spembly-Amoils, Ltd., Andover, England). 5 This apparatus regulated the flow of nitrous oxide through the tip of the cryoprobe. The cryoprobe used in the study (No. 7107) had a flat tip 12 mm in diameter. Local epicardial temperature could be mea-
sured by a thermocouple at the tip of the probe, and intra- mural temperature could be measured by a needle ther- mistor. For reversible interruption of reentrant activation, the myocardial temperature at a localized epicardial site was reduced to between -5 ~ and +5 ~ C for 10 to 30 seconds. 5 Three to six different epicardial sites were tested in each experiment, and the effects of transient epicardial cooling on ventricular activation patterns were analyzed. In some experiments, the completion of the stimulation pro- tocol required that the transient cooling procedure be re- peated more than one time at the same site. In those experiments, rewarming followed by reinduction of the control tachycardia was performed before another cooling procedure was evaluated. To achieve cryoablation, the temperature at the tip of the cryoprobe was reduced to be- tween -55 ~ and -65 ~ C for 2 minutes. 5 Sometimes tran- sient cooling of two contiguous sites was performed, in which case the probe was rapidly moved to the second site to achieve local cooling before the effects of cooling on the first site had expired. Alternatively, cryoablation was applied to one site, and transient cooling was applied to a contiguous site.
Prevention of the induction of reentry by cryothermal techniques was considered to have been achieved if three extrastimuli introduced at the shortest possible coupling interval from at least two sites failed to induce a reentrant rhythm.
The site from which the reentrant circuit could be con- sistently terminated by cooling was compared with the epicardial site of the last 20 msec isochrone during sinus rhythm, and the distance between a central point of the two sites was measured in millimeters.
R E S U L T S
A reproducible monomorphic reen t ran t ventricu- lar tachycardia with the reent rant circuit completely identified on the epicardial surface could be induced by p rogrammed st imulat ion in 12 of 20 dogs. In six dogs, the tachycardia was sustained (lasting for more than 1 minute). In the remaining six dogs, nonsus- ta ined ventricular tachycardia, defined as three or more beats and lasting for <1 minute, was induced. In three of these dogs two dist inct ventricular tachy- cardias could be induced, as shown by analysis of ac- t ivat ion maps. In dogs with sustained ventricular tachycardia we utilized reversible cooling to identify the critical epicardial sites for the prevention of ini- t iat ion of reentry and for the terminat ion of reen- t ran t excitation once it was initiated. These sites were no t necessarily similar. In dogs with nonsustained tachycardia, only the critical site for the prevention of initiation of reent ry was identified. The sites crit- ical for reentry were correlated with the site of the last 20 msec epicardial isochrone during sinus rhythm.
Fig. 1 illustrates isochronal maps from a dog in which the critical site for prevent ion of initiation of reent ry was identical with the site f rom which the re-
May 1990 1016 Assadi et al. American Heart Journal
S2 S I N U S C O N T R O L
$2 C R Y O VT
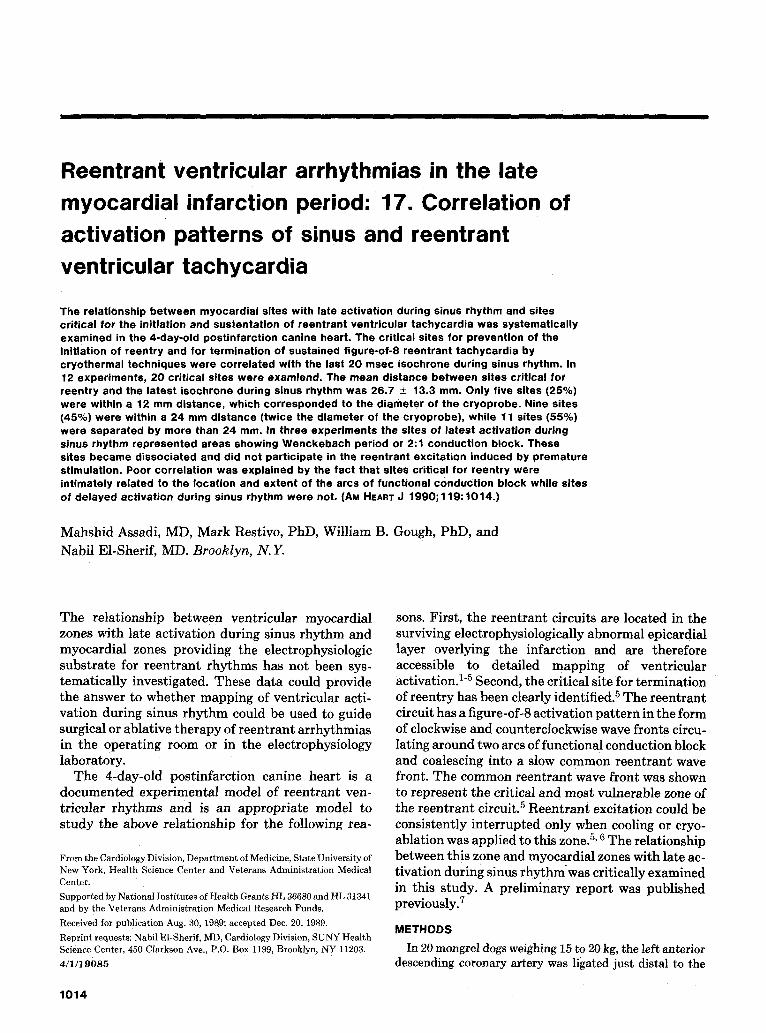
Fig. 1. Epicardial isochronat activation patterns dUring sinus rhythm (upper left map), initiation of re- entry by a single premature Stimulus (upper right map), prevention of initiation of reentry by cooling (lower left map) and sustained monomorphic reentrant ventricular tachycardia (VT, lower right map). The ac- tivation maps were obtained from a canin e experiment 4 days postligation of the left anterior descending artery (LAD). In this and subsequent maps, epicardial activation is displayed as if the heart were viewed from the apex located at the center of the circular map, The perimeter of the circle represents the atl'io- ventricular junction. The epicardial outline of the ischemic zone is represented by the dotted line. Acti- vation isochrones are drawn at 20 msec intervals. Arcs of functional conduction block are represented by heavy solid lines. The site of cryoprobe application is represented by the dark-shaded circle. Represen- tative surface electrocardiograms are shown in the upper right panel. Note that the site of the last 20 msec isochrone during sinus rhythm (the lightly shaded area) correlates with the critical site for prevention of initiation of reentry as well as with the critical site for termination of sustained reentrant VT. The lower right panel illustrates the orientation of myocardial fibers in the surviving ischemic epicardial layer per- pendicular to the direction of the LAD. The arrow represents the longitudinal axis of propagation of the slow common reentrant wave front during a sustained figure-0f-8 activation pattern that is oriented par- allel to the long axis of the fibers and perpendicular to the nearby LAD segment. See text for details.
e n t r a n t t achyca rd ia could be t e rmina ted . T h e ma- jor i ty of the epicardial surface of the r ight and left ventr icles was ac t iva ted within 40 msec dur ing sinus rhy thm. This cor responded to the surface QRS dura t ion of 42 msec. Mos t of the epicardial surface of the ischemic zone was also ac t iva ted within the 21 to 60 msec isochrones. However , a small pa rasep ta l area showed late ac t iva t ion (the 61 to 80 msec isochrone identif ied by the lightly-shaded zone). In this exper- imen t a sus ta ined m o n o m o r p h i c t achycard ia with a
posit ive QRS configurat ion in lead I I was reproduc- ibly in i t ia ted by a single p r e m a t u r e s t imulus ($1S2 protocol) appl ied to the r ight ventr icular outflow tract . T h e act ivat ion m a p of the $2 s t imula ted bea t (Fig. 1, upper right panel) showed the deve lopmen t of a long cont inuous arc of funct ional conduct ion block ( represented by the heavy solid line) within the border of the ischemic zone. T h e act ivat ion wave f ront c i rculated a round bo th ends of the arc of block and coalesced a t the 100 msec isochrone. T h e com-
Volume 119 Number 5 SinLts versus reentrant activation patterns 1017
S
t.
T V
100 m s e c
/f II l/ II II 1
S 3 " C O N T " 40 " .
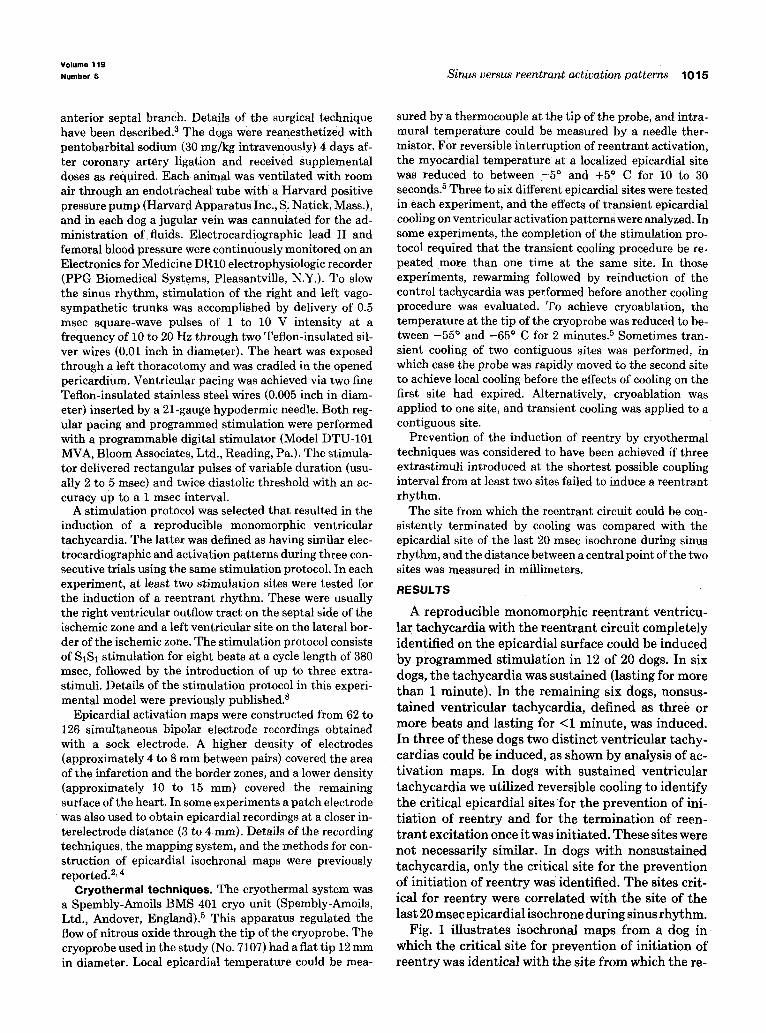
Fig. 2. Rec•rdings •btained fr•m an experiment in which the site •f latest activati•n during sinus rhythym (the lightly shaded area) did not corresponded to the critical site for prevention of initiation of reentry (the map in the lower left panel) nor to the critical site for termination of sustained reentrant ventricular tachycardia (the map in the lower right panel). Both sites are represented by a dark-shaded circle. See text for details. Representative surface electrocardiograms are shown on the upper left panel.
mon wave front advanced within the arc of block be- fore reactivating an area on the other side of the arc at the 180 msec isochrone to initiate the first reen- trant cycle. During sustained tachycardia (Fig. 1, lower middle panel) , the reentrant circuit had a fig- ure-of-8 activation pattern in the form of clockwise and counterclockwise wave fronts around two sepa- rate arcs of functional conduction block. The two wave fronts joined into a common wave front that conducted slowly between the two arcs of block. In the majority of experiments, the sites of the two arcs of block during the reentrant tachycardia were dif- ferent from the arc of block during initiation of reen- try by premature stimulation. In Fig. 1, however, the basal arc of block during sustained ventricular ta- chycardia was close to the basal extension of the arc during initiation of reentry. The direction of propa- gation of the common reentrant wave front during sustained reentrant activation was perpendicular to
the left anterior descending artery and parallel to the direction of myocardial fibers in the surviving epi- cardial layer (see Fig. 1, lower right panel) . In five of the six dogs in which sustained tachycardia could be induced by programmed stimulation, the QRS con- figuration was positive in lead II. In all five dogs the longitudinal axis of the common reentrant wave front during the sustained figure-of-8 activation pattern was approximately parallel to a line drawn perpen- dicular to the nearby left anterior descending artery segment (4 to 22 degrees, mean _+ SD, 9 _+ 4 degrees).
Following cyroablation, a reentrant rhythm could not be induced by a stimulation protocol utilizing up to three extrastimuli applied at the original stimula- tion site or to the left lateral border of the ischemic zone. Fig. 1 shows that the critical site for prevention of initiation of reentry (the dark-shaded circle rep- resenting the position of the cyroprobe) was within 10 mm of and partially overlapped the site of the last 20
M a y 1 9 9 0
1018 Assadi et al. American Heart Journa,
V T .... L A D
4 0 a I �9
,o:// /
. . . . . . .
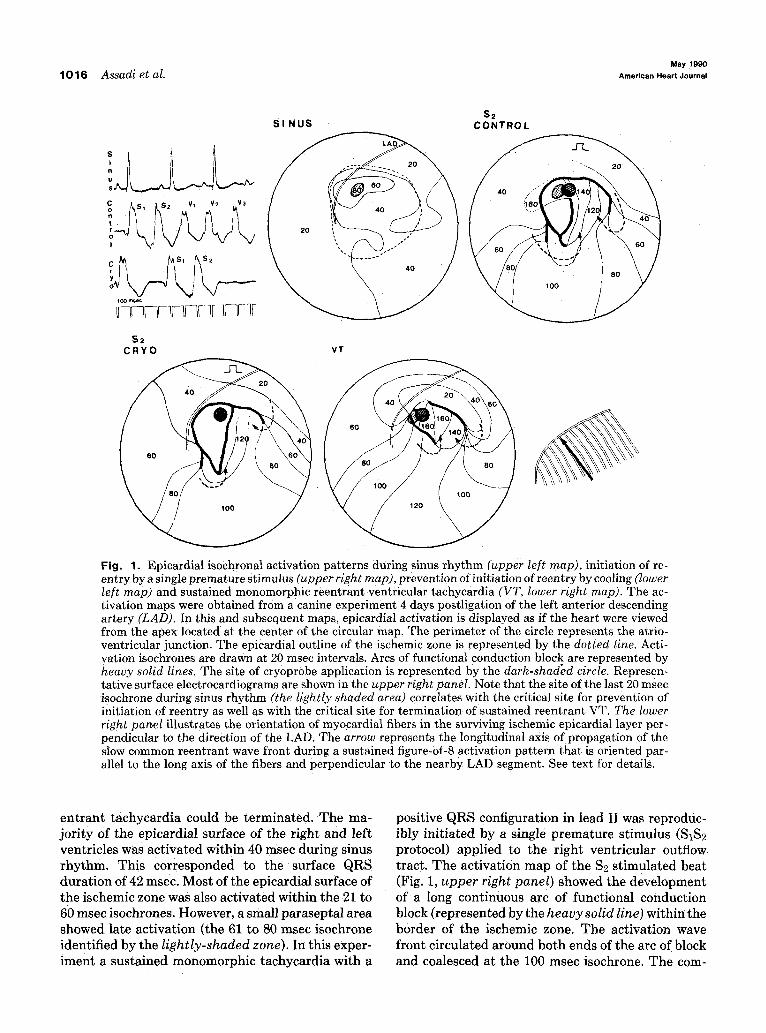
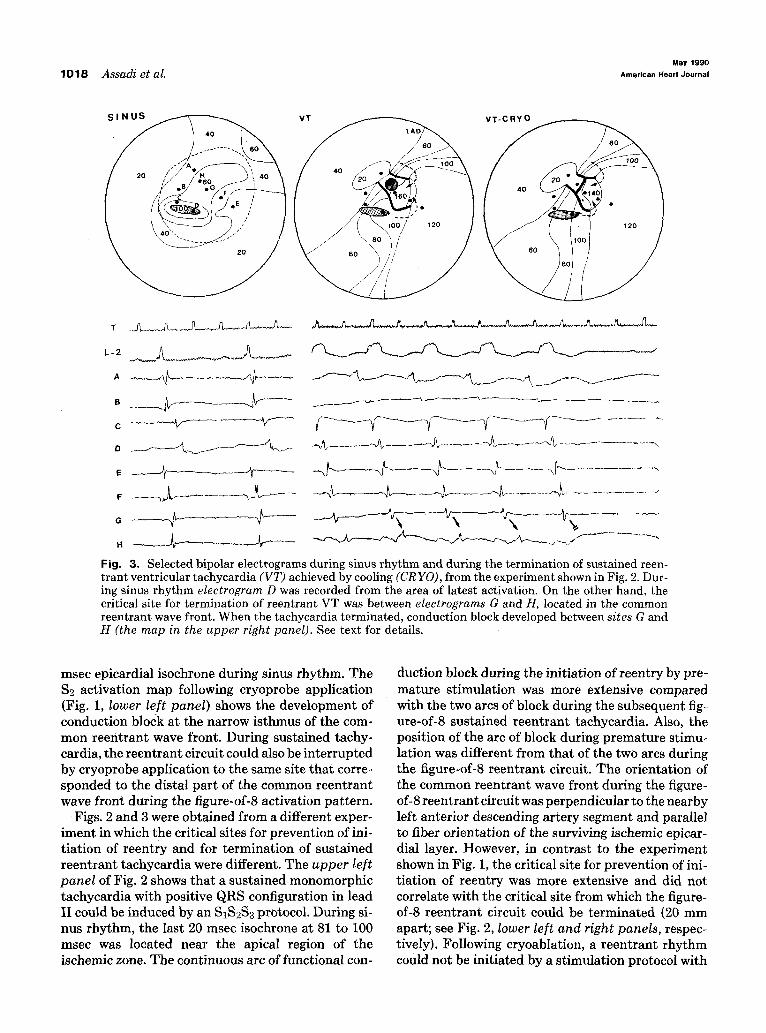
Fig. 3. Selected bipolar electrograms during sinus rhythm and during the termination of sustained reen- trant ventricular tachycardia (VT) achieved by cooling (CR YO), from the experiment shown in Fig. 2. Dur- ing sinus rhythm electrogram D was recorded from the area of latest activation. On the other hand, the critical site for termination of reentrant VT was between electrograms G and H, located in the common reentrant wave front. When the tachycardia terminated, conduction block developed between sites G and H (the map in the upper right panel). See text for details.
msec epicardial isochrone during sinus rhythm. The $2 activation map following cryoprobe application (Fig. 1, lower left panel) shows the development of conduction block at the narrow isthmus of the com- mon reentrant wave front. During sustained tachy- cardia, the reentrant circuit could also be interrupted by cryoprobe application to the same site that corre- sponded to the distal part of the common reentrant wave front during the figure-of-8 activation pattern.
Figs. 2 and 3 were obtained from a different exper- iment in which the critical sites for prevention of ini- tiation of reentry and for termination of sustained reentrant tachycardia were different. The upper left panel of Fig. 2 shows that a sustained monomorphic tachycardia with positive QRS configuration in lead II could be induced by an S1S2S3 protocol. During si- nus rhythm, the last 20 msec isochrone at 81 to 100 msec was located near the apical region of the ischemic zone. The continuous arc of functional con-
duction block during the initiation of reentry by pre- mature stimulation was more extensive compared with the two arcs of block during the subsequent fig- ure-of-8 sustained reentrant tachycardia. Also, the position of the arc of block during premature stimu- lation was different from that of the two arcs during the figure-of-8 reentrant circuit. The orientation of the common reentrant wave front during the figure- of-8 reentrant circuit was perpendicular to the nearby left anterior descending artery segment and parallel to fiber orientation of the surviving ischemic epicar- dial layer. However, in contrast to the experiment shown in Fig. 1, the critical site for prevention of ini- tiation of reentry was more extensive and did not correlate with the critical site from which the figure- of-8 reentrant circuit could be terminated (20 mm apart; see Fig. 2, lower left and right panels, respec- tively). Following cryoablation, a reentrant rhythm could not be initiated by a stimulation protocol with
Volume 119 N u m b e r 5 Sinus versus reentrant activation patterns 1019
S2-r Sa
" - - - - - I 1 2 0
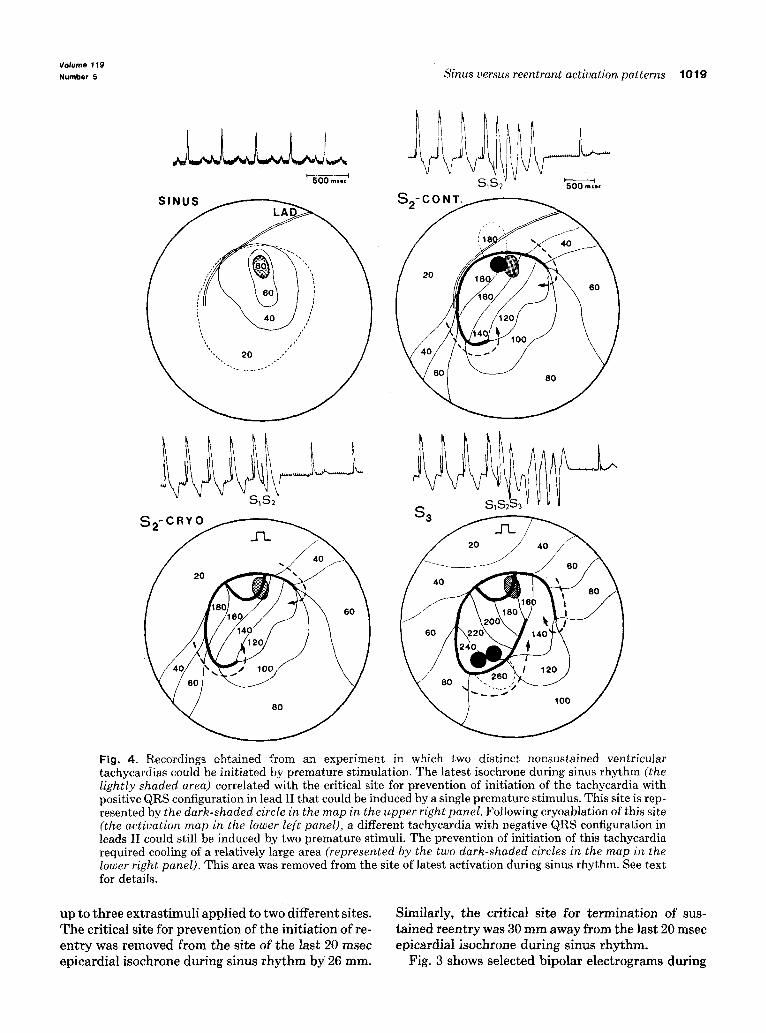
Fig, 4. Recordings obtained from an experiment in which two distinct nonsustained ventricular tachyeardias could be initiated by premature stimulation. The latest isochrone during sinus rhythm (the lightly shaded area) correlated with the critical site for prevention of initiation of the tachycardia with positive QRS configuration in lead II that could be induced by a single premature stimulus. This site is rep- resented by the dark-shaded circle in the map in the upper right panel. Following cryoablation of this site (the activation map in the lower left panel), a different tachycardia with negative QRS configuration in leads II could still be induced by two premature stimuli. The prevention of initiation of this tachycardia required cooling of a relatively large area (represented by the two dark-shaded circles in the map in the lower right panel). This area was removed from the site of latest activation during sinus rhythm. See text for details.
up to th ree ex t ras t imul i appl ied to two different sites. T h e critical site for p reven t ion of the ini t iat ion of re- en t ry was removed f rom the site of the last 20 msec epicardial isochrone dur ing sinus r h y t h m by 26 mm.
Similarly, the critical site for t e rmina t ion of sus- ta ined r een t ry was 30 m m away f rom the last 20 msec epicardial isochrone dur ing sinus rhy thm.
Fig. 3 shows selected b ipolar e lec t rograms during

May 1990 1 0 2 0 Assadi et al. American Heart Journal
S 1 21 j
l ~ ~ ~ ~ f
S 2
S I N U S 1
LAD
40
S I N U S 2
s J ' " 40
2O
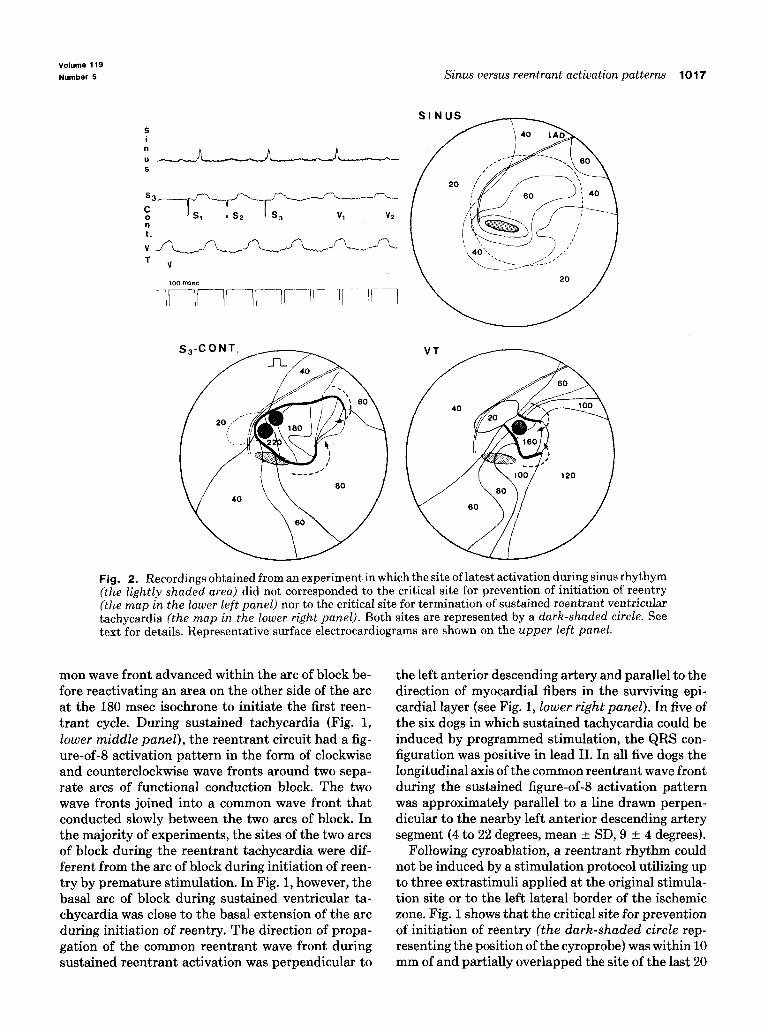
Fig. 5. Recordings obtained from a different experiment showing an area with 2:1 conduction block dur- ing sinus rhythm (see the selected electrograms in the upper left panel and the two sinus maps labeled 1 and 2 in the lower two panels). A late activation isochrone at 120 to 140 msec occurred during every other sinus beat (represented by the lightly shaded area in Sinus 1 map). This area was contiguous to an area where the infarction extended to the epicardial surface (represented by the striped area). The critical site for prevention of initiation of reentry (represented by the dark-shaded circle in the $2 map in the upper right panel) did not correlate with the sites of conduction delay and block during sinus rhythm. See text for details.
sinus rhythm and during the termination of reen- t rant tachycardia by cooling. During sinus rhythm, electrogram D was recorded from the area of the last 20 msec isochrone at the apical region of the ischemic zone. The electrogram showed a multiphasic "frac- t ionated" configuration and had a duration of 55 msec. The moment of activation at this site was con- sidered to be synchronous with the initial large biphasic deflection that was recorded 99 msec from the onset of epicardial activation. The smaller am- plitude terminal deflections may have reflected elec- trotonic activity of a slower and more complicated local conduction pat tern than is represented in the isochronal map. The critical site for termination of the reentrant circuit was between electrograms G and H, located in the common reentrant wave front in the left paraseptal region of the ischemic zone. Before termination of the tachycardia, an incremen- tal beat-to-beat increase of the conduction time be- tween sites G and H occurred and was associated with
equal increases in the tachycardia cycle length. When conduction block developed between the two sites, the reentrant circuit was terminated and electrogram H showed an electrotonic potential but no local acti- vation potential. This was represented on the iso- chronal map by an arc of conduction block that joined the two separate arcs of the figure-of-8 reentrant cir- cuit into a continuous line of conduction block (Fig. 3, upper right panel).
In three experiments, the cryothermal lesion pre- vented the initiation of a reproducible reentrant ventricular tachycardia when the control stimulation protocol was tested. However~ a more aggressive stimulation protocol induced a different reentrant tachycardia. This is shown in Fig. 4. During sinus rhythm, the last 20 msec epicardial isochrone at 61 to 80 msec was located at the left paraseptal region of the ischemic zone (Fig. 4, upper left panel). During ventricular pacing, a single premature stimulus ($2) reproducibly induced a nonsustained tachycardia

Volume 119
Number 5 Sinus versus reentrant activation patterns 1021
with positive QRS configuration in lead II. The ini- tiation of reentry by the control $1S2 protocol could be prevented by cryoablation of the distal part of the common reentrant wave front prior to reexcitation, which created complete conduction block around the site of the cryoprobe (Fig. 4, lower left panel). This site was within 12 mm of and partially overlapped the site of the last 20 msec epicardial isochrone during sinus rhythm (Fig. 4, upper right panel). However, following cryoablation of this site, the introduction of a second premature stimulus ($3) could reproduci~ly initiate a different nonsustained tachycardia with negative QRS configuration in lead II. The $3 stim- ulus resulted in a longer arc of conduction block and the common reentrant wave front continued to con- duct slowly past the area of original cryoablation to- ward the apical region of the ischemic zone before reactivating myocardial sites on the other side of the arc of block to initiate reentry (Fig. 4, lower right panel). The slower conduction of the reentrant wave front and the longer pathway explained the longer coupling interval of the first reentrant beat with neg- ative QRS (270 msec) compared with the first reen- t rant beat with positive QRS (170 msec). The initi- ation of the new reentrant circuit could only be interrupted when cooling was applied to a relatively large area (12 • 24 mm) of the common reentrant wave-front immediately proximal to the reactivation site (Fig. 4, the two shaded circles in the lower right panel). This site was obviously far removed from the site of the last 20 msec epicardial isochrone during sinus rhythm (56 mm apart).
In three experiments the site of the last 20 msec epicardial isochrone during sinus rhythm repre- sented areas showing Wenckebach period or 2:1 con- duction block. In two of the three experiments these sites were contiguous to areas where the infarction extended to the epicardial surface. This is shown in Fig. 5. In this experiment there was an apical area where the infarction extended to the epicardial sur- face (the striped zone). Contiguous with this zone there was an area of surviving ischemic epicardium that showed 2:1 conduction block during sinus tachycardia (represented by electrograms B and C in the upper left panel). The activation maps during two consecutive sinus beats are shown in the lower panel. During every other sinus beat, this area was activated 100 to 140 msec from the onset of epicardial activation. Analysis of electrogram A recorded from outside this area and electrogram B from inside the area shows that both have "split potentials." The initial deflection represented an electrotonic poten- tial and the second represented an activation potential. 4 During conduction block, the electrotonic deflection was only recorded at site B. In this exper-
iment, a single premature stimulus reproducibly in- duced a nonsustained monomorphic tachycardia. The activation map of $2 is shown on the upper right panel and illustrates the development of a continu- ous arc of functional conduction block inside the epicardial border of the ischemic zone. A slow com- mon reentrant wave front conducted between the two limbs of the arc of block before activating an epicar- dial site on the septal border of the ischemic zone to initiate reentry. The critical site from which the ini- tiation of reentry could be prevented (the dark- shaded circle) was 26 mm away from the last 20 msec epicardial isochrone during sinus rhythm (the light- ly-shaded area). In fact, the site of the last 20 msec epicardial isochrone during sinus rhythm was part of a dissociated zone that did not participate in epicar- dial activation during reentry.
Table I summarizes the results from all experi- ments. In the 12 experiments we defined 15 critical sites for the prevention of initiation of reentry (in three experiments there were two sites corresponding to two distinct reentrant circuits) as well as six sites for termination of sustained figure-of-8 reentry. A total of 20 different sites were available for analysis (in one experiment, the sites for either prevention of initiation or termination of reentry were similar). The mean distance between sites critical for reentry and the last 20 msec epicardial isochrone during si- nus rhythm was 26.7 _+ 13.3 mm. Five sites (25%) were within a 12 mm distance, which corresponded to the diameter of the cryprobe. Nine sites (45 % ) were within a 24 mm distance (twice the diameter of the cryoprobe), while 11 sites (55%) were separated by more than 24 mm.
DISCUSSION
The present study is the first to correlate sites of late epicardial activation during sinus rhythm with sites critical for initiation and sustentation of reen- trant ventricular tachycardia. The present protocol has not tested directly the effects of a cryoablative lesion of the site of the late epicardial isochrone dur- ing sinus rhythm on the prevention of initiation or the termination of reentrant ventricular tachycardia. However, the area of the cryoablative lesion has been tested before in the same experimental model and was shown to only extend slightly beyond the area directly in contact with the cryoprobe. ~ This would allow reasonable conclusions to be drawn from the present study. There is no standard definition of how close the site of latest activation during sinus rhythm and the critical site for initiation and sustentation of reentrant ventricular tachycardia should be for a good correlation. If mapping of delayed activation during sinus rhythm is used to guide therapy of re-

May 1990 1022 Assadi et al. American Heart Journal
Table I . Correlation of the site of latest isochrone during sinus rhythm with the critical sites during reentrant excitation
Last 20 msec Experiment isochrone during
No. sinus rhy thm
Distance in mm between site of prevention of init iation o[ reentry and
last 20 msec isochrone during sinus rhythm
Distance in mm between site of termination of sustained reentry and
last 20 msec isochrone during sinus rhy thm
1 6 0 - 8 0 m s e c 10 10
2 6 0 - 8 0 m s e c 8 16 3 8 0 - 1 0 0 m s e c 3 0 26
4 8 0 - 1 0 0 m s e c 12 22
5 1 0 0 - 1 2 0 m s e c 30 25
6 1 0 0 - 1 2 0 m s e c 36 40
7* 6 0 - 8 0 m s e c 12 - - 56
8* 8 0 - 1 0 0 m s e c 14 - - 47
9* lO0-120msec 18 - - 42
10 1 2 0 - 1 4 0 m s e c 27 - -
11 1 2 0 - 1 4 0 m s e c 25 - -
12 1 4 0 - 1 6 0 m s e c 38 - -
*Two dist inct reen t ran t circuits could be init iated by p rematu re st imulation.
entrant tachycardia, a good correlation will depend on the anticipated size of the surgical or ablative le- sion. The latter will depend on the surgical or abla- tive procedure that is being contemplated. In the present study, a surgical or cryoablative lesion of a 24 by 24 mm area centered around the site of most de- layed activation during sinus rhythm probably would have resulted in successful prevention of 45 % of re- entrant tachycardias. A larger lesion may have suc- ceeded in a few more cases. However, a discrete lesion of 12 by 12 mm, corresponding to the diameter of the flat tip of the cryoprobe utilized in the present experiments, would have succeeded in only 25 % of reentrant tachycardias.
Electrophysiologic basis of delayed activation during sinus and reentrant rhythms. Our finding that myocar- dial sites with the most delayed activation during si- nus rhythm did not usually correspond to the critical sites during reentrant excitation was not unexpected, given the different electrophysiologic basis for the activation pattern of these rhythms. The critical sites of delayed activation during reentrant excitation are initimately related to the location and extent of the arcs of functional conduction block. This is not the case during sinus activation. The epicardial activa- tion pattern during sinus rhythm in the present ex- perimental model was characterized by concentric isochrones of delayed activation in the ischemic epi- cardial zone, with the latest activation usually in the center of the ischemic zone. This is explained by the anatomic characteristics of the infarction, in which the surviving epicardial layer is activated during si-
nus rhythm from the border of the ischemic zone. In a previous study, 9 we have shown that the epicardial ischemic layer has a characteristic pattern of refrac- tory distribution in the form of concentric rings of isorefractoriness that increase in duration from the border zone to the center of the ischemic zone. How- ever, no electrophysiologic correlation could be made between the pattern of delayed activation during a relatively slow basic rhythm and the pattern of refractory distribution. By contrast, a spatially non- uniform refractory distribution does correlate with the sites of functional unidirectional conduction block during premature stimulation. The activation pattern during the initiation of reentry induced by premature stimulation was explained by the charac- teristic refractory pattern, since the arc of functional unidirectional conduction block has been found to occur along the gradient of refractoriness. 9 The crit- ical zone, from where the initiation of reentry could be prevented or sustained reentry could be termi- nated, was dependent on the position of the func- tional arcs of block in the two situations. Since the sites of the arcs of block were different during the initiation of reentry and during sustained reentry, it was not surprising that the critical zones were also different in the two situations. Our findings that the two arcs of functional conduction block during sus- tained reentry were usually oriented parallel to the direction of myocardial fibers in the surviving epi- cardial layer is similar to the findings of previously published reports. 1~ 11 However, whether these lines of dissociated conduction represent conduction

Volume 119
Number 5 Sinus versus reentrant activation pat terns 1023
block 12 or pseudoblock due to very slow conduction across the fibers 11 has not been resolved.
In some experiments, myocardial zones with func- tional conduction block (Wenckebach period or 2:1 conduction) were seen during sinus rhythm. A dy- namic Wenckebach-like conduction pattern during sinus rhythm was described in association with the spontaneous onset of reentrant rhythm, i.e., reen- trant rhythms not induced by premature stimula- t ionJ 3 The presence of marked lengthening of re- fractoriness in a spatially nonuniform pattern ex- plains the occurrence of functional conduction block at the relatively long cycle lengths associated with si- nus rhythmJ 3 In fact, in those experiments, prema- ture stimulation consistently resulted in a more ex- tensive functional arc of block at sites distant from the sites of block during sinus rhythm (see Fig. 5). In other words, the sites of functional conduction block during sinus rhythm did not participate in the reen- trant excitation pattern induced by premature stim- ulation.
Value of abnormal electrograms during sinus rhythm. Several studies 14-1s have correlated the sites from which abnormal bipolar electrograms were recorded during sinus rhythm with the sites of delayed activa- tion during possible reentrant tachycardia or with the sites deemed critical during surgical therapy of the tachycardia. A correlation between the sites was found by some authors 14, is but not by othersJ 5"17 Abnormal electrograms during sinus rhythm in- cluded delayed, split, or fractionated potentials. These electrograms were thought to represent ab- normal myocardial conduction and thus the sites from which the electrograms were recorded could somehow be critical for the initiation and sustenta- tion of reentrant tachycardia. However, the electro- physiologic basis of these electrograms was not clear. In the present study, delayed electrograms that were inscribed in the ST-T segment of the surface QRS complex represented concentric isochrones of de- layed activation of the ischemic epicardial zone. Split or double potentials were seen close to sites of func- tional conduction block and sometimes represented a large electrotonic potential synchronous with the surface QRS and a delayed activation potential (see Fig. 5). Fractionated electrograms were uncommonly seen during sinus rhythm in the 4-day-old canine in- farct model and may have represented the superim- position of more than one activation or electrotonic potential from a markedly disorganized activation pattern (see Fig. 3). Double potentials and fraction- ated electrograms were recorded from isolated epi- cardial preparations of a 2-month-old canine infarct and were found to correlate with asynchronous action
potential upstrokes of normal surviving myocardial fibers that had been uncoupled by intervening fi- brous tissue. 19
How relevant is the animal model? The relevance of the present study depends on the appropriateness of the canine experimental model of subacute infarc- tion, in which reentrant tachycardia is usually in- duced by premature stimulation compared with clinical sustained ventricular tachycardia. The latter commonly occurs spontaneously in the chronic postinfarction heart where areas of extensive fibrosis and disorganized myocardial fibers are frequently present. Fractionated and split electrograms are commonly recorded from these areas, 17 similar to the ones recorded from chronic canine infarction preparations. 19 It should be emphasized, however, that reentrant excitation has not been definitely shown to occur in areas of extensive fibrosis with dis- organized, isolated, and uncoupled myocardial bun- dles in which very slow and possibly discontinuous conduction could be demonstrated. This is not sur- prising, since very slow and circuitous conduction is probably not tantamount to successful reentrant ex- citation compared with the presence of a critical zone of functional unidirectional conduction block. Areas of very slow conduction during a basic relatively slow cardiac rhythm may not participate in reentrant ex- citation induced by premature stimulation (see Fig. 5). Therefore the significance of these areas in the initiation and/or sustentation of clinical reentrant tachycardia is doubtful. On the other hand, a figure- of-8 reentrant activation pattern similar to the one originally described in the present canine model was recently found during clinical reentrant ventricular tachycardia. 2~ Although the reentrant circuit was usually localized in the surviving subendocardial myocardial layer rather than in the subepicardial re- gion, as is the case with the experimental model, this could be related to the difference in the anatomic characteristics of both infarctions rather than in the electrophysiologic substrate. Further, there is some evidence that a figure-of-8 reentrant tachycardia in clinical subjects could also be terminated from a crit- ical site in the slow common reentrant wavefront. 21
In conclusion, the present study has demonstrated that late activation zones during sinus rhythm in the postinfarction heart may not have electrophysiologic correlation to activation patterns during both initia- tion and sustentation of reentrant tachycardia. In a majority of the experiments, neither mapping of si- nus activation nor the localization of sites of abnor- mal electrograms during sinus rhythm were found to identify the critical sites from which reentrant exci- tation could be prevented or terminated.
May 1990 1 0 2 4 Assadi et al. American Heart Journal
REFERENCES
1. E1-Sherif N, Smith A, Evans K. Canine ventricular arrhyth- mias in the late myocardial infarction period: 8. epicardial mapping of reentrant circuits. Circ Res 1981;49:255-65.
2. EI-Sherif N, Mehra R, Gough WB, Zeiler RH. Ventricular ac- tivation pattern of spontaneous and induced ventricu]ar rhythms in canine one-day-old myocardial infarction. Evi- dence for focal and reentrant mechanisms. Circ Res 1982; 51:152-66.
3. Wit AL, Allessie MA, Bonke FIM, Lammers W, Smeets J, Fenoglio JJ Jr. Electrophysiologic mapping to determine the mechanism of experimental ventricular tachycardia initiated by premature impulses: experimental approach and initial re- sults demonstrating reentrant excitation. Am J Cardiol 1982; 49:166-85.
4. Mehra R, Zeiler RH, Gough WB, E1-Sherif N. Reentrant ven- tricular arrhythmias in the late myocardial infarction period. 9. Electrophysiologic-anatomic correlation of reentrant cir- cuits. Circulation 1983;67:11-24.
5. EI-Sherif N, Mehra R, Gough WB, Zeiler RH. Ventricular ar- rhythmias in the late myocardial infarction period. Interrup- tion of reentrant circuits by cryothermal techniques. Circula- tion 1983;68:644-56.
6. Gessman L, Agarwal JB, Endo T, Helfant RM. Localization and mechanism of ventricular tachycardia by ice mapping one -week after the onset of myocardial infarction in dogs. Cir- culation 1983;68:657-66.
7. Assadi M, Gough WB. Correlation of isochronal activation maps of sinus and reentrant ventricular rhythms in canine in- farction IAbstract]. Circulation 1986;74:II-t17.
8. EI-Sherif N, Mehra K, Gough WB, Zeiler RH. Reentrant ven- tricular arrhythmias in the late myocardial infarction period. 11. Burst pacing versus multiple premature stimulation. J Am Coll Cardiol 1984;4:295-304.
9. Gough WB, Mehra R, Restivo M, Zeiler RH, E1-Sherif N. Re- entrant ventricular arrhythmias in the late myocardial infarc- tion period. 13. Correlation of activation and refractory maps. Circ Res 1985;57:432-42.
10. Cardinal R, Vermeuler M, Shenasa M, Roberge F, Page P, Helle F, Savard P. Anisotropie conduction and functional dis- sociation of ischemic tissue during reentrant ventricular tachycardia in canine myocardial infarction. Circulation 1988;77:1162-76.
11. Dillon SM, Allessie MA, Ursell PC, Wit AL. Influences of an-
isotropic tissue structure on reentrant circuits in the epicardial border zone of subacute canine infarcts. Circ Res 1988;63:182- 206.
12. E1-Sherif N, Restivo M, Williams C, Henkin R, Gough WB. Sustained reentrant activation orients around arcs of abrupt functional conduction block in the canine post infarction heart [Abstract]. J Am Coll Cardiol 1989;13:128A.
13. E1-Sherif N, Gough WB, Zeiler RH, Hariman R. Reentrant ventricular arrhythmias in the late myocardial infarction pe- riod. 12. Spontaneous versus induced reentry and intramural versus epicardial circuits. J Am Coil Cardiol 1985;6:124-32.
14. Fontaine G, Guiraudon G, Frank R, Fillette F, Tonet J, Gros- gogeat Y. Correlations between latest delayed potentials in si- nus rhythm and earliest activation during chronic ventricular tachycardia. In: Bricks W, Loogen F, Schuth HD, Seipel L, eds. Medical and surgical management of tachyarrhythmias. New York: Springer-Verlag, 1980:138-49.
15. Klein H, Karp RB, Kouchoukas NT, Zorn GL, James TN, Waldo AL. Intraoperative electrophysiologic mapping of the ventricles during sinus rhythm in patients with a previous myocardial infarction. Identification of the electrophysiologic substrate of ventricular arrhythmias. Circulation 1982;66:847- 53.
16. Cassidy DM, Vassallo JA, Buxton AE, Doherty JV, Marchil- inski FE, Josephson ME. The value of catheter mapping dur- ing sinus rhythm to localize the site of origin of ventricular ta- chycardia. Circulation 1984;69:1103-10.
17. Kienzle MG, Miller J, Falcone RA, Harken A, Josephson ME. Intraoperative endocardial mapping during sinus rhythm: re- lationship to site of origin of ventricular tachycardia. Circula- tion 1984;70:957-65.
18. Weiner I, Mindich B, Pitchon R. Fragmented endocardial electrical activity in patients with ventricular tachycardia: a new guide to surgical therapy. AM HEART J 1984;107:86-96.
19. Gardner PI, Ursell PC, Fenoglio JJ Jr, Wit AL. Electrophys- iologic and anatomic basis for fractionated electrograms recorded from healed myocardial infarcts. Circulation 1985;72:596-611.
20. Harris L, Downar E, Mickleborough L, Shaikh N, Parson I, Chen T, Gray G. Activation sequence of ventricular tachycar- dia: endocardial and epicardial mapping studies in the human ventricle. J Am Coll Cardiol 1987;10:1040-7.
21. Downar E, Mickleborough L, Harris L, Parson I. Intraopera- tive electrical ablation of ventricular arrhythmias: a "closed heart" procedure. J Am Coll Cardiol 1987;10:1048-56.