respiratory therapists in leadership roles csrt 2o12, vancouver, bc
TRANSCRIPT

1 1
Respiratory Therapists in Non-Traditional Leadership Roles Dan Belford RRT. MEd, MBA (c)
2 2
Leadership
• There are almost as many definitions of leadership as there are persons who have attempted to define the concept.
• Google search for leadership = about 496,000,000 results.
• No one leadership definition is correct.

3
Adaptive Leadership
• Our personal leadership definition can be very different from other’s leadership definition.
• “Leadership is the ability to step outside the culture... to start evolutionary change processes that are more adaptive” (Schein, 1992, p. 3).

4 4
Leading Change
• There are some theorists that argue that leading change is the fundamental role of a leader everything else is secondary.
• “Management is efficiency in climbing the ladder of success; leadership determines whether the ladder is leaning against the right wall." — Stephen R. Covey

5
Leadership’s Traits
• Psychologists have not sorted out which traits define leaders or whether leadership exists outside of specific situations.
• Culture. • Context. • Process. • Outcome.
6 6
What we know…. • We know with absolute certainty that a
handful of people have changed millions of lives and reshaped the world.

7
8 8
What does it take to become a Respiratory Therapist?
• Strong back ground in math and science. • Good physical and Mental Health. • Ability to work under intense pressure. • Stamina. • High degree of integrity. • Tact and discretion. • Critical Thinking Skills. • Teamwork and leadership skills.
9 9
What does it take to become a Leader?
• If knowledge is possessing facts, and thinking is the application of knowledge “critical thinking” in the simplest of terms is the application of knowledge in more complex ways.
10
What does that mean…
• Critical thinkers strive to be clear, accurate, precise, logical, complete, significant and fair when they listen, speak, read and write.
• Critical thinkers think deeply and broadly. • Their thinking is adequate for their
intended purpose (Paul, Scriven, Norris & Ennis).
11 11
Critical Thinking Skills
• The six core critical thinking skills are: • Analysis. • Inference. • Interpretation. • Explanation. • Self-regulation. • Evaluation.
12 12
Decisions
• Leaders deal with complex problems that require complex solutions.
• Leaders who can think critically will be more effective.
• Evidence suggests that formal classroom instruction rarely leads to critical thinking (Lizzio & Wilson, 2207)

13 13
Self-Reflection
• Without self-reflection it is difficult for students to develop critical thinking skills.
• Utilizing context based knowledge with real world inputs demonstrate increased critical thinking compared to those who experience traditional classroom lectures (Tiwari, 2006).
14 14
What Organizations want… • Organizations are
seeking well trained individuals that have technical skills and have critical thinking skills to be effective in a constantly changing environment.

15 15
Patient Care
• Critical thinking is required during clinical simulations and during clinical placements.
• Nowhere is critical thinking more impetrative than in the life and death world of critical care.
• Without critical thinking patients can be mismanaged, leading to adverse outcomes.
16 16
Failure to Critically Think
• In the business setting, failure to think critically can result in missed opportunities, faulty decisions, inefficiencies, and ineffectiveness.
• “The downfall of many organizations can be tied to faulty leadership” (Carroll & Mul, 2008, Spreier 2006).
17
Research in Motion
• RIM’s leadership did not respond more quickly to a fast-changing market.
• RIM’s technology had transformed it into a global technology leader over the past decade.
• Assumed the BlackBerry technology would be enough to keep it at the top indefinitely.
18 18
Decision Making
• How leaders make decisions impacts the quality of their decisions.
• For some of us the most challenging leadership development opportunities arise when moving from being subject matter experts to assuming leadership positions.
19 19
From Clinical Profession to Leader
• It can be challenging because in the previous role a strong emphasis is placed on data and logical reasoning.
• We need to learn soft skills leaders require to manage people and teamwork.
• Such as showing empathy (emotional intelligence) and listening.
• Typically not part of our education or training • And these skills do not necessarily reflect our
natural preferences.
20 20
The Transition
• There are several factors for success: • Be willing to take risks. • Having mentors. • Being part of a support network. • Commitment to life long learning. • Using failure as a learning experience.
21 21
Career Path Progression
• ACLS Instructor • Critical Care Instructor. • Regional Charge RRT. • OPSEU President. • Interprofessional Practice Leader. • Clinical Manager: Emergency Department
and a Urgent Care Center. • Clinical Manger: Level 3 ICU, Respiratory
Therapy Department and a Telemetry Unit.
22 22
Organizational Challenges
• Organizations face key challenges as they try to transform and evolve.
• The ability to lead change has become a skill as organizations, are required to transform in order to meet higher expectations of success.

23 23
Organizational Culture
• In healthcare effective leaders create fertile, supportive environments for creative thought and can challenge assumptions about how particular branches of healthcare are delivered.
24 24
Managing Change
• Organizational culture is an important factor affecting strategy execution.
• A recent Wharton School of Business Study assesses that managing change is the single most important requisite for execution for success.

25 25
Leading Organizational Cultural Change
• To many leaders, the ability to change is synonymous with the ability to manage organizational cultural change.
• Because culture is enduring and difficult to change, strategy formulation must consider culture.

26 26
Cultural Leadership • Leadership is an important component in
building and maintaining organizational culture • Cultural leadership performs 3 important tasks: • It sustains the mission, creates a distinctive role,
and establishes the basic commitments of the organization.
• It embodies its purpose by actually implementing its mission and in the process gives shape to its culture.
• It maintains organizational values and identity.
27 27
A Case Study in Organizational Cultural Change
• Implementation of Interprofessional Care (IPC) within a multi-site community based hospital in Ontario.
• A collaborative, team-based approach that enables improved patient care.
• IPC leverages individual and team capacity to optimize health outcomes.
28 28
Why IPC
• A non- controlled study of the impact of a medical emergency team in a 300 bed hospital found that the incidence of unexpected cardiac arrest declined by 50%>( Buist,M.D., et al. Effects of a medical emergency team on the reduction of incidence of mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ 2002;324(7334):387-390.
29 29
Deliverable:
• Development of a formal strategic plan for interprofessional care that will encompass interprofessional models of care to support collaborative practice among care providers.
30 30
Timeline 2008-2009
• All levels of administration, union leadership,
and various disciplines representing frontline health care professionals were engaged.
• Focus groups were conducted with respect to Interprofessional care with over 140 participants.
• Organizational “snap shot” of Interprofessional care
31 31
Predominant Themes: Barriers
• Resistance to change/fear factor. – Hierarchies
• medical model dominance. – Physician & Nurse driven organization. – Turf wars & silos/territorialism.
• Individual groups vs. collective good.
32 32
Predominant Themes:
Enablers • Provincial and federal support and funding are now
available – Time and resources available.
• MOH, Professional Colleges, Government all
working together.
• Strong Senior leadership endorsement. – Commitment from organization and individuals –
Dedicated Project Lead
– Right people are at the table in Steering Committee, Focus Groups, Education, working groups.
33 33
All Health Professionals Share Similar Standards of Practice
• Client Centered Care. • Interdisciplinary Collaboration. • Accountability. • Practice knowledge - assess, plan, implement,
and evaluate. • Applied Knowledge. • Code of Ethics. • Communication. • Continuing Competence.
Belford & Matthews
34 34
Sustainability
• The core strategy for sustainability is your desire to create and commitment to an organization or a business unit, or a product or service or even a process that will endure long after you are gone (Werbach, 2009, p.82)
35 35
Sustainability Reporting • The Global Reporting Initiative de facto global standard
for sustainability reporting. • Key organizational values, policies, strategies,
operational management systems, goals, and targets (e.g. employees, shareholders, and suppliers)
• The interests and the expectations of stakeholders specifically invested in the success of the organization.
• Significant risks to the organization. • Critical success factors for organizational success. • The core competencies of the organization and how
they can or could contribute to sustainable development (Werbach, 2009, p.114).

36 36
Interprofessional Core Competencies
I. Interpersonal and Communication Skills
II. Patient/Client & Family Centred Care
III. Collaborative Practice: A. Collaborative Decision-Making B. Roles and Responsibilities C. Team Functioning D. Continuous Quality Improvement
37 37
Clinical Simulation

38 38
Education
• Focus on Interprofessional Core Competencies, not technical performance.
• 180 Participants – RN, RPN, RRT, HCA, Pastoral Care, Social Work, Administrators
• Realism of scenarios. • Debriefing led by Clinical Educators.

39 39
Evaluation • Informal evaluation amongst participants
as the program progressed good word-of-mouth.
• Formal evaluation (qualitative and quantitative) resulting in a formal study.
40 40
Application of Interprofessional Practice Model
• Application of an interprofessional practice
model in the ED and ICU during clinical manager roles.
41 41
Emergency Manager Role
• Introduced Interprofessional practice model within the Emergency Department.
• Within a “See and Treat” area. • Team composed of MD, Nurse Practioner,
Register Nurse, Registered Practical Nurse. • Ministry funded “Pay for Results” Program • Goal was to decrease CTAS 3 waiting time by
improving provider to be seen times.
42 42
Scope of Practice
• 2 MDs coverage 24/7. • Introduced Nurse Practioner Role to treat
patients within ED: CTAS , 3, 4, and 5. • Registered Nurse: introduced 27 medical
directives to implement care at Triage. • Registered Practical Nurse: ACLS Course,
IV insertion, Pediatric clinical up grading.
43 43
Emergency Manager Role
• Created an Interprofessional team that applied LEAN methodology that results in process improvement.
• Physical redesigned the “See and Treat” area to improve patient flow.
• Provider to be seen times for CTAS 3 patients decreased from 8 hours to 1.8 hours (Ministry Bench Mark 2 hours).
44
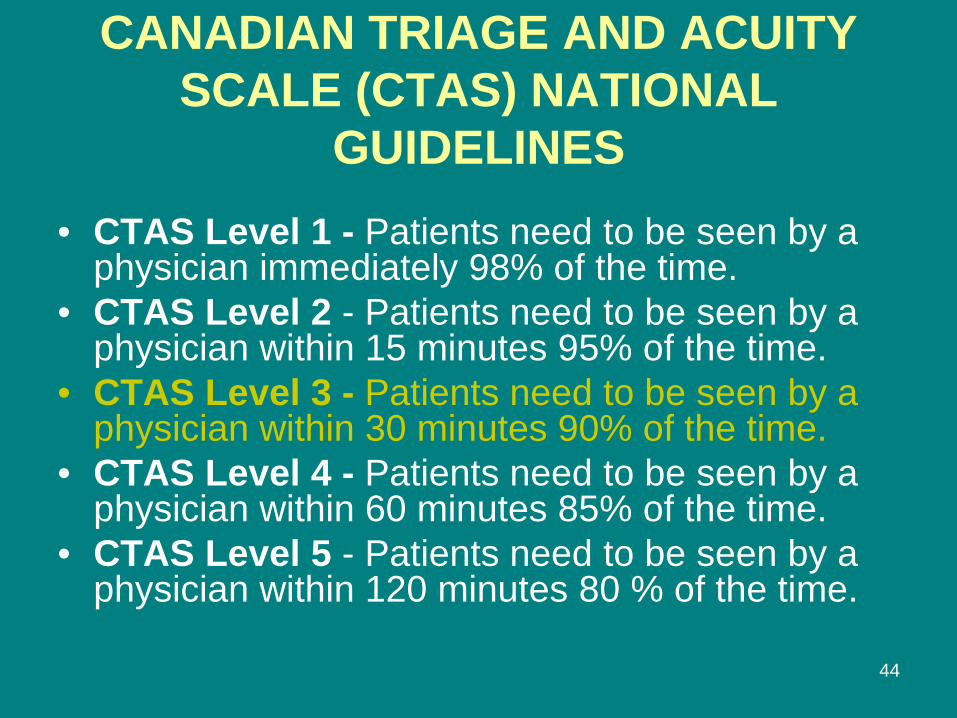
CANADIAN TRIAGE AND ACUITY SCALE (CTAS) NATIONAL
GUIDELINES
• CTAS Level 1 - Patients need to be seen by a physician immediately 98% of the time.
• CTAS Level 2 - Patients need to be seen by a physician within 15 minutes 95% of the time.
• CTAS Level 3 - Patients need to be seen by a physician within 30 minutes 90% of the time.
• CTAS Level 4 - Patients need to be seen by a physician within 60 minutes 85% of the time.
• CTAS Level 5 - Patients need to be seen by a physician within 120 minutes 80 % of the time.
45
CTAS 3
• Level 3 - Urgent • Could potentially progress to a serious problem. • Can be associated with significant discomfort • Can affect activities of daily living. • Conditions: moderate trauma, asthma, GI bleed,
vaginal,bleeding and pregnancy, acute psychosis and/or suicidal thoughts and acute pain.

46 46
Urgent Care Center • Conversion of a 30,000 visit per year Emergency
Department into an Urgent Care Center. • Redirection of CTAS 1,2, and 3 to a Full Service
Emergency. • First Urgent Care Center in Ontario to accept
Ambulances (CTAS 4 and 5). • Introduction a RN/RPN collaborative practice
model. • Increased UCC visits and improved patient/client
satisfaction results.

47 47
Results
• All healthcare providers working to full scope of practice.
• Decrease CTAS 3 “provider to be seen times” from 8 hours to 1.8 hours ( below Ministry bench mark of 2 hours)..
• Improved retention and recruitment of staff.
48 48
ICU Manager Role • Introduced Unit Council/Shared governance
model. • Unit Council promotes staff empowerment to
participate in excellent patient client centered care and advancing professional practice.
• Able to retain and recruit staff long standing Full time vacancies .
• Improved Infection Control practices utilizing a standard work tool developed during a Nursing Clinical Practice Fellowship.
49
Organizational Restructuring…
50 50
Giving back to the Profession! • Manager Cardio Respiratory, Neurodiagnostics,
and Sleep Lab • 115 staff composed of RRTs, RNs, Echo
Technologists, Cardio Technologists, ECG Technicians.
• Reorganization of reporting structure within areas.
• Moving towards full scope of practice for all healthcare providers.
• Process of establishing RACE Team, Anesthetic Assistant role.

51 51
Being Recognized…
52 52
References • Kilminister, S., Hale, C., Lascelles, M., Morris, P., Roberts, T., Stark, P., Sowter, J.,
and Thistlewaite, J. (2004). Learning for real life: Patient-focused interprofessional workshops offer added value. Medical Education 38, 717-726
• Marlow, A., Spratt, C., and Reilly, A. (2008). Collaborative action learning: A professional development model for educational innovation in nursing. Nurse Education in Practice 8, 184-189.
• Redfern, L. (2008). The challenge of leadership, 15, pp. 1-3. Retrieved March 2.2012, from Academic Search Complete
• Shirey, M. R. (2011). Addressing strategy execution challenges to lead sustainable change. The Journal of Nursing Administration, 4, pp. 1-4. Retrieved February 12, 2012, from Academic Search Complete
• Salas, E., Wilson, K., Lazzara, E., King, H., Augenstein, J., Robinson, D., and Birnbach, D. (2008). Simulation-based training for patient safety: 10 principles that matter. Journal of Patient Safety 4(1), 3-8.
• Werbach, A. (2009). Strategy for Sustainability (1st ed.). Boston, MA: Harvard Business Press.
• Zakaria, S., Fadzialh, W., Yusoff, W., Hisham, R., & Madun, R. (2012). Leadership challenges during the change transformation process. The International Journal of Interdisciplinary Social Science, 6, pp.224-232. Retrieved, from Academic Search Complete
53 53
References • Baldoni, J. (2010). What does the organization need to do? Journal for Quality and Participation,
pp. 10-14. Retrieved March 02, 2012, from Academic Search Complete Booth, A., and Falzon, S. (2003). Working together supporting projects through action learning.
Health Information and Libraries Journal 20, 225-231. • Bennis, W. (2012). The challenges of leadership in the modern world: introduction to the special
issue. American Psychologists, , pp.1-7. Retrieved March 1, 2012, from Academic Search Complete
• Bond, A. S., & Naughton, N. (2011). The role of coaching in managing leadership transitions. International Coaching Psychology Review, 6, pp. 165-179. Retrieved March 1,2012, from Academic Search Complete
• Eiser, B. J. (2008). Meeting the challenge of moving from technical expert to leader. Leadership in Action, 28, pp. 13-24. Retrieved, January 15
• Flores, K. L., Matkin, G. S., Burbach, M. E., Quinn, C. E., & Harding, H. (2012). Deficit critical thinking skills among college graduates: implications for leadership. Educational Philosophy and Theory, 44, pp. 212-230. Retrieved January 17, 2012, from Academic Search Complete
• Kerfoot, K. M. (2010). Doing what only what you can do: the challenge to the promoted leader. Nursing Economics, 28, pp. 403-404. Retrieved January 16,2012, from Academic Saerch Complete
• Khan, O. (2005). The challenge of adaptive leadership. Leader to Leader, pp. 52-58. Retrieved April 15, 2012, from Academic Search Complete
54 54
Thank You to the Canadian Society of Respiratory Therapist !
Questions?