reversed intracranial blood flow in patients with an intra...
TRANSCRIPT
484
Reversed Intracranial Blood Flow in PatientsWith an Intra-aortic Balloon Pump
Lawrence M. Brass, MD
As a preliminary investigation into the cerebral effects of mechanical cardiac assist devices,using transcranial Doppler ultrasonography I examined the basal cerebral arteries in threepatients placed on an intra-aortic balloon pump. Unassisted systoles had normal bloodvelocities and waveforms. When the pump was in use, diastolic blood velocity during ballooninflation increased. As the balloon was deflated and intra-aortic pressure was dramaticallylowered, diastolic blood velocity within the intracranial vessels decreased sharply. In twopatients there was a reversal of blood flow in the middle cerebral, anterior cerebral, basilar, andvertebral arteries during late diastole. Although the clinical effects of cessation and reversal ofblood flow in the cerebral circulation while on an intra-aortic balloon pump remain to bedetermined, transcranial Doppler ultrasonography appears to be a useful tool for measuringthese hemodynamic effects. It may also be helpful in quantifying the effects of such pumps oncerebral blood flow and devising inflation/deflation timing sequences that maximize forwardblood flow. (Stroke 1990^1:484-487)
When medical treatment fails to sustain car-diac output, mechanical assist devices canbe used to support left ventricular func-
tion. One of the most widely used devices is theintra-aortic balloon pump.1 The most common appli-cations of this device include its use in patients withunstable angina and cardiogenic shock, for preoper-ative support, and in weaning patients from cardio-pulmonary bypass.
Intra-aortic balloon pumping decreases myocardialoxygen consumption, increases coronary blood flow,and increases cardiac output in patients with cardio-genic shock. In this procedure, a balloon is placedinto the aorta just distal to the left subclavian artery,usually via the femoral artery. The balloon is con-nected to an external pump via a catheter. Thepumping is timed so that the balloon inflates imme-diately after the aortic valve closes. Balloon inflationdecreases diastolic aortic runoff and increases dia-stolic aortic pressure; these changes increase perfu-sion of the coronary arteries. The balloon deflatesjust before systole. Balloon deflation results in sys-tolic unloading and a decrease in the aortic imped-ance to left ventricular ejection. This combinationcauses relatively little change in the mean aortic
From the Yale Stroke Program, Department of Neurology, YaleUniversity School of Medicine, New Haven, Connecticut
Presented in part at the 41st Annual Meeting of the AmericanAcademy of Neurology, Chicago, Illinois, April 1989.
Address for reprints: Lawrence M. Brass, MD, Department ofNeurology LCI-700, Yale University School of Medicine, 333Cedar Street, New Haven, CT 06510.
Received May 5, 1989; accepted October 16, 1989.
pressure but decreases the left ventricular pressureby approximately 20% and increases cardiac outputby up to 40% in patients with cardiogenic shock.2
Using transcranial Doppler ultrasonography (TCD),I examined three patients placed on an intra-aorticballoon pump in a preliminary investigation of theeffects of the device on the cerebral circulation.
Case ReportsMethods
I used a Transpect TCD (Medasonics, MountainView, California) with a 2-MHz pulsed Dopplerprobe. The pulse repetition frequency is adjustable to3.9, 5.25, 7.8, or 10.5 kHz by software under usercontrol. The spatial peak temporal average intensityof the ultrasound is 161 mW/cm2. The TCD tech-nique has been described.3
A System 90T Transport intra-aortic baiioon pump(Datascope Corp., Paramus, New Jersey) was used inall patients. It is a helium-charged, mobile intra-aortic balloon pump that times balloon inflation/deflation automatically, with only minimal adjust-ments required by the operator. The device triggersballoon inflation/deflation from patient electrodes orexternally generated electrocardiographic signals, apressure transducer or externally generated pressuresignals, or a fixed internal square wave.
Three patients in the cardiac care unit on anintra-aortic balloon pump were studied at the requestof their physicians.
CasesI initially studied a 63-year-old right-handed man
admitted to the hospital for an acute myocardial
by guest on June 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Brass Reversed Blood Flow With IABP 485
MIDS" '"
t t
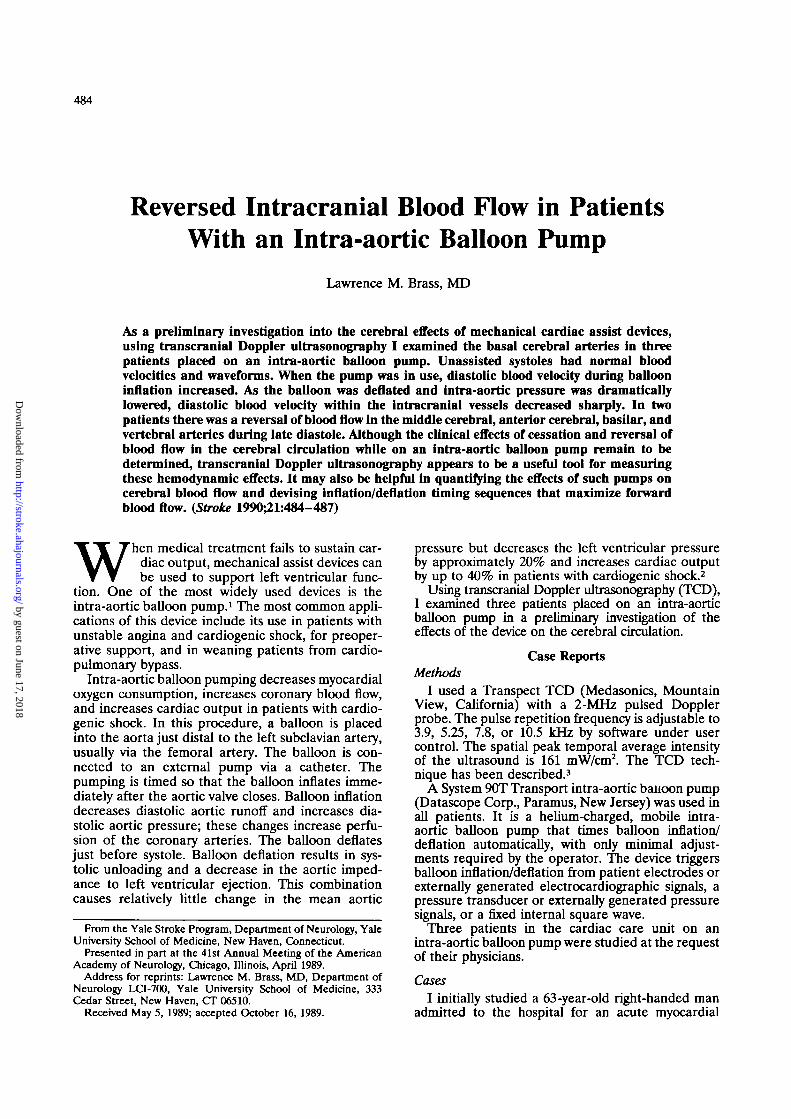
FIGURE 1. Transcranial Dopp-ler ultrasonogram of blood veloc-ity in middle cerebral artery whileintra-aortic balloon pump is oper-ating. Arrows indicate reversal ofMood flew during late diastole.
infarction. Six weeks earlier, he had suffered a minorbrainstem infarction. TCD examination was per-formed before a planned coronary artery bypass graftfor unstable angina, at a time when the patient wason an intra-aortic balloon pump. In the posteriorcirculation, a reversal of blood flow late in diastolewas noted. Two other men, 54 and 61 years old, in thecardiac care unit after an acute myocardial infarctionwere also studied by TCD. All three patients werestudied when the intra-aortic balloon pump wasabout to be discontinued and could be safely turnedoff and on.
All three patients had normal TCD examinationswith the pump turned off. Systolic blood velocities inthe middle cerebral artery ranged from 70 to 105cm/sec, in the anterior cerebral artery from 62 to 115cm/sec, and in the basilar artery from 42 to 73 cm/sec.
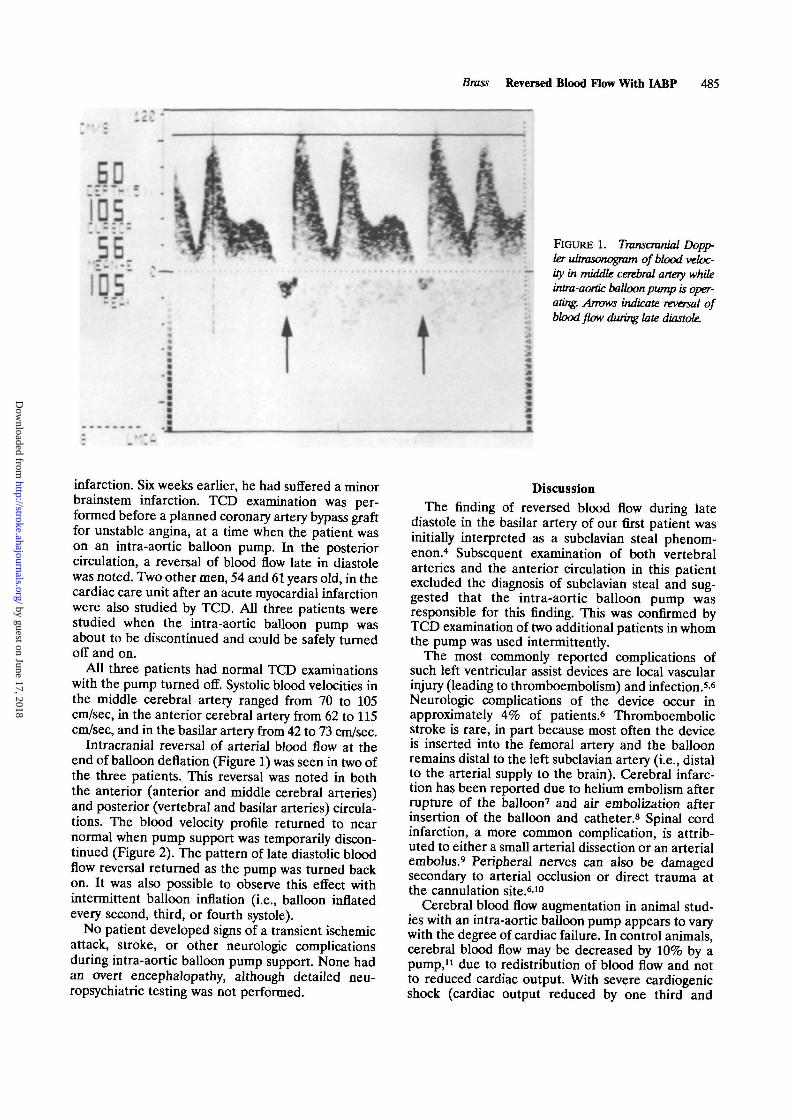
Intracranial reversal of arterial blood flow at theend of balloon deflation (Figure 1) was seen in two ofthe three patients. This reversal was noted in boththe anterior (anterior and middle cerebral arteries)and posterior (vertebral and basilar arteries) circula-tions. The blood velocity profile returned to nearnormal when pump support was temporarily discon-tinued (Figure 2). The pattern of late diastolic bloodflow reversal returned as the pump was turned backon. It was also possible to observe this effect withintermittent balloon inflation (i.e., balloon inflatedevery second, third, or fourth systole).
No patient developed signs of a transient ischemicattack, stroke, or other neurologic complicationsduring intra-aortic balloon pump support. None hadan overt encephalopathy, although detailed neu-ropsychiatric testing was not performed.
DiscussionThe finding of reversed blood flow during late
diastole in the basilar artery of our first patient wasinitially interpreted as a subclavian steal phenom-enon.4 Subsequent examination of both vertebralarteries and the anterior circulation in this patientexcluded the diagnosis of subclavian steal and sug-gested that the intra-aortic balloon pump wasresponsible for this finding. This was confirmed byTCD examination of two additional patients in whomthe pump was used intermittently.
The most commonly reported complications ofsuch left ventricular assist devices are local vascularinjury (leading to thromboembolism) and infection.5-6
Neurologic complications of the device occur inapproximately 4% of patients.6 Thromboembolicstroke is rare, in part because most often the deviceis inserted into the femoral artery and the balloonremains distal to the left subclavian artery (i.e., distalto the arterial supply to the brain). Cerebral infarc-tion has been reported due to helium embolism afterrupture of the balloon7 and air embolization afterinsertion of the balloon and catheter.8 Spinal cordinfarction, a more common complication, is attrib-uted to either a small arterial dissection or an arterialembolus.9 Peripheral nerves can also be damagedsecondary to arterial occlusion or direct trauma atthe cannulation site.610
Cerebral blood flow augmentation in animal stud-ies with an intra-aortic balloon pump appears to varywith the degree of cardiac failure. In control animals,cerebral blood flow may be decreased by 10% by apump,11 due to redistribution of blood flow and notto reduced cardiac output. With severe cardiogenicshock (cardiac output reduced by one third and
by guest on June 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from
486 Stroke Vol 21, No 3, March 1990
FIGURE 2. Tnwscmnial Dopp-ler ultrasonogram of blood veloc-ity in middle cerebral artery whileintra-aortic balloon pump isturned off. There are no negativevelocities (Le., no reversal of bloodflow). This tracing was madewithin minutes of that shown inFigure 1.
cerebral perfusion reduced by 80%), the addition ofan intra-aortic balloon pump increased cerebralblood flow by 50% over that in animals with cardio-genic shock and no pump.12
In human studies, Gee et al13 noted an overallreduction of 11.4% in ocular blood flow measured byocular pneumoplethysmography in patients on anintra-aortic balloon pump. In 56 patients, 73%showed a decrease (average 24%), 23% showed anincrease (average 26%), and 4% showed no changein blood flow.
Reversed blood flow in the intracranial arteriesduring diastole is seen in few clinical diseases. Theseinclude increased intracranial pressure,14 intracranialcirculatory arrest,15 and, in the posterior circulation,the subclavian steal syndrome.4
Although it is well established that intra-aorticballoon pumping improves cardiac output anddecreases myocardial work, its effects on the cerebralcirculation have not been systematically examined.The clinical significance of this dramatic alteration inthe cerebral blood flow pattern is unknown. Neuro-logic sequelae from such a pump may be detectableonly with careful psychometric testing, as is neededto detect the intellectual impairment and subtlepersonality changes following cardiopulmonarybypass.16-17
Neuropsychological deficits may be found in 50-75% of patients undergoing coronary artery bypasssurgery.18-19 Early reports of the neurologic compli-cations of cardiopulmonary bypass greatly underesti-mated these complications because of the lack ofdetailed cognitive testing. Early work suggests thatTCD may be a useful tool for monitoring cerebralperfusion during cardiac surgery.20 Similar work
remains to be done for both the clinical and hemo-dynamic effects of intra-aortic balloon pumps.
TCD provides valuable information about theblood flow patterns with intra-aortic balloon pump-ing. TCD is superior to conventional cerebral bloodflow techniques for detecting these changes becauseit can measure subsecond changes in velocity. Similarblood flow patterns are seen in the subclavian stealsyndrome.4-21 In this disease, with blood flow abnor-malities restricted predominantly to the posteriorcirculation, the TCD pattern is usually benign.21
Long-term monitoring of the cerebral circulationwith TCD can identify microemboli within the mid-dle cerebral artery during cardiopulmonary bypassprocedures.22 Similar techniques during the use ofleft ventricular assist devices may help identify occultcerebral embolization with intra-aortic balloonpumps.
Currently, this device uses a square-wave functionto control gas flow into the balloon. With TCD, itmay be possible to devise nonlinear inflation/deflation sequences for intra-aortic balloon pumpsthat maximize forward blood flow in the intracranialcirculation.
TCD measures of cerebral blood flow velocity mayhelp determine optimal regimens for the use ofintra-aortic balloon pumps and other left ventricularassist devices. Further conclusions from this observa-tion await larger clinical series and the use ofdetailed cognitive testing.
AcknowledgmentI would like to thank Medasonics (Mountain View,
California) for their technical support of theTranspect TCD.
by guest on June 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Brass Reversed Blood Flow With IABP 487
References1. Bolooki H: Current status of circulatory support with an
intra-aortic balloon pump. Cardiol Clin 1985;3:266-2762. Braunwald E: Mechanical circulatory support, in Braunwald E
(ed): Heart Disease. Philadelphia, WB Saunders Co, 1988, pp531-533
3. Aaslid R, Markwalder TM, Nornes H: Noninvasive transcra-nial Doppler ultrasound recording of flow velocity in basalcerebral arteries. / Neurosurg 1982;57:769-774
4. Klingelhdfer J, Conrad B, Benecke R, Frank B: TranscranialDoppler ultrasonography of carotid-basilar collateral circula-tion in subclavian steal. Stroke 1988;19:1036-1042
5. Wasfie T, Freed PS, Rubenfire M, Wajszczuk W, Reiraann P,Brozyna W, Schork MA, Kozlowski J, Kantrowitz A: Risksassociated with intraaortic balloon pumping in patients withand without diabetes mellitus. Am J Cardiol 1988;61:558-562
6. Kantrowitz A, Wasfie T, Freed PS, Rubenfire M, WajszczukW, Schork MA: Intraaortic balloon pumping 1967 through1982: Analysis of complications in 733 patients. Am J Cardiol1986;57:976-983
7. Fredriksen JW, Smith J, Brown P, Zinetti C: Arterial embo-lism from a ruptured intraaortic balloon. Ann Thorac Surg1988;46:690-692
8. Haykal HA, Wang AM: CT diagnosis of delayed cerebral airembolism following intraaortic balloon pump catheter inser-tion. Comput Radiol 1986;10:307-309
9. Rose DM, Jacobowitz IJ, Acinapura AJ, Cunningham JN Jr:Paraplegia following percutaneous insertion of an intra-aorticballoon. J Thorac Cardiovasc Surg 1984;87:788-789
10. Wilbourn AJ, Furlan AJ, Hulley W, Ruschhaupt W: Ischemicmonomelic neuropathy. Neurology 1983;33:447-451
11. Oster H, Stanley TH, Olsen DB, Nielsen M, Kolff WJ:Regional blood flow after intra-aortic balloon pumping beforeand after cardiogenic shock. Trans Am Soc Artif Intern Organs1974;20:721-723
12. Bhayana JN, Scott SM, Sethi GK, Takaro T: Effects ofintraaortic balloon pumping on organ perfusion in cardiogenicshock. / Surg Res 1979;26:108-113
13. Gee W, Smith RL, Perline RK, Gallagher HS: Assessment ofintra-aortic balloon pumping by ocular pneumoplethysmogra-phy. Am Surg 1986;52:489-491
14. Hassler W, Steinmetz H, Gawlowski J: Transcranial Dopplerultrasonography in raised intracranial pressure and in intra-cranial circulatory arrest. / Neurosurg 1988;68:745-751
15. Hassler W, Steinmetz H, Pirschel J: Transcranial Doppler ofintracranial circulatory arrest. / Neurosurg 1989;71:195-201
16. Aberg T, Kihlgren M: Cerebral protection during open heartsurgery. Thorax 1977;32:525-533
17. Furlan AJ, Breuer AC: Central nervous system complicationsof open heart surgery. Stroke 1984;15:912-915
18. Shaw PJ, Bates D, Cartlidge NEF, French JM, Heaviside D,Julian DG, Shaw DA: Long-term intellectual dysfunctionfollowing coronary artery bypass graft surgery: A six monthfollow-up study. QJMed 1987;62:259-268
19. Smith PL: The cerebral complications of coronary arterybypass surgery. Ann R Coll Surg Engl 1988;70:212-216
20. Lundar T, Lindberg H, Lindegaard KF, Tjonneland S, Rian R,Bo G, Nornes H: Cerebral perfusion during major cardiacsurgery in children. Pediatr Cardiol 1987;8:161-165
21. Hennerici M, Klemm C, Rautenberg W: The subclavian stealphenomenon: A common vascular disorder with rare neuro-logical deficits. Neurology 1988;38:669-673
22. Padayachee TS, Parson S, Theobold R, Linley TJ, GoslingRG, Deverall PB: The detection of microemboli in the middlecerebral artery during cardiopulmonary bypass: A transcranialDoppler ultrasound investigation using membrane and bubbleoxygenators. Ann Thorac Surg 1987;44:298-302
KEYWORDS •• ultrasonics
cerebral blood flow • intra-aortic balloon pump
by guest on June 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from
L M BrassReversed intracranial blood flow in patients with an intra-aortic balloon pump.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1990 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.21.3.484
1990;21:484-487Stroke.
http://stroke.ahajournals.org/content/21/3/484World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 17, 2018http://stroke.ahajournals.org/
Dow
nloaded from