risk factors for neurological complications after acoustic neurinoma radiosurgery: refinement from...
TRANSCRIPT

PII S0360-3016(00)00570-8
CLINICAL INVESTIGATION Brain
RISK FACTORS FOR NEUROLOGICAL COMPLICATIONS AFTER ACOUSTICNEURINOMA RADIOSURGERY: REFINEMENT FROM FURTHER
EXPERIENCES
KEN ITO, M.D.,* MASAHIRO SHIN, M.D.,† MASAKI MATSUZAKI, M.D.,* KEIKO SUGASAWA, M.D.,*AND TOMIO SASAKI, M.D.†
Departments of *Otolaryngology and†Neurosurgery, Faculty of Medicine, University of Tokyo, Tokyo, Japan
Purpose: Further actuarial analyses of neurological complications were performed on a larger population treatedby stereotactic radiosurgery at our institution, to establish the optimal treatment parameters.Methods and Materials: Between June 1990 and September 1998, 138 patients with acoustic neurinomasunderwent stereotactic radiosurgery at Tokyo University Hospital. Of these, 125 patients who received medicalfollow-up for 6 months or more entered the present study. Patient ages ranged from 13 to 77 years (median, 53years). Average tumor diameter ranged from 6.7 to 25.4 mm (mean, 13.9 mm). Maximum tumor doses rangedfrom 20 to 40 Gy (mean, 29.8 Gy) and peripheral doses from 12 to 25 Gy (mean, 15.4 Gy). One to 12 isocenterswere used (median, 4). Follow-up period ranged from 6 to 104 months (median, 37 months). The potential riskfactors for neurological complications were analyzed by two univariate and one multivariate actuarial analyses.Neurological complications examined include hearing loss, facial palsy, and trigeminal nerve dysfunction.Variables included in the analyses were four demographic variables, two variables concerning tumor dimensions,and four variables concerning treatment parameters. A variable with significantp values (p < 0.05) on all threeactuarial analyses was considered a risk factor.Results: The variables that had significant correlation to increasing the risk for each neurological complicationwere: Neurofibromatosis Type 2 (NF2) for both total hearing loss and pure tone threshold (PTA) elevation;history of prior surgical resection, tumor size, and the peripheral tumor dose for facial palsy; and the peripheraltumor dose and gender (being female) for trigeminal neuropathy. In facial palsies caused by radiosurgery,discrepancy between the course of palsy and electrophysiological responses was noted.Conclusion: Risk factors for neurological complications seem to have been almost established, without largedifferences between institutions treating a large number of patients by radiosurgery. Radiosurgical doses andtumor dimensions were considered the two important risk factors for the 7th and 5th nerve injuries. Neurofi-bromatosis Type 2 was an important factor for hearing loss. © 2000 Elsevier Science Inc.
Radiosurgery, Acoustic neurinoma, Peripheral tumor dose, Hearing loss, Facial palsy, Trigeminal dysfunction.
INTRODUCTION
Stereotactic radiosurgery now has a place as an alternativeto microsurgery for acoustic neurinomas. Although radio-surgery has an inherent disadvantage in that it does notdirectly reduce the tumor volume, it has less treatment-associated morbidity, requires a shorter period of hospital-ization, permits sooner return to independent functioningafter treatment, and costs less in total management chargesthan microsurgery (1). Tumor control has also been shownto be acceptable (2, 3). However, as always occurs with arelatively new treatment, analyses of the complications andresults should continue in each institution treating a largenumber of patients. Risk factors for neurological complica-tions after radiosurgery have changed from early smallerstudies (4, 5) to the more recent studies with increased
number of patients (2, 3). The most important trend is theentry of dosages into risk factors for neurological compli-cations, because the dose can be most easily controlled bythe treating physician. However, the number of institutionsreporting the results is still small. In this paper, as a con-tinued effort to identify risk factors after our first report ofthe earlier 4-year period with a small number of patients (6),a larger study, with 125 patients over 8 years, is shown, andthe most important factors, which are common among re-ports from other institutions with large numbers of patients,are identified. Univariate and multivariate analyses werechosen, and, to exclude significance by chance, the criteriawere made more strict, and the number of nominated pa-rameters were reduced from the previous study. In addition,the unique course of severe facial palsy, with higher periph-
Reprint requests to: Dr. Ken Ito, Laboratoire EMI 99-27 IN-SERM, CHU Hopital Pellegrin, Baˆt. PQR entre´e 3, 2eme etage,Place Ame´lie Raba Leon, 33076 Bordeaux, France. E-mail: [email protected]
Acknowledgment—The present study was supported in part by afellowship to Dr. Ken Ito from the Canon Foundation.
Accepted for publication 10 March 2000.
Int. J. Radiation Oncology Biol. Phys., Vol. 48, No. 1, pp. 75–80, 2000Copyright © 2000 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/00/$–see front matter
75

eral doses, is described with a brief discussion of its mech-anism.
METHODS AND MATERIALS
Between June 1990 and September 1998, 138 patientswith acoustic neurinomas underwent unilateral stereotacticradiosurgery at the Tokyo University Hospital. Of these,125 patients (90.6%) who received medical follow-up for 6months or more were included in this study. Patient char-acteristics are shown in Table 1. Early extensive neuro-otological follow-up results, including detailed examina-tions of hearing and vestibular functions, were previouslypublished elsewhere for about one-third of these patients(6). This report also includes patients treated during theearlier period without hearing or vestibular function follow-up, who had been excluded from our previous study.
A 201-source60Co g unit was used for radiosurgery. CTor MRI was used to plan the radiosurgery. Treatment vari-ables are shown in Table 1. The peripheral tumor doseswere higher on average (around 18 Gy) in the earlier 2-yearperiod, and were reduced (around 14 Gy) thereafter.
The follow-up period ranged from 6 to 104 months (me-dian, 37 months). The detailed patient follow-up protocolappears elsewhere (7). In brief, the protocol called forneuro-otological examinations and imaging (CT and MRI)at the 3rd, 6th, and 12th month in the first year, and at6-month or 1-year intervals thereafter. The neuro-otologicalexaminations included facial nerve function (House–Brack-mann grade, HB-grade), trigeminal nerve function, andhearing.
The details of the actuarial analyses for determining risk
factors for neuro-otological complications were previouslydescribed (6). In this study, however, the criteria for adopt-ing a variable as a risk factor were made more strict. Inbrief, two univariate analysis methods (the Wilcoxon testand the log–rank test) and one multivariate analysis methodusing the Cox proportional hazards model were employed,and variables with significantp values (p , 0.05) on allthree actuarial analysis methods were considered risk fac-tors for the complication. A risk factor is a variable associ-ated with a significantly higher incidence or earlier onset ofa given complication. The variables nominated as potentialrisk factors for neuro-otological complications are four de-mographic variables consisting of age, gender (male/fe-male), prior operation (yes/no), and neurofibromatosis Type2 (NF2, yes/no); two parameters concerning tumor dimen-sions consisting of average tumor diameter (mm) and tumorvolume (cc); and four treatment variables consisting ofmaximum tumor dose (Gy), peripheral tumor dose (Gy),number of isocenters, and treatment Planning with MRI(yes/no).
The following neuro-otological complications concerningthe 5th, 7th, and 8th cranial nerves were examined: (1) lossof any measurable hearing, (2) pure tone threshold (PTA)elevation of 20 dB or more, (3) development of any facialnerve dysfunction including transient spasm, (4) develop-ment of facial palsy, (5) development of severe, intractablefacial palsy (HB-Grade 5 or more), and (6) development ofany trigeminal nerve dysfunction.
RESULTS
The summarized list of the potential risk factors for eachneurological complication appears in Table 2. Thep valuesfrom two univariate analyses and a multivariate analysis arealso shown. Described below are the results for each neu-rological complication. It must be noted that the proportionand the onset of the complications can be distorted becauseof the variation in the follow-up periods. The ‘true’ medianonset latency can be larger than mentioned below, if it isequal to or more than the criterion for entrance into thestudy, i.e., 6 months. The actuarial analyses, however, han-dle precisely the variation of follow-up periods, and theirresults are not distorted for this reason.
Total hearing lossTwelve (14%) of the 84 patients with any measurable
hearing before treatment became totally deaf after radiosur-gery. The median onset was 10 months. NF2 was the onlypotential risk factor for the deafness after radiosurgery,which marked highly significantp values from all threeanalyses.
PTA elevation of 20 dB or morePTA elevation of 20 dB or more occurred in 35 (42%) of
the 83 patients whose hearing level was determined by puretone audiometry before treatment. The median onset was 12months. As with total deafness, NF2 was found to be the
Table 1. Patient characteristics (n 5 125) and treatmentparameters
Characteristic orparameter
Number (%) of patients, orvalue range (median or mean)
Age (years) 13–77 (median, 53)Gender
Male 64 (51%)Female 61 (49%)
Side of treatmentRight 66 (53%)Left 59 (47%)
Neurofibromatosis* 6 (4.8%)Prior surgical resection 31 (25%)Average tumor diameter 6.7–25.4 mm (mean, 13.9 mm)Tumor volume 0.15–8.6 cc (mean, 1.8 cc)Treatment planning by
CT 111 (89%)MRI 14 (11%)
No. of Isocenters 1–12 (median, 4)Maximum tumor dose 20–40 Gy (mean, 29.8 Gy)Peripheral tumor dose 10–25.2 Gy (mean, 15.4 Gy)
, 16 Gy 84 (67%). 16 Gy 41 (33%)
*With bilateral tumors. Radiosurgery was performed only onone side.
76 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000
only risk factor for the threshold elevation in the middlefrequency, with highly significantp values from all threeanalyses.
Any facial nerve dysfunction including transient spasmForty-four (36%) of the 123 patients with reliable fol-
low-up records for facial nerve function experienced facialpalsy or transient facial spasm after treatment. The medianonset was 6 months. Peripheral tumor dose was recognizedas a highly significant risk factor by all three analyses. Byunivariate analyses, the number of isocenters and treatmentplanning with MRI were also suspected to be factors thatreduced the radiosurgical toxicity.
Any facial palsyDelayed facial palsy or its exacerbation occurred in 20
(16%) of the 123 patients, with a median onset of 5 months.
Prior surgery, peripheral tumor dose, and tumor size were,in this order, the three most important variables significantlyassociated with facial palsy.
Severe facial palsySevere facial palsy with an HB-grade of 5 or more
occurred in 8 (6.5%) of the 123 patients, with a medianonset of 4.5 months. Tumor size and peripheral tumor dosewere the two most important risk factors in this order,recognized by all three analyses.
Any trigeminal nerve dysfunctionDelayed trigeminal nerve dysfunction occurred in 31
(25%) of the 124 patients with a reliable neurological fol-low-up for facial sensation. The median onset was 5months. Peripheral tumor dose was revealed to be a risk
Table 3. Comparison of the patients and their results after radiosurgery treated with lower doses(peripheral dose, 16 Gy) and those treated with higher doses (peripheral dose. 16 Gy); for
neurological complications, the numbers, proportions, and the onsets are shown
Peripheral tumor dose , 16 Gy . 16 Gy
No. of patients 84 41Age (years) 13–77 (median, 53) 26–73 (53)Male/female 41/43 23/18Neurofibromatosis Type 2 5 (6%) 1 (2.4%)Average tumor diameter 6.7–25.4 mm (mean, 13.3 mm) 8.3–21 mm (14.3 mm)Prior operation (n) 21 (25%) 10 (24%)No. of isocenters (n) 1–12 (mean, 5.7) 1–10 (3.8)Follow-up period (months) 6–104 (median, 35.5) 11–98 (47)Total deafness (n) 9 (of 56: 11%) 3 (of 28: 7.3%)
Onset (months) 0–18 (median, 9) 3–12 (11)PTA up by. 20 dB (n) 21 (of 56: 25%) 14 (of 27: 34%)
Onset (months) 0–37 (median, 12) 3–39 (21.5)Any 7th symptom (n) 18 (of 83: 21%) 26 (of 40: 63.4%)
Onset (months) 0–23 (median, 6) 0–19 (6.5)7th palsy (n) 8 (of 83: 9.5%) 12 (of 40: 29%)
Onset (months) 0–8 (median, 4) 0–13 (5)Severe 7th palsy (n) 2 (of 83: 2.4%) 6 (of 40: 14.6%)
Onset (months) 0–7 (median, 3.8) 0–13 (4.5)Any 5th symptom (n) 13 (of 84: 15.5%) 18 (of 40: 44%)
Onset (months) 0–11 (median, 6) 0–27 (3.5)
Table 2. Risk factors for neurological complications; thep values of actuarial analyses are shown for each risk factor
Wilcoxon Log–Rank Cox
Total deafness Neurofibromatosis Type 2 0.0045 0.0013 0.0014(n 5 84)
PTA elevation by. 20 dB Neurofibromatosis Type 2 0.0103 0.0005 0.0002(n 5 83)
Any 7th symptom Peripheral tumor dose 0.0004 0.0001 0.0001(n 5 123)
Facial palsy Prior operation 0.0036 0.0026 0.0025(n 5 123) Peripheral tumor dose 0.0196 0.0209 0.0082
Tumor volume 0.0345 0.0288 0.0433Severe facial palsy Tumor diameter 0.0084 0.0089 0.0087
(n 5 123) Peripheral tumor dose 0.0452 0.0452 0.0297Any 5th symptom Peripheral tumor dose 0.0039 0.0046 0.0039
(n 5 124) Being female 0.0412 0.0491 0.0155
77Risk factors for neurological complications after acoustic neurinoma radiosurgery● K. ITO et al.
factor from all three analyses. Furthermore, patient gender(being female) passed the present criteria of a risk factor.
Tumor increase was noted in 11 patients (8.8%) duringthe follow-up period, with median onset of 12 months.Tumor growth or shrinkage was determined as a change indiameter by more than 2 mm on MRI.
Comparison of results with different dosagesTable 3 shows patient characteristics and complications
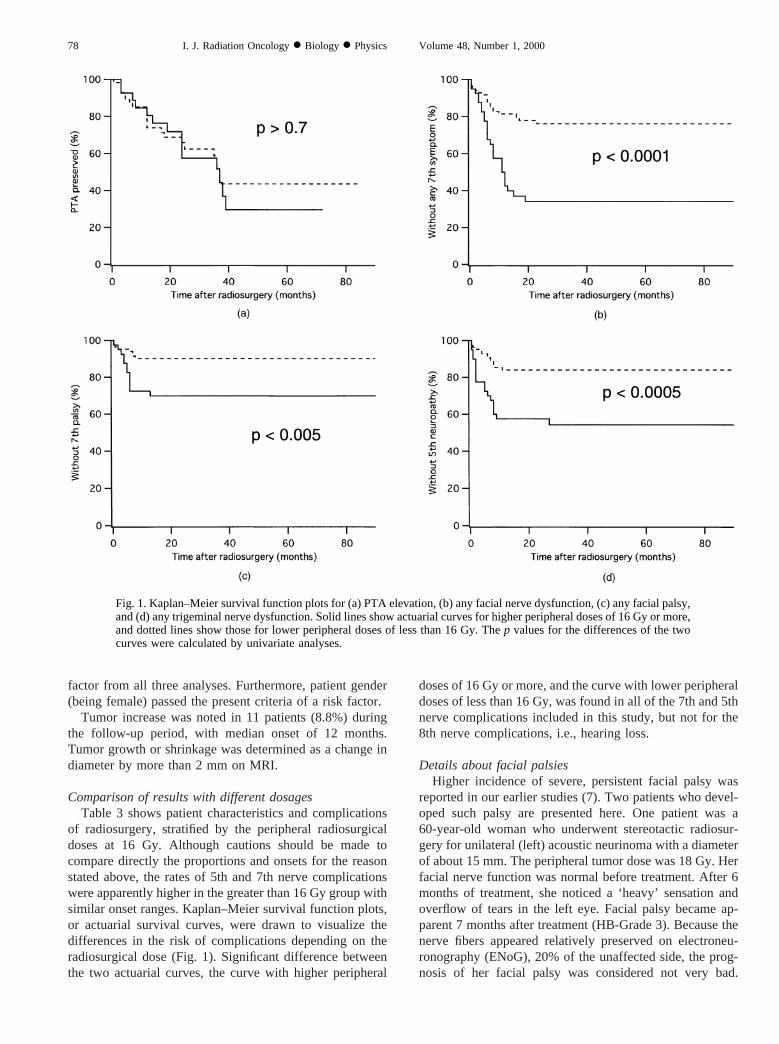
of radiosurgery, stratified by the peripheral radiosurgicaldoses at 16 Gy. Although cautions should be made tocompare directly the proportions and onsets for the reasonstated above, the rates of 5th and 7th nerve complicationswere apparently higher in the greater than 16 Gy group withsimilar onset ranges. Kaplan–Meier survival function plots,or actuarial survival curves, were drawn to visualize thedifferences in the risk of complications depending on theradiosurgical dose (Fig. 1). Significant difference betweenthe two actuarial curves, the curve with higher peripheral
doses of 16 Gy or more, and the curve with lower peripheraldoses of less than 16 Gy, was found in all of the 7th and 5thnerve complications included in this study, but not for the8th nerve complications, i.e., hearing loss.
Details about facial palsiesHigher incidence of severe, persistent facial palsy was
reported in our earlier studies (7). Two patients who devel-oped such palsy are presented here. One patient was a60-year-old woman who underwent stereotactic radiosur-gery for unilateral (left) acoustic neurinoma with a diameterof about 15 mm. The peripheral tumor dose was 18 Gy. Herfacial nerve function was normal before treatment. After 6months of treatment, she noticed a ‘heavy’ sensation andoverflow of tears in the left eye. Facial palsy became ap-parent 7 months after treatment (HB-Grade 3). Because thenerve fibers appeared relatively preserved on electroneu-ronography (ENoG), 20% of the unaffected side, the prog-nosis of her facial palsy was considered not very bad.
Fig. 1. Kaplan–Meier survival function plots for (a) PTA elevation, (b) any facial nerve dysfunction, (c) any facial palsy,and (d) any trigeminal nerve dysfunction. Solid lines show actuarial curves for higher peripheral doses of 16 Gy or more,and dotted lines show those for lower peripheral doses of less than 16 Gy. Thep values for the differences of the twocurves were calculated by univariate analyses.
78 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000

However, the palsy gradually progressed to HB-Grade 5, 10months after treatment. Oral steroids were ineffective. Thepalsy started to subside spontaneously 4.5 years after treat-ment, and had improved to HB-Grade 3 (at 5 years aftertreatment and thereafter). The ENoG results stayed almoststable throughout the follow-up period, ranging from 12%to 21% of the responses on the unaffected side. On otherneurological outcomes, her pretreatment hearing of about60 dB in PTA was totally lost 11 months after treatment,and she complained of persistent facial hypesthesia in theregion of the third branch of the trigeminal nerve 10 monthsafter treatment. There had been no caloric response beforetreatment. The tumor size has remained unchanged. Anotherpatient was a 59-year-old woman who underwent radiosur-gery for unilateral (right) acoustic neurinoma with a diam-eter of about 20 mm. The peripheral dose was 18 Gy. Shehad no symptoms suggesting facial nerve injury beforetreatment. Facial spasm was noted in the right lower lid 6months after treatment, and facial palsy developed gradu-ally thereafter. On examination 7 months after treatment,HB-Grade 3 palsy was found and the ENoG revealed nerve-fiber preservation of 82% compared to the unaffected side.Despite oral steroid therapy, palsy exacerbated as with theformer patient, and reached HB-Grade 5, 1 year after treat-ment. Spontaneous remission did not occur until 2 yearsafter treatment. Regarding other neurological outcomes,persistent facial hyperesthesia developed 7 months aftertreatment. She was already deaf, and there had been nocaloric response before treatment. The tumor size remainedunchanged.
DISCUSSION
Because radiosurgery has been widely performed as analternative treatment for acoustic neurinomas, numerousefforts have been made to determine the optimal treatmentparameters both to minimize the neurological complicationsand to maximize the effect of radiosurgery. In the earlierperiod with a limited number of patients, risk factors forneurological complications reported by major institutionsperforming radiosurgery used to vary greatly (4–6, 8). Withan increase in the number of patients and with longerfollow-up periods, the risk factors seem to have stabilized,which means less difference between institutions (2, 3)(Table 4). In the present study, gender (being female) wasdetermined as the second most important risk factor fortrigeminal neuropathy. However, we have no valid expla-nation for the mechanism of the influence of gender on theneuropathy. Only continued follow-up studies will be ableto determine the validity of this risk factor. Judging from therisk factors common to two or more institutions, radiosur-gical doses and tumor dimensions are the two important riskfactors for 7th and 5th nerve injuries, while neurofibroma-tosis Type 2 is the only important factor for hearing loss.The most important point was the entry of radiosurgicaldose into the risk factors for 7th and 5th neuropathies. Asthe radiosurgical doses had already been reduced on the
whole to diminish complications, recent results did statisti-cally confirm the appropriateness of this decision. The orderin which neurological complications showed radiosurgicaldoses as a significant risk factor is interesting, because itreflects the proximity of each nerve from the focus ofirradiation, i.e., from the tumor probably arising from thelower vestibular nerve. In our previous study with a smallernumber of patients (6), only vestibular dysfunction showedthe dosage as a significant risk factor. In the present study,both 7th and 5th nerve complications had the dosage as asignificant risk factor, with greater significance in 7th nerveinjury than in the 5th. The fact that the doses failed to enterinto risk factors for hearing loss, despite the proximity of thecochlear nerve to the center of irradiation, would supportour hypothesis that the mechanism of cochlear nerve injurywould differ from those of vestibular, 7th, and 5th nerveinjuries (6).
Nevertheless, the problem of choosing the optimal doseshas not been fully solved. Studies with large numbers ofpatients, including our study, have shown that a peripheraltumor dose of less than 16 Gy is recommended (2, 3), buthave not yet shown the optimal dose, i.e., 12 Gy, 14 Gy, or15 Gy. To draw conclusions on this issue, further follow-upstudy will be necessary. Another problem will be the pos-sibility of reduced tumor control with lower dosages. Tumorshrinkage rate was reported to be lower with lower dosages,although the difference failed to reach significance (3). Inour present study, as well, tumor growth rates were higherfor lower dosages (11% in the, 16 Gy group as comparedwith 4.9% in the. 16 Gy group), also without significance.However, the difference might reach significance with in-creases in the number of patients and with longer follow-upperiods. If this is confirmed in the future, our standard
Table 4. Comparison of recently reported risk factors
Institution Risk factor
Facial Palsy (VII)Pittsburgh Tumor diameter
Minimum tumor dosePlanning with MRI*
Mayo Clinic Radiosurgical doseTokyo Prior operation
Tumor sizePeripheral tumor dose
Trigeminal Neuropathy (V)Pittsburgh Tumor diameter
Minimum tumor dosePlanning with MRI*
Mayo Clinic Tumor diameterTokyo Peripheral tumor dose
Gender (female)Hearing Loss (VIII)
Pittsburgh NF2Tumor diameter
Planning with MRI*Tokyo NF2
*This parameter REDUCES the risk.NF2 5 neurofibromatosis Type 2.
79Risk factors for neurological complications after acoustic neurinoma radiosurgery● K. ITO et al.

peripheral tumor dose of 14 Gy might need to be increasedslightly.
From the findings of the present study, unsatisfactoryresults involving facial nerve injuries in our previous reportof the earlier period (6), especially severe persistent palsy,proved to be due to higher peripheral tumor doses. In facialpalsies caused by radiosurgery, discrepancy between thecourse of palsy and ENoG responses, which approximatethe proportion of uninjured nerve fibers (9), was noted. Withordinary peripheral facial palsy, such as Bell’s palsy, theprognosis of the palsy can be estimated fairly well unless
the response has reached less than 10% on ENoG, whichindicates nerve degeneration of more than 90% (9–12). Thecourses of palsy in the two cases described above betrayedthe estimations of good prognoses from ENoG results. It hasyet to be determined whether or not the disease processes offacial palsy caused by irradiation are different from thosewith Bell’s palsy or other peripheral facial palsies.
To establish the optimal radiosurgical doses and toachieve acceptable tumor control with lower dosages, fol-low-up studies should be continued with larger populationsand longer follow-up periods.
REFERENCES
1. Pollock BE, Lunsford LD, Kondziolka D,et al. Outcomeanalysis of acoustic neuroma management: A comparison ofmicrosurgery and stereotactic radiosurgery.Neurosurgery1995;36:215–224.
2. Miller RC, Foote RL, Coffey RJ,et al. Decrease in cranialnerve complications after radiosurgery for acoustic neuromas:A prospective study of dose and volume.Int J Radiat OncolBiol Phys1999;43:305–311.
3. Flickinger JC, Kondziolka D, Pollock BE,et al. Evolution intechnique for vestibular schwannoma radiosurgery and effecton outcome.Int J Radiat Oncol Biol Phys1996;36:275–280.
4. Flickinger JC, Lunsford LD, Linskey ME,et al.Gamma kniferadiosurgery for acoustic tumors: Multivariate analysis of fouryear results.Radiother Oncol1993;27:91–98.
5. Foote RL, Coffey RJ, Swanson JW,et al. Stereotactic radio-surgery using the gamma knife for acoustic neuromas.Int JRadiat Oncol Biol Phys1995;32:1153–1160.
6. Ito K, Kurita H, Sugasawa K,et al. Analyses of neuro-otological complications after radiosurgery for acoustic neuri-nomas.Int J Radiat Oncol Biol Phys1997;39:983–988.
7. Ito K, Kurita H, Sugasawa K,et al. Neuro-otological findingsafter radiosurgery for acoustic neurinomas.Arch OtolaryngolHead Neck Surg1996;122:1229–1233.
8. Linskey ME, Flickinger JC, Lunsford LD. Cranial nervelength predicts the risk of delayed facial and trigeminal neu-ropathies after acoustic tumor stereotactic radiosurgery.Int JRadiat Oncol Biol Phys1993;25:227–233.
9. Fisch U. Maximal nerve excitability testing vs electroneu-ronography.Arch Otolaryngol1980;106:352–357.
10. Brackmann DE. Recent advances in neuro-otology.HeadNeck Surg1981;4:22–28.
11. Gersdorff MC. Comments regarding prognostic significanceof stapes reflex in Bell’s palsy, application of electroneu-ronography in managing Bell’s palsy, and tuberculosis of themiddle ear in facial paralysis, management of an injured facialnerve following middle ear surgery.Am J Otol1991;12:468–469.
12. Rossi G, Solero P. Electroneuronography in the diagnosis andprognosis of diseases of the facial nerve.Acta Otolaryngol(Stockh)1980;89:271–276.
80 I. J. Radiation Oncology● Biology ● Physics Volume 48, Number 1, 2000