the life-threatening iatrogenic obstetric disease due to...
TRANSCRIPT

Placenta accreta The life-threatening iatrogenic
obstetric disease due to the cesarean section epidemy
Doc. Vedran Stefanovic
HYKS, Naistenklinikka
27.9.2012
GKS päivät

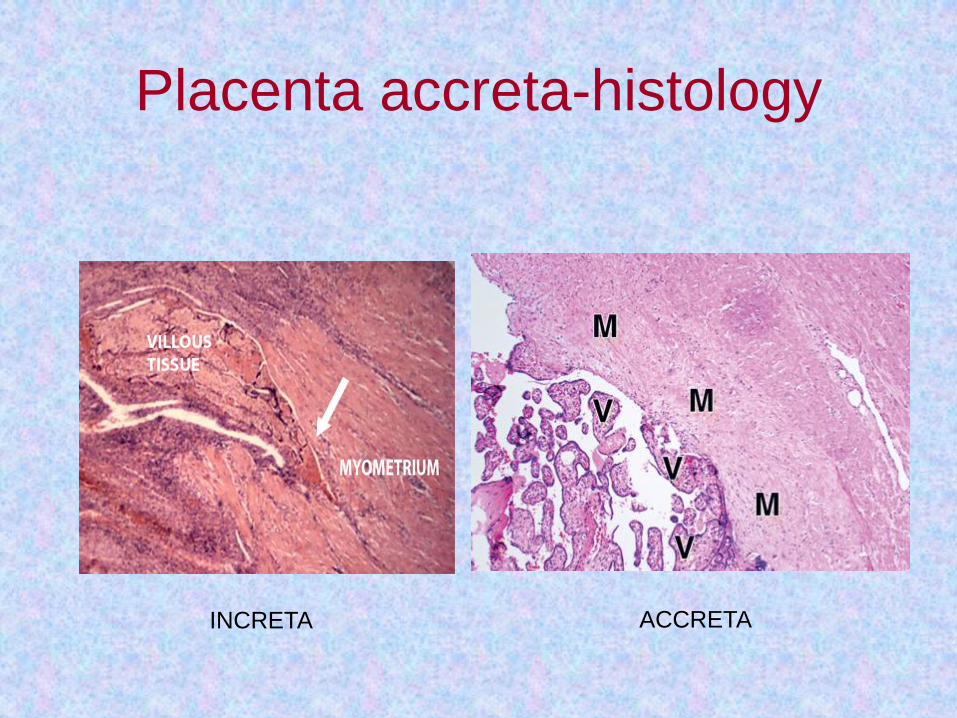
Placenta accreta
• The life-threatening condition
characterized by placental villi abnormally
adherent to the ( usually injured)
myometrium due to the absence or defect
in the normal decidua basalis

Placenta accreta
• According to the degree of invasion
according to the verified histopathology it
is devided into three groups:
• 1.Placenta acreta (vera)
• 2.Placenta increta
• 3.Placenta percreta

Placenta accreta (vera)
Abnormal adherence of
the placenta to the
myometrial wall, with
absence of decidua
basalis.

Placenta increta
Placenta attaches
deep into the uterine
wall and penetrates
into the uterine
muscle, but does not
penetrate the uterine
serosa

Placenta percreta
Placental villi
penetrate
myometrium and
through to uterine
serosa.

Image: Anesthesiology.org

One day you will see this!!!

Why PA is the Devil of Obstetrics?

Incidence
• The incidence varies according to the sources of
literature (dg criteria not consistent)
• The incidence may be as high as 1 in 533
pregnancies during the last two decades
• 1970s the incidence 1 in 4027 pregnancies
• 1980s 1 in 2510 pregnancies
• Nowadays most probably 1:1000
• The real false-positive and false-negative
incidence is unknown

• Pathologic diagnosis will lead to
underestimation of the true prevalence of
PA
• The use of clinical criteria will likely lead to
overestimation
• 20 % of women with placenta accreta are
primiparous

Use this ICD diagnosis !
• O43.2 Morbidly adherent placenta
• O43.2 Istukan kiinnikasvaminen kohtulihakseen
• O43.2 Sjukligt fastvuxen moderkaka

Placenta accreta Risk factors
• Approximately 95% of women diagnosed
with placenta accreta have identifiable risk
factors
• Placenta previa (≥ 90% of cases)
• Previous cesarean section
• Other factors:
– Advanced maternal age
– Other prior uterine surgery (myomectomy,
D&C,manual removal of placenta)
– IVF treatment,smoking, hypertension


Placenta accreta
The absolute truth is that the incidence of PA
has dramatically increased over the years
and is nowadays
the most common cause
of peripartum hysterectomy !! -

PA and prior CS (hysterotomy)

Placenta accreta
Diagnosis
• Obstetrical history (CS)
• Placenta praevia (>90%)
• Ultrasonography (gray-scale & Doppler)
• MRI

US criteria for PA

Transverse transabdominal US image shows the hyperechoic placenta surrounded by the
hypoechoic myometrium (arrowheads).
Baughman W C et al. Radiographics 2008;28:1905-1916
©2008 by Radiological Society of North America




On a sagittal image, the placenta is seen traversing the hypoechoic subplacental zone
(arrowheads) and appears to be bulging into the myometrium (arrow).
Baughman W C et al. Radiographics 2008;28:1905-1916
©2008 by Radiological Society of North America

Placental lacunae.
Baughman W C et al. Radiographics 2008;28:1905-1916
©2008 by Radiological Society of North America

Figure 2b. Placental lacunae.
Baughman W C et al. Radiographics 2008;28:1905-1916
©2008 by Radiological Society of North America
PA diagnosis
• Combination of ultrasound and MRI optimizes
diagnostic accuracy
• – Ultrasound sensitivity 77%, specificity 96%
• – MRI sensitivity 88%, specificity 100%
• More data are needed with fast sequences
(HASTE) Warshak et al, Obstet Gynecol, 2006
&Comstock, Ultrasound Obstet Gynecol, 2005
MRI useful especially in cases of posterior placenta and dubious cases

Antenatal diagnosis of placenta
accreta leads to reduced blood loss
(and most certainly other co-
morbidity)
Tikkanen et al, 2011
Eller, 2009
Chestnut, 1995

Placenta accreta- multidisciplinar
approach
• Eller at al, 2011
• N= 174
• End points: transfusion of ≥ 4 RBC units and re-operation within 7 days
• Maternal morbidity in cases of placenta accreta managed by a multidisciplinary care team is substantially lower compared to standard obstetric care (obstetrician, neonatologist, gyn.oncologist, interventional radiologist, urologist, anestesist)

Placenta percreta with bladder
invasion
• Macroscopic hematuria in only 25-31% of cases
• Value of cystoscopy for diagnosis based on personal
opinion, no true studies
• Studies show lower frequency of ureter injuries after
ureteral stent placements

When to deliver? (1)
• After 35 weeks, 93% of patients with PA
haemorrhage necessitating delivery (O´Brien, 1996)
• Planned delivery at 34 to 35 weeks did not
significantly increase neonatal morbidity in a cohort
of 99 cases ( Warshak, 2010)

When to deliver (2)
• In order to avoid emergency cesarean section
and improve preoperative preparations in
elective cases and to minimize complications
of prematurity, it is acceptable to schedule
cesarean delivery at 34-35 weeks!
• In patients experiencing earlier ante partum
haemorrhage treatment in casu
• Prenatal betamethasone one week before
elective cesarean delivery (rescue dose?)

How to deliver? (1)
• Ureteral stents on the day of cesarean section to avoid bleeding or/and uterine contractions
• Regional anaesthesia with easy conversion to GA if needed
• Preoperative balloon catheter insertion via a.femoralis (hybrid suite)
• Vertical skin incision
• Vertical uterine incision (classical cesarean) in order to avoid any contact with placenta

How to deliver? (2) Deliver infant and clamp the cord
Gentle attempt to remove placenta, if not succesful
a) conservative treatment
- leaving placenta in situ and MTX (see and wait) OR
b) emergent hysterectomy
c) delayed scheduled hysterectomy
In clear percreta cases
1. step-by step devascularization
and hysterectomy,urologist in situ !! OR
2. leaving placenta in situ (MTX) with total
conservative approach or scheduled delayed
hysterectomy

Image: courtesy of Dr. J. Jalkanen
Balloon occlusion (BO) • According to the available literature BO is useful in
diminishing the amount of blood loss in cases of PA
• The most common site is internal iliac artery, common
iliac artery would be better for a short period of time (20
min with intermitent deflation)
• Infrarenal portion of the abdominal aorta is also worthy
of consideration in extreme cases (5 case reports)
• There are no data on the real effectiveness of
prophylactic embolization!

Omar et al: Staged Endovascular Balloon Occlusion versus
Conventional Approach for Patients with Abnormal
Placentation: A Literature Review, 2012
Abundant collateral circulation Blood flow in internal iliac arteries after
previous total surgical occlusion

MTX and conservative treatment of
placenta accreta
• Spontaneous expulsion/resolution in 37/48 ( 6 abstracts and ”succesful treatment” including 5 MPR)-altogether succesful treatment in 48/53 (90,6%)
• Follow up 6 hrs – 8 months
• 5/53 (9.4%) cases of delayed hysterectomy (1 sepsis, 4 PPH)

Methotrexate in full-term placenta
Does it work?
• Reports of faster S-hCG drop with MTX
than with spontaneous resolution
• No controls
• Doppler flow usually correlates with S-hCG
drop and disappearance
• Negative S-hCG (of course) does not
exclude delayed haemorrhage
• Breast-feeding is safe (Stefanovic, unpublished)

Fertility and pregnancy outcome after conservative treatment for placenta accreta
Sentilhes, Hum Reprod, 2010
Accreta recurrence rate 28.6%

Prenatal counselling in PA cases
• Remember to offer tubal ligation (sterilization) if anticipated difficult hysterectomy and future fertility is not desirable !!

Solheim et al: The effect of cesarean delivery rates on the
future incidence of placenta previa, placenta accreta, and
maternal mortality.
J Matern Fetal Neonatal Med. 2011
- If primary and secondary cesarean rates
continue to rise as they have in recent
years, by 2020 the cesarean delivery rate
will be 56.2%, and there will be an
additional 6236 placenta previas, 4504
placenta accretas, and 130 maternal
deaths annually.

”Surprise ” accreta
• 1. Try to avoid further placental forced
removal
• 2. At the same time CALL FOR HELP
• 3. Bakri balloon tamponade (at least 400ml) +
Lynch sutures (sandwich)
• 4.Depending of bleeding status:
– Additional measures, a. uterine ligation or
hysterectomy
– If stable, but still bleeding,primipara and
transportation possible send forward!!

Conclusions
• Placenta accreta ”has arrived to stay” !
• Every obstetrician should be prepared for its
management
• Placenta previa + CS accreta unless proven
otherwise
• Consult! Call for help!
• Avoid chaos!
• Finnish PA registry ?