the russ hedrick r. r. center nutritional guide · 2018-08-16 · the russ hedrick r. r. center...
TRANSCRIPT

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE i
The Russ Hedrick Recovery Resource Center
Nutritional Guide to Optimize Recovery and
Ameliorate Post-Acute Withdrawal Symptoms
2018
Library of Congress cataloging-in publication
data
© 2018 Rajan Masih
All rights reserved
Except in the United States of America, this
book is sold subject to the condition that it shall
not, by the way of trade or otherwise be
circulated without the publisher’s prior consent
in any form of binding or cover other than that
in which it is published and without a similar
condition including this condition being
imposed on the subsequent purchaser.
The scanning, uploading and distribution
of the book via any other means without
permission of the publisher is punishable by
law. Please purchase only authorized electronic
editions, and do not participate in or encourage
electronic piracy of copyrighted materials. Your
support of the author’s rights is appreciated.

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE ii

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE iii
Acknowledgements
The authors wish to acknowledge the many
people who made this book possible.
Margaret Rioux
Jerrena Auville
Teresa Landis
Bob Borror

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE iv

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE v
Authors
Editors in Chief
Raj Masih MD, MPH, MPHN
Regional Health Promotion and Wellness
Coordinator PHG Petersburg, WV
Michael Landis MBA, AADC
Executive Director, PHG Petersburg, WV
Barbra Masih MS, CRC, PLPC
Substance Abuse Counselor, PHG Petersburg,
WV
Wade Rohrbaugh, Certified Recovery Coach,
CCAR, FAADP
Coordinator of the Russ Hedrick Recovery
Resource Center, Petersburg, WV
Christian J. Landis
Garrett Community College, Deep Creek, MD
Contributing Authors
Krystal Bates
Nutritional Expert, Charlotte, NC

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE vi
Kabeer Masih, MS
Texas Tech University School of Medicine EL
Paso, Texas
Justin Bates BS
University of San Francisco, CA
Brandon Bates, BS
News Anchor, WBIR, Knoxville, TN
Kevin Knowles, CCAR, FAADP
Berkeley County Community Recovery
Services Coordinator

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE vii
Dedications
This book is dedicated to my mother Catherine
Masih
&
Russ Hedrick

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE viii

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE ix
Table of Contents Pages
Background
Dopamine Deficiency Syndrome in
Addictions
Role of Nutrition
2016 Study of 1850 Patients with
Substance use Disorder
Research Questions
Research Objectives
Dopamine Deficiency Syndrome in
Addictions
Organization of the US Healthcare System
for Addictions Treatment
What is Dopamine
6 Phenylalanine Rich Foods
18 Top Foods for Dopamine
Central Nervous System effects of
Dopamine Restoration
Decreased Dopamine Transporters in a
Methamphetamine Abuser
The Cocaine Abuser’s Brain
D2 Receptors + Anhedonia
PET Scan Imaging
Effect on Energy
Effect on Sleep
Effect on Mood
Effect on Cravings
Effect on Restless Leg Symptoms
Engagement in Counseling and Goal
Setting Objectives
Pathophysiology of nutritional
deficiencies that occur with Substance
Use Disorder
Organization of the US Healthcare System

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE x
for Addictions Treatment
What is Dopamine
Central Nervous System Effects of
Dopamine Restoration
Whole Foods High in l-Tyrosine
Cheese (Parmesan)
Soy Foods (Roasted Soybeans)
Lean Beef & Lamb (Roast Beef)
Lean Pork (Chops, cooked)
Fish & Seafood (Salmon, cooked)
Chicken & Turkey (Chicken Breast,
cooked)
Seeds & Nuts (Pumpkin Seeds)
Eggs & Dairy (Eggs)
Beans & Lentils (White Beans, cooked)
Wholegrains (Wild Rice, cooked)
Phenyalanine Rich Foods:
Soy Foods (Roasted Soybeans)
Cheese (Parmesan)
Seeds & Nuts (Pumpkin Seeds)
Lean Beef & Lamb (Roast Beef)
Chicken & Turkey (Chicken Breast,
cooked)
Lean Pork (Chops, cooked)
Fish & Seafood (Tuna, cooked)
Eggs & Dairy (Eggs)
Beans & Lentils (Pinto Beans, cooked)
Wholegrains (Kamut, cooked)
Magnesium Rich Foods
Foods Rich in Zinc
Sample Food for Dopaminergic
Potentiation
Fava Bean Dopamine Delights (Dr. Oz,
2017)
References

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE xi


THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 1
Background
Substance Use Disorder (SUD) is a
primary, chronic brain disorder, characterized
by compulsive substance use, withdrawal, and
repeated use despite adverse consequences
(ASAM, 2017).
One of the primary pathological
mechanisms underlying SUD is impairment in
the dopamine reward system in the nucleus
accumbens and the amygdala of the brain. The
decreased metabolism of dopamine in the D2
receptors of the nucleus accumbens and the
amygdala results in a decreased dopaminergic
reward in response to normal pleasurable
stimuli (Volkow, 2007). This condition is
known as dopamine deficiency syndrome or
reward deficiency syndrome.
According to the CDC, in 2016, more
than 23,000,000 Americans suffered from SUD.
Less than 10% received any kind of treatment
at all, and those that received treatment are very
likely to relapse within one year (CDC, 2016).
Treatment for substance use disorder has
traditionally included behavioral modification,
detoxification, treatment modalities utilizing
counseling, and medication assisted treatment
utilizing medication such as methadone,
Suboxone, and Vivitrol (ASAM, 2017). In 2016

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 2
54,000 Americans died from opioid overdoses
(CDC, 2017).
Research conducted into the nutritional
and metabolic status of people with substance
use disorder who are currently in detox are eye-
opening and reveal a variety of nutritional
deficiencies including deficiencies in serum
zinc levels, vitamin D, vitamin C, vitamin B-
12, and lower than normal serum albumin
levels (Willis, 2016). People with substance use
disorder who are successful in going through
detoxification frequently suffer from anhedonia
meaning they are unable to derive pleasure
from normal stimuli. In response to this, people
with substance use disorder frequently turn to
consuming large amounts of caffeine, foods
containing simple sugars, carbonated
beverages, and nicotine products (Willis, 2016).
It may take months to years for brain
physiology and chemistry to normalize or
approach normalcy in the dopamine reward
system of the D2 receptors. This period of
months to years is a period of great
vulnerability to relapse, but is also a potential
time for targeted nutritional interventions.
More and more, the treatment of
addiction has become a multimodal integrated
treatment model utilizing trained specialists in
addiction medicine, counseling, behavioral
therapies, 12- step Self-Help modalities, and

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 3
alternative and complementary interventions
such as mindfulness, meditation, and
acupuncture. The role of the dietetics
professional, and the targeted nutritional
intervention as part of an integrated treatment
approach to the disease of addiction has not
been widely accepted and no formal programs
exist on a national or international level. Given
the stimulation of the dopamine D2 receptors
by food products it stands to reason that
nutritional interventions including dietary
optimization can play an important role in the
facilitation of normal brain physiology and
biochemistry in an effort to ensure a successful
launch into recovery.
Dopamine Deficiency Syndrome in
Addictions:
Dopamine Deficiency Syndrome (DDS)
also known as Reward Deficiency Syndrome
has been described before by others (Blum,
2011) (Volkow, 2007). Single Photon CT Scan
(SPECT) and Positron Emission Tomography
(PET) of the brain have been utilized to
extensively study the role of DDS in addiction,
particularly opioid addiction (Volkow, 2007).
These brain imaging studies have confirmed
that individuals with OPRD-1 and OPRM-1
genotypes are predisposed to not only
dopamine deficiency in the limbic system and

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 4
nucleus accumbens of the brain, but are also
susceptible to opioid and alcohol addiction
(Volkow, 2007). Dopamine deficiency
syndrome has also been associated with food
addiction (Volkow, 2007).
Individuals with DDS have been shown
to have reduced dopamine release (in the
physiological “pleasure centers” of the brain
including the nucleus accumbens and the limbic
system) and reduced dopamine metabolism in
response to normal “pleasurable stimuli” such
as food, sex, love, and normal physiologically
“satisfying stimuli” such as holding one’s
newborn baby, receiving recognition, or
interacting with nature (Volkow, 2007). Thus,
even as small children they never receive the
sensation of abject pleasure associated with the
normal physiological circumstances and events
that trigger the release of dopamine in the
limbic system (Volkow, 2007) (Blum, 2011).
Compounds such as simple sugar,
caffeine, and nicotine which are capable of
releasing dopamine in the limbic system of the
brain to the magnitude of 2-4 times more than
the normal physiologic release in response to
pleasurable stimuli become novel and create
intense sensations of euphoria and pleasure in
individuals with DDS (Blum, 2011). For the
first time in their lives these individuals with
DDS may experience a sensation of “normalcy”

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 5
and pleasure in response to sugar, caffeine, or
nicotine (Volkow, 2007) (Blum, 2011). This
then induces neuroplastic and neuro-adaptive
responses in the mesolimbic system and pre-
frontal cortex of the brain in individuals with
DDS, and dopamine release takes on “salience”
and the “brain expects it” (Volkow, 2007)
(Blum, 2011).
Children with DDS may exhibit
maladaptive behaviors such as overeating,
binge-eating, consuming and craving large
quantities of sugary foods and sugary beverages
(Volkow, 2007) (Blum, 2011). Additionally,
these children may exhibit pathologic behaviors
such as obsessively playing video games, or
“acting-out”.
Later in life if these susceptible
individuals with the genotypes for DDS are
exposed to alcohol or other drugs such as
marijuana, opioids, cocaine, or
methamphetamine, the neuroplastic and neuro-
adaptive changes in the mesolimbic system and
pre-frontal cortex become attenuated leading to
a pattern of craving and recurrent misuse. As
use continues, tolerance invariably develops,
thus more and more of the substance is required
to cause sufficient dopamine release. Additional
neuro-adaptive changes occur at a cellular
level, whereby, if the individual does not have
the drug in their system for a period of time,

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 6
they experience synaptic irritability and axonal
depolarization leading to the classic symptoms
of drug withdrawal (Volkow, 2007) (Blum,
2011). This then creates an intolerable
physiologic state to the individual wherein the
drug must be obtained at all costs to alleviate
the symptoms of withdrawal. Axonal
depolarization at the Dopamine D-2 receptor is
mediated by Na/K ATPase inhibition and leads
to severe depression, anxiety, insomnia, muscle
pain, tremor, intense fatigue, and possible
seizures (Rosen, Klintmam, et al., 2003).
Protracted use of these drugs and alcohol
can cause significant dopamine depletion
particularly in the Dopamine D-2 receptors, and
this is magnified by decreased dopamine
sensitivity at the synaptic end-plate (Rosen,
Klintmam, et al., 2003). Functional MRI (f-
MRI) and SPECT imaging during acute and
post-acute withdrawal demonstrate functional
depletion of dopamine metabolism in the limbic
system (Rosen, Klintmam, et al., 2003).
This state of dopamine depletion,
decreased dopamine sensitivity, and decreased
dopamine metabolism during acute and post-
acute withdrawal syndrome (PAWS) is the
primary mechanism behind relapse, and
represents the single most important barrier to
treatment success (Blum, 2011). This state of
dopamine depletion also represents a potential

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 7
breakthrough area for targeted nutritional
interventions that will be explored further in
this paper and Nutrition Research proposal.

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 8

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 9

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 10

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 11

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 12

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 13

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 14

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 15
THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 16

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 17

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 18

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 19

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 20

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 21

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 22

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 23

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 24
THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 25

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 26

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 27

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 28

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 29

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 30
THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 31
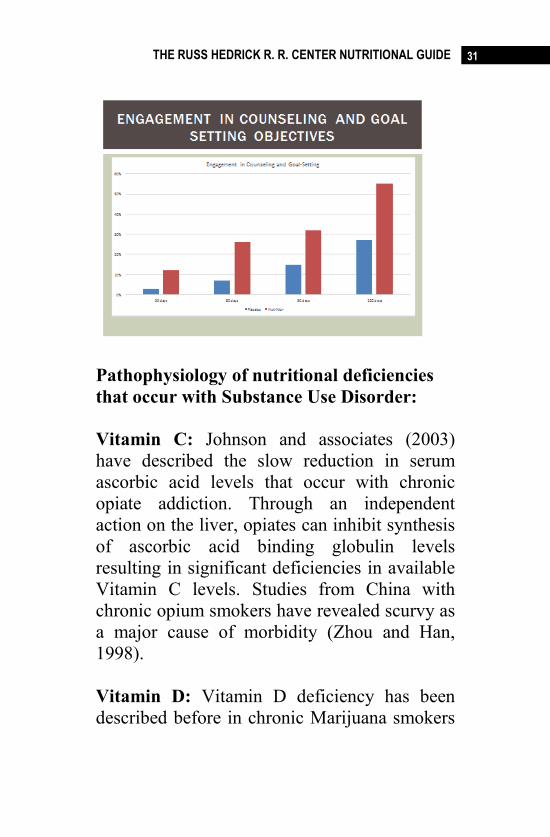
Pathophysiology of nutritional deficiencies
that occur with Substance Use Disorder:
Vitamin C: Johnson and associates (2003)
have described the slow reduction in serum
ascorbic acid levels that occur with chronic
opiate addiction. Through an independent
action on the liver, opiates can inhibit synthesis
of ascorbic acid binding globulin levels
resulting in significant deficiencies in available
Vitamin C levels. Studies from China with
chronic opium smokers have revealed scurvy as
a major cause of morbidity (Zhou and Han,
1998).
Vitamin D: Vitamin D deficiency has been
described before in chronic Marijuana smokers

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 32
(Chester, 2011). Vitamin D deficiency can lead
to accelerated osteoarthritis, osteopenia,
frequent fractures and altered immune status
with increased susceptibility to infections with
gram positive bacteria.
Vitamin B-12: Cyanocobalamin deficiency is
commonly found in cocaine and
methamphetamine users due to it being a
substrate in stimulant metabolic pathways
(Kolger, Murray, et al. 1998).
Folic Acid: Alcohol abuse can cause depletion
of folic acid leading to deficiency syndrome
with megaloblastic anemia and neurologic
sequelae such as alcohol-induced seizure
disorder (AISD) (Talbott, 2002).
Thiamine: Thiamine deficiency is common in
alcoholics and can lead to neuro-psychiatric
symptoms such as Wernicke-Korsakoff
syndrome, Wernickes’s encephalopathy, and
Korsakoff Psychosis. Cognitive impairment is
also a consequence of thiamine deficiency in
alcoholics (Talbott, 2002).
Zinc: Zinc deficiency is common in alcoholics
and lead to poor wound healing, prostate
problems, and accelerated development of
alcoholic liver disease (Talbott, 2002).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 33
Additionally, zinc deficiency attenuates opioid
withdrawal symptoms in chronic opioid abusers
(Talbott, 2002).
Magnesium: magnesium deficiency has been
well described in chronic alcoholics (Talbott,
2002). Proposed mechanisms for magnesium
deficiency include gastro-intestinal losses,
malabsorption and chelation. Additionally,
alcohol independently induces magnesium
excretion leading to profound hypomagnesemia
(Talbott, 2002). Symptoms of hypomagnesemia
include seizures, tremors, irritability, sleep
deprivation and concurrent refractory
hypokalemia (Talbott, 2002).
Protein deficiencies: Protein malnutrition has
been reported in both cocaine and
methamphetamine abusers (Mohs, 1990). The
profound anorexigenic effect of these stimulant
drugs leads to loss of appetite, decreased
protein intake, and decreased endogenous
protein synthesis in skeletal muscle (Mohs,
1990) leading to significant muscle wasting and
weight loss.
Alcoholics similarly are often protein deficient,
exhibiting serum hypoalbuminemia which
contributes to ascites, pleural effusions, and a
predisposition to enteric infections in ascetic
fluid (Talbott, 2002).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 34
Optimizing these nutritional deficiencies
is critical for successful recovery from opioid
and alcohol addiction (Blum, 2016).
Organization of the US Healthcare System
for Addictions Treatment:
The United States is currently
experiencing an epidemic. In 2016 more than
54,000 people died from opioid overdoses in
the United States. Currently deaths from opioid
overdoses exceed those from firearms and
automobile accidents combined (CDC, 2017).
According to the CDC approximately 144
people buying reading from opioid overdoses
(CDC, 2017).Synthetic drugs such as fentanyl,
carfentanyl, and acetyl- fentanyl are
increasingly mixed with heroin and brought in
to the US from Mexico by criminal drug cartels
(DEA, 2017).In October of 2017 President
Donald Trump declared a state of emergency to
deal with the opioid crisis. This has allowed
many new resources and innovative treatment
modalities to become widely integrated into the
Healthcare System. In spite of this surge in
resources and federal attention, and the death
rate from opioid overdoses continues to climb
(CDC, 2017). Many Federal authorities believe
that the true plateau of this epidemic has not
been reached yet.

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 35
Treatment for substance use disorder in
the United States broadly falls into two
categories: medical model and traditional
models. In October of 2016, the Surgeon
General of the United States addressed
Congress and declared addiction a chronic brain
disease and not a “moral failing” (US Surgeon
General Dr.Vivek Murthy, 2016). He
encouraged the Federal government and
physicians to recognize this and to adopt the
medical model of treatment for addiction.
The medical model of treatment involves
the use of detoxification, inpatient treatment,
intensive outpatient treatment, and medication
assisted treatment (MAT) (Rosen, Klintmam, et
al., 2003).Typically, detoxification is an
inpatient process in a medically supervised
setting. This is for those patients who are at-risk
of significant withdrawal symptoms up such as
seizures. Detoxification can last anywhere from
5 to 10 days. The usual inpatient treatment for
substance use disorder is 20 to 60 days long,
and is conducted in a formal treatment center
(Rosen, Klintmam, et al., 2003). Inpatient
treatment consists of the use of medications in
conjunction with counseling and behavioral
modification therapy. Intensive outpatient
therapy usually less from six months to a year
and is conducted by trained substance abuse
counselors (Rosen, Klintmam, et al., 2003).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 36
Medication assisted treatment (MAT) is
always medically supervised and conducted by
a Physician. The goals of medication assisted
treatment include preventing withdrawal
symptoms, reducing cravings, and facilitating
recovery. Medications that are utilized in this
form of treatment include methadone,
Suboxone, Vivitrol, Campral and Antabuse.
These forms of treatment often involve
replacing one addictive drug with another, and
are extremely expensive. The cost of Vivitrol
injection is $1100 per month (Alkemes, 2017).
The cost of 6 months of injectable
buprenorphine is $ 6400 (Alkemes, 2017).
Conversely, traditional addiction
treatment consists of mutual support meetings
including Alcoholics Anonymous, Narcotics
Anonymous, Cocaine Anonymous or faith-
based initiatives such as Celebrate Recovery or
Refuge Recovery (Fried, Febo, Waite, et al.,
2016).
What is Dopamine?
Dopamine is in neurotransmitter in the
central nervous system and an adrenergic
agonist in the peripheral nervous system (Blum,
2011). Dopamine produces psychotropic effects
including mood elevation, euphoria, satisfaction
and empathy in physiologic doses (Blum,

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 37
2011). Additionally, dopamine plays a role in
movement, blood pressure control and
temperature regulation. Dopamine is
synthesized from the amino acids L-tyrosine
and phenylalanine by the enzyme amino acid
decarboxylase (AADC), in the presence of
pyridoxal 5-phosphate, ionic zinc and
magnesium (Blum, 2011).
Adequate levels of bioavailable substrate
(L-tyrosine) and phenylalanine are needed to
synthesize dopamine in the central nervous
system. L-tyrosine and phenylalanine have
excellent bioavailability when given as an
intravenous infusion (2.75% Travasol Amino
Acid with Dextrose), and is rapidly taken up by
the adrenal glands and the central nervous
system (CNS) (Blum, 2016).
Central Nervous System Effects of
Dopamine Restoration:
Studies in opioid dependent patients
demonstrated excellent bioavailability of both
L-tyrosine and phenylalanine when consumed
orally both as a neuronutraceutical (Blum,
2011) and through consuming 0.8 gms/Kg of
protein containing whole foods (Volkow,
2015). Trachtenberg, Ramsey and associates
(2014) demonstrated increased central nervous
system metabolic restoration of dopamine in the

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 38
limbic system compared to controls after 8
weeks of a proprietary supplement containing
11mg of L-tyrosine and 170 mg of
phenylalanine, along with 51 mg of Magnesium
chloride, with 14 mg of zinc per serving
administered 4 times daily. This increased
dopamine restoration in the limbic system was
associated with decreased cravings, increased
program compliance, and greater sobriety at 1
year compared to controls.
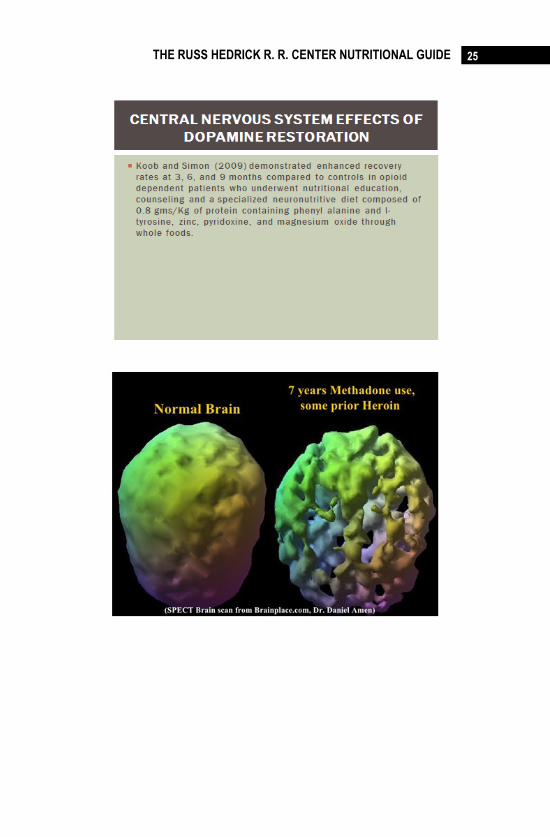
Koob and Simon (2009) demonstrated
enhanced recovery rates at 3, 6, and 9 months
compared to controls in opioid dependent
patients who underwent nutritional education,
counseling and a specialized neuronutritive diet
composed of 0.8 gms/Kg of protein, zinc,
pyridoxine, and magnesium oxide through
whole foods. Study subjects in this cohort were
not allowed to consume caffeinated beverages,
nicotine, or simple sugar containing products
for the first 90 days of the program.
Wiss (2016) studied the effects of an
extract of mucuna pruriens in opiate addicts,
and found that taking this extract 3 times a day
for 30 days boosted CNS dopamine levels
compared to controls in a small study.
Additionally, this extract was found to increase
levels of the neurotransmitter norepinephrine
which also plays an important role in mood and
depression (Wiss, 2016).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 39
A 2015 study by Ciubotariu and
associates demonstrated the positive effects of
zinc supplementation in opioid dependent
patients to increase dopamine levels and to
reduce symptoms of opioid withdrawal
(Ciubotariu, Ghiciuc, et al., 2015). Their study
demonstrated increased dopamine metabolism
in the nucleus accumbens by SPECT and f-MRI
imaging compared to controls.
In addition to dietary supplementation
with dopamine precursors and the use of
targeted whole foods to enhance dopamine
synthesis in the CNS, many studies have shown
the benefits of targeted nutrition education to
enhance long-term recovery. Empowering
patients with life-long learning related to
nutritional solutions to dopamine deficiency
syndrome have been shown to have positive
outcomes (Grant, Haughton, et al., 2004).
The Society for the Study of Addiction
(SSA, 2017) promotes the use of inpatient daily
intravenous infusions of amino acid complexes
containing L-tyrosine and phenylalanine in
addiction to zinc and magnesium for 30 days as
an adjunct to motivational interviewing and
cognitive behavioral therapy in treatment
centers endorsed by the organization (SSA,
2017).
Thus, there exists a large volume of
empirical research data on the importance of

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 40
dopamine deficiency syndrome in patients with
addiction, and the ability of whole foods
containing optimal levels of L-tyrosine and
phenylalanine along with zinc and magnesium
to optimize CNS dopamine levels in the limbic
system. Early optimization of CNS dopamine
levels are associated with improved outcomes
including sobriety and recovery. This stands in
stark contrast to the pharmaceutical industry
backed, medical model of addiction which
promotes the use of potentially harmful and
equally addictive pharmacologic products such
as Methadone and Suboxone.

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 41
Whole Foods High in l-Tyrosine
Cheese (Parmesan) Tyrosine
100g
Per ounce
(28g)
Per cubic inch
(10g)
1995mg
(228% RDI)
559mg
(64% RDI)
200mg
(23% RDI)
Other Cheeses High in Tyrosine (%RDI per
ounce): Gruyere (57%), Swiss (54%), Edam
(47%), Reduced-Fat Mozzarella (45%), Blue
Cheese (41%), Monterey & Hard Goat’s
Cheese (38%), and Cottage Cheese (21%).
Soy Foods (Roasted Soybeans) Tyrosine
100g
Per cup
(93g)
Per ounce
(28g)
1497mg
(171% RDI)
1392mg
(159% RDI)
419mg
(48% RDI)
Other Soy Foods High in Tyrosine (%RDI per
ounce): Koyadofu (Dried, Frozen Tofu) (51%),
Soy Flour (42%), Soy Chips (33%), Tempeh
(21%), Fried Tofu & Natto (18%), Sprouted
Soybeans, stir-fried (15%), and Silken Tofu
(10%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 42
Lean Beef & Lamb (Roast Beef) Tyrosine
100g
Per piece
(296g)
Per 3oz
(85g)
1386mg
(158% RDI)
4103mg
(469% RDI)
1178mg
(135% RDI)
Other Cuts of Beef & Lamb High in Tyrosine
(%RDI per 3oz, cooked): Grilled Steak (133%),
Beef Sirloin & Beef Ribs (127%), Beef
Tenderloin (122%), Lamb Shoulder (116%),
New Zealand & Australian Lamb (112%), and
Stewing Lamb 110%.
Lean Pork (Chops, cooked) Tyrosine
100g
Per chop
(180g)
Per 3oz
(85g)
1228mg
(140% RDI)
2210mg
(253% RDI)
1044mg
(119% RDI)
Other Cuts of Pork High in Tyrosine (%RDI
per 3oz, cooked): Bacon (150%), Low Fat
Ground Pork (130%), Pork Sirloin (117%),
Pork Ribs (112%), Ham (111%), Loin of Pork
(110%), Pork Tenderloin and Pork Shoulder
(103%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 43
Fish & Seafood (Salmon, cooked) Tyrosine
100g
Per 1/2 fillet
(155g)
Per 3oz
(85g)
1157mg
(132% RDI)
1793mg
(205% RDI)
983mg
(112% RDI)
Other Fish & Seafood High in Tyrosine (%RDI
per 3oz, cooked): Tuna (98%), Snapper (86%),
Mackerel (85%), Shrimp (84%), Halibut (83%),
Haddock (76%), Cod (66%), and Crab (64%).
Chicken & Turkey (Chicken Breast, cooked) Tyrosine
100g
Per breast
(181g)
Per 3oz
(85g)
1155mg
(132% RDI)
2091mg
(239% RDI)
982mg
(112% RDI)
Other Cuts of Chicken & Turkey High in
Tyrosine (%RDI per 3oz, cooked): Fat-Free
Ground Turkey (109%), Stewing Chicken
(108%), Turkey Breast (106%), Turkey Leg
Meat (105%), Chicken Wing (99%), Turkey
Wing (97%), Chicken Drumstick (94%) and
Turkey Drumstick (90%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 44
Seeds & Nuts (Pumpkin Seeds) Tyrosine
100g
Per cup
(129g)
Per ounce
(28g)
1093mg
(125% RDI)
1410mg
(161% RDI)
306mg
(35% RDI)
Other Seeds & Nuts High in Tyrosine (%RDI
per ounce): Peanuts (31%), Sesame Seeds
(24%), Sunflower Seeds (21%), Chia Seeds
(18%), Pine Nuts, Macadamia Nuts, Flaxseeds
& Pistachio Nuts (16%), and Almonds (14%).
Eggs & Dairy (Eggs) Tyrosine
100g
Per cup
(243g)
Per egg
(50g)
499mg
(57% RDI)
1213mg
(139% RDI)
250mg
(29% RDI)
Other Dairy Foods High in Tyrosine (%RDI per
cup):Fat-free Natural Yogurt (81%), Natural
Yogurt (49%), Skimmed Milk (48%), Semi-
Skimmed Milk (47%), Buttermilk (45%),
Whole Milk (44%), Sour Cream (34%), and
Butter (11%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 45
Beans & Lentils (White Beans, cooked)
Tyrosine
100g
Per cup
(179g)
Per tablespoon
(11g)
274mg
(31% RDI)
490mg
(56% RDI)
30mg
(3% RDI)
Other Beans & Lentils High in Tyrosine (%RDI
per cup, cooked): Adzuki Beans (59%), Lentils
(55%), Split Peas (54%), Roman (Cranberry)
Beans (53%), Kidney Beans & Black Beans
(49%), Broad Beans (Fava Beans) (47%), Pinto
Beans (46%), and Chickpeas (Garbanzo Beans)
(41%).
Wholegrains (Wild Rice, cooked)
Tyrosine
100g
Per cup
(164g)
Per 1/2 cup
(82g)
169mg
(19% RDI)
277mg
(32% RDI)
139mg
(16% RDI)
Other Wholegrains High in Tyrosine (%RDI
per cup, cooked): Raw Oats (102%), Teff
(38%), Kamut (27%), Brown Rice (22%),
Millet (21%), Bulgur (19%), Quinoa & Cous
Cous (18%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 46
Phenyalanine Rich Foods:
Soy Foods (Roasted Soybeans) Phenylalanine
100g
Per cup
(93g)
Per ounce
(28g)
2066mg
(236% RDI)
1921mg
(220% RDI)
578mg
(66% RDI)
Other Soy Foods High in Phenylalanine (%RDI
per ounce): Koyadofu (Dried, Frozen Tofu)
(75%), Soy Flour (58%), Soy Chips (44%),
Tempeh (29%), Sprouted Soybeans, stir-fried
(28%), Fried Tofu (27%), Boiled Soybeans
(18%) and Silken Tofu (14%).
Cheese (Parmesan) Phenylalanine
100g
Per ounce
(28g)
Per cubic inch
(10g)
1922mg
(220% RDI)
538mg
(61% RDI)
192mg
(22% RDI)
Other Cheeses High in Phenylalanine (%RDI
per ounce): Gruyere (56%), Swiss (53%), Edam
(46%), Monterey (41%), Reduced-Fat
Mozzarella & Colby (40%), Hard Goat’s
Cheese (39%), 8and Cottage Cheese (22%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 47
Seeds & Nuts (Pumpkin Seeds) Phenylalanine
100g
Per cup
(129g)
Per ounce
(28g)
1733mg
(198% RDI)
2236mg
(256% RDI)
485mg
(55% RDI)
Other Seeds & Nuts High in Phenylalanine
(%RDI per ounce):Watermelon Seeds (65%),
Peanuts (39%), Sunflower Seeds (38%),
Almonds (36%), Pistachio Nuts (35%), Chia
Seeds (32%), Flaxseeds (31%), Sesame Seeds
(30%), and Cashew Nuts (25%).
Lean Beef & Lamb (Roast Beef) Phenylalanine
100g
Per piece
(296g)
Per 3oz
(85g)
1464mg
(167% RDI)
4333mg
(495% RDI)
1244mg
(142% RDI)
Other Cuts of Beef & Lamb High in
Phenylalanine (%RDI per 3oz, cooked): Lamb
Shoulder & Beef Sirloin (141%), Australian &
New Zealand Lamb (135%), Beef Ribs (134%),
Stewing Lamb & Beef Rib Eye Steak (133%),
Beef Pot Roast (132%), and Beef Tenderloin
(129%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 48
Chicken & Turkey (Chicken Breast, cooked) Phenylalanine
100g
Per piece
(181g)
Per 3oz
(85g)
1294mg
(148% RDI)
2342mg
(268% RDI)
1100mg
(126% RDI)
Other Cuts of Chicken & Turkey High in
Phenylalanine (%RDI per 3oz, cooked):
Stewing Chicken (128%), Fat-Free Ground
Turkey (120%), Chicken Wings (117%),
Turkey Breast (110%), Chicken Thighs
(109%), Chicken Drumsticks & Turkey Leg
Meat (106%), and Turkey Wings (103%).
Lean Pork (Chops, cooked) Phenylalanine
100g
Per chop
(180g)
Per 3oz
(85g)
1288mg
(147% RDI)
2318mg
(265% RDI)
1095mg
(125% RDI)
Other Cuts of Pork High in Phenylalanine
(%RDI per 3oz, cooked):Bacon (157%), Low
Fat Ground Pork (131%), Pork Sirloin (123%),
Pork Tenderloin & Pork Ribs (118%), Ham
(114%), Loin of Pork (111%), and Pork
Shoulder (108%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 49
Fish & Seafood (Tuna, cooked) Phenylalanine
100g
Per 1/2 fillet
(154g)
Per 3oz
(85g)
1101mg
(126% RDI)
1696mg
(194% RDI)
936mg
(107% RDI)
Other Fish & Seafood High in Phenylalanine
(%RDI per 3oz, cooked):Lobster (108%),
Salmon (101%), Snapper (100%), Mackerel
(99%), Crab (97%), Halibut (96%), Haddock
(88%), and Cod (71%).
Eggs & Dairy (Eggs) Phenylalanine
100g
Per cup
(243g)
Per egg
(50g)
680mg
(78% RDI)
1652mg
(189% RDI)
340mg
(39% RDI)
Other Dairy Foods High in Phenylalanine
(%RDI per cup): Fat-free Natural Yogurt
(88%), Natural Yogurt (53%), Skimmed Milk
(49%), Semi-Skimmed Milk (48%), Buttermilk
(47%), Whole Milk (45%), and Sour Cream
(35%).
THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 50
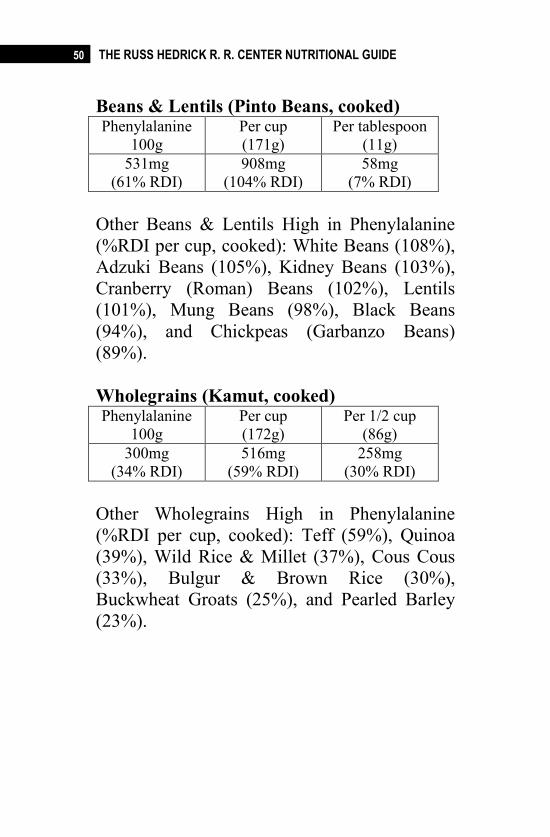
Beans & Lentils (Pinto Beans, cooked) Phenylalanine
100g
Per cup
(171g)
Per tablespoon
(11g)
531mg
(61% RDI)
908mg
(104% RDI)
58mg
(7% RDI)
Other Beans & Lentils High in Phenylalanine
(%RDI per cup, cooked): White Beans (108%),
Adzuki Beans (105%), Kidney Beans (103%),
Cranberry (Roman) Beans (102%), Lentils
(101%), Mung Beans (98%), Black Beans
(94%), and Chickpeas (Garbanzo Beans)
(89%).
Wholegrains (Kamut, cooked) Phenylalanine
100g
Per cup
(172g)
Per 1/2 cup
(86g)
300mg
(34% RDI)
516mg
(59% RDI)
258mg
(30% RDI)
Other Wholegrains High in Phenylalanine
(%RDI per cup, cooked): Teff (59%), Quinoa
(39%), Wild Rice & Millet (37%), Cous Cous
(33%), Bulgur & Brown Rice (30%),
Buckwheat Groats (25%), and Pearled Barley
(23%).

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 51
Magnesium Rich Foods
(Men RDA 400 milligrams and Women RDA
310 milligrams a day)
Spinach — 1 cup: 157 milligrams (40% DV)
Chard — 1 cup: 154 milligrams (38% DV)
Pumpkin seeds — 1/8 cup: 92 milligrams (23%
DV)
Yogurt or Kefir — 1 cup: 50 milligrams (13%
DV)
Almonds — 1 ounce: 80 milligrams (20% DV)
Black Beans — ½ cup: 60 milligrams (15%
DV)
Avocado — 1 medium: 58 milligrams (15%
DV)
Figs — ½ cup: 50 milligrams (13% DV)
Dark Chocolate — 1 square: 95 milligrams
(24% DV)
Banana — 1 medium: 32 milligrams (8% DV)
Other foods that are also high in magnesium
include: salmon, coriander, cashews, goat
cheese and artichokes.

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 52
Foods Rich in Zinc
Food
Milligrams (mg)
per
serving
Percent
DV*
Oysters, cooked, breaded and
fried, 3 ounces
74.0 493
Beef chuck roast, braised, 3
ounces
7.0 47
Crab, Alaska king, cooked, 3
ounces
6.5 43
Beef patty, broiled, 3 ounces 5.3 35
Breakfast cereal, fortified
with 25% of the DV for zinc,
¾ cup serving
3.8 25
Lobster, cooked, 3 ounces 3.4 23
Pork chop, loin, cooked, 3
ounces
2.9 19
2Baked beans, canned, plain
or vegetarian, ½ cup
2.9 19
Chicken, dark meat, cooked,
3 ounces
2.4 16
Yogurt, fruit, low fat, 8
ounces
1.7 11
Cashews, dry roasted, 1
ounce
1.6 11
Chickpeas, cooked, ½ cup 1.3 9
Cheese, Swiss, 1 ounce 1.2 8
Oatmeal, instant, plain,
prepared with water, 1 packet
1.1 7
Milk, low-fat or non- fat, 1
cup
1.0 7
Almonds, dry roasted, 1
ounce
0.9 6

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 53
Food
Milligrams (mg)
per
serving
Percent
DV*
Kidney beans, cooked, ½ cup 0.9 6
Chicken breast, roasted, skin
removed, ½ breast
0.9 6
Cheese, cheddar or
mozzarella, 1 ounce
0.9 6
Peas, green, frozen, cooked,
½ cup
0.5 3
Flounder or sole, cooked, 3
ounces
0.3 2
Sample Food for Dopaminergic Potentiation:
Fava Bean Dopamine Delights (Dr. Oz, 2017)
Makes 12 crostini
Ingredients:
12 brown rice crackers
3 tbsp extra virgin olive oil
Salt and freshly ground black pepper
1 cup fava beans, shelled
1/2 small Spanish onion
1 organic garlic clove
1 tbsp finely diced red pepper
10 black olives (pitted)
6 sprigs tarragon, leaves only
Directions:
THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 54
Cook the fava beans in boiling water for 2
minutes. Drain and rinse under cold running
water. Purée the beans in a food processor with
the onion, garlic, olives, the remaining 1 tbsp
olive oil, and the tarragon leaves. Season with
salt and pepper to taste.
Just before serving, spread the fava bean
paste onto the rice crackers. Garnish with the
diced red pepper and a sprinkling of black
pepper.
Menus will be developed by the RD to
ensure that each meal delivers the goals of
providing 0.8 gm/Kg of l-tyrosine and
phenylalanine, zinc, and magnesium while
avoiding caffeine and simple sugars in an effort
to provide adequate dopamine precursor
substrate to boost dopamine levels in the limbic
system.

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 55
References
1. Beheshti, A., Lucas, L., Dunz, T., Haydash,
M., Chiodi, H., Edmiston, B., Horzempa, J.
(2015). An Evaluation of Naloxone Use for
Opioid Overdoses in West Virginia: A
Literature Review. American Medical
Journal, 6(1), 9–13.
http://doi.org/10.3844/amjsp.2015.9.13
2. Blum, K., Febo, M., & Badgaiyan, R.
(2016). Fifty Years in the Development of a
Glutaminergic-Dopaminergic Optimization
Complex (KB220) to Balance Brain
Reward Circuitry in Reward Deficiency
Syndrome: A Pictorial. Austin Addiction
Sciences, 1(2), 1006.
3. Blum K, Gold MS. Neuro-chemical
activation of brain reward meso-limbic
circuitry is associated with relapse
prevention and drug hunger: a hypothesis.
Med Hypotheses. 2011;76:576–584.
[PubMed]
4. Blum K, Thompson B, Demotrovics Z,
Femino J, Giordano J, et al. The Molecular
Neurobiology of Twelve Steps Program &
Fellowship: Connecting the Dots for
Recovery. J Reward Defic Syndr.
2015;1:46–64. [PMC free article]
5. Blum K, Trachtenberg MC, Ramsay JC.
Improvement of inpatient treatment of the

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 56
alcoholic as a function of neurotransmitter
restoration: a pilot study. Int J Addict.
1988;23:991–998. [PubMed]
6. Blum, K., Whitney, D., Fried, L., Febo, M.,
Waite, R. L., Braverman, E. R., …
Badgaiyan, R. D. (2016). Hypothesizing
that a Pro-Dopaminergic Regulator
(KB220zTM
Liquid Variant) can Induce
“Dopamine Homeostasis” and Provide
Adjunctive Detoxification Benefits in
Opiate/Opioid Dependence. Clinical
Medical Reviews and Case Reports, 3(8),
125. http://doi.org/10.23937/2378-
3656/1410125
7. Brown RJ, Blum K, Trachtenberg MC.
Neurodynamics of relapse prevention: a
neuronutrient approach to outpatient DUI
offenders. J Psychoactive Drugs.
1990;22:173–187. [PubMed]
8. Ciubotariu, D., Ghiciuc, C. M., &
Lupușoru, C. E. (2015). Zinc involvement
in opioid addiction and analgesia – should
zinc supplementation be recommended for
opioid-treated persons? Substance Abuse
Treatment, Prevention, and Policy, 10, 29.
http://doi.org/10.1186/s13011-015-0025-2
9. Fernstrom JD. Large neutral amino acids:
dietary effects on brain neurochemistry and
function. Amino Acids. 2013;45(3):419–
430. [PubMed]

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 57
10. Gold MS, Badgaiyan RD, Blum K. A
Shared Molecular and Genetic Basis for
Food and Drug Addiction: Overcoming
Hypodopaminergic Trait/State by
Incorporating Dopamine Agonistic Therapy
in Psychiatry. Psychiatr Clin North Am.
2015;38:419–462. [PubMed]
11. Green, A. R., Aronson, J. K., & Cowen, P.
J. (1985). The pharmacokinetics of L-
tryptophan following its intravenous and
oral administration. British Journal of
Clinical Pharmacology, 20(4), 317–321.
12. Koob, G. F., & Simon, E. J. (2009). The
Neurobiology of Addiction: Where We
Have Been and Where We Are Going.
Journal of Drug Issues, 39(1), 115–132.
13. https://pdfs.semanticscholar.org/d545/18ef3
2aa87df79f92baac798e80366d3e129.pdf
14. Lindseth, G., Helland, B., & Caspers, J.
(2015). The Effects of Dietary Tryptophan
on Affective Disorders. Archives of
Psychiatric Nursing, 29(2), 102–107.
http://doi.org/10.1016/j.apnu. 2014.11.008
15. Miller, M., Chen, A. L., Stokes, S. D.,
Silverman, S., Bowirrat, A., Manka, M., …
Blum, K. (2012). Early Intervention of
Intravenous KB220IV- Neuroadaptagen
Amino-Acid Therapy (NAAT)TM
Improves
Behavioral Outcomes in a Residential
Addiction Treatment Program: A Pilot

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 58
Study. Journal of Psychoactive Drugs,
44(5), 398–409.
16. Massatti R, Beeghly C, Hall O, Kariisa M,
Potts L. Increasing heroin overdoses in
Ohio: Understanding the issue. Ohio
Department of Mental Health and
Addiction Services;
2014.http://mha.ohio.gov/portals/0/assets/re
search/reports/heroinoverdosereportfin4301
4.pdf.
17. Drug Abuse. Data for West Virginia.
Prescription Drug Abuse: Strategies to Stop
the Epidemic. 2013
http://healthyamericans.org/reports/drugabu
se2013/release.php?stateid=WV.
18. CDC. Making a difference by serving as a
model of prevention. Centers for Disease
Control and Prevention; 2014.
http://www.cdc.gov/injury/pressroom/press
releases/2014/pressrelease_pdo-
wvirginia.html.
19. McLaughlin T, Febo M, Badgaiyan RD,
Barh D, Dushaj K, Braverman ER, et al.
KB220Z™ a Pro-Dopamine Regulator
Associated with the Protracted, Alleviation
of Terrifying Lucid Dreams. Can We Infer
Neuroplasticity-induced Changes in the
Reward Circuit? J Reward Defic Syndr
Addict Sci. 2016; 2:3–13.

THE RUSS HEDRICK R. R. CENTER NUTRITIONAL GUIDE 59
20. Plunkett A, Kuehn D, Lenart M, Wilkinson
I. Opioid maintenance, weaning and
detoxification techniques: where we have
been, where we are now and what the
future holds. Pain Manag. 2013; 3:277–284.
[PubMed]
21. Purves D, Augustine GJ, Fitzpatrick D, et
al., editors. Neuroscience. 2nd edition.
Sunderland (MA): Sinauer Associates;
2001. GABA and Glycine.Available from:
https://www.ncbi.nlm.nih.gov/
books/NBK11084/
22. Sarkissian, C. N., Kang, T. S., Gámez, A.,
Scriver, C. R., & Stevens, R. C. (2011).
Evaluation of orally administered
PEGylated phenylalanine ammonia lyase in
mice for the treatment of Phenylketonuria.
Molecular Genetics and Metabolism,
104(3), 249–254.
http://doi.org/10.1016/j.ymgme.2011.06.01
6