toxicologic pathology - federal university of rio de janeiro diagnosis between... · society of...
TRANSCRIPT

http://tpx.sagepub.com/Toxicologic Pathology
http://tpx.sagepub.com/content/27/6/664The online version of this article can be found at:
DOI: 10.1177/019262339902700608
1999 27: 664Toxicol PatholTokunaga
Komyo Eto, Yukio Takizawa, Hirokatsu Akagi, Koichi Haraguchi, Shigeyuki Asano, Naohiko Takahata and HidehiroPathologic Point of View
Differential Diagnosis between Organic and Inorganic Mercury Poisoning in Human Cases-The
Published by:
http://www.sagepublications.com
On behalf of:
Society of Toxicologic Pathology
can be found at:Toxicologic PathologyAdditional services and information for
http://tpx.sagepub.com/cgi/alertsEmail Alerts:
http://tpx.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://tpx.sagepub.com/content/27/6/664.refs.htmlCitations:
What is This?
- Nov 1, 1999Version of Record >>
by guest on September 28, 2011tpx.sagepub.comDownloaded from

664
Differential Diagnosis between Organic and Inorganic MercuryPoisoning in Human Cases-The Pathologic Point of View*
KOMYO ETO,1 YUKIO TAKIZAWA,1 HIROKATSU AKAGI,1 KOICHI HARAGUCHI,1 SHIGEYUKI ASANO,2 NAOHIKO TAKAHATA,3 AND HIDEHIRO TOKUNAGA4
1National Institute for Minamata Disease, Minamata City, Kumamoto, Japan,2Department of Pathology, Iwaki Kyoritsu General Hospital, Fukushima, Japan,3Department of Psychiatry and Neurology, Sapporo Medical University, Hokkaido, Japan, and4Department of Surgical Pathology, Kumamoto University School of Medicine, Kumamoto, Japan
* Address correspondence and reprint request to: Dr. Komyo Eto,National Institute for Minamata Disease, Environment Agency, 4058-18, Hama, Minamata City, Kumamoto 867-0008, Japan; e-mail:[email protected].
ABSTRACT
Differences in pathology were found between acute and chronic exposure to methylmercury, mercury vapor, and inorganic mercury.Characteristic pathologic changes produced by organic mercury in the brain have previously been described in patients with Minamatadisease. The brains of patients who presented with acute onset of symptoms and died within 2-mo showed loss of neurons withreactive proliferation of glial cells, microcavitation, vascular congestion, petechial hemorrhage, and edema in the cerebral cortices,predominantly in the calcarine, pre- and postcentral, and transverse temporal cortices and in the cerebellar cortex. The neuropathologicchanges in the patients with acute onset of symptoms who survived for a long period (> 10 yr) were also included neuronal loss withreactive proliferation of glial cells in similar anatomic locations. The neuropathologic changes in patients with inorganic mercurypoisoning are quite different. Autopsies performed on 3 individuals with fatal cases of acute inorganic mercury poisoning who wereexposed to mercury vapor for about 2 wk revealed diffuse organized pneumonia, renal cortical necrosis, disseminated intravascularcoagulopathy, and infarctions in the brain and kidneys. In 2 other patients who worked in mercury mines for about 10 yr and whosuffered from chronic inorganic poisoning, no specific lesions were demonstrated in the brain. However, the assay and the histochem-istry of mercury revealed that inorganic mercury was present in the brain in all 3 groups irrespective of the brain lesions and theduration of clinical signs.
Keywords. Methylmercury; inorganic mercury; Minamata disease; human autopsy cases; pathology
INTRODUCTION
Minamata disease was first discovered about 40 yr ago,between 1953 and 1956. The disease was associated withthe intake of large amount of fish or shellfish contami-nated with methylmercury in Minamata Bay, as deter-mined by the study group from the Kumamoto UniversitySchool of Medicine. The pathology of Minamata diseasehas been described in detail in earlier reports (12, 14, 15,28, 30, 34, 41-43, 45-48) and reviews (10, 26, 27, 32,33, 35-39).
Recently, mercury pollution has resurfaced from thedumping of a large quantity of inorganic mercury in Bra-zil along the Amazon River (1-4, 8, 19). Exposure tomercury has also been reported in workers in gold minesin Tanzania (18), Indonesia (48), and the Philippines (un-published workshop).Many autopsy cases of Minamata disease are in the
files in Kumamoto Prefecture, Japan. There are also 2autopsy cases of chronic inorganic mercury poisoningsin workers in mercury mines in Hokkaido from 1967 to1968 (29). Recently, autopsies have been performed infatal cases of acute mercury vapor poisoning in IwakiCity, Fukushima Prefecture, Japan (6). It is important todistinguish pathologically between organic (methylmer-cury) and inorganic mercury poisoning.
-
Here, we report on the accumulation of mercury in thebrain and other organs and on the pathologic changes inthe brain.
MATERIALS AND METHODS
The autopsy findings and the result of histochemicalstudies were compared and reviewed in 3 groups of pa-tients. Acute inorganic mercury poisoning (Tables I andII) was found in a 64-yr-old man (IKH K-31) and a 50-yr-old man (IKH K-32) autopsied at Iwaki Kyoritsu Gen-eral Hospital (IKH) in 1993. These 2 patients were ex-posed to mercury vapor for 2-3 hr and developed symp-toms of acute inorganic mercury poisoning. Chronic in-organic mercury poisoning (Tables I and II) was foundin a 51-yr-old man (HU 594) and a 64-yr-old man (HU602), who were autopsied at Hokkaido University in1967 and 1968. These 2 patients had a history of chronicmercury vapor exposure for 9-10 yr. Organic mercury
TABLE I.-Autopsy cases of inorganic mercury poisoning.
Abbreviations: IKH = Iwaki Kyoritsu General Hospital; HU = Hokkaido Uni-versity.
by guest on September 28, 2011tpx.sagepub.comDownloaded from

665
TABLE H.-Mercury levels ()JLg/g) in the nervous system of individ-uals with inorganic mercury poisoning.
Abbreviations: IKH = Iwaki Kyoritsu General Hospital; HU = Hokkaido Uni-versity ; n.d. = not done.
° H. Akagi and Y. Haraguchi, unpublished observations, 1994.b Y Ohta, Tokyo Atomic Industrial Research, 1970 (cited in 29).
poisoning (Tables III and IV) was found in a 47-yr-oldman who died 45 days after acute onset (KU 3350), a23-yr-old woman who presented an acute onset but sur-vived for 18 yr (KU 6383), and a 71-yr-old man whoshowed a chronic onset and survived for 25 yr (KU7903). All 3 of these individuals were autopsied at Ku-mamoto University between 1959 and 1982.
Total mercury analysis of the nervous system and gen-eral organs was performed using flameless atomic ab-sorption spectrophotometry, and methylmercury analysisof the nervous system and general organs was performedby electron capture detector (ECD)-gas chromatography(44).Mercury in control cases was measured by Eto et al
(13). The levels of total mercury and methylmercury inthe cerebrum, cerebellum, liver, and kidney were mea-sured in the residents living in nonpolluted areas of Ku-mamoto Prefecture from June 1972 to August, 1973 andfrom October 1987 to September 1991.
For histochemical detection of mercury modified meth-ods of Sakai et al (24) and Tokunaga et al (50) were used.For histologic studies, hematoxylin and eosin, Klfver-Barrera (20), Bodian’s axon (7), and Holzer’s glial fiberstains (16) were used. The electron microscopic obser-vations were performed using a JEM-2000CX electronmicroscope (Nihon-Denshi Co., Tokyo).
TABLE III.-Three fatal cases of organic mercury poisoning (Mina-mata disease).
Abbreviation: KU = Kumamoto University.
TABLE IV.-Mercury levels (Rglg) in the nervous systems of indi-viduals with organic mercury poisoning (Minamata disease).
Abbreviations: KU = Kumamoto University; n.d. - not done.° Takeuchi and Eto (40).&dquo; Eto et a] (11).c Takeuchi et al (44).
RESULTS
Inorganic Mercury PoisoningFour autopsy cases of inorganic mercury poisoning
were examined, including 2 cases of acute inorganic mer-cury poisoning from short-term exposure to mercury va-por and 2 cases from prolonged exposure that resulted inlong survival (Table I). In the first man (IKH K-31), theaverage value of total mercury in the brain was 1.08 J.1g/g and that of methylmercury was 0.025 Rglg. In the sec-ond man (IKH K-32), the average value of total mercurywas 0.73 J.1g/g and that of methylmercury was 0.077 jig/g. In the brain of the third man (HU 594), the averagevalue of total mercury was 11.38 J-Lg/g, and that in thebrain of the fourth man (HU 602) was 10.82 J-Lg/g, asmeasured by Akagi’s method (5) and reported by Taka-hata et al (29) (Table II).
FIG. 1.-Decreased number of Purkinje and granule cells in the cer-ebellum of a man (IKH K-31 ) with acute inorganic mercury poisoning.Note bullous lesions, which are postmortem changes H&E. X60.
by guest on September 28, 2011tpx.sagepub.comDownloaded from
666
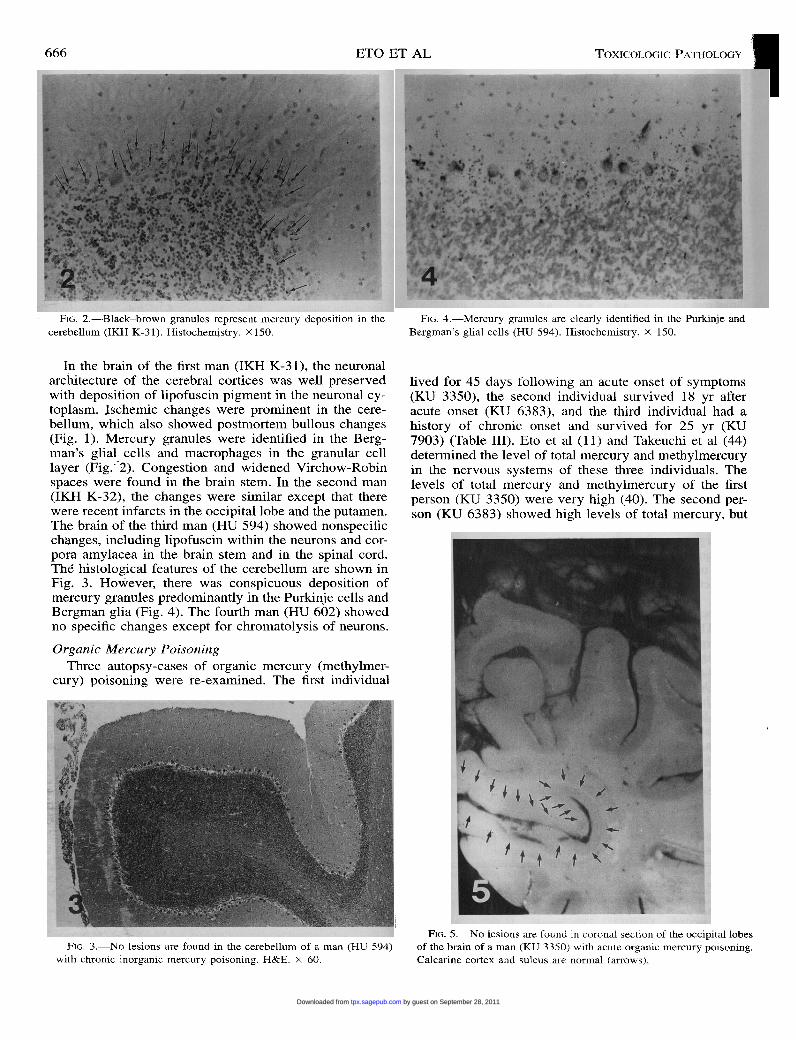
FIG. 2.-Black-brown granules represent mercury deposition in thecerebellum (IKH K-31). Histochemistry. X 150.
In the brain of the first man (IKH K-31), the neuronalarchitecture of the cerebral cortices was well preservedwith deposition of lipofuscin pigment in the neuronal cy-toplasm. Jschemic changes were prominent in the cere-bellum, which also showed postmortem bullous changes=(Fig. 1). Mercury granules were identified in the Berg-man’s glial cells and macrophages in the granular celllayer (Fig.~ 2). Congestion and widened Virchow-Robinspaces were found in the brain stem. In the second man
(IKH K-32), the changes were similar except that therewere recent infarcts in the occipital lobe and the putamen.The brain of the third man (HU 594) showed nonspecificchanges, including lipofuscin within the neurons and cor-pora amylacea in the brain stem and in the spinal cord.The histological features of the cerebellum are shown inFig. 3. However, there was conspicuous deposition ofmercury granules predominantly in the Purkinje cells andBergman glia (Fig. 4). The fourth man (HU 602) showedno specific changes except for chromatolysis of neurons.
Organic Mercury PoisoningThree autopsy-cases of organic mercury (methylmer-
cury) poisoning were re-examined. The first individual
FtG. 3.-No lesions are found in the cerebellum of a man (HU 594)with chronic inorganic mercury poisoning. H&E. X 60.
FIG. 4.-Mercury granules are clearly identified in the Purkinje andBergman’s glial cells (HU 594). Histochemistry. X 150.
lived for 45 days following an acute onset of symptoms(KU 3350), the second individual survived 18 yr afteracute onset (KU 6383), and the third individual had ahistory of chronic onset and survived for 25 yr (KU7903) (Table III). Eto et al (11) and Takeuchi et al (44)determined the level of total mercury and methylmercuryin the nervous systems of these three individuals. Thelevels of total mercury and methylmercury of the first
person (KU 3350) were very high (40). The second per-son (KU 6383) showed high levels of total mercury, but
I _
FIG. 5.-No lesions are found in coronal section of the occipital lobesof the brain of a man (KU 3350) with acute organic mercury poisoning.Calcarine cortex and sulcus are normal (arrows).
by guest on September 28, 2011tpx.sagepub.comDownloaded from

667
FIG. 6.-Decreased number of neurons with gliosis, microcavitation,and edema in the calcarine cortex (KU 3350). H&E. X 150.
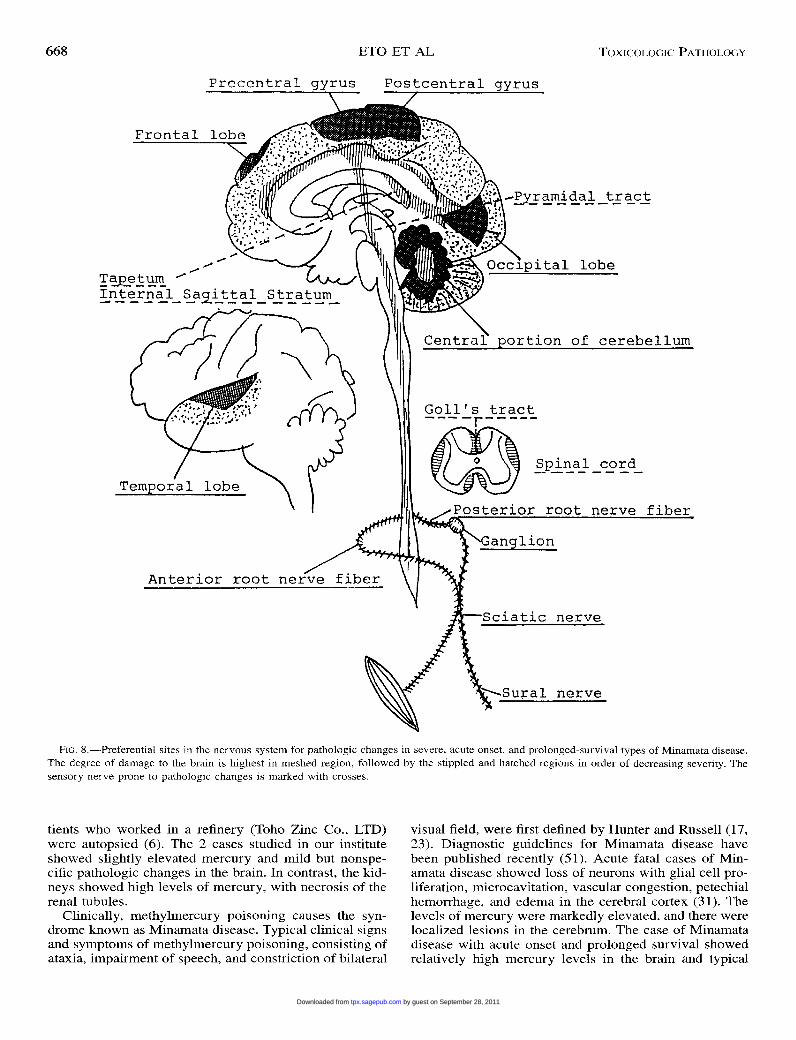
the methylmercury levels were low. The levels of totalmercury and methylmercury of the third person wereslightly higher than the average values of the control cas-es, which was determined in the residents of non-pollutedareas in Japan (Table IV). The brain of the first personweighed 1,300 g and was edematous. The calcarine cor-tices showed no atrophy (Fig. 5). Microscopically, therewas a decrease in the number of neurons, with glial pro-liferation, microcavitation, and edema in the calcarinecortex (Fig. 6). The second person with Minamata diseasewith acute onset and long-term survival (KU 6383)showed relatively unique localization of the pathologicchanges in the brain (Fig. 7). The calcarine cortex wasspongy, by light microscopy. The cerebellum showed al-most total loss of granules cells with preservation of Pur-kinje cells. Peripheral sensory nerves were damagedmore severely than were motor nerve fibers. Patients withacute onset and long survival always showed secondaryWallerian degeneration of the pyramidal tracts, internalsagittal stratum, and central parts of the cerebral whitematter. Secondary Wallerian degeneration of the pyra-midal tracts, predominantly in the lateral tracts also was
found in the spinal cord. The degeneration of the poste-rior columns, particularly of Goll’s tracts, was observedin prolonged cases, probably as a result of ganglion cellinvolvement in the posterior spinal ganglia and of pos-terior root nerve fiber damage (Fig. 8).
Both inorganic mercury as a vapor and organic mer-cury (methylmercury) entered into the brain diffusely,passing through the blood-brain barrier (Figs. 9 and 10).The mercury assay of general organs showed extremelyhigh total mercury in the kidneys. Total mercury in theliver, lung, and thyroid gland was relatively high in thefirst and third persons (Table V). However, the levels oftotal mercury in the kidney in the second person withMinamata disease (KU 6383) were higher than these inother organs (Table VI).
Normal Human Mercury Levels
Mercury contents in the cerebrum, cerebellum, liver,and kidney of residents living in areas of Kumamoto Pre-fecture, Japan, not polluted with mercury were measuredby Eto. et al (13) (Table VII).
DISCUSSION
Methylmercury and vapor of inorganic mercury easilypass through the blood-brain barrier and enter into thebrain tissue. A large quantity of inorganic mercury hasbeen used to make amalgam in gold mines. When themercury is heated up, it vaporizes and spreads into theatmosphere. The mercury vapor is inhaled and absorbedin the lung and enters the brain, passing through theblood-brain barrier, when gold miners are exposed, caus-ing inorganic mercury poisoning. Mercury chloride(HgCl,), a form of inorganic mercury, affects the epithe-lial cells of proximal tubuli of the kidney. Takahata et al(29) reported 2 cases of inorganic mercury poisoning.Both individuals had very high levels of mercury in thebrain, levels higher than those in acute cases of inorganicmercury poisoning after short-term exposure to mercuryvapor. However, no lesions were found. Clinically, thesepatients showed gingivitis, tremor, erethism, disturbanceof speech, delirium, and rigidity. In August 1993, 3 fatalcases of acute mercury vapor poisoning among 27 pa-
FIG. 7.-Occipital lobe (4 arrows), transverse temporal gyrus (3 arrows), pre- and postcentral gyri (2 arrows), and frontal lobe (1 arrow) of awoman (KU 6383) with acute organic mercury poisoning show severe cortical atrophy with subcortical gliosis. Holzer’s stain.
by guest on September 28, 2011tpx.sagepub.comDownloaded from
668
FIG. 8.-Preferential sites in the nervous system for pathologic changes in severe, acute onset, and prolonged-survival types of Minamata disease.The degree of damage to the brain is highest in meshed region, followed by the stippled and hatched regions in order of decreasing severity. Thesensory nerve prone to pathologic changes is marked with crosses.
tients who worked in a refinery (Toho Zinc Co., LTD)were autopsied (6). The 2 cases studied in our instituteshowed slightly elevated mercury and mild but nonspe-cific pathologic changes in the brain. In contrast, the kid-neys showed high levels of mercury, with necrosis of therenal tubules.
Clinically, methylmercury poisoning causes the syn-drome known as Minamata disease. Typical clinical signsand symptoms of methylmercury poisoning, consisting ofataxia, impairment of speech, and constriction of bilateral
visual field, were first defined by Hunter and Russell (17,23). Diagnostic guidelines for Minamata disease havebeen published recently (51). Acute fatal cases of Min-amata disease showed loss of neurons with glial cell pro-liferation, microcavitation, vascular congestion, petechialhemorrhage, and edema in the cerebral cortex (31). Thelevels of mercury were markedly elevated, and there werelocalized lesions in the cerebrum. The case of Minamatadisease with acute onset and prolonged survival showedrelatively high mercury levels in the brain and typical
by guest on September 28, 2011tpx.sagepub.comDownloaded from

669
FIG. 9.-Total mercury levels in different areas of cerebrum in a man
(IKH K-31) with acute inorganic mercury poisoning following short-term exposure to mercury vapor. From H. Akagi and Y. Haraguchi,unpublished observations, 1994.
lesions predominantly localized in the calcarine and cer-ebellar cortices. The chronic onset with prolonged sur-vival in 1 case of Minamata disease was associated with
mercury levels slightly higher than those of control cases(13). Mild localized lesions of the brain were also found.The histopathologic changes associated with organic
mercury poisoning were localized clearly in the nervoussystem, but those associated with the cases of inorganicmercury poisoning were not. The workers in mercurymines inhale vapor of metallic mercury, which easilypasses through blood-brain barrier and gains access intoneurons. Mercurial granules are taken into lysosomes andare deposited there (25). In contrast to the cases of meth-ylmercury intoxication, Nissl substance (ribosome) in theneurons is not damaged by inorganic mercury (14).Therefore, the neurons are not destroyed, even though arelatively large amount of inorganic mercury is depositedwithin the cells. Inorganic mercury can be detected byhistochemistry, but methylmercury can be identified onlywhen it transforms into inorganic mercury in some or-gans. The involvement of endoplasmic reticulum (9) andmicrotubules (21, 22), with preservation of mitochondria,was demonstrated by electron microscopy in cases of or-ganic mercury poisoning (12). In contrast, these organ-
I I
FIG. 10.-Total mercury levels (pLg/g) in different areas of cerebrumin a man (KU 7903) with chronic onset of Minamata disease with long-term survival [Takeuchi et al (44)] and the schematic representation ofthe distribution of mercury deposits in neurons (A) and phagocytes (*)as determined by histochemistry.
TABLE V.-Organ mercury levels ()JLg/g) in individuals with inorganicmercury poisoning. From H. Akagi and Y. Haraguchi, unpublished ob-servations, 1994.
Abbreviations: IKH = Iwaki Kyoritsu General Hospital; n.d. = not done.
by guest on September 28, 2011tpx.sagepub.comDownloaded from

670
TABLE VI.-Organ mercury levels (pglg) in an individual with mer-cury poisoning (Minamata disease). From Eto et al (11).
Abbreviations: KU = Kumamoto University; n.d. = not done.
elles were not involved in inorganic mercury poisoning,and instead numerous dense inclusions were found in the
cytoplasm (29).The results of these comparative studies between in-
organic and organic (methylmercury) poisoning of hu-mans in Japan showed that the levels of mercury in theorgans and the pathologic changes and clinical signs andsymptoms varied widely from case to case depending onthe exposed amounts and types of mercury. We hope thatour study will contribute to the differential diagnoses be-tween organic and inorganic poisoning in the mining op-erations of developing countries in the world.
TABLE VIL-Mean (±SD) total mercury (T Hg) and methylmercury(M Hg) levels (f.1g/g) determined at autopsy in organs of residents livingin nonpolluted areas.
ACKNOWLEDGMENTS
We extend our sincere appreciation to Dr. Tadao Tak-euchi, Professor Emeritus, Kumamoto University, for hiscontinuous support and advice and to the members of
Department of Pathology, Kumamoto University Schoolof Medicine, for their assistance at the autopsies. We alsothank Professor Cheng-Mei Shaw, Department of Neu-ropathology, University of Washington, for his helpfulcomments.
REFERENCES
1. Akagi H, Malm O, and Branches FJP (1996). Human exposure tomercury due to gold mining in the Amazon, Brazil—A review.
Environ. Sci. 7: 199-211.2. Akagi H, Malm O, Branches FJP, Kinjo Y, Kashima Y, Guimaraes
JRD, Oliveira RB, Haraguchi K, Pfeiffer WC, Takizawa Y, andKato H (1995). Human exposure to mercury due to goldmining inthe Tapajos River Basin, Amazon, Brazil: Speciation of mercuryin human hair, blood and urine. Water Air Soil Pollu. 80: 85-94.
3. Akagi H, Malm O, Kinjo Y, Harada M, Branches FJP, Pfeiffer WC,and Kato H (1993). Methylmercury pollution in Amazon, Brazil.Proc. Int. Symp. Assess. Environ. Pollu. Health Effects Methylmer-cury, pp. 41-48.
4. Akagi H, Malm O, Kinjo Y, Harada M, Branches FJP, Pfeiffer WC,and Kato H (1995). Methylmercury pollution in the Amazon, Bra-zil. Sci. Total Environ. 175: 85-95.
5. Akagi H and Nishimura H (1991). Speciation of mercury in theenvironment. In: Advances in Mercury Toxicology, T Suzuki (ed).Plenum, New York, pp. 53-76.
6. Asano S, Mochizuki M, Hasuike M, Kurisaki E, Gunji H, Sato H,and Eto K (1996). Accidental three fatal cases of acute mercuryvapor poisoning—Clinical and pathological study. Jpn. J. Toxicol.9: 423-426 (in Japanese).
7. Bodian P (1936). A new method for staining nerve fibers and nerveending in mounted paraffin section. Anat. Rec. 65: 89-97.
8. Branches F, Harada M, Akagi H, Malm O, Kato H, and PfeifferWC (1993). Human mercury contamination as a consequence ofgold mining activity in the Tapajos River Basin, Amazon, Brazil.Proc. Int. Symp. Assess. Environ. Pollut. Health Effects Methyl-mercury, pp. 19-32.
9. Cavanagh JB (1977). Metabolic mechanisms of neurotoxicitycaused by mercury. In: Neurotoxicology, Vol. 1, L Roizin, H Shi-raki, and N Grcevic (eds). Raven Press, New York, pp. 283-288.
10. Eto K (1997). Pathology of Minamata disease. Toxicol. Pathol. 25:614-623.
11. Eto K, Katsuragi S, and Takeuchi T (1976). An autopsy case ofchildhood Minamata disease: A long term survived case after anacute occurrence. Adv. Neurol. Sci. 20: 444-457 (in Japanese).
12. Eto K, Oyanagi S, Itai Y, Tokunaga H, Takizawa Y, and Suda I(1991). A fetal type of Minamata disease—An autopsy case reportwith special reference to the nervous system. Mol. Chem. Neuro-pathol. 16: 171-186.
13. Eto K, Suda I, Takizawa Y, Muto H, Tokunaga H, and Iwasaki H(1993). Studies on the mercury content and histochemistry of mer-cury in several organs from residents living in non-polluted areasof mercury from 1987 to 1991 in Kumamoto Prefecture and TokyoCity. J. Kumamoto Med. Soc. 67: 22-32 (in Japanese).
14. Eto K, and Takeuchi T (1977). Pathological changes of human suralnerves in Minamata disease (methylmercury poisoning). Light andelectron microscopic studies. Virchows Arch. B Cell Pathol. 23:109-128.
15. Eto K and Takeuchi T (1978). A pathological study of prolongedcases of Minamata disease, with particular reference to 83 autopsycases. Acta Pathol. Jpn. 28: 565-584.
16. Holzer W (1921). Über eine neue Methode des Gliafaserfärbung.Z. Ges. Neurol. Psychiatry. 69: 354-363.
17. Hunter D, and Russell DS (1954). Focal cerebral and cerebellar
by guest on September 28, 2011tpx.sagepub.comDownloaded from

671
atrophy in a human subject due to organic mercury compounds. J. Neurol. Neurosurg. Psychiatry. 17: 235-241.
18. Ikingura JR and Akagi H (1996). Monitoring of fish and humanexposure to mercury due to gold mining in the Lake Victoria gold-fields, Tanzania. Sci. Total Environ. 191: 59-68.
19. Kinjo Y, Akagi H, and Kato H (1993). Methods for epidemiologicalsurvey on environmental pollution by methylmercury originatingfrom gold mining activities. Proc. Int. Symp. Assess. Environ. Pol-lut. Health Effects Methylmercury. pp. 57-63.
20. Klüver H and Barrera E (1953). A method for the combined stain-ing of cells and fibers in the nervous system. J. Neuropathol. Exp.Neurol. 12: 400-403.
21. Miura K (1986). Mode of toxic action of methylmercury. In: RecentAdvances in Minamata Disease Studies.—Methylmercury Poison-ing in Minamata and Niigata, Japan, T Tsubaki and H Takahashi(eds). Kodansha, Tokyo, pp. 169-188.
22. Miura K and Imura N (1991). Microtubules: A susceptible targetof methylmercury cytotoxicity. In: Mercury Toxicology, T Suzuki(ed). Plenum Press, New York, pp. 241-253.
23. Pentschew A (1958). Quecksilbervergiftung. Handb. D. Spez. Path.Ant. Histol. B 13: 2007-2024.
24. Sakai K, Okabe M, Eto K, and Takeuchi T (1975). Histochemicaldemonstration of mercury in human tissue cells of Minamata dis-
ease by use of autoradiographic procedure. Acta Histochem. Cy-tochem. 8: 257-264.
25. Shirabe T, Eto K, and Takeuchi T (1979). Identification of mercuryin the brain of Minamata disease victims by electron microscopicX-ray microanalysis. Neurotoxicology 1: 349-356.
26. Shiraki H (1979). Neuropathological aspects of organic mercuryintoxication including Minamata disease. In: Handbook of ClinicalNeurology, Vol. 36, PJ Vinken and GW Bruyn (eds). North Hol-land, Amsterdam, pp. 83-145.
27. Shiraki H and Takeuchi T (1971). Minamata disease. In: Pathologyof Nervous System, Vol. II, J Minckler (ed). McGraw-Hill, NewYork, pp. 1651-1665.
28. Suda I, Eto K, Tokunaga H, Furusawa R, Suetomi K, and TakahashiH (1989). Different histochemical findings in the brain producedby mercuric chloride and methyl mercury chloride in rats. Neuro-toxicology 10: 113-126.
29. Takahata N, Hayashi H, Watanabe S, and Anso T (1970). Accu-mulation of mercury in the brains of two autopsy cases with chron-ic inorganic mercury poisoning. Folia Psychiatr Neurol. Jpn. 24:59-69.
30. Takeuchi T (1961). A pathological study of Minamata disease inJapan. In: Symposium of Geographic Neurology. International
Congress of Neurology, September 13, 1961, in Rome.31. Takeuchi T (1968). Pathology of Minamata disease. In: Minamata
Disease, Kumamoto University Study Group, Kutsuna M (ed). Shu-han, Kumamoto, Japan, pp. 141-256.
32. Takeuchi T (1972). Biological reactions and pathological changesin human beings and animals caused by organic mercury contam-ination. In: Environmental Mercury Contamination, R Hartung andBD Dinman (eds). Ann Arbor Science, Ann Arbor, Michigan, pp.247-289.
33. Takeuchi T (1977). Neuropathology of Minamata disease in Ku-mamoto, especially at the chronic stage. In: Neurotoxicology, Vol.1, L Roizin, H Shiraki, and N Grcevic (eds). Raven Press, NewYork, pp. 235-246.
34. Takeuchi T (1977). Pathology of fetal Minamata disease. Pediatri-cian 6: 69-87.
35. Takeuchi T (1979). Processes of pathological research to Minamatadisease. In: Minamata Disease, S Arima (ed). Seirinsha. Tokyo, pp.27-48 (in Japanese).
36. Takeuchi T (1985). Human effects of methyl mercury as an envi-ronmental neurotoxicant. In: Neurotoxicology, K Blum and L Man-zo (eds). Marcel Dekker, New York, pp. 345-367.
37. Takeuchi T and Eto K (1975). Minamata disease. In: Studies on theHealth Effects of Alkylmercury in Japan, Environmental Agency,Tokyo, pp. 28-62.
38. Takeuchi T and Eto K (1977). Pathology and pathogenesis of Min-amata disease. In: Minamata Disease: Methylmercury Poisoning inMinamata and Niigata, Japan, T Tsubaki and K Irukayama (eds).Kodansha, Tokyo, pp. 103-141.
39. Takeuchi T and Eto K (1986). Pathology of mild prolonged casesof Minamata disease. In: Recent Advances in Minamata Disease
Studies—Methylmercury Poisoning in Minamata and Niigata, Ja-pan, T Tsubaki and H Takahashi (eds). Kodansha, Tokyo, pp. 117-134.
40. Takeuchi T and Eto K (1999). The Pathology of Minamata Dis-ease—A Tragic Story of Water Pollution. Kyushu University Press,Fukuoka, Japan.
41. Takeuchi T, Eto K, Okabe M, Katsuragi S, and Miyajima H (1977).Grade and distribution of pathological lesions in the nervous sys-tem in Minamata disease, from observations of 72 autopsy and 6
biopsy cases. J. Kumamoto Med. Soc. 51: 216-231 (in Japanese).42. Takeuchi T, Eto K, Oyanagi S, and Miyajima H (1978). Ultrastruc-
tural changes in human sural nerves in the neuropathy induced byintrauterine methylmercury poisoning. Virchows Arch. B Cell
Pathol. 27: 137-154.43. Takeuchi T, Eto K, and Tokunaga H (1989). Concept of methyl-
mercury-induced hydrargyria from the view point of histochemis-try. Bull. Shokei Women’s Junior College 21 : 15-29 (in Japanese).
44. Takeuchi T, Eto K, and Tokunaga H (1989). Mercury level andhistochemical distribution in a human brain with Minamata disease
following a long-term clinical course of twenty-six years. Neuro-toxicology 10: 651-658.
45. Takeuchi T, Eto N, and Eto K (1979). Neuropathology of childhoodcases of methylmercury poisoning (Minamata disease) with pro-longed symptoms, with particular reference to the decorticationsyndrome. Neurotoxicology 1: 1-20.
46. Takeuchi T, Kambara T, Morikawa N, Matsumoto H, and Murao M
(1958). Pathological studies on encephalopathia from unknowncause in Minamata district of Kumamoto Prefecture (the so-calledMinamata disease) in Japan. Acta Pathol. Jpn. 7(suppl.): 607-611.
47. Takeuchi T, Kambara T, Morikawa N, Matsumoto H, Shiraishi Y,and Ito H (1959). Pathologic observations of the Minamata disease.Acta Pathol. Jpn. 9 (suppl.): 769-783.
48. Takeuchi T, Morikawa N, Matsumoto H, and Shiraishi Y (1962).A pathological study of Minamata disease in Japan. Acta Neuro-pathol. 2: 40-57.
49. Takizawa Y (ed) (1996). Proceedings of the International Work-shop on the Fate of Mercury in Gold Mining and Measures toControl the Environmental Pollution in Various Countries. Nation-
al Institute for Minamata Disease, Minamata, Kumamoto, Japan.50. Tokunaga H, Furusawa R, and Eto K (1988). Identification of mer-
cury granules from pigments in tissues by photoemulsion method.Pathol. Clin. Med. 6: 845-848 (in Japanese).
51. Tsubaki T and Takahashi H (eds) (1986). Recent Advances in Min-amata Disease Studies—Methylmercury Poisoning in Minamata
and Niigata, Japan. Kodansha, Tokyo, pp. 207-210.
by guest on September 28, 2011tpx.sagepub.comDownloaded from