trattamento conservativo delle lesioni pre-neoplastiche e · diagnosis and counselling with regard...
TRANSCRIPT
04/06/2015
Trattamento conservativo delle lesioni pre-neoplastiche e
neoplastiche dell’endometrioDr Valeria Masciullo
Divisione di Ginecologia Oncologica

Rationale
The subfertility of this population is often due to the same risk factors
associated with the development of endometrial carcinoma: polycistic
ovarian syndrome, ovarian disfunction, chronic anovulation, obesity and
hyperinsulinemia
Many women diagnosed EC and AH have a strong desire to preserve
fertility therefore conservative treatment should be offered to these
patients
3-5% of women diagnosed with endometrial cancer (EC) and atypical
hyperplasia (AH) are under the age of 40, of these 70% are nulliparous
Hormone therapy is usually administered to promote remission and allow
pregnancy: medroxyprogesterone acetate (MPA), megestrol acetate
(MA), intrauterine devices containing progestogen
Absence of Guidelines concerning the management and
prognosis of conservative AH and EC treatments

Women with desire of childbearing;
Women who suffer from medical comorbidities;
Women at high risk for surgical complications.

The optimal dose, duration and regimen
for conservative treatment are unclear
MPA and MGA give similar results
MPA doses (400 mg/day) may be sufficient for
conservative therapy for grade 1 EA and reduce the risk
of vascular events
Both MPA and MGA are effective over a variety of
dosages and schedules
Other treatments include: 17αa-hydroxyprogesterone
caproate, oxyprogesterone acetate,
hydroxyprogesterone, norethisterone and tamoxifen.

MPA 44%
Megestrol acetate 35%
17alpha-OH-progesterone 5%
Oxyprogesterone acetate 4%
OH-progesterone acetate 4%
Norethindrone 3%
Unspecified 3%
Norethindrone/mestranol 1%
Medrogestone 1%
PROGESTINS USED FOR TREATMENT OF EARLY
GRADE 1 EC (n=81):
Ramirez, 2004

quadro istologico di atrofia della componente
ghiandolare;
edema e decidualizzazione dello stroma;
assottigliamento della mucosa;
conversione dell'epitelio ghiandolare in cilindrico
monostratificato senza mitosi;
remissione di quadri di iperplasia;
riduzione dello spessore endometriale a 2 – 3 mm.
Razionale per l’uso dei progestinici

MEDROXYPROGESTERONE ACETATE (MAP)
Brand name: Provera, Depoprovera, Farlutal
Dose: 200-800 mg for 26 weeks
Side effects: Fluid retention
Vaginal bleeding
Muscle cramps
Skin rashes
Breast changes
Blood clots
Blood sugar levels

Multicenter Phase II Study of Fertility-Sparing Treatment With
Medroxyprogesterone Acetate for Endometrial Carcinoma and Atypical
Hyperplasia in Young Women
Ushijima K et al. Japan Gynecologic Cancer Study
Group
JOURNAL OF CLINICAL ONCOLOGYVOLUME 25 NUMBER 19 JULY 1, 2007
,


RESULTS
Complete response was found in 55% of
EC cases and 82% of AH cases.
14 recurrences were found in 30 patients
(47%) between 7 and 36 months.

Treatment and follow-up outcomes
Months after initial MPA treatment
0 12 24 36 48 60 72 84 96 108 120 132
T.Yahata et al, Human Reproduction, 2005

MEGESTROL ACETATE (MA)
Brand name: Megace
Dose: 160 mg
Side effects: Weight Gain
Tromboembolic phenomena
Glucocorticoid effects
Dyspnea
Alopecia
Hypertension
Carpal tunnel syndrome

Treatment and follow up outcomes
Megestrol acetate should be the preferred
treatment because it is associated with a
better remission probability and a lower
progression rate
The treatment period should not exceed 12
months because the remission probability does
not increase after 1 year
Koskas M, Fert and Ster 2014
Levonorgestrel-releasing
intrauterine system (20 mcg 24 hr)
Management of patients with non-atypical and
atypical endometrial hyperplasia with a
levonorgestrel-releasing intrauterine system: Long
term follow-up
Wildemeersch et al.
Maturitas 57 (2007): 210-213

High local concentration
Low systemic absorption
3
months
86%reduction
12
months
97% reduction
50 % amenorrhea
Levonorgestrel-releasingintrauterine system

Systemic effects
Plasma concentration of LVG remains stable and is lower than oral
therapy
Suhonen SP, Fert Ster 1995; 63:336-342

LVG-IUD oral LNG
30 µg/24 hr 2 mg E2/250 µg LVG
Endometrium (ng) 808 ± 511 3.5
Miometrium (ng) 2.43 ± 1 .86 1.42 ± 0.46
Fallopian tubes (ng) 1.8 1.7
Plasma (ng) 0.1-0.2 1.7
C.G.Nilsson, Clinical Endocrinology (1982) 17,529-536
LVG-IUD: systemic effects

Contraindication
Patient with previous TVP
Patient with myoma SM G0
Obese patient and smoker
Patients with diagnosis of diabetes mellitus

Side effects
•Intermenstrual bleeding 12%
• Weight gain 17%
• Acne 10%
• Mood disorders 3%
• Decreased libido 2%
• Swollen legs 1%
• Hypertension 1%
Breast tenderness is the most frequent

Receptor status
The absence of progesterone receptor might
be related to the failure of progestin treatment.
The response rate of MPA in patients with
advanced or recurrent endometrial carcinoma
is 37% for those with PR + status and 8% for those
with a PR - status.
Thigpen et al, 1999

Progression of the disease during
conservative treatment
Diagnosis and counselling with regard to the
potential risks with progression of the disease are
mandatory when continuing or re-starting
treatment.
A pre-treatment laparoscopic procedure
including adnexal exploration and peritoneal
cytology is proposed to verify the absence of
extrauterine disease.
Morice et al., 2005


There is no standard recommendation
for the appropriate timing to
pathologically evaluate response by
progestins
The mean time to response is reported at 2-6
months with a minimal time to response in most
studies of 3 months.(Kempson et al., Cancer 1968)
The standard method for evaluating the initial
response should be a D&C (dilatation and curettage),
which may have therapeutic as well as diagnostic
purposes, after 3 months treatment by MPA.
(Yamazawa et al, Human Reproduction 2006)

Interpretation of pathological
specimens obtained during the
treatment course
There are not strict pathological criteria to
assess response by progestin and
considered only the absence of
endometrial adenocarcinoma and
atypical hyperplasia as a complete
response regardless of hormonal effects.
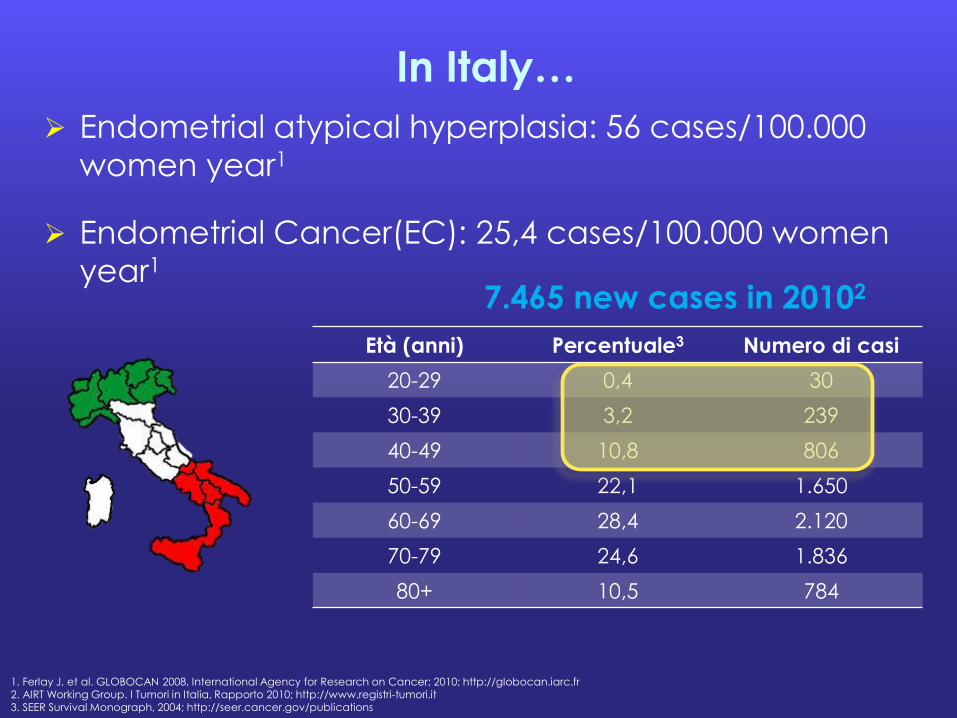
In Italy…
Endometrial atypical hyperplasia: 56 cases/100.000
women year1
Endometrial Cancer(EC): 25,4 cases/100.000 women
year1
Età (anni) Percentuale3 Numero di casi
20-29 0,4 30
30-39 3,2 239
40-49 10,8 806
50-59 22,1 1.650
60-69 28,4 2.120
70-79 24,6 1.836
80+ 10,5 784
7.465 new cases in 20102
1. Ferlay J, et al. GLOBOCAN 2008, International Agency for Research on Cancer; 2010; http://globocan.iarc.fr2. AIRT Working Group. I Tumori in Italia, Rapporto 2010; http://www.registri-tumori.it3. SEER Survival Monograph, 2004; http://seer.cancer.gov/publications

Background
cell growth
tissue invasion
adhesions molecules
secretive fenotype differentiation
senescence
There is no consensus on the ideal type of progestin
4. Dai D, et al. Cancer Res 2002;62:881-8865. Mazzon I et al. Int J Gynecol Cancer 2005;15:974-8
Progestin4
Histeroscopic removal of the tumor may represent, in selected patients,
an additional advantage
Medical therapy Surgical therapy


Aims of the study
1. To estabilish guidelines concerning the managment
and prognosis of conservative AH and EC treatments;
2. To assess response to therapy;
3. To evaluate side effects;
4. To assess compliance to therapy;
5. To study recurrence and progression probability ;
6. To study reproductive outcomes as pregnancy rate;
7. To evaluate quality of life of these patients

Materiali e Metodi
Multicentrico (3 Centri)
Prospettico
Ottobre 2006 – Febbraio 2013
43 pazienti consecutive
Isteroscopia + biopsia per:
PEA (14/43; 32,6%),
Sospetto ecografico (16/43; 37,2%)
Sterilità primaria (13/43; 30,2%)

43 pazienti
Iperplasia atipica(n=24)
Ca. endometrio(n=19)
Counseling
•EC G3
•Paura
•Regressione
•Pluriparità
•Paura
•Perse (n=2)
Iperplasia atipica(n=19)
Ca. endometrio(n=17)
MRI
Caratteristiche delle pazienti
Materiali e Metodi

Criteri di inclusione
CRITERI ONCOLOGICI:
1. Paziente in età fertile;
2. Forte desiderio riproduttivo;
3. Non controindicazioni alla terapia progestinica ad alte dosi;
4. Diagnosi di AH o EC endometrioide G1 (FIGO IA) mediante adeguata biopsia in corso di isteroscopia

CRITERI RESETTOSCOPICI6:
1. Lesione unifocale;
2. Dimensioni della lesione < 2 cm
3. Aggredibilità mediante resettoscopia
6. Mazzon I et al. Int J Gynecol Cancer 2005;15:974-8

Ca. endometrio
(n=17)
Iperplasia
atipica
(n=19)
Trattamento
chirurgico
(n=6)
Trattamento medico
MEGESTROLO AC. 160mg/die(n=17)
Isteroscopia + biopsia (ogni 3 mesi)
Qualità della vita (EORTC QLQ-C30)
Stato psichico (HADS)
Abitudini di vita

Ricerca di gravidanza
FOLLOW-UP
ogni 3 mesi:
Isteroscopia + biopsia
Ecografia TV
RISPOSTA COMPLETA
(6 mesi)
Isteroscopia + biopsia
RISPOSTA INIZIALE
(3 mesi)
Isteroscopia + biopsia
Iperplasia
atipica
(n=19)
Risposta iniziale
(n=17)
Risposta
completa
(n=12)
Persistenza
(n=3)
(1 N.V. e 1 persistenza)
(4 in corso)
Ca. endometrio
(n=17)
Risposta iniziale
(n=11)
Risposta
completa
(n=15)
Persistenza
(n=2)
(1 N.V. e 5 persistenza)

Ca. endometrio
(n=17)
Risposta iniziale
(n=11)
Risposta
completa
(n=15)
Persistenza
(n=2)RISPOSTA COMPLETA
(6 mesi)
Isteroscopia + biopsia
Iperplasia
atipica
(n=19)
RISPOSTA INIZIALE
(3 mesi)
Isteroscopia + biopsia
Risposta iniziale
(n=17)
Risposta
completa
(n=12)
Persistenza
(n=3)
(1 persa e 1 persistenza)
(4 in corso)
(1 persa e 5 persistenza)
MEGESTROLO AC. 160 mg/die
Risposta completa (n=2)
In corso (n=1)
TRATTAMENTO CHIRURGICO
STANDARD
EI: Adk. endometrioide G1 (FIGO IA) (n=2)
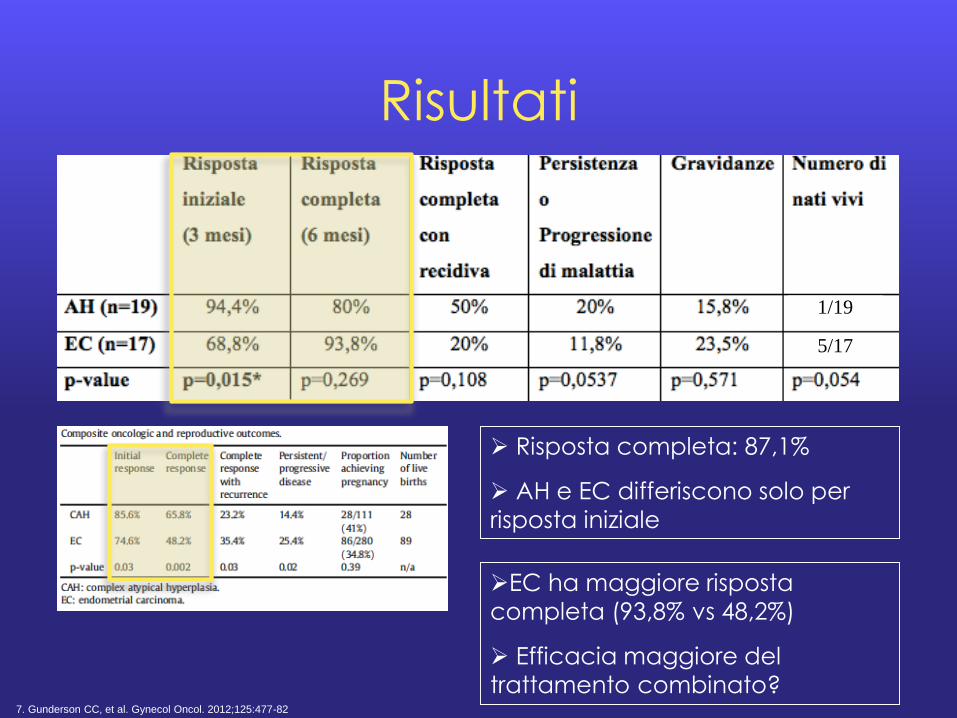
Risultati
Risposta completa: 87,1%
AH e EC differiscono solo per
risposta iniziale
1/19
5/17
EC ha maggiore risposta
completa (93,8% vs 48,2%)
Efficacia maggiore del
trattamento combinato?7. Gunderson CC, et al. Gynecol Oncol. 2012;125:477-82

Risultati
Risposta completa: 87,1%
AH e EC differiscono solo per
risposta iniziale
1/19
5/17
EC ha maggiore risposta
completa (93,8% vs 48,2%)
Efficacia maggiore del
trattamento combinato?
Trattamento Risposta completa
Recidiva
Medico (n=11)
81,8% 22,2%
Combinato (n=6)
100% 16,7%
p-value p<0,001 p=0,809

Risultati
1/19
5/17
Recidiva: 33,3%
AH ha maggiore recidiva di EC
Comportamento biologico diverso9?
Recidiva di AH correla con timing della gravidanza
Se concepimento non immediato10,11: recidiva 40-47%
8. Gunderson CC, et al. Gynecol Oncol. 2012;125:477-82
9. Trimble CL, et al. Cancer 2006;106:812–9
10. Ushijima K, et al. J Clin Oncol 2007;25:2798-2803
11. Hahn HS,e t al. Int J Gynecol Cancer 2009;19:1068–1073

?
Recidiva e trattamento
Ramirez et al: 72%
di risposta al trattamento della
recidiva12
Trattamento
progestinico di
seconda linea:
75% di risposta
12. Ramirez PT, et al. Gynecol Oncol. 2004;95:133-8
13. Gallos ID, et al. Am J Obstet Gynecolo 2012;207:266.e1-12
EI: Ca. ovarico
endometrioide G2
sincrono (1/43; 2,7%)
Gallos et al: 3,6%
neoplasia ovarica
sincrona13

Risultati
1/19
5/17
Il minor numero di recidive di EC
Diverso follow-up AH (12 mesi) vs
EC (24 mesi)
Coesistenza di PCO, obesità,
anovularietà cronica
Più gravidanze dopo PMA
Effetto protettivo della gravidanza?14. Gunderson CC, et al. Gynecol Oncol. 2012;125:477-82

Qualità della vita (QoL)
“... la percezione dell’individuo della sua posizione nella
vita, nel contesto della cultura e del sistema di valori in cui
vive ed in relazione ai suoi obiettivi, alle sue aspettative, ai
suoi modelli e rapporti ..." (OMS, 1993)
E' uno degli end point, insieme a DFS e OS, per valutare i
risultati dei trattamenti oncologici15
European Organization for
Research and Treatment of
Cancer Core Quality of Life Questionnaire (EORTC QLQ-C30)
e ̀ un questionario specifico per
adulti affetti da neoplasia, che
indaga diverse aree della QoL
attraverso 30 domande
15. Bifulco G, et al. Gynecol Oncol. 2012;124:444-51


Stato psichico
La diagnosi di neoplasia ginecologica ha un impatto
negativo sullo stile di vita, sul lavoro, sulla sessualità,
sull’immagine corporea e sul potenziale riproduttivo con
conseguente stress emotivo, ansia cronica e alterazione
comportamentale16
Il questionario Hospital Anxiety and Depression Scale (HADS) valuta il livello di ansia e depressione delle pazienti
attraverso 14 domande (score 0-3)
Cut-off: 8 su 21 per ansia
e depressione
patologiche17
16. Bifulco G, et al. Gynecol Oncol. 2012;124:444-51
17. Bjelland I, et al. J Psychosom Res. 2002;52:69-77

Stato psichico
Durante il follow-up meno pazienti presentano ansia patologica
Effetto depressivo del progestinico?
Score di ansia
Persistenza/Progressione
Risposta completa
8 5,5% 11,1%
< 8 11,1% 72,2%
Ansia correla all'andamento di malattia (p=0,002)

Stato psichico
Non ci sono modificazioni relative alla depressione
nè in numero di diagnosi, nè nello score
Poche pazienti per valutare la correlazione
con l'andamento della malattia

Conclusioni/1
AH e EC sono rare in età fertile
Terapia medica e combinata sono efficaci nel
trattamento conservativo di pazienti selezionate e con
desiderio riproduttivo
Megestrolo ac. (MA) 160 mg/die è ben tollerato
Risposta completa: 87,1% pazienti
Recidiva: 33,3% pazienti
E' possibile un trattamento progestinico di seconda
linea con MA o Mirena con una risposta del 75%

Conclusioni/2
Purtroppo non ci sono fattori predittivi di risposta
Conclusioni/3
Questo ribadisce l'importanza di un follow-up stretto
Solleva il problema dell'opportunità di una terapia di
mantenimento nelle pazienti che non abbiano un
desiderio riproduttivo immediato
Conferma la necessità di eseguire un trattamento
chirurgico standard al termine del ciclo riproduttivo

Comparazione di costi
DRG 354 COSTI
ISTEREC LPT 5988,84 5667,33
ISTEREC LPS 5988,84 5003,00
ISTEREC VAG 5988,84 5494,56
RESETTOSCOPIA 5988,84 1534,00

