what is being done where endovascular treatment of infrarenal abdominal aortic aneurysm with short...
TRANSCRIPT
What Is Being Done Where
Endovascular Treatment of Infrarenal Abdominal Aortic Aneurysm with Short and Angulated Neck
in High-Risk Patient-Greece-
E. Rose, M.D., 7/27/2013

Introduction
Endovascular treatment of Abdominal Aortic Aneurysms (AAA) associated with lower operative risk, shorter OR time
Aortic morphology may affect choice of open vs. closed treatment
Short or angulated proximal neck also makes open repair more difficult
Very sick patient with multiple comorbidities much more likely to die on the table
Case Report
77 year-old male, sudden onset abdominal pain radiating to back.
CT abdomen revealed infrarenal AAA, maximum diameter 9 cm.
Multiple comorbidities, including CABG, subsequent removal of sternum for infection, subsequent MI X 2
Too high risk for open repair
Koutsias S, Antoniou G, Karathanos C, et al. Case Report: Endovascular Treatment of Infrarenal Abdominal Aortic Aneurysm with Short and Angulated Neck in High-RiskPatient. Case Reports in Vascular Medicine 2013, http://dx.doi.org/10/1155/2013/898024.

DSA Arteriography
DSA arteriography that shows the short and angulated neck of the AAA.
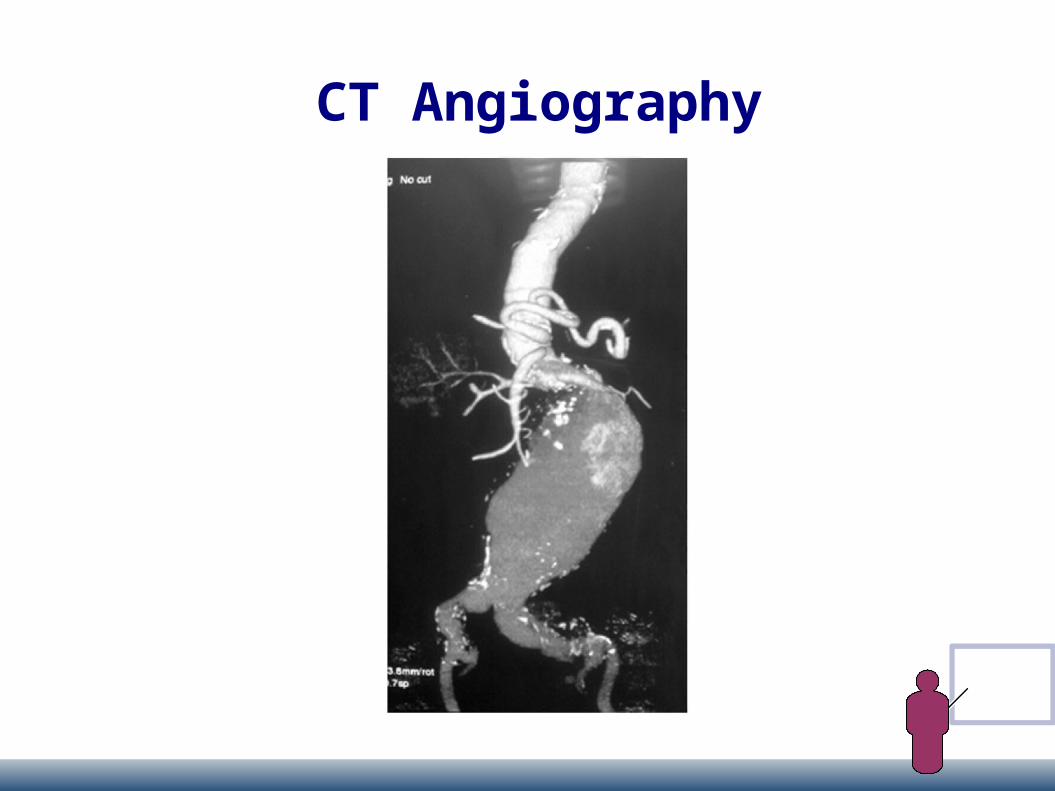
CT Angiography

Procedure
30 mm diameter free flow thoracic tube endograft (Valiant) implanted in proximal neck
Bifurcated Talent device inserted inside Valiant graft with overlapping
Two sequential iliac extensions in left external iliac artery, one to the right
Patient survived the procedure
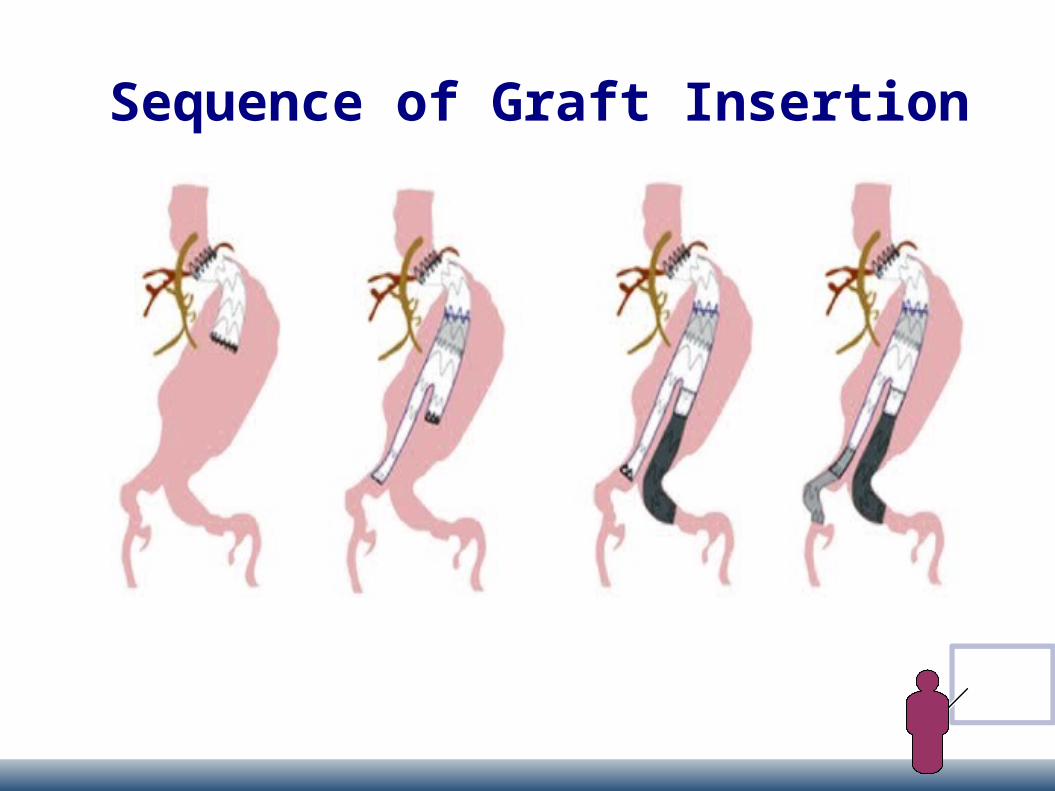
Sequence of Graft Insertion
Follow-up Treatment
CT angiogram 1 month showed exclusion of AAA
Patent 3-component stent graft, no endoleak CT angiogram at 2 months showed occlusion of
left limb of graft Endovascular repair unsuccessful; required fem-
fem bypass 9 months later no endoleak, good functioning

CT Angiogram Month 1
Complete exclusion ofaneurysm

CT Angiogram Month 9
No endoleak detected
Left limb of graft occluded,Fem-fem bypass patent
Long Term Outcome
1 year later presented with abdominal pain Type I endoleak with mild graft migration Abdominal pain resolved; no treatment needed Another year later admitted with abdominal
pain, severe hypotension, renal shutdown CT showed large retroperitoneal hematoma Taken to OR for open repair Died the next day
Discussion
3-year mortality in high-risk patient with large AAA is 55%
Nonintervention for AAA with high surgical risk only an option for patients with short life expectancy
Laparoscopic proximal aortic banding or fenestrated endograft are other options
More invasive More time-consuming Can take months to get fenestrated and branched endografts
The Authors' Conclusions
Insertion of thoracic endograft followed by placement of bifurcated aortic endograft proved feasible
Offered acceptable duration of aneurysm exclusion
Gives another alternative for treatment of high risk patients with difficult anatomy in an emergency situation