what is new in cardiac ct? in search of the comprehensive and conclusive heart scan
TRANSCRIPT
WHAT IS NEW IN CARDIAC CT? IN SEARCH OF THE COMPREHENSIVE AND CONCLUSIVE HEART SCAN
Review Article
According to World Health Organization statistics for2007, cardiovascular deaths account for 33.7% of alldeaths worldwide, whereas cancer represents 29.5%, otherchronic diseases, injury and communicable diseasescontribute to 26.5%, 7%, and 4.6%, respectively [1].Considering the fact that cardiovascular deaths top the list,it would be useful to have a perfect diagnostic test to showthe disease clearly in its extent and nature. However, thecurrent noninvasive tests of ECG, Echo and TMT areindirect means of judging the presence of significantCoronary artery disease (CAD) and may even beinconclusive.
In our study of patients with mildly positive TMT (CSI2010) 85% of patients had CAD, majority of who had softplaques.
Invasive Coronary angiography (ICA) the goldstandard for coronary anatomy has had a profound impacton the diagnosis and management of ischemic heartdisease, setting up the potential for both surgical andpercutaneous coronary revascularization and thefoundation for contemporary myocardial reperfusiontherapy. The enormity of the significance of ICA and howit has completely revamped cardiovascular medicine in thepast four decades cannot be adequately emphasized.Although the value of ICA remains unquestioned, itdepicts the coronary artery as a simple two-dimensionalprojection of the lumen. Unfortunately, the silhouette or“luminogram” is a relatively poor representation ofcoronary anatomy and a limited standard on which to base
WHAT IS NEW IN CARDIAC CT? IN SEARCH OF THE COMPREHENSIVE ANDCONCLUSIVE HEART SCAN
Rochita VenkataramananSenior Consultant Radiologist, Apollo Hospital, 21, Greams Lane, Chennai 600 006, India.
E-mail:[email protected]
Coronary CT Angiography (CT) with its noninvasive cross sectional information has seen remarkable growth inrecent years. With the introduction of the new generation scanners, like the 320-slice CT, it has risen to a wholenew level. Percent diameter stenosis determined with the use of 320-slice CT shows good correlation withInvasive catheter angiogram (ICA) without significant underestimation or overestimation. Plaque compositionon CT regardless of lesion severity has emerged as a strong predictor of major cardiac events. The percentagestenosis mismatch between CT and ICA can be explained by the 2 dimensional nature of ICA and itsinterpretive inconsistencies. In the upcoming years, we need to evolve from focusing on lumen stenosis to acomprehensive assessment of CAD and its impact on patient outcome.
Key words: 320 slice, CT Angiography accuracy, Coronary artery plaque composition, CABG, Percentstenosis disagreement.
therapeutic decisions [2]. It is also invasive and requiresan additional stress test to add functional information tojudge the significance of a stenotic segment.
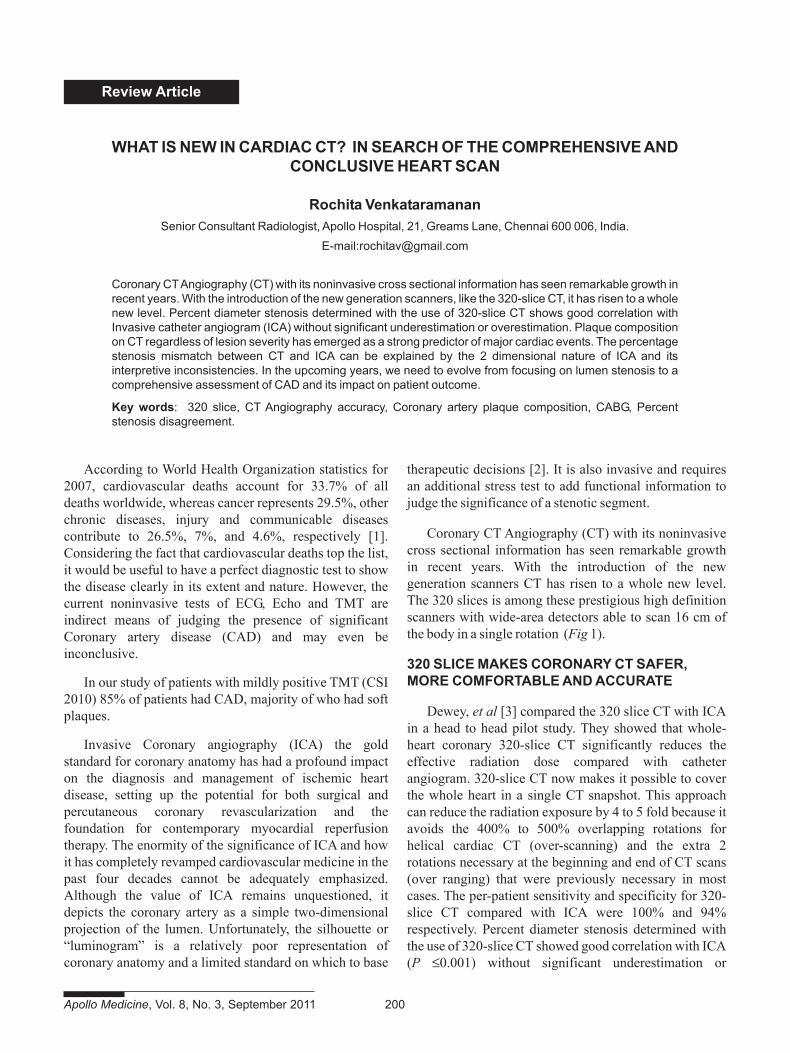
Coronary CT Angiography (CT) with its noninvasivecross sectional information has seen remarkable growthin recent years. With the introduction of the newgeneration scanners CT has risen to a whole new level.The 320 slices is among these prestigious high definitionscanners with wide-area detectors able to scan 16 cm ofthe body in a single rotation (Fig 1).
320 SLICE MAKES CORONARY CT SAFER,MORE COMFORTABLE AND ACCURATE
Dewey, et al [3] compared the 320 slice CT with ICAin a head to head pilot study. They showed that whole-heart coronary 320-slice CT significantly reduces theeffective radiation dose compared with catheterangiogram. 320-slice CT now makes it possible to coverthe whole heart in a single CT snapshot. This approachcan reduce the radiation exposure by 4 to 5 fold because itavoids the 400% to 500% overlapping rotations forhelical cardiac CT (over-scanning) and the extra 2rotations necessary at the beginning and end of CT scans(over ranging) that were previously necessary in mostcases. The per-patient sensitivity and specificity for 320-slice CT compared with ICA were 100% and 94%respectively. Percent diameter stenosis determined withthe use of 320-slice CT showed good correlation with ICA(P ≤0.001) without significant underestimation or
Apollo Medicine, Vol. 8, No. 3, September 2011 200
Review Article
201 Apollo Medicine, Vol. 8, No. 3, September 2011
overestimation. Comparison of 320-slice CT with ICArevealed a significantly smaller effective radiation dose(4.2 mSv for CT vs. 8.5 mSv for ICA) and amount ofcontrast agent required (median 80 ml for CT vs. 111 mLfor ICA P≤0.001) for 320-slice CT. The majority ofpatients (87%) indicated that they would prefer CT overICA for future diagnostic imaging (P≤0.001).
PROGNOSTIC VALUE OF CT ANGIOGRAPHYFOR MAJOR ADVERSE CARDIAC EVENTS:SCORING OVER THE CLINICAL RISK MODEL
While it is exciting to produce exquisitely beautiful CTimages of CAD, the clinical usefulness of CT and theconcern whether CT actually improves patient outcomesis an issue which needs to be resolved. Some authors feelthreatened by the enthusiasm for and proliferation ofunproven screening tests. Several recent studies haveaddressed this concern.
Vincenzo Russo, et al [4] performed CT for a total of441 patients with suspected CAD. Patients were followedup as to the occurrence of hard cardiac events (cardiacdeath, nonfatal myocardial infarction, and unstable anginarequiring hospitalization). 67.3% patients had CAD.During a mean follow-up of 31 months 44 hard cardiacevents occurred in 40 patients. Calcium scoring showed astatistically significant incremental prognostic value ascompared to a baseline clinical risk model (P≤0.018),
whereas CT angiography provided an additionalincremental prognostic value as compared with a baselineclinical risk model plus calcium scoring (P≤0.016).However, plaque composition (calcified versus soft and/ormixed plaques) and the presence of soft or mixed plaques,regardless of lesion severity, was found to be the strongestpredictor of events as a potential marker of plaquevulnerability (P≤0.0001). During follow-up, an excellentprognosis was noted in patients with normal coronaryarteries on CT.
CT provides independent and incremental prognosticinformation as compared to baseline clinical risk factorsand calcium scoring in patients with suspected CAD [5,6].
CT ANGIOGRAPHY VALUE IN THE EMERGENCYROOM. NO MORE GUESSING
Arthur Nasis, et al [7] showed that when CT is used inthe ER for patients with chest pain with low to intermediaterisk, those patients without overt plaque can be immediatelydischarged from the hospital. Patients with non-obstructiveplaque and mild to moderate stenosis can be discharged aftera negative 6 hour troponin level, and patients with severestenosis need to be admitted to the hospital for furthermanagement. At follow-up, there were no deaths or cases ofacute coronary syndrome and the rate of readmission to thehospital because of chest pain was higher in those patientswho had not had a CT. Mean length of stay was lower with
Fig.1 The contours of the arteries are sharper and rounder on the 320 slice CT as compared to the 64 slice which shows aflattening of the artery due to artefact between the subsequent scanned segments (yellow lines).
Review Article
Apollo Medicine, Vol. 8, No. 3, September 2011 202
those patients who had a CT. Tailoring troponinmeasurement to CT findings allows safe and early dischargeof patients resulting in reduced length of stay.
CT ANGIOGRAPHY USEFULNESS FORPERCUTANEOUS CORONARY INTERVENTIONAND THROMBOLYSIS
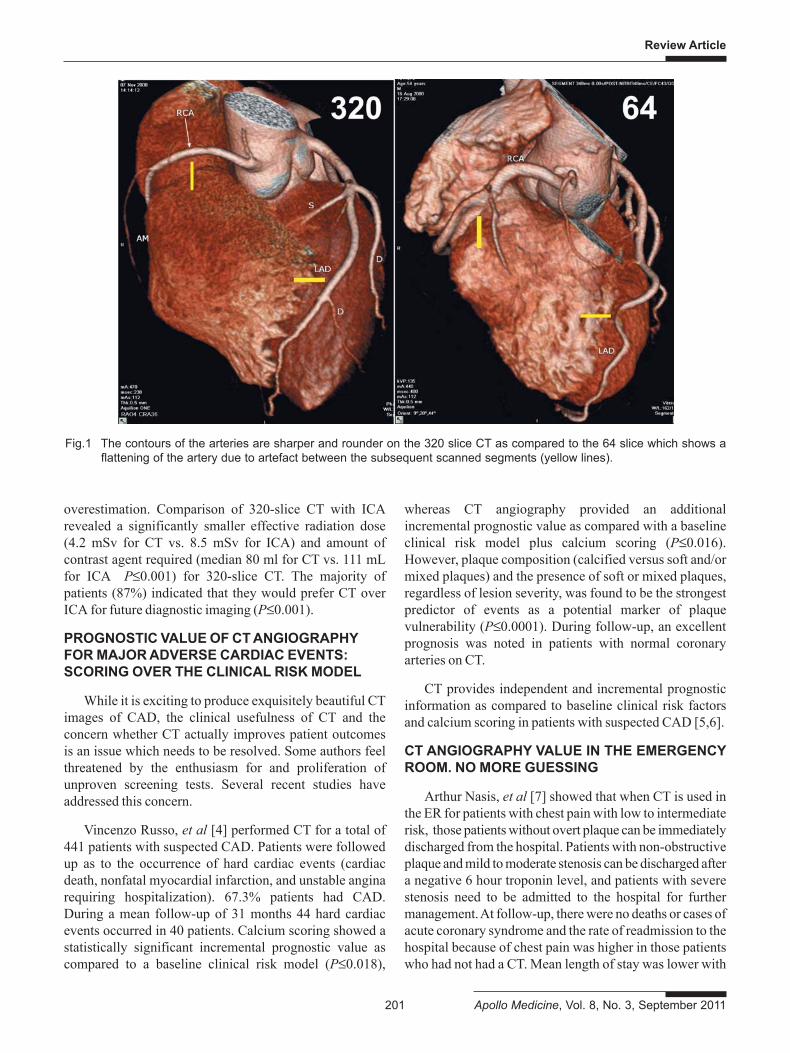
Coronary artery lesions that are more than 2 cm inlength, across an excessively angulated segment, withheavy calcification, across ostia or bifurcations, withirregular surfaces and adherent thrombi, past tortuoussegments or those that are totally occluded are consideredcomplex and have limited success after stenting [8]. It istherefore important to identify these lesions. Brett MWertman, et al [9] demonstrated that CT is quite capable
of identifying these Type C complex lesions that areassociated with higher contrast use and greater procedurelength during PCI. This comes as no surprise and is aforegone conclusion given the cross sectional nature ofCT (Fig 2).
Post-procedural myocardial injury is associated withthick soft plaques as detected by CT [10]. Those patientswho had a large soft plaque in the lesion being stenteddemonstrated a rise in the troponin T levels after theprocedure. Plaque analysis by CT would therefore be auseful method for predicting post-procedural myocardialinjury after percutaneous coronary intervention.
Makoto Yamashita, et al [11] demonstrated that inpatients with Acute MI, CT can differentiate Angiographic
Fig.2 (a) Coronary plaque with partly soft and part calcific nature (mixed plaque) in the mid LAD. (b) The 3D image gives therelation of the stenotic segment to side branches as well as the curvature of the artery. (c) The lesion length and vesseldiameter can be measured. (d) The myocardium Sagittal view reveals a dark area in the suendocardium of the anteriorwall representing ischaemia.
Review Article
203 Apollo Medicine, Vol. 8, No. 3, September 2011
TIMI grade 3 (normal) from TIMI grade 2 (sluggish) flowby comparing the density of contrast at the distal end of thethrombolysed artery with that proximal to the stenoticlesion. CT number distal /CT number proximal should bemore than 0.54 for TIMI 3. CT can be used to assesscoronary reperfusion noninvasively after thrombolysis.
PLAQUE REGRESSION ASSESSMENT BY CTANGIOGRAPHY
The discovery of early CAD on CT would be futile ifthese could not be resolved by medication. Howeverseveral multicenter, randomized lipid-lowering trialsusing both catheter angiographic and clinical assessmentshowed a negligible improvement ((1 to 3%) of luminalcaliber on ICA. Yet these same studies yielded 25% to75% reduction in acute events, including myocardialinfarction [12-14]. This points to the fact that the benefitsof lipid-lowering therapy are derived by stabilization oflipid-rich plaques, not changes in angiographic lumensize. Regression in the size of the plaque can be wellassessed by CT.
Kaori Inoue, et al suggest that the use of statins even ata low dose may result in significant changes in plaquemorphology on CT and an absolute decrease in plaquevolume without significant change in lumen size and whenthe changes in lipid profile are not statistically significant.This suggests that the changes in the plaque morphologymay even occur with relatively less robust changes in thelipid profile, and may occur early after statin use [15].
STRESS MYOCARDIAL CT PERFUSION IS HERE
Stress myocardial computed tomography perfusion(CTP) is a novel examination that provides both anatomicand physiological information (i.e., myocardialperfusion). Multiple single-center studies haveestablished the feasibility of stress myocardial CTP.Furthermore, it has been illustrated that a combinedCCTA/CTP protocol improves the diagnostic accuracy todetect hemodynamic significant stenosis as comparedwith CTA alone. Stress and reversible myocardialperfusion deficit measured by CT using a visual semiquantitative approach and a visually guided software-based approach show strong similarity with SPECT[16,17].
CT AND ICA DISAGREEMENT ON PERCENTAGESTENOSIS. “NEVER THE TWAIN SHALL MEET”
Despite good sensitivity and specificity for detectingsignificant coronary artery disease in patients,disagreement on individual coronary arterial stenosisseverity is common between CT and the current “gold
standard” ICA. This is true for IVUS and histopathologyas well, which also do not correlate with ICA. Catheterangiogram readings vary from doctor to doctor and suchinconsistencies as well as the modality’s limitations as a 2-dimensional technique are important reasons fordiscrepant results between CT and ICA that are lessacknowledged.
CT and ICA are fundamentally different technologies.Expecting good agreement on the degree of lumennarrowing is rather unrealistic. Importantly, percentage ofstenosis is of uncertain relevance for patient outcome.Arbab-Zadeh and Hoe clearly point out that assessment oftotal (calcified and non-calcified) coronary atheroscleroticplaque burden, number of lesions and location, as well asplaque characterization, show strong promise for superiorprognostic impact than mere lesion quantification andthus, deserve more of our attention. In the upcoming years,we need to evolve from focusing on lumen stenosis to acomprehensive assessment of CAD and its impact onpatient outcome [18].
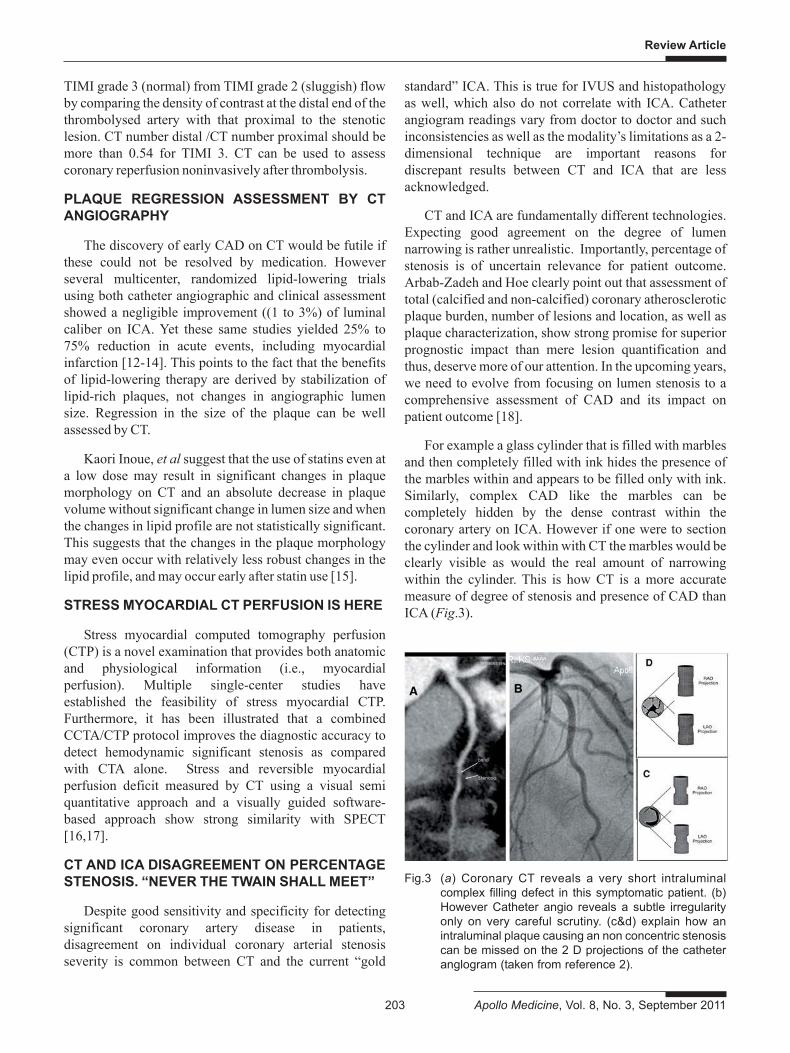
For example a glass cylinder that is filled with marblesand then completely filled with ink hides the presence ofthe marbles within and appears to be filled only with ink.Similarly, complex CAD like the marbles can becompletely hidden by the dense contrast within thecoronary artery on ICA. However if one were to sectionthe cylinder and look within with CT the marbles would beclearly visible as would the real amount of narrowingwithin the cylinder. This is how CT is a more accuratemeasure of degree of stenosis and presence of CAD thanICA (Fig.3).
Fig.3 (a) Coronary CT reveals a very short intraluminalcomplex filling defect in this symptomatic patient. (b)However Catheter angio reveals a subtle irregularityonly on very careful scrutiny. (c&d) explain how anintraluminal plaque causing an non concentric stenosiscan be missed on the 2 D projections of the catheteranglogram (taken from reference 2).
Review Article
Apollo Medicine, Vol. 8, No. 3, September 2011 204
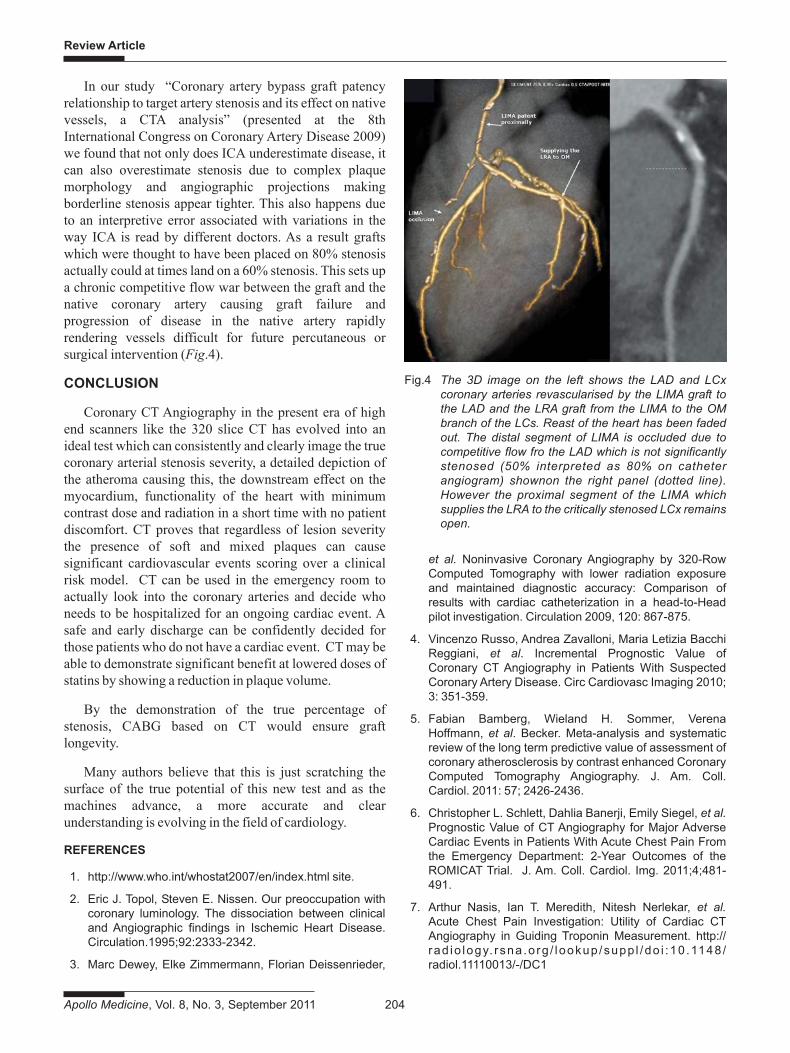
In our study “Coronary artery bypass graft patencyrelationship to target artery stenosis and its effect on nativevessels, a CTA analysis” (presented at the 8thInternational Congress on Coronary Artery Disease 2009)we found that not only does ICA underestimate disease, itcan also overestimate stenosis due to complex plaquemorphology and angiographic projections makingborderline stenosis appear tighter. This also happens dueto an interpretive error associated with variations in theway ICA is read by different doctors. As a result graftswhich were thought to have been placed on 80% stenosisactually could at times land on a 60% stenosis. This sets upa chronic competitive flow war between the graft and thenative coronary artery causing graft failure andprogression of disease in the native artery rapidlyrendering vessels difficult for future percutaneous orsurgical intervention (Fig.4).
CONCLUSION
Coronary CT Angiography in the present era of highend scanners like the 320 slice CT has evolved into anideal test which can consistently and clearly image the truecoronary arterial stenosis severity, a detailed depiction ofthe atheroma causing this, the downstream effect on themyocardium, functionality of the heart with minimumcontrast dose and radiation in a short time with no patientdiscomfort. CT proves that regardless of lesion severitythe presence of soft and mixed plaques can causesignificant cardiovascular events scoring over a clinicalrisk model. CT can be used in the emergency room toactually look into the coronary arteries and decide whoneeds to be hospitalized for an ongoing cardiac event. Asafe and early discharge can be confidently decided forthose patients who do not have a cardiac event. CT may beable to demonstrate significant benefit at lowered doses ofstatins by showing a reduction in plaque volume.
By the demonstration of the true percentage ofstenosis, CABG based on CT would ensure graftlongevity.
Many authors believe that this is just scratching thesurface of the true potential of this new test and as themachines advance, a more accurate and clearunderstanding is evolving in the field of cardiology.
REFERENCES
1. http://www.who.int/whostat2007/en/index.html site.
2. Eric J. Topol, Steven E. Nissen. Our preoccupation withcoronary luminology. The dissociation between clinicaland Angiographic findings in Ischemic Heart Disease.Circulation.1995;92:2333-2342.
3. Marc Dewey, Elke Zimmermann, Florian Deissenrieder,
et al. Noninvasive Coronary Angiography by 320-RowComputed Tomography with lower radiation exposureand maintained diagnostic accuracy: Comparison ofresults with cardiac catheterization in a head-to-Headpilot investigation. Circulation 2009, 120: 867-875.
4. Vincenzo Russo, Andrea Zavalloni, Maria Letizia BacchiReggiani, et al. Incremental Prognostic Value ofCoronary CT Angiography in Patients With SuspectedCoronary Artery Disease. Circ Cardiovasc Imaging 2010;3: 351-359.
5. Fabian Bamberg, Wieland H. Sommer, VerenaHoffmann, et al. Becker. Meta-analysis and systematicreview of the long term predictive value of assessment ofcoronary atherosclerosis by contrast enhanced CoronaryComputed Tomography Angiography. J. Am. Coll.Cardiol. 2011: 57; 2426-2436.
6. Christopher L. Schlett, Dahlia Banerji, Emily Siegel, et al.Prognostic Value of CT Angiography for Major AdverseCardiac Events in Patients With Acute Chest Pain Fromthe Emergency Department: 2-Year Outcomes of theROMICAT Trial. J. Am. Coll. Cardiol. Img. 2011;4;481-491.
7. Arthur Nasis, Ian T. Meredith, Nitesh Nerlekar, et al.Acute Chest Pain Investigation: Utility of Cardiac CTAngiography in Guiding Troponin Measurement. http://rad io logy. rsna .o rg / lookup /supp l /do i :10 .1148 /radiol.11110013/-/DC1
Fig.4 The 3D image on the left shows the LAD and LCxcoronary arteries revascularised by the LIMA graft tothe LAD and the LRA graft from the LIMA to the OMbranch of the LCs. Reast of the heart has been fadedout. The distal segment of LIMA is occluded due tocompetitive flow fro the LAD which is not significantlystenosed (50% interpreted as 80% on catheterangiogram) shownon the right panel (dotted line).However the proximal segment of the LIMA whichsupplies the LRA to the critically stenosed LCx remainsopen.
Review Article
205 Apollo Medicine, Vol. 8, No. 3, September 2011
8. SG Ellis, MG Vandormael, MJ Cowley, et al. Coronarymorphologic and clinical determinants of proceduraloutcome with angioplasty for multivessel coronarydisease. Implications for patient selection. MultivesselAngioplasty Prognosis Study Group. Circulation 1990,82:1193-1202.
9. Brett M. Wertman, Victor Y. Cheng, Saibal Kar, et al.Characterization of complex coronary artery stenosismorphology by Coronary Computed TomographicAngiography. J. Am. Coll. Cardiol. Img. 2009: 2; 950-958.
10. Tadayuki Uetani, Tetsuya Amano, Ayako Kunimura, et al.The Association Between Plaque Characterization by CTAngiography and Post-Procedural Myocardial Infarctionin Patients With Elective Stent Implantation. J. Am Coll.Cardiol Img 2010: 3;19-28.
11. Makoto Yamashita, Souki Lee, Shuichi Hamasaki, et al.Noninvasive evaluation of coronary reperfusion by CTAngiography in patients with STEMI. J Am Coll CardiolImg. 2011: 4; 141-149.
12. Brown BG, Zhao XQ, Sacco DE, et al. View of treatmentto achieve regression of coronary atherosclerosis and toprevent plaque disruption and clinical cardiovascularevents. Br Heart J. 1993: 69: S48-S53.
13. Scandinavian Simvastatin Survival Study Group.Randomised trial of cholesterol lowering in 4444 patients
with coronary heart disease: the ScandinavianSimvastatin Survival Study. Lancet. 1994: 344: 1383-1389.
14. Brown BG, Zhao XQ, Sacco DE, et al. Lipid lowering andplaque regression: new insights into prevention of plaquedisruption and clinical events in coronary disease.Circulation. 1993: 87: 1781-1790.
15. Kaori Inoue, Sadako Motoyama, Masayoshi Sarai, et al.Serial Coronary CT Angiography – Verified Changes inPlaque Characteristics as an End Point: Evaluation ofEffect of Statin Intervention. J Am Coll Cardiol Img 2010:3; 691-698.
16. Tust Techasith, Ricardo C Cury. Stress Myocardial CTPerfusion: An Update and Future Perspective. J Am CollCardiol Img 2011: 4; 905-916.
17. Balaji K. Tamarappoo, Damini Dey, Ryo Nakazato, et al.Comparison of the Extent and Severity of MyocardialPerfusion Defects Measured by CT CoronaryAngiography and SPECT Myocardial Perfusion Imaging.J Am Coll Cardiol Img 2010: 3; 1010-1019.
18. Armin Arbab-Zadeh, John Hoe. Quantification ofCoronary Arterial Stenoses by Multidetector CTAngiography in Comparison With ConventionalAngiography: Methods, Caveats, and Implications. J AmColl Cardiol Img. 2011: 4; 191-202.

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/