advanced diploma in principles of nutrition · advanced diploma in principles of nutrition course...
TRANSCRIPT

ADVANCED DIPLOMA IN PRINCIPLES OF NUTRITION
@ShawPhotoTomCourse Educators: Thomas Woods, William Eames
BY AMANDA BRODERICK BSc ANutR
BSC HONS Sports Biomedicine and Nutrition
BY AMANDA BRODERICK LESSON: 7

Course Educator:
Amanda Broderick Course Educator
B.A. (Hons.)
Special Diets Semester :
Practical Lesson 7Osteoporosis
@ShawNutritionA [email protected]

Practical Lesson 7 Learning Outcomes
Iodine deficiency Alcohol
Calcium deficiency
Practical Advice on:
Calcium regulation
What aids the absorption of calcium
Bone Biology
Risk Factors for osteoporosis

Function Forms part of the thyroid hormones - thyroxine
and triiodothyronine Necessary for maintenance of metabolic rate Thermoregulation Protein synthesis Integrity of connective tissue
Protein synthesis in the brain and central nervous system are dependent on iodine
Requirement: LRNI 70ug/day- may be sufficient to prevent
goitre RNI 140ug/day
Iodine

Sources:Milk and milk products Beer and lager Cereals and cereal products Fish and fish dishes
Concentrated sources of iodine:Marine fish Shellfish Sea salt Dried seaweeds
Iodine

Normally well absorbed Inhibited by goitrogens e.g. thiocyanates and
cyanoglucosides
Found in: Turnips, Cabbage, Cassava, Millet, Maize, Bamboo
shoots, Lima beans, Sweet potato
Calcium, magnesium, manganese and fluoride can inhibit absorption
Not a huge problem in Western society unless intake is very low
Absorption and Bioavailability of Iodine

Deficiency in adults - fall in blood level of hormone thyroxine (T4) and stimulation of thyroid-stimulating hormone (TSH)
TSH causes hyperplasia of thyroid gland - goitre develops
In pregnant women, iodine deficiency associated with: Stillbirths Spontaneous abortions Perinatal deaths Congenital abnormalities In infants and young people, deficiency can cause: Impairment of brain development Cretinism-characterised by mental retardation Hypothyroidism and dwarfism
Deficiency of Iodine
Goitre

Biological mechanisms help protect against iodine toxicity
Body can block iodine uptake once intake exceeds 2mg/day
Persistently high iodine intakes can cause hyperthyroidism and may be linked to thyroid cancer
Requirements of iodine
EVM could not establish a safe upper limit
For guidance purposes, a supplemental intake of 0.5mg/day (in addition to dietary iodine) would not be expected to have any significant adverse effects in adult
Toxicity of Iodine

Folate- alcohol interferes with the intake, absorption, transport, storage and release of folate
Vitamin B12- consumption lowers B12 levels
Vitamin A- alcohol promotes a deficiency in vitamin A and enhances its toxicity
Calcium- alcohol causes a loss of calcium in the body by increasing urinary calcium excretion
Nutritional deficiencies common among alcoholics:
Alcohol
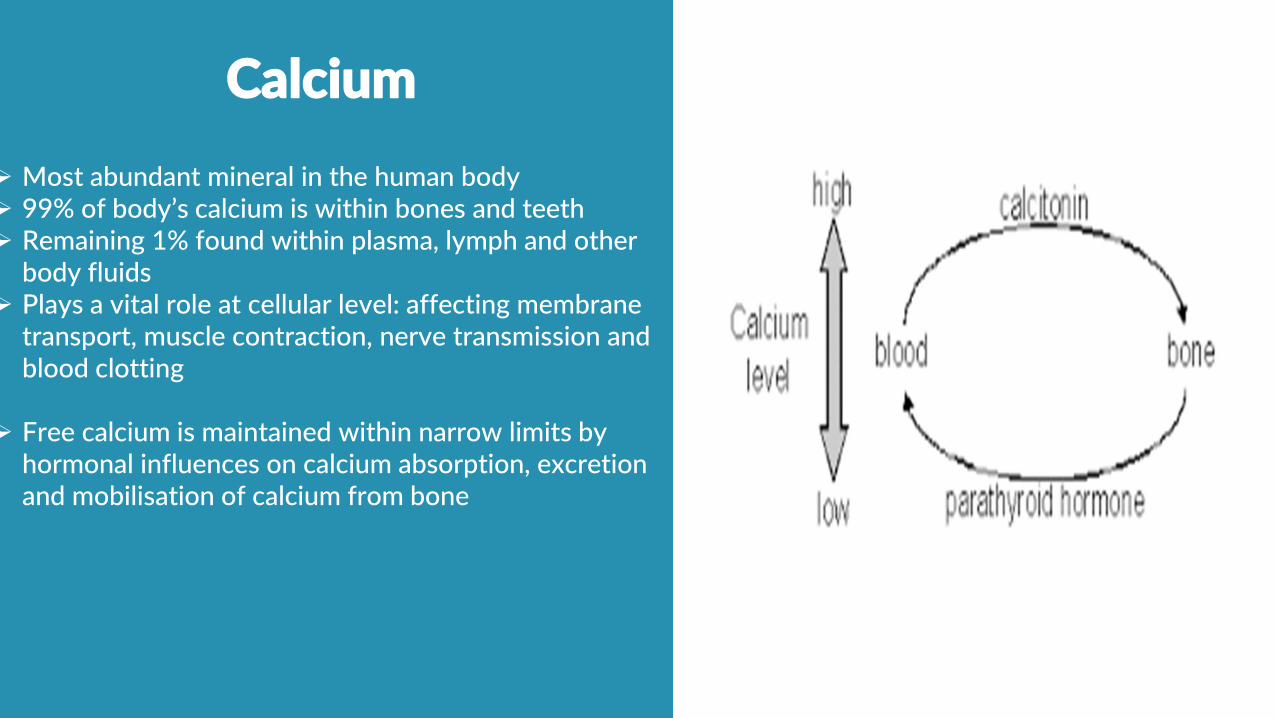
Most abundant mineral in the human body 99% of body’s calcium is within bones and teeth Remaining 1% found within plasma, lymph and other
body fluids Plays a vital role at cellular level: affecting membrane
transport, muscle contraction, nerve transmission and blood clotting
Free calcium is maintained within narrow limits by hormonal influences on calcium absorption, excretion and mobilisation of calcium from bone
Calcium

Parathyroid hormone (PTH): raises plasma calcium by:
Increasing resorption of calcium and stimulates the formation of Vitamin D which increases calcium absorption from GI tract
Hormone Calcitonin: decreases plasma calcium levels
Inhibits the release of calcium from bone Increases urinary excretion
Calcium

Calcium is Tightly Regulated

Highest requirements during periods of growth, infancy and adolescence
UK Department of Health Guidelines: 1-3 years: 350mg/day 4-6 years: 450 mg/day 7-10 years: 550mg/day 11-18 years: 1000mg/day for males and 800mg/day for females Adults over 19 years: 700 mg/day No additional calcium required during pregnancy Additional 550mg calcium/day is considered necessary to meet the needs
of lactating women For those with osteoporosis- 1,000mg/day (NICE guidelines) Taking 1,500mg/day is unlikely to cause harm
See manual for sources of calcium
Calcium- Requirements
Calcium supplementation is effective in post-menopausal women in retarding bone loss
Calcium supplementation - may maintain bone mass in established osteoporosis
Sources:• Milk and dairy products- rich source, well
absorbed and easily available• Green leafy veg, bony fish, dried fruit, seeds,
pulses and various fortified foods
Calcium

Supplements - may be necessary if not obtaining sufficient calcium in the diet
Doses should be taken in doses <500mg at a time to maximise absorption
Absorption decreases with higher loads Iron supplements should not be taken at the
same time as calcium supplements
National Osteoporosis Society recommend 1200mg/day calcium through diet
Calcium
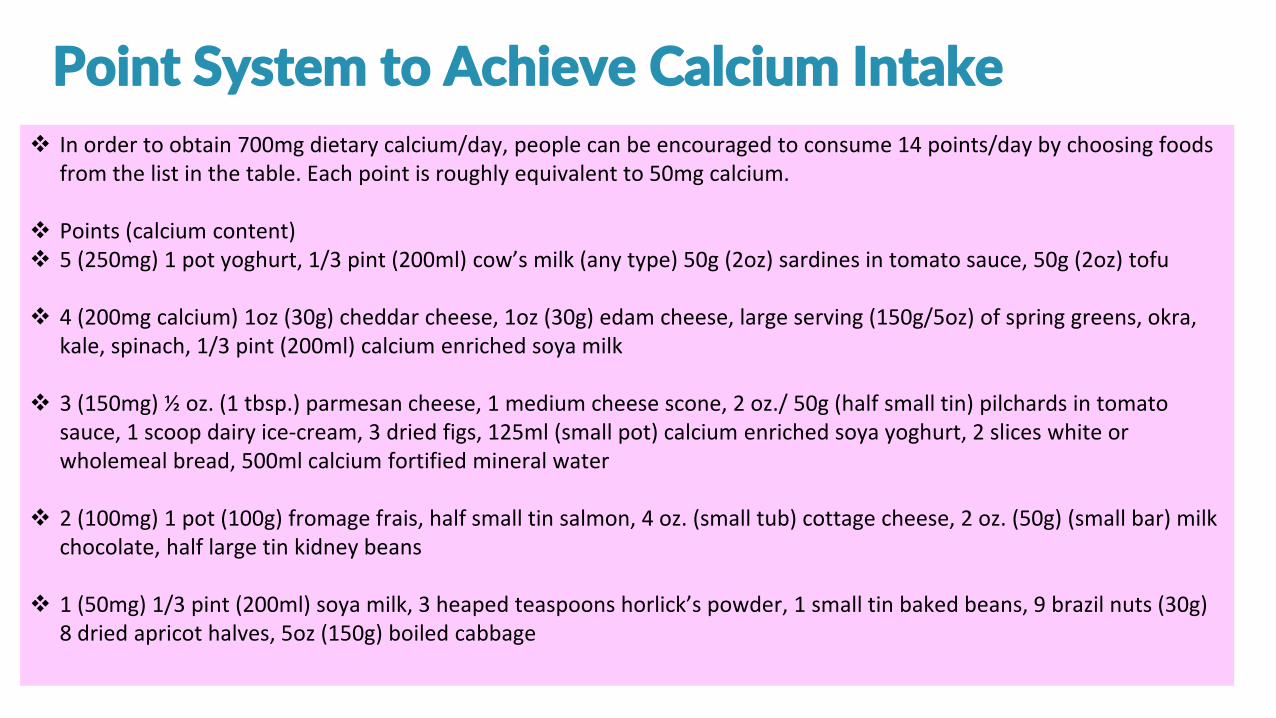
In order to obtain 700mg dietary calcium/day, people can be encouraged to consume 14 points/day by choosing foods from the list in the table. Each point is roughly equivalent to 50mg calcium.
Points (calcium content) 5 (250mg) 1 pot yoghurt, 1/3 pint (200ml) cow’s milk (any type) 50g (2oz) sardines in tomato sauce, 50g (2oz) tofu
4 (200mg calcium) 1oz (30g) cheddar cheese, 1oz (30g) edam cheese, large serving (150g/5oz) of spring greens, okra, kale, spinach, 1/3 pint (200ml) calcium enriched soya milk
3 (150mg) ½ oz. (1 tbsp.) parmesan cheese, 1 medium cheese scone, 2 oz./ 50g (half small tin) pilchards in tomato sauce, 1 scoop dairy ice-cream, 3 dried figs, 125ml (small pot) calcium enriched soya yoghurt, 2 slices white or wholemeal bread, 500ml calcium fortified mineral water
2 (100mg) 1 pot (100g) fromage frais, half small tin salmon, 4 oz. (small tub) cottage cheese, 2 oz. (50g) (small bar) milk chocolate, half large tin kidney beans
1 (50mg) 1/3 pint (200ml) soya milk, 3 heaped teaspoons horlick’s powder, 1 small tin baked beans, 9 brazil nuts (30g) 8 dried apricot halves, 5oz (150g) boiled cabbage
Point System to Achieve Calcium Intake

Lactose- enhances calcium absorption Pytates, oxalates and other substances inhibit
absorption
Absorption is impaired by: Vitamin D deficiency In those with fat malabsorption
People most likely to be at risk of calcium inadequacy are those who:
Have high calcium needs Avoid milk and dairy products Have fat malabsorption
Absorption and Bioavailability
Bioavailability of calcium in different foods varies:

Protein: Sufficient intake is important for bone health Protein deficiency - adversely affects bone loss,
risk of falling and response to injury Excess dietary protein may increase urinary
excretion of calcium where calcium intake is low High intake of protein in nutritionally balanced
diet is not detrimental to bone health
Alcohol Excessive alcohol intake is toxic to osteoblasts -
reducing bone formation Positive association between bone mineral
density and moderate alcohol consumption
Dietary Factors with an effect on calcium
bioavailability

Sodium: high intake may cause calcium excretion
Phosphorous- increased intake relative to calcium results in secondary hyperparathyroidism, bone loss and ultimately poor skeletal health- commonly found in fizzy drinks
Potassium- diets low in potassium may increase calcium loss- found in fruit, veg, milk
Dietary Factors with an effect on calcium
bioavailability

Magnesium- deficiency may be a risk for osteoporosis. More evidence needed to link it with osteoporosis
Vitamin A- some studies show a link between high intake and risk of bone fracture
Vitamin K- positively associated with Bone mineral density- good sources include broccoli, cauliflower, and dark green veg
Dietary Factors with an effect on calcium
bioavailability

Caffeine - small negative effect on calcium-hypercalciuric action on kidney
Effect usually offset by addition of milk to tea and coffee
Phytates and oxalates - bind to calcium in the gut and decrease its absorption
Phytic acid - found in cereal bran, beans and grains Oxalates - rhubarb and spinach
Phytoestrogens - potential reduction in bone resorption and increase in bone formation
Fruit and veg - provide many of the micronutrients shown to have positive effect on bone
Aid in maintenance of acid-base balance in the body
Dietary Factors with an effect on calcium
bioavailability

Dietary Factors with an effect on calcium
bioavailability
Overall a healthy well-balanced diet that provides vitamins, minerals and protein from
the four major food groups (fruit and veg, bread, potatoes, pasta and cereals, milk and dairy products, meat, fish, eggs, pulses, nuts and seeds) is likely to meet the requirements
for healthy bones, and also reduce the risks of other chronic diseases.

Osteoporosis
What is it? Most common bone disease worldwide Progressive skeletal disease Results in low bone mass and porous, weak
bones More likely to experience fractures and bone
breaks
Where does it occur? Typically at the hip, spine and forearm

Osteoporosis
Who is it most likely to affect? Can occur in all age groups More common in females than men
How can you reduce your risk? Achieve optimal bone mass Maintain bones throughout adulthood Reduce the rate of bone loss in later life

Specialised connective tissue Constantly being turned over throughout life
Main purpose of the turnover: Maintain skeletal integrity Calcium homeostasis
Bone cells:1. Osteoclasts - break down old bone2. Osteoblasts - build bone cells3. Osteocytes - maintain bone tissue
2 different types of bone tissue: Cortical Trabecular
Bone Biology

Defined as the highest level of bone mass achieved as a result of normal growth
About 26% of final adult bone is accumulated between:
11.5 - 13.5 years in girls 13.1 and 15.1 years in boys
Majority of bone mass is achieved by 18 years
An additional 5 - 10% can be achieved in 3rd
decade of life
Obtaining peak bone mass is highly dependent on lifestyle factors (25%)
Skeletal Development
Peak Bone Mass

Modifiable /environmental factors affecting bone mass: Endocrine factors (sex steroids, calcitriol (i.e.
vitamin D), insulin-like growth factor-I (IGF-I))Mechanical forces (physical activity, body
weight) Nutrition (such as calcium and protein intake) Exposure to risk factors (such as smoking,
excessive alcohol and caffeine consumption)
Skeletal Development

Bone mass remains stable until 45-50 years
Bone loss: bone resorption begins to exceed bone formation
Why: change in hormone levels
E.g. drop in oestrogen levels after menopause
Bone Loss

Population group Risk factors
Women Oestrogen deficiency caused by: • Early menopause or hysterectomy (age<45 years)• Prolonged secondary amenorrhoea (>6months, excluding
pregnancy) as a result of over-exercising or over-dieting
Men Low levels of male hormone testosterone (hypogonadism)
Women and men • Previous fragility fracture• Close family history of osteoporosis• Long-term use of oral corticosteroids (e.g. for asthma or arthritis)• Malabsorption problems (coeliac disease, crohn’s disease, gastric
surgery)• Low BMI (<19kg/m2)• Long-term immobility• Heavy drinking• smoking
Risk Factors for Osteoporosis
Lifestyle advice: Adequate nutrition - in particular calcium and vitamin D Regular weight bearing exercise Avoid tobacco and alcohol abuse
Drug treatment: Bisphosphonates: anti-resorptive agents and they reduce
the relative risk of vertebral and non-vertebral fractures by 40-50%
Parathyroid hormone stimulates bone formation. It has been shown to reduce significantly vertebral and other fractures but not hip fractures in women with severe osteoporosis
Combined calcium and vitamin D supplementation is often prescribed as part of osteoporosis treatment
Treatment of Osteoporosis

Try attend all of the sessions live and see your knowledge grow
Lesson 8 will cover Vegetarian and Raw Food Diets
Recordings are uploaded within 24 hours of the completion of each live session
Further reading links are available if you wish to learn more
Next Steps

Further Learning
To expand upon the subjects covered in todays lesson:
• Basic nutrition- Diploma in Nutrition
• Weight loss- Ultimate weight Loss Programme

Advanced Course Resources
• Free Short Videos• Topical Items that Pop Up Frequently• Easy way of communicating that free content is
available without spamming you!!!!
Facebook: www.facebook.com/shawacademyTwitter: @shawacademy, @ShawNutritionA
Before we begin let us gauge your experience level

www.shawacademy.com
Contact us anytime on:
UK: +44 (0) 207 022 6483