ash highlights 2015 - nihr · dr shankara paneesha ash highlights 2015 . ... dr shankara paneesha...
TRANSCRIPT

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
ASH Highlights 2015

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Themes of ASH 2015
Novel therapies
- Myeloma
– AML
– Lymphoma
– Pd-L1 & PD-l inhibitors
Emerging concepts in biology
– HIF-1a pathway
Cautionary tales
ASH Choosing Wisely list

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
IFM/DFCI 2009: Phase III Study Design
Primary objective: PFS
Secondary objectives: ORR, MRD, TTP, OS, Safety
Attal M, et al. ASH 2015. Abstract 391. Slide credit: clinicaloptions.com
RVd*†
8 cycles
Pts 65 yrs of age or younger
with symptomatic, measurable NDMM
(N = 700) RVd*
3 cycles
Lenalidomide
maintenance
12 mos RVd*
2 cycles
consolidation
MEL200
ASCT†
*RVD: bortezomib 1.3 mg/m2 IV on Days 1, 4, 8, 11 + lenalidomide 25 mg on Days 1-14 + dexamethasone 20 mg on Days 1, 2, 4, 5, 8, 9, 11, 12.
†Included PBSC collection with cyclophosphamide 3 g/m2 + G-CSF after cycle 3.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
IFM/DFCI 2009 : Responses
Response, % RVd (n = 350) Transplantation (n = 350) P Value
CR 49 59
.02 VGPR 29 29
PR 20 11
< PR 2 1
≥ VGPR 78 88 .001
Negative MRD by FCM 65 80 .001
Attal M, et al. ASH 2015. Abstract 391.
Slide credit: clinicaloptions.com
Treatment Phase ≥ VGPR Rate, %
P value RVd (n = 350) Transplantation (n = 350)
After induction 47 50 NS
After transplant or
cycle 4 of consolidation 55 73 < .0001
After consolidation completed 71 81 < .006
At end of maintenance phase 78 88 < .001

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
IFM/DFCI 2009 : PFS (Primary Endpoint)
Parameter RVd
(n = 350)
Transplantation
(n = 350) P Value
Median follow-up, mos 41 41
Progression or death, n 204 158
Median PFS, mos 34 43
4-yr PFS, % 35 47
HR (95% CI) 1 0.69 (0.56-0.84) < .001
Attal M, et al. ASH 2015. Abstract 391.
Slide credit: clinicaloptions.com
At second interim analysis in June 2015 with median follow-up of 39 mos, the data and safety monitoring board for this trial recommended that the trial be stopped

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
IFM 2009: Overall Conclusions
ASCT vs RVD in pts with NDMM is associated with:
– 31% reduced risk of progression or death (P < .001)
– Improved TTP and rate of MRD negativity
– Similar, low rate of mortality
Longer follow-up required to make any conclusions about
OS
Authors concluded that ASCT should remain a standard of
care for eligible pts with myeloma
Similar, confirmatory trial ongoing in US
Attal M, et al. ASH 2015. Abstract 391. Slide credit: clinicaloptions.com

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Blinatumomab in MRD-Positive BCP ALL:
Study Design International, multicenter, open-label phase II study from 2010-2013
– 46 centers
– 11 countries
Primary endpoint: achieving MRD < 10-4 in cycle 1
Secondary endpoints: OS, RFS, DoR, MRD < 10-4, safety
CD19+ BCP ALL pts
18 yrs of age or older with < 5% BM blasts,
MRD ≥ 10-3 after ≥ 3 chemotherapies,
and no prior allo-SCT, CNS/extramedullary involvement, or Ph+ ALL eligible for TKIs
(N = 116)
•Blinatumomab
•15 µg/m2 QD IVCI
Slide credit: clinicaloptions.com
•Cycle 1*
Gökbuget N, et al. ASH 2015. Abstract 680.
Followed for 2-yr efficacy,
survival
*28 days on tx, 14 days off.
Pts with MRD response received
≤ 3 additional cycles and/or allo-SCT (eligible pts); tx
discontinuation upon hematologic relapse

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Blinatumomab in MRD-Positive BCP ALL:
Efficacy
Median follow-up: 30 mos
Complete MRD response: 80%
Transplant realization rate: 72%
•Slide credit: clinicaloptions.com •Gökbuget N, et al. ASH 2015. Abstract 680.
Outcome, Mos Blinatumomab
(n = 110)
MRD Complete vs
Incomplete, P Value
Median OS
MRD complete responder
MRD incomplete responder
36.5
38.9
12.5
.002
Median RFS
CR1
CR2/CR3
MRD complete responder
MRD incomplete responder
18.9
24.6
11.0
23.6
5.7
.003
Median DoR
MRD complete responder
MRD incomplete responder
NR
NR
17.2
.049

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Blinatumomab in MRD-Positive BCP ALL:
Conclusions 80% of MRD-positive BCP ALL pts achieved complete MRD response
on blinatumomab therapy
Achieving complete (vs incomplete) MRD response was associated
with improved outcomes
– OS: 38.9 vs 12.5 mos; P = .002
– RFS: 23.6 vs 5.7 mos; P = .003
– DOR: NR vs 17.2 mos; P = .049
67% of pts in CR following blinatumomab were able to receive allo-
SCT
Most neurologic AEs were grade ≤ 2
– 10% of pts required therapy interruption or discontinuation
•Slide credit: clinicaloptions.com •Gökbuget N, et al. ASH 2015. Abstract 680.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
•Slide credit: clinicaloptions.com •Stone RM, et al. ASH 2015. Abstract 6.
RATIFY: Midostaurin in FLT3-Positive AML:
Study Design
Double-blind, placebo-controlled, randomized phase III study of midostaurin, an FLT3 inhibitor
– Primary endpoint: OS (not censored for SCT)
– Secondary endpoint: EFS
•18-60 yrs of age with
•FLT3-mutated
•(non-APL) AML
•(N = 717)
•Daunorubicin
•60 mg/m2 IVP D1-3 +
•Cytarabine
•200 mg/m2/d IVCI D1-7 +
•Midostaurin
•50 mg PO BID D8-21
•(n= 360) Daunorubicin
60 mg/m2 IVP D1-3 +
Cytarabine
200 mg/m2/d IVCI D1-7 +
Placebo
D8-21
(n = 357)
•Cytarabine
•3 g/m2 over 3h q12h
•D1,3,5 +
•Midostaurin
•50 mg PO BID D8-21
•(n = 231)
Cytarabine
3 g/m2 over 3h q12h
D1,3,5 +
Placebo
D8-21
(n = 210)
•Midostaurin
•50 mg PO BID D1-28
•(n = 120)
Placebo
D1-28
(n = 85)
•Stratified by ITD/TKD;
randomized
•Induction*
•(1-2 cycles)
•Consolidation
•(up to 4 cycles)
•Maintenance
•(12 cycles)
•CR
•CR
*Hydroxyurea allowed for ≤ 5 days prior to induction therapy.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
RATIFY: Efficacy
•Slide credit: clinicaloptions.com •Stone RM, et al. ASH 2015. Abstract 6.
Characteristic
Midostaurin +
Chemo
(n = 360)
Placebo +
Chemo
(n = 357)
P Value
Median OS, mos (range) 74.7 (31.7-NE) 25.6 (18.6-42.9)
4-yr OS, % (95% CI)
Uncensored*
Censored for SCT†
51.4 (46.0-57.0)
63.8 (56.0-71.0)
44.2 (39.0-50.0)
55.7 (47.0-63.0)
.0074
.04
SCT, n (%)
Any time
CR1 only
212 (59)
100 (28)
196 (55)
79 (22)
.28
.08
CR, n (%)
By Day 60
In induction/consolidation
212 (59)
239 (66)
191 (53)
211 (59)
.15
.045
Median EFS, mos (range)
By day 60
In induction/consolidation
8.0 (5.1-10.6)
11.3 (8.4-15.1)
3.0 (1.9-5.9)
6.1 (4.7-7.5)
.0025
.0002
DFS, mos (range) 25.9 (19.4-NE) 14.4 (11.0-22.2) .002
*HR: 0.77. †HR: 0.75.
Longer OS shown in midostaurin arm in all FLT3 cohorts.
4-yr EFS rate was 28% with midostaurin vs 20% in placebo, regardless of FLT3
status.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
RATIFY: Conclusions
Midostaurin added to standard chemo in pts with newly
diagnosed FLT3-mutated AML
– Improved OS and EFS, regardless of ITD/TKD stratification
group and despite high SCT rate (57%), vs placebo
– Reduced risk of death by 23% vs placebo
Safety/tolerability similar in midostaurin and placebo arms
Study investigators suggest midostaurin addition to current
standard chemo with 1-yr subsequent maintenance as a
new standard of care for these pts
•Slide credit: clinicaloptions.com •Stone RM, et al. ASH 2015. Abstract 6.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
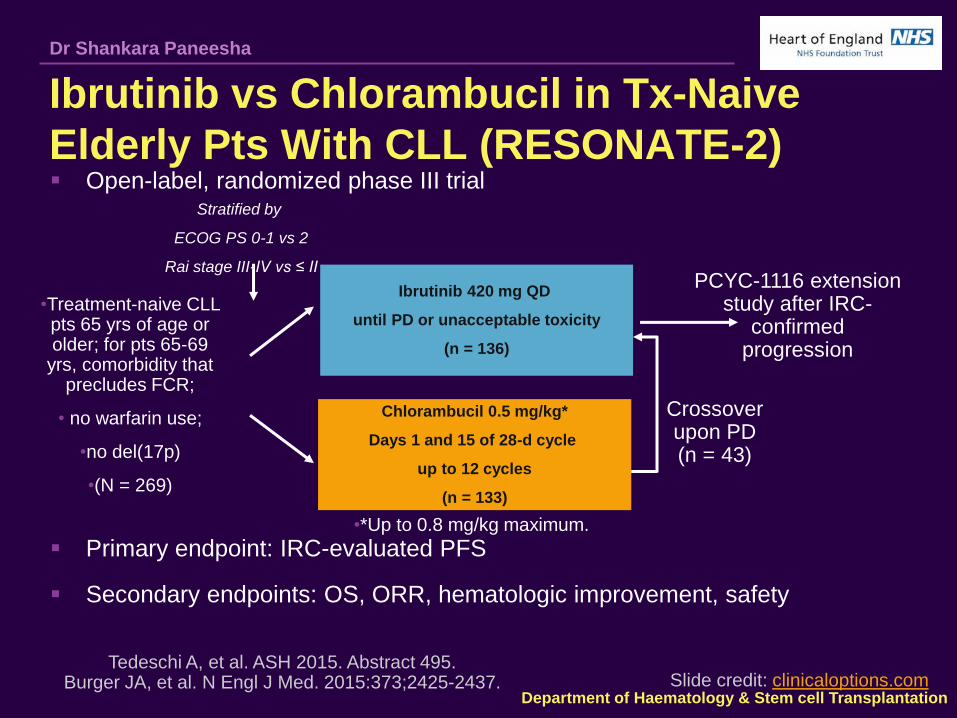
Ibrutinib vs Chlorambucil in Tx-Naive
Elderly Pts With CLL (RESONATE-2) Open-label, randomized phase III trial
Primary endpoint: IRC-evaluated PFS
Secondary endpoints: OS, ORR, hematologic improvement, safety
•Treatment-naive CLL pts 65 yrs of age or older; for pts 65-69
yrs, comorbidity that precludes FCR;
• no warfarin use;
•no del(17p)
•(N = 269)
Ibrutinib 420 mg QD
until PD or unacceptable toxicity
(n = 136)
Chlorambucil 0.5 mg/kg*
Days 1 and 15 of 28-d cycle
up to 12 cycles
(n = 133)
PCYC-1116 extension study after IRC-
confirmed progression
Stratified by
ECOG PS 0-1 vs 2
Rai stage III-IV vs ≤ II
Tedeschi A, et al. ASH 2015. Abstract 495. Burger JA, et al. N Engl J Med. 2015:373;2425-2437. Slide credit: clinicaloptions.com
Crossover upon PD (n = 43)
•*Up to 0.8 mg/kg maximum.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
•20
RESONATE-2: PFS (Primary Endpoint)
PFS results not dependent on age, Rai stage, ECOG PS, or bulky disease
1 Richter’s transformation in chlorambucil arm; none on ibrutinib arm
Tedeschi A, et al. ASH 2015. Abstract 495. Burger JA, et al. N Engl J Med. 2015:373;2425-2437. Slide credit: clinicaloptions.com
IRC Assessment Investigator Assessment
•100
•80
•60
•40
•20
•0
•PF
S (
%)
•Mos
•27 •0 •3 •6 •9 •12 •15 •18 •21 •24
•Pts at Risk, n Ibrutinib
Chlorambucil •136 133
•133 121
•130 95
•126 85
•122 74
•98 49
•66 34
•21 10
•2 0
•0 0
Ibrutinib
Chlorambucil
Median, mos
HR: 0.16 (95% CI: 0.09-0.28; P < .001)
Chlorambucil 18.9
Ibrutinib NR
•100
•80
•60
•40
•0
•PF
S (
%)
•Mos
•27 •0 •3 •6 •9 •12 •15 •18 •21 •24
•Pts at Risk, n Ibrutinib
Chlorambucil •136 133
•133 121
•129 88
•125 88
•123 69
•104 46
•69 31
•22 10
•2 0
•0 0
Ibrutinib
Chlorambucil
Median, mos
HR: 0.09 (95% CI: 0.04-0.17; P < .001)
Chlorambucil 15.0
Ibrutinib NR

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
RESONATE-2: OS
84% reduction in risk of death with ibrutinib
Tedeschi A, et al. ASH 2015. Abstract 495. Burger JA, et al. N Engl J Med. 2015:373;2425-2437. Slide credit: clinicaloptions.com
•100
•80
•60
•40
•20
•0
•OS
(%
)
•Mos •0 •27 •3 •6 •9 •12 •15 •18 •21 •24
•Pts at Risk, n Ibrutinib
Chlorambucil
•136 133
•134 127
•131 125
•131 121
•131 118
•129 113
•74 62
•32 24
•4 1
•0 0
HR: 0.16 (95% CI: 0.05-0.56; P = .001 by log-rank test)
Ibrutinib
Chlorambucil

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Ibrutinib vs Temsirolimus in Previously Treated
MCL: MCL3001 (RAY) Randomized, open-label phase III trial
Primary endpoint: PFS
Secondary endpoints: ORR, OS, DoR, time to next
treatment, and safety •Slide credit: clinicaloptions.com
•Rule S, et al. ASH 2015. Abstract 469. Dreyling M, et al. Lancet. 2015;[Epub ahead of print].
•Ibrutinib 560 mg QD PO
•(n = 139) •Previously treated
pts with MCL
•(N = 280)
•Temsirolimus IV
•Cycle 1: 175 mg Days 1, 8, 15
•Subsequent cycles: 75 mg Days 1, 8, 15
•(n = 141)
•Crossover to ibrutinib arm if
progressive disease
•(n = 32)
Stratified by sMIPI and prior lines of therapy
•Median drug exposure: 14 mos of ibrutinib vs 3 mos of temsirolimus.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Median DoR:
– Not reached (95% CI: 16.2-NE) with ibrutinib vs 7.0 mos (95% CI: 4.2-9.9)
for temsirolimus
MCL3001 (RAY): Response
•Slide credit: clinicaloptions.com •Rule S, et al. ASH 2015. Abstract 469.
Dreyling M, et al. Lancet. 2015;[Epub ahead of print].
Outcome, % Ibrutinib
(n = 139)
Temsirolimus
(n = 141) P Value
ORR by IRC
CR
PR
SD
71.9
18.7
53.2
10.8
40.4
1.4
39.0
30.5
< .0001
ORR by previous lines
of therapy
1
2
3
71.9
68.4
75.0
48.0
39.5
33.3

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
•Median, mos
•HR (95% CI) 0.43 (0.32-0.58)
• P < .0001
MCL3001 (RAY): Survival Outcomes
Consistent PFS improvement across pt subgroups
23% of pts treated with temsirolimus crossed over to ibrutinib at
progression
•Slide credit: clinicaloptions.com
•Rule S, et al. ASH 2015. Abstract 469. Dreyling M, et al. Lancet. 2015;[Epub ahead of print].
•PFS •OS
•100
•80
•60
•40
•20
•0 •30 •27 •24 •21 •18 •15 •12 •9 •6 •3 •0
•0
•0
•0
•0
•5
•1
•8
•3
•34
•11
•45
•19
•77
•33
•83
•45
•101
•69
•114
•93
•139
•141
•Ibrutinib
•Temsirolimus
•Pts at Risk, n
•Mos
•PF
S (
%)
•Ibrutinib
•14.6
•Temsirolimus
•6.2
•Ibrutinib
•Temsirolimus
•100
•80
•60
•40
•20
•0 •30 •27 •24 •21 •18 •15 •12 •9 •6 •3 •0
•Mos
•OS
(%
)
•0
•0
•2
•2
•14
•10
•35
•25
•64
•48
•84
•71
•92
•78
•103
•85
•113
•100
•125
•116
•139
•141
•Median, mos
•HR (95% CI) 0.76 (0.53-1.09)
• P < .1324
•Ibrutinib
•NR
•Temsirolimus
•21.3

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Nivolumab in R/R cHL: Phase I Dose
Expansion Cohort
Primary endpoints: safety and tolerability
Secondary endpoints included: ORR, DoR, PFS
•cHL pts with
• ECOG PS 0/1, previous treatment with ≥ 1
chemotherapy, no autoimmune or previous organ allograft or
allogeneic BMT
•(N = 23)
•Nivolumab 3 mg/kg IV
•Wk 1, Wk 4, then Q2W
•for up to 2 yrs
•Ansell S, et al. N Engl J Med. 2015;372:311-319. Ansell S, et al. ASH 2015. Abstract 583. •Slide credit: clinicaloptions.com

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Idelalisib Given Front-Line for the Treatment of Chronic
Lymphocytic Leukemia Results in Frequent and Severe
Immune-Mediated Toxicities
Benjamin L Lampson, et al.
Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
PI3Kdelta Inhibitors Increase Genomic Instability By
Upregulating Aid Expression
Mara Compagno et al.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
Phase I Study of Rituximab, Lenalidomide, and Ibrutinib in
Previously Untreated Follicular Lymphoma (Alliance 051103)
Chaitra S. Ujjani, et al.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
ASH Choosing Wisely list Do not transfuse more than the minimum number of red blood cell
(RBC) units necessary to relieve symptoms of anemia or to return a
patient to a safe hemoglobin range (7 to 8 g/dL in stable, non-cardiac,
in-patients).
Don't test for thrombophilia in adult patients with venous
thromboembolism (VTE) occurring in the setting of major transient
risk factors (surgery, trauma or prolonged immobility).
Don't use inferior vena cava (IVC) filters routinely in patients with
acute venous thromboembolism (VTE).
Don't administer plasma or prothrombin complex concentrates for
non-emergent reversal of vitamin K antagonists (i.e. outside of the
setting of major bleeding, intracranial hemorrhage or anticipated
emergent surgery).
Limit surveillance computed tomography (CT) scans in asymptomatic
patients following curative-intent treatment for aggressive lymphoma.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha
ASH Choosing Wisely list Don't treat with an anticoagulant for more than three months in a
patient with a first venous thromboembolism occurring in the setting
of a major transient risk factor.
Don't routinely transfuse patients with sickle cell disease for chronic
anemia or uncomplicated pain crisis without an appropriate clinical
indication.
Don't perform baseline or routine surveillance computed tomography
(CT) scans in patients with asymptomatic, early stage chronic
lymphocytic leukemia.
Don't test or treat for suspected heparin-induced thrombocytopenia
(HIT) in patients with a low pre-test probability of HIT.
Don't treat patients with immune thrombocytopenic purpura in the
absence of bleeding or a very low platelet count.

Department of Haematology & Stem cell Transplantation
Dr Shankara Paneesha