causes, consequences and strategies
TRANSCRIPT
Clinician Burnout: Causes, Consequences and Strategies
Constance McLaughlin, MBA, BSN, RN-BC, Anup D. Salgia, DO, FACEP
2
Table of contents
Executive summary ..................................................................................................................... 3
Introduction ................................................................................................................................. 3
What is burnout? ......................................................................................................................... 4
Impact of clinician burnout .......................................................................................................... 5
Contributors to burnout ............................................................................................................... 6
Beating burnout ........................................................................................................................... 9
Strategies to reduce burnout related to technology ................................................................... 12
How is Cerner helping ............................................................................................................... 14
Improving the clinician workflow ................................................................................................ 14
Leadership education tools ....................................................................................................... 16
Professional fulfillment and improved wellness ......................................................................... 17
3
Executive summary
Burnout levels among physicians, nurses and ancillary health care professionals have hit an all-time high with little sign
of retreating. There are many contributing factors to the burnout epidemic, such as increased regulation, greater burden
in meeting quality measures and clinically irrelevant reporting, work-life balance pressures, financial obligations and
medical record and coding requirements through the electronic health record (EHR). The COVID-19 pandemic of 2020
has thrown medicine into a crisis, exacerbating burnout in a workforce weakened by illness and exhaustion. A recent
study by Reaction Data (2019) shows that despite the frustration technology has imposed upon the medical profession,
EHRs contribute about 10%-20% of the burnout problem, though some research and opinion pieces estimate EHR-
related burnout to be higher. Nonetheless, it is a significant issue that is impacting health care professions today.
Introduction
Meet Jaime. She has worked as a nurse practitioner for 12 years, dedicating her work to the health of others. Working in
the hospital and clinic over the years has been both challenging and joyous, but over the past year, her patient workload
has been quite heavy. Lately, she experiences a new, unexplained anxiety before her shifts start. Added stressors with
payment reform and mandates with electronic documentation and charge submissions don’t make it easier.
Jamie is reminded to attest online for her MIPS program, but the website is still down. She is starting to feel a bit
indifferent to it all; co-workers seem detached and management appears to be at odds with one another and the clinical
staff. Jamie still loves caring for patients, but other distractions seem to add a level of complexity; she’s thinking that,
perhaps, a change in jobs may be something to consider — perhaps even going part-time. During a recent routine
doctor’s visit, she was diagnosed with hypertension, noticeable weight gain and a reported lack of energy. She knows
there is something wrong but can’t quite put her finger on it.
Dr. Danielle Ofri at Bellevue Hospital, in her provocative New York Times opinion piece, "The Business of Health Care
Depends on Exploiting Doctors and Nurses" notes, “In a factory, if 30 percent more items were suddenly dropped onto an
assembly line, the process would grind to a halt. Imagine a plumber or a lawyer doing 30 percent more work without
billing for it. But in health care there is a wondrous elasticity — you can keep adding work and magically it all somehow
gets done. The nurse won’t take a lunch break if the ward is short of staff members. The doctor will 'squeeze in' the extra
patients.” Dr. Ofri goes on to write “…by far the biggest culprit of the mushrooming workload is the electronic medical
record, or EMR. It has burrowed its tentacles into every aspect of the health care system. There are many salutary
aspects of the EMR, and no one wants to go back to the old days of chasing down lost charts and deciphering
inscrutable handwriting. But the data entry is mind-numbing and voluminous.” Similarly, Atul Gawande, MD noted in his
op-ed in the New Yorker that he “feel[s] that a system that promised to increase my mastery over my work has, instead,
increased my work’s mastery over me.”
4
What is burnout?
More than half of U.S. doctors and nurses experience symptoms of burnout. Unfortunately, many have either chosen to
ignore them, have misinterpreted them or decided to leave or reduce their clinical practice because of them. Recent data
show that over 50% of providers and about one-third of nurses suffer from burnout. About 43% of nurses reported signs
of emotional exhaustion — an early indicator of burnout [1].
In 1974, clinical psychologist Herbert Freudenberger identified the presence of emotional and physical exhaustion along
with emotional detachment in his co- workers [2]. He referred to this experience as “burnout.” Since then the topic has
been researched extensively and more notably by Christine Maslach. In 1981, Maslach published a methodology to
understand the variables causing burnout syndrome [3]. Current research validates this, evidenced by epidemic
proportions of burnout among clinicians, resulting in overwhelming feelings of frustration in their careers and a loss of
professional fulfillment stemming from factors ranging from loss of autonomy to decreased efficiency.
In 2013, The U.S. National Institute for Occupational Safety and Health recognized job stress as “the harmful physical
and emotional responses that occur when the requirements of the job do not match the capabilities, resources, or needs
of the worker.”[4] Stressors that contribute to burnout are individually felt and can be caused by under-staffed shifts
resulting in excessive workloads, personal challenges or emotional exhaustion from caring for patients [5].
Similarly, in 2019, the World Health Organization (WHO) officially recognized occupational burnout as a disease by
assigning it an ICD-11 diagnostic code. Accordingly, the WHO notes that burnout is characterized by 1) feelings of
energy depletion or exhaustion; 2) increased mental distance from one’s job, or feelings of negativism or cynicism
related to one's job; and 3) reduced professional efficacy [6].
Several investigations suggest that an increased burden placed on nurses in the form of increased workload, sparse
staffing models and unrealistic management expectations [7,8] are strong predictors of physical and emotional burnout.
This forecasts poor patient outcomes, workplace and patient safety concerns, increased errors and an uptick in hospital-
acquired infections.
Clinicians feel the effects of burnout yet remain in their respective professions, conceding that physical and emotional
stress are a predictable and acceptable part of a professional clinician’s job. Suboptimal physical ergonomics and the
strain of compartmentalizing emotions in order to provide compassionate and competent care for high-acuity patients
(and their families) are equally draining. Constant interruptions, persistent heightened mental alertness and shift work can
negatively alter decision-making abilities affecting patient care, general wellness and personal relationships. Finally, the
stigma associated with asking for help can be viewed as weakness. The threat of jeopardizing licensure deters nurses
and physicians from seeking professional help with stress, anxiety and depression.

5
.
Impact of clinician burnout
A report from the National Academy of Sciences, Engineering and
Medicine points out that the stability of a clinician’s well-being holds
consequences for clinicians themselves, their patients, health care
organizations and society as a whole [9]. Over time, continuous
exposure to stressors like increased workload, increased patient
complexity and misalignment of organizational and personal values can
lead to overall poor health. Chronic health conditions like hypertension,
high cholesterol, cardiovascular disease, insomnia, anxiety and
depression can result from burnout if unchecked.
Burnout leads to job dissatisfaction and has the potential to increase
adverse patient outcomes. Resulting feelings of disengagement,
physical and emotional exhaustion, loss of control, decreased
productivity and cynicism can be transferred to other co-workers, teams, units and patients, ultimately affecting the
organization’s very culture.
With patient safety initiatives at the forefront of modern health care delivery, clear evidence shows that disproportionately
higher staffing ratios and dissatisfactory work environments are highly correlated to poor patient outcomes, reduced
patient satisfaction and shorter tenure of the clinical workforce [7]. Lower staff-to-patient ratios results in lower burnout
rates, less chance for error and decreased incidences of hospital-acquired infections [10]. Lighter staff workloads also
afford more time and attention to the patient and lift the burden of feeling mentally and physically stretched.
A California study showed that each
additional patient per nurse was associated
with a 7% increase in the likelihood of
patient morbidity within 30 days of admission
and a 7% increase in the odds of failure-to-
rescue (not recognizing an emergency until
it is too late) [7]. Studies also suggest that
care organizations consider the cost of
staffing and hospital-acquired infections
versus the cost of losing physicians and
nurses (to burnout).
There are two distinct
advantages to staff retention:
morbidity reduction and cost
savings [8,11]. Figure 1
illustrates personal and
professional impacts of burnout.
Figure 1: Personal and Professional Repercussions of Burnout Adapted from Mayo Clin Proc. 2017;92(1):129-146
Stress and eventual burnout
leave the health care worker with
feelings of disengagement,
physical and emotional
exhaustion, loss of control,
decreased productivity and
cynicism. This negativity can be
transferred to other co-workers,
teams, units and patients,
ultimately affecting the
organization’s very culture.
6
Burnout among physicians results in emotional exhaustion, depersonalization (viewing/treating people like they are
objects), a diminished sense of personal success, substance abuse, depression, post-traumatic stress disorder (PTSD)
and suicidality [12,13] (Fig. 1). Physician suicide rates are more than twice that of the U.S. population [14]. Female
physicians reported higher burnout rates than male physicians (39% vs 28%) and lower rates of professional fulfillment
(37% vs 51%). Emotional exhaustion is at the core of physician burnout. Physicians working in outpatient settings like
primary care and emergency medicine experience higher burnout compared to those working in inpatient facilities [15].
Impairment in judgement is highly associated in physicians who experience tiredness, exhaustion, fatigue, inattention
and irritability [16,17]. Burnout may also put a physician at increased risk of motor vehicle accidents and near-miss
events, even after adjusting for fatigue [18]. Psychologically, physician burnout might contribute to increased incidence of
stress, disruptive behavior, mood disorders and depression [19-21]. The presence of any of these conditions can
severely impact a physician’s well-being, disrupting their personal life and decreasing professional effectiveness. This
creates a slippery slope as it increases the odds of substance abuse and increased alcohol abuse/dependence,
especially in surgeons [22]. Though the consequences of nurse burnout are less defined, the findings from physician
studies should be cause for alarm among nurses.
Contributors to burnout
Peripheral stressors compound the prevalence of burnout. Workload affected by staffing levels, patient complexity and
increased patient volume as increased numbers of baby boomers utilize the health care system all play a role in burnout.
Organizational culture, inadequate leadership support, low employee engagement, financial pressures of school and
personal debt pile on to the problem. The nature of this highly charged subject brings with it much emotion.
Psychologists believe that humans tend to imitate and respond to others’ emotions [23]. Negative emotions are thought
to be transferred easier and imitated at a higher rate than otherwise neutral or positive feelings, leading us to conclude
that strong, negative emotions around clinician burnout and the reasons therein can spread from unit to unit or within
other business units like financial offices or clinics threatening an organization’s culture – a phenomenon referred to as
burnout contagion [24,25]. The National Academy of Medicine’s committee on System Approaches to Improve Patient
Care by Supporting Clinician Well-Being recommends that organizations take a systems approach to begin proactive
changes within the organization versus the individual level.
Public health crisis: COVID-19 pandemic
The COVID-19 pandemic has thrust front-line doctors and nurses into a chaotic public health crisis that is likely to be a
defining time in their careers. A report by the International Council of Nurses found that over 90,000 nurses worldwide
have been infected by COVID-19. The same report projects that over 200,000 health care workers have been infected.
Those who have died number in the thousands. Not all who have contracted COVID-19 have fully recovered, as a small
subset of these health care workers have experienced some type of post-recovery disability. It is unknown if these
disabilities are permanent or short-term. The pandemic has exacerbated the common contributors of burnout, and yet
has introduced new stressors. Wearing physically restrictive personal protective equipment for unusually long periods of
time, and the unabating threat of becoming infected or bringing it home to their loved ones, add to the pressures of the
job. Additionally, post-traumatic stress disorder (PTSD) has been reported to be 10%-20% higher among emergency
care workers and as high as 30% among ICU workers. Management of critical medical situations, caring for severely
traumatized people, frequent witnessing of death and trauma, operating in crowded settings and interrupted circadian
rhythms due to shift work are all reported as contributors to PTSD in this pandemic.
7
Aging populations and health care workforce
Projections from a 2019 report by the American Association of Medical Colleges predicts a severe shortage of
physicians up to 121,000 by 2031 [26]. As the baby boomer generation ages into retirement, their demands on the
medical system will outstrip the supply physicians. The study goes on to note that 30% of U.S. doctors are over the age
of 65, nearing retirement themselves, compounding the problem. Similarly, The U.S. Bureau of Labor Statistics predicts
1.2 million nursing vacancies between 2014 & 2022 and estimates the need to add 200,000+ RNs each year to fill
vacancies due to attrition, accepting non-clinical roles and those retiring [27-31]. As it stands, 50% of the current nursing
workforce is 50 years of age or older [32].
Experience gap among providers
Amid an aging clinical workforce, a decrease in nursing school applicants is a
concern. The AACN suggests that nursing schools have too few seats to address
the shortage due to fewer teaching faculty and facilities. As fewer people pursue
careers in nursing, a tsunami of retiring nurses is exacerbating the shortage.
An experience gap among nurses is another issue that negatively impacts
nursing. As newer nurses simply do not possess the same experience the retiring
workforce holds, this creates a substantial gap in the quality of care. Training time
among newer nurses has shortened, yet the care complexities of the aging
population has intensified. The Advisory Board Executive Nursing Center recently
published the "Experience-Complexity Gap” citing another dimension to the
shortage [33]. Their findings emphasize the importance of precepting early-career
nurses more effectively. The development of standardized preceptor programs
and redistributing and differentiating experienced nursing staff to ensure high-
quality preceptor programs can be an effective means of training novice nurses.
This experience gap has a significant impact on the quality of care, noting that
novice nurses recognize signs/symptoms in deteriorating patients less effectively. In addition, the experience gap can
contribute to a rise in the number of medication errors. A report by HealthAffairs estimates in 2015 showed health care
lost 1.7 million years of clinical experience when nearly 60,000 nurses retired – a staggering number that ultimately
affects staffing, retention, workload and attitudes within the profession, contributing to work stress and eventual burnout
[34].
Technology
The Health Information Technology for Economic & Clinical Health (HITECH) act of 2009 was passed to promote the
adoption of electronic health records (EHR) to improve quality, safety and efficiency. This legislation outlined provisions
for data protection and security and gave the newly created Office of National Coordinator for Health Information
Technology (ONC) authority to set standards in EHR technologies and stimulate incentives through demonstrated
meaningful use of EHRs. As new rules were published, and the measures instituted by CMS & ONC became
increasingly complex, providers became increasingly pressured to meet Meaningful Use measures and adopt the
technology at a rapid pace.
Meeting the regulatory demands of technology adoption itself took a toll on clinicians’ experiences and the promises
technology would bring. Similarly, EHR vendors were required to hastily adapt solutions to pass regulatory muster.
Within a few years, physicians began blaming the EHR as a significant contributor to burnout [35]. Research, opinion
pieces and health care IT publications discuss how the EHR contributes to clinician burnout. The combination of growing
regulatory requirements, health care administrative goals, payor demands and the resulting mismatch in care processes
and application workflows created the perfect storm for EHR- related burnout.
A report by HealthAffairs
estimates in 2015,
Health care lost
1.7 million years of clinical
experience when nearly
60,000 nurses retired – a
staggering number that
ultimately affects staffing,
retention, workload, and
attitudes within the
profession contributing to
work stress and eventual
burnout [34].
8
The use of the EHR is still largely manual and the amount of data collected can frequently be perceived to be not
necessarily relevant to patient care. Yet clinicians spend an average of 2-3 hours a day in extra screen time (all clinicians
combined). Christine Sinksy, MD, Vice President of Professional Satisfaction at the American Medical Association refers
to this as “work outside of work,” frequently called “pajama time.” [36]. A study by Hendrich, et al., reported that nurses
spend approximately 35% of their time documenting, 21% of their time coordinating patient care and only 19% on direct
patient care [37]. In general, the nursing profession lacks documentation standards, leading to excessive, unnecessary
documentation and administrative documentation that could be delegated to non-clinical staff. Similarly, physicians
spend up to 73% of their time on non-clinical tasks as newer technology forces more screen time in the form of inbox
communication, portal messaging with patients and other non-reimbursable tasks [38]..
After over a decade of inputting data into EHR systems, clinicians often find it
difficult to effectively extract data in the form of patient knowledge discovery,
adding to the frustration of working with EHRs. Clinicians are drowning in a sea of
patient data.
Surveys indicate that clinical, top-of-license care process workflows are disrupted
by technology in the form of alerts, errors and excessive documentation. The
Annual Physician Lifestyle Report (Medscape survey) indicates that, over the last
five years, the top three themes indicated as the most significant burnout causes
were excessive paperwork and charting, spending too much time at work and
increased use of the EHR [39]. Other important findings from the survey include a
lack of interoperability, redundant data gathering, unintuitive or non-user-friendly
systems and too much manual effort [1]. For example, the sending of Continuity
of Care Documents (CCDs) between physicians – if not automated, can lead to
an unmanageable administrative burden. Regulatory mandates, like this and
others, take doctors away from the patient-physician interaction. From a pure
clinician perspective, the same themes repeat in terms of not meeting the actual needs of the clinician: poor system
usability, non-integrated systems, poor interoperability, lack of documentation standards, limited functionality/missing
components and redundant data gathering (overlapping data collection with other clinical disciplines) [40,41].
Alert fatigue also plays a central role in burnout. The U.S. Agency for Healthcare Research and Quality (AHRQ) defines
alert fatigue as “workers (in the case of health care, clinicians) become desensitized to safety alerts, and as a result,
ignore or fail to respond appropriately to such warnings. This phenomenon occurs because of the sheer number of
alerts, and it is compounded by the fact that the vast majority of alerts generated by CPOE systems (and other health
care technologies) are clinically inconsequential, meaning that in most cases, clinicians should ignore them. The problem
is that clinicians then ignore both the bothersome, clinically meaningless alarms and the critical alerts that warn of
impending serious patient harm.” [42].
The medical field has seen many advancements, and the industry is just beginning to identify how technology could
invariably enhance medicine while reducing current clerical, manual aspects of the EHR. We are nearly fully digitized but
not yet transformed. As the industry grows by way of apps on FHIR®, artificial intelligence and virtual assistants,
business intelligence and natural language processing, vendors are beginning to standardize their code to enable better
communication and integration. Health care software vendors and third-party companies are developing ways to capture
conversations (between patient and provider) through natural language processing (NLP), to identify relevant information
related to the visit (pulling from all data in the record and the conversation) and to suggest tests/treatments all while
compiling a note without the provider touching a keyboard.
Historically, nurses have manually collected massive amounts of patient data which has swelled since the advent of
digitization. System customizations have gotten expansive to the point that some of the data collected is arguably not
clinically relevant and probably will never be consumed. Until recently, the nursing industry continued to function the
same as they had on paper [43]. Over the past few years, work efforts to review clinical documentation processes and
content have emerged. Nursing leaders are coming together to discuss standard content for nursing documentation that
will ensure relevant, timely data collection and pave the way for effective data sharing between clinical teams. Changes in
content and timing of collection will potentially show an increase in time efficiencies and more accurate documentation;
however, transformation has yet to be realized for nursing as well.
After over a decade of
inputting data into EHR
systems, clinicians often
find it difficult to
effectively extract data in
the form of patient
knowledge discovery,
adding to the frustration
of working with EHRs.
Clinicians are drowning
in a sea of patient data.
9
In the era of health care reform and a focus on patient-centered care, patients expect safe, high-quality care. Health care
organizations’ focus on improving the ways in which clinicians can successfully carry out their responsibilities directly
affects patient satisfaction and may contribute to higher levels of patient safety and quality of care [44]. Cimiotti, et al.,
discovered a significant link between health care associated infection (a nursing sensitive indicator), workload,
leadership support and education. An emphasis on nurse engagement, professional development and appropriate
staffing mix may pave the way to increase nurse retention rates and help renew nurses’ sense of resilience.
Beating burnout
Engagement level and resilience plays a significant role in clinician retention. Research points to a combination of
individual programs and an organizational approach to creating less stressful work environments [45,46]. Focusing on
staff wellness and safety enhances health system improvements and performance.
Staff wellness proves to be most impactful when hospital leadership emphasizes their commitment to employee well-
being. Health care organizations may approach this concept by instituting practice models that encourage a professional
workplace environment, emulating top employers across the country [48,49]. Empowering clinicians by giving them a
seat at the table with regard to clinical practice decisions has shown to improve
commitment to their respective professions and place of employment. This
provides a renewed sense of professionalism and commitment to safety elicited
from evidence-based practice. This framework encourages interdisciplinary
collaboration and workforce engagement, which has been shown to increase
clinician and patient satisfaction, retention and improved safety. Simply put, a
healthy practice environment points to decreased burnout.
Resilience plays a key role in burnout and retention. Given the evidence, it is
imperative that health care leaders remove barriers, bolster communication and
provide ways for caregivers to identify and acknowledge clinicians’ basic and
psychological needs in the workplace [50]. Instituting and engaging employees
in individual wellness programs can help increase clinicians’ coping
mechanisms against the impacts of a stressful health care environment [51].
Wellness programs and educational offerings in communication skills, team
building and emotional intelligence provide support and a sense of
understanding. These types of programs can increase self-confidence and
provide a sense of personal achievement which aids in boosting coping
mechanisms [52,53]. According to the Institute for Healthcare Improvement,
“…health is more than the absence of disease, so too joy is more than the
absence of burnout.” [54].
The Stanford Medical Center WellMD program engages physicians in regular surveys and wellness programs.
Accordingly, the Stanford program “focuses on the need for professional fulfillment rather than simply the avoidance of
burnout.” Stanford recognizes that burnout is multidimensional and approaches it as such [47]. Even diet may play a role
in burnout. A new area under investigation at Stanford is the part diet plays in physician performance and how it may
impact burnout.
Empowering clinicians
by giving them a seat at
the table about clinical
practice decisions
improves commitment to
their respective
professions and place of
employment. This
provides a renewed
sense of
professionalism,
commitment to safety
and evidence-based
practice.
10
.
The Mayo Clinic encourages physicians to form peer groups of 6-7 physicians and meet every two weeks during one
hour of protected time. The COMPASSS trial COMPASS (Colleagues Meeting to Promote and Sustain Satisfaction)
found that these meetings with colleagues led to an improvement in both meaning in work and burnout for participants.
This, and other programs like it, help improve professional satisfaction.
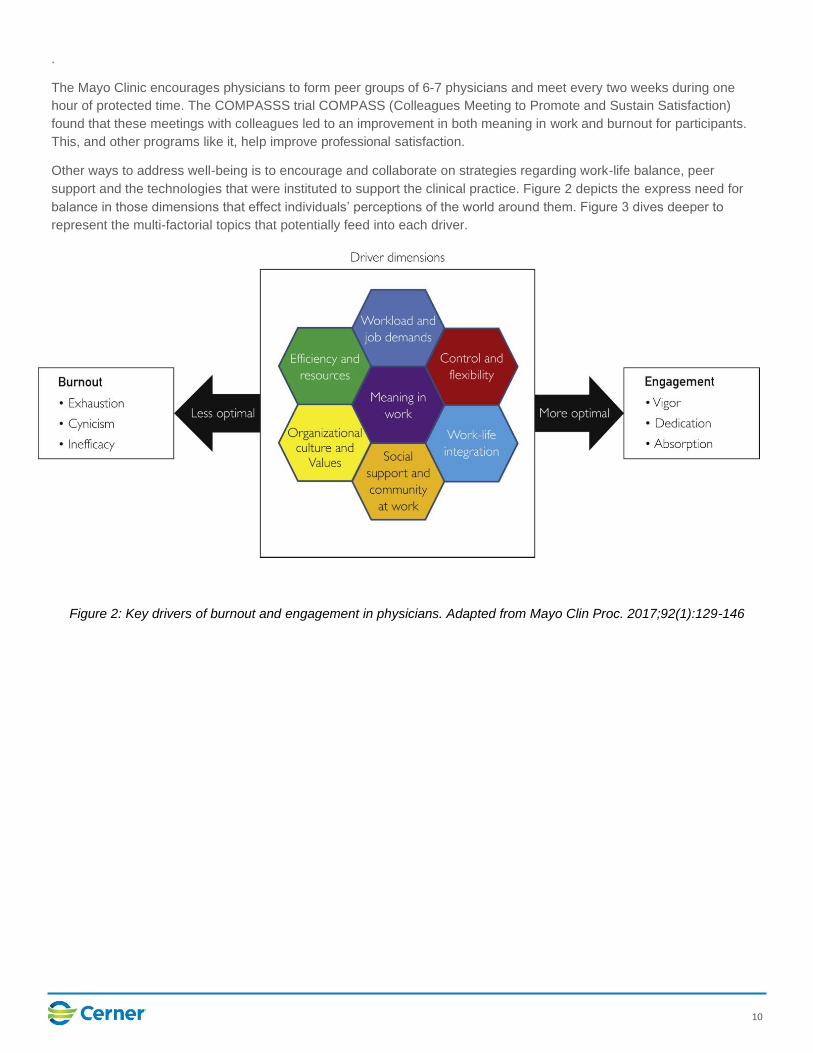
Other ways to address well-being is to encourage and collaborate on strategies regarding work-life balance, peer
support and the technologies that were instituted to support the clinical practice. Figure 2 depicts the express need for
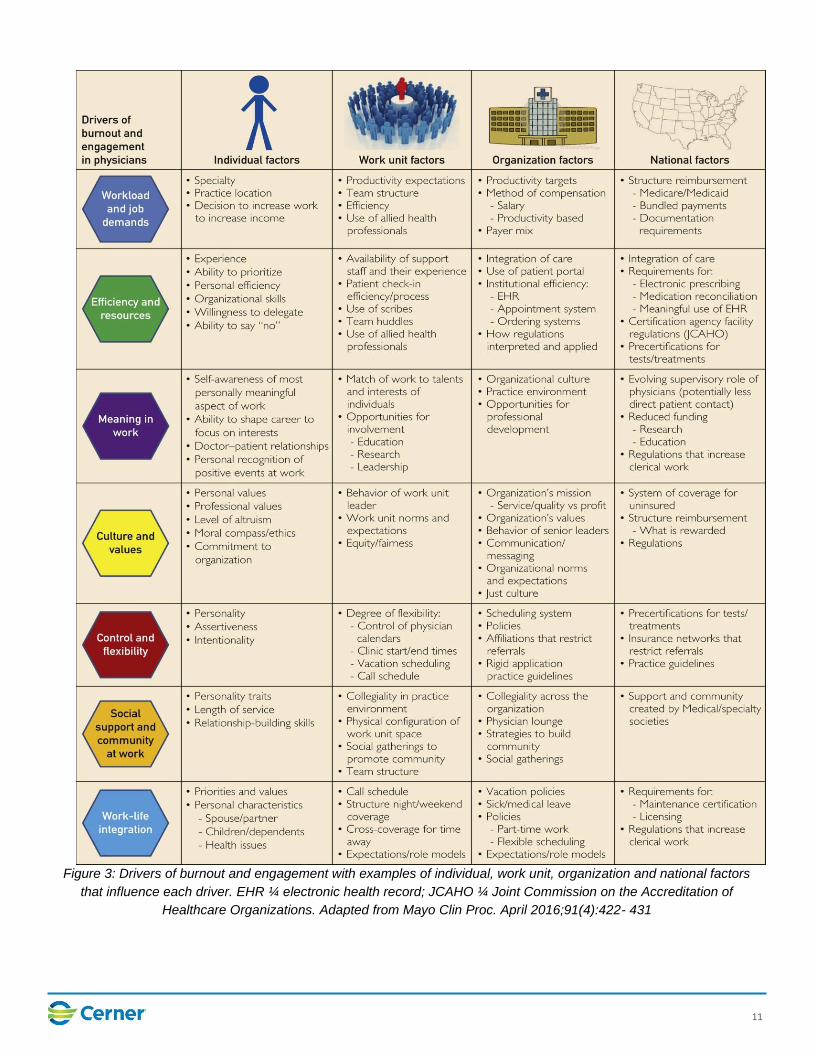
balance in those dimensions that effect individuals’ perceptions of the world around them. Figure 3 dives deeper to
represent the multi-factorial topics that potentially feed into each driver.
Figure 2: Key drivers of burnout and engagement in physicians. Adapted from Mayo Clin Proc. 2017;92(1):129-146
11
Figure 3: Drivers of burnout and engagement with examples of individual, work unit, organization and national factors
that influence each driver. EHR ¼ electronic health record; JCAHO ¼ Joint Commission on the Accreditation of
Healthcare Organizations. Adapted from Mayo Clin Proc. April 2016;91(4):422- 431
12
Strategies to reduce burnout related to technology
1. Culture – Unfavorable organizational culture is an important predictor of clinician burnout. Clinician engagement is
related to the practice of participative management, social support and team interaction. Engaged staff members
exhibit more organizational citizenship behavior which benefits the organization. A culture of engagement is also
associated with overall superior performance. Physicians experience highest levels of engagement when they have
an acceptable degree of control over their work environment. Engaged physicians tend to receive higher patient
satisfaction ratings on patient surveys. Evidence also suggests that organizations with high staff morale outperform
those with low morale [46].
2. Training and education strategies – Provide consistent and efficient training sessions and targeted ongoing
education when needed. The KLAS Arch Collaborative demonstrates that an increase in training hours is highly
correlated with improved physician satisfaction [58]. Furthermore, continuous training programs have demonstrated
higher degrees of clinician satisfaction with the EHR. These programs are useful when new functionality is added to
the EHR, when code upgrades are implemented and when new regulatory rules are issued.
Cerner works to provide optimal educational and training products and services. Implementing a winning strategy
with adoption coaches at the elbow support, experienced clinical professionals and online training are just a few
ways we strive to help care organizations realize optimal training with the EHR.
3. EHR personalization – A qualitative assessment found that physicians value personalization of their individual
experiences with EHR systems [58].
The Millennium® EHR platform is designed to meet the specific capabilities of individual health care systems, clinical
and medical specialties and individual preferences. Following our Model Experience, a standard for adoption, we
deliver a user experience that grows with the evolving needs of care organizations. The Model Experience includes
workflow views that are personalized to specialties and venues of care. It is built for the needs of individual roles and
supports a streamlined chart review process that allows users to review data, document and make clinical decisions
without chart hopping, which may improve efficiency.
4. Clinician participation in innovation – The American Medical Association, the American Medical Informatics
Association and the American Nurses Association all encourage clinicians to participate in EHR design, system
workflow correlation to clinical practice and testing, giving them a seat at the table. Best practice is to support
standardization of technology and care process workflows which allows for the best possible adoption outcomes, as
well as a more seamless transition when taking new updates to EMR software.
Cerner recommends clinicians, particularly nurses, physicians and pharmacists, to be active participants in their
organization’s health care IT (HIT) governance process. When clinicians are fully engaged in a structured manner,
implementations tend to be more successful by every measure. As a participating member of the HIT governance
process, physicians and nurses secure their place in making decisions about the technology that supports and
impacts their practice and patient outcomes. Effective governance is challenging for most organizations regardless
of size or complexity and crucial to assuring technology supports business and clinical needs – aligning with the
strategic plan. [55,56]
13
.
5. Understand and reform practice inefficiencies – User data and time motion studies
performed by informatics teams provide information to assess specific support
needs and can highlight where efficiencies in care processes can be gained.
Cerner Lights On Network® and Cerner Advance, the Cerner user analytics
platform, provides helpful user data at the facility, unit and individual levels.
Rounding informatics teams trained to observe care process workflows and assess
for standardization and workarounds add weight to the Advance data that coincides
to provide guidance toward standardization and effective EHR use [57].
6. Streamlining physician documentation - Four major factors influencing satisfaction
with electronic documentation tools are time efficiency, availability/accessibility,
expressivity and quality [59]. Embedded voice recognition software, the use of
scribes, macros like dot phrases and typing are the most widely used methods to
document. A combination of these is a common approach. Evidence is unclear on
exactly which type of documentation strategy is optimal, suggesting that
documentation strategies are largely dependent on end-user preferences.
Cerner is leading the charge in documentation improvement with Virtual Scribe,
powered by AWS (Amazon Web Services) engine. It is an intelligent system that
captures voice and transcribes the patient visit in real time.
7. Standardized nursing documentation – The ANA advocates for the standardization of nursing documentation as it helps
to reduce cognitive burden, increase efficiency and allow for more direct patient care time, ultimately supporting better
patient outcomes [60].
The Essential Clinical Dataset (ECD) is the Cerner answer to address the need to standardize nursing documentation
globally, regardless of vendor [61]. The ECD provides the means to assure the necessary elements are presented for
documentation as determined by evidence based practice, regulatory requirements and practice based evidence.
8. Standardized ordersets – Reduction in serious medication errors have clearly been shown by using standardized
ordersets (Bates, et al., JAMA, 1998). The rationale for ordersets are to reduce the time required to enter orders, to
reduce errors and to increase accuracy during order entry. Furthermore, they should increase the completeness of
orders, have “built-in” decision support and evidence-driven care and reduce the variability in the care process enhancing
compliance with best practices.
9. Normalize alerts – Reduce alert fatigue. The design of mindful, helpful and appropriate alerts will help reduce alert
fatigue. For example, one study noted the creation of a list of 33 class-based, low-priority drug-drug interactions (DDI) do
not warrant being interruptive alerts in the EHR. In one institution, these accounted for 36% of the interactions displayed
[62].
Cerner has developed analytics dashboards to measure the effectiveness and types of alerts (interruptive vs passive
alerts) so to move the unnecessary, disruptive alerts within clinical workflow to a less conspicuous space.
10. Ensure clinical decision support (CDS) is effective – Following the five rights of clinical decision support: right
information, right person, right format, right channel and right time are useful in designing appropriate and well- regarded
systems. Recognizing that CDS is not a means to replace decision making by clinicians, it can certainly reduce cognitive
burden and call out subtle clinical findings for clinicians to consider.
11. Enabling team-based care – distributing the burden or work of providing care among multiple team members can be part
of the solution to alleviate clinician burnout. Concepts include multi-contributor patient care and documentation, message
pools, integrated care planning and discharge process, which highly emphasize social support structures within the
workplace [9].
The ANA advocates for
the standardization of
nursing documentation
as it helps to reduce
cognitive burden,
increase efficiency and
allow for more direct
patient care time,
ultimately supporting
better patient outcomes
[60].
14
How is Cerner helping?
All of health care is moving at a rapid pace from digitized health care (a substitution for paper) to data-enabled
transformational changes in the industry. As we enter a new age promised by artificial intelligence (AI), machine learning,
blockchain and other advancements, Cerner will continue to lead the industry in reducing clinician burnout. We have
pivoted from simplified documentation and order entry to truly intelligent systems that leverage patient data to recognize
sepsis, SIRS, obstetric emergencies and many others. It is for this reason we have developed the Cerner Now/Next
concept. Among many initiatives, Now/Next keeps care organizations current on innovations with targeted software
updates. This can help a hospital system stay current with regulation, maintain healthy populations and satisfy payor
requirements.
It is doubtful that AI and machine learning would ever fully replace physician decision making. It will, rather, augment
decision making for clinicians. For example, within 30 seconds or so of a face-to-face conversation with a patient, the
average clinician can determine patient anxiety levels and emotions, educational level, general income bracket, ability to
leverage resources, medication compliance likelihood and other factors. Clinicians then rapidly adapt to interact with a
patient based on these observations.
What if a truly intelligent system objectively captured data points that aid the clinician in providing appropriate resources
to uplift and prevent patients from slipping through the cracks? It takes a clinician time and effort to search for
appropriate resources that match patients’ needs. We are leveraging artificial intelligence engines that help clinicians do
their job better.
Cerner is a participant in the ENABLE Study (Evaluation of Novel electronic health record use metrics and their
Association with Burnout and plans to Leave practice), funded by the American Medical Association, in collaboration with
Yale University and MedStar Health. Coauthoring the study is Dr. Anup Salgia. This paper will investigate the cause and
effects of physician burnout as it relates to the EHR. The findings from studies like this and others are already making a
positive impact in designing an optimal physician experience with Cerner solutions.
Improving the clinician workflow
To address these issues, Cerner is working to create a unified, efficient and standard experience for all clients through
several initiatives. These initiatives and suggestions are designed to help make the physician’s day easier
Adoption coaching
We understand that the more support and ongoing education we provide to our physician end users beyond go-live, the
greater satisfaction we see. Cerner adoption coaching services offer a full-scale model designed to help ensure
successful end-user adoption. We provide the support and guidance to help implement and optimize Cerner solutions to
increase user adoption, improve efficiency and improve user satisfaction. Coaching also allows for knowledge sharing
between peers and uses data analytics to benchmark local specialties against national user data.
Advanced interoperability
Interoperability allows clinicians to exchange and use patient information in near real time to make clinical decisions for
their patients. Cerner is a founding member of the CommonWell Health Alliance, a not-for-profit trade association
devoted to the simple vision that health data should be available to individuals and caregivers regardless of where care
occurs. To date, Cerner has connected the health care data of millions of patients securely with clinicians worldwide. Our
efforts in this realm are unparalleled in the industry.

15
Cerner.NEXT
The expanded Cerner-AWS (Amazon Web Services) collaboration is enabling physicians to make intelligent data-driven
decisions. This is being built on a massive foundation of data that is being scaled up to build a clinical decision support
infrastructure that improves patient care and patient outcomes.
Evolving the EHR
Work to advance care process workflows by enhancing the user experience and focusing on intuitive application design. Cerner invests in contemporary technologies such as natural language processing and an array of artificial intelligence solutions.
Human factors engineering team
Comprised of interaction and visual designers, human factors researchers and design strategists, this team is committed
to designing solutions around the end-user, creating consistent experiences for our clients. We do this by enhancing
workflows through advanced design practices, end-user feedback and current usability research, ensuring that the
perspective we gain during our research is from individuals who actively use the solutions being tested.
Product design workgroups
Cerner is committed to improving the EHR in partnership with clients, including the ENABLE study mentioned above, as
well as our focused clinician groups, such as the nursing client council and physician workgroups and affinity
groups/councils.
Learning framework
Our new approach to contemporary learning combines self-paced education in a variety of methods. This new blended
learning approach is prescriptive, engaging and role-based. It provides a well-rounded, multi-phased learning process to
help the learner stay on track in their learning journey.
Model system
The Cerner collection of strategic recommendations for leveraging best practices in outcomes excellence, for process
alignment and for health system experiences contribute to the optimal setup and use of the EHR. Adopting these sets of
recommendations allow clinicians and staff to perform at the top of their licensure.
Open standards
Cerner has delivered on its pledge to allow developers to advance physician usability using API/FHIR integration. There
are several apps in our app store that address specific clinical workflows such as anesthesiology, dermatology and
others. For more information, visit code.cerner.com (Cerner Open).
Regulatory
Cerner will remain an advocate at the national and state levels to lend a voice in the industry that benefits both patients
and clinicians alike.
16
Leadership education tools
In addition to the strategies mentioned, Cerner hosts workshops and programs to educate hospital, nursing and physician leadership on the skills necessary to address clinician burnout.
Cerner Advance
Delivering the best EHR experience to your clinicians is critical to their productivity, satisfaction and ability to deliver high-
quality outcomes. Cerner Advance is a tool to provide visibility to the clinician experience by bringing together end-user
data and expert analysis on a single platform.
Cerner Health Conference
Cerner hosts a weeklong annual conference that is attended by 10,000+ attendees who represent hundreds of clients
from across the globe. The conference fosters collaboration and networking in addition to providing updates to clients on
future developments at Cerner.
Clinical Community Forum
Meetings and activities specifically for clinicians who use Cerner solutions in practice.
CNO/CNIO Summit
The three-day annual meeting hosted by Cerner is specifically designed for CNOs/CNIOs to network with fellow CNOs,
CNIOs and Cerner associates. The summit is an excellent opportunity to discuss and learn about nursing-related
industry topics.
Physician, Nursing & Informatics Leadership Workshops
Increasing clinician leadership skills will assist with decreasing the rate of burnout. Cerner provides a workshop to
address core knowledge and skills nursing and physician leaders need in the dynamic health care environment with a
major focus on change management, leadership and governance.
Physician Architect Program
Cerner offers a program developed by physicians for physicians to help bridge the gap between the clinical and technical
aspects of Cerner solutions. This interactive course gives physicians an in-depth understanding of software
configurations, privileges, preferences and architecture. With this knowledge, physicians can have better conversations
with their IT colleagues in designing a system that works optimally for their particular institution.
Professional fulfillment and improved wellness
Below are other areas of focus above and beyond the EHR to help increase professional fulfillment and improve
clinician wellness.
Health care IT operations governance
Effective governance is critical and challenging for most organizations regardless of size or complexity. Clinical
representation and inclusion within the process is key to ensure the necessary input and successful adoption of the
invested technology selected to support clinical practice and business operations.
Change management (C.L.E.A.R.)
It has been said that change is the only constant in life. In 2019, Cerner made a commitment to helping clients manage
change by creating a consulting group that specifically addresses change management. Using the most tested
techniques, this offering can help manage culture in an ever-changing technology world. Whether a health care
organization is taking a software upgrade or a full EHR implementation, our change management group can provide the
tools and resources to simplify the most complex of software implementations.
EHR optimization
Invest in optimizing the EHR. Streamline workflows, reduce required activities and data entry, and ensure clinicians are
practicing at the top of their license. Provide the necessary staff to help with data entry and chart prep, ultimately
generating better reimbursement.
Workforce management
Cerner Clairvia℠ to ensure that care organizations balance the ideal utilization of nursing resources, especially as
technology becomes a key lever for success.
Cerner views clinician burnout as a serious threat to the entire health care industry. We are optimistic that technology will
continue to lead the way to improved clinician experiences. The first step in reducing clinician burnout is to acknowledge it
exists, then discover the cause and effect, and finally put actions in place to lower stress and create work-life balance.
References
1. Medscape Lifestyle Report 2017: Race and Ethnicity, Bias and Burnout. Accessed October 1, 2019 from
https://www.medscape.com/features/slideshow/lifestyle/2017/overview#page=1
2. Reith, T.P. (2018) Burnout in United States Healthcare Professionals: A Narrative Review. Cureus 10 (12): e3681. DOI
10.7759/cureus.3681
3. Maslach, C, Jackson, S (1981). The measurement of experienced burnout. Journal of Occupational
Behaviour, Vol. 2, 99-113 (1981)
4. NIOSH. Stress at Work. Cincinnati, OH: U.S. National Institute for Occupational Safety and Health; 1999. DHHS
(NIOSH) Publication Number 99–101.
5. Khamisa, N., Peltzer, K., & Oldenburg, B. (2013). Burnout in relation to specific contributing factors and health outcomes among nurses: a systematic review. International journal of environmental research and public health, 10(6), 2214–2240. doi:10.3390/ijerph10062214
6. CNN Health 2019. Burnout is an official medical diagnosis, World Health Organization says. Accessed October 2019
https://www.cnn.com/2019/05/27/health/who-burnout-disease-trnd/ index.html
7. Aiken, L. et al (2012). Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and
patients in 12 countries in Europe and the United States. BMJ 2012;344:e1717 doi: 10.1136/bmj.e1717
8. Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and health care-associated infection [published
correction appears in Am J Infect Control. 2012 Sep;40(7):680]. Am J Infect Control. 2012;40(6):486–490.
doi:10.1016/j.ajic.2012.02.029
9. National Academies of Sciences, Engineering, and Medicine. 2019. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. Washington, DC: The National Academies Press. https://doi.org/10.17226/25521.
10. Aiken, L.H., Clarke, S.P., Sloane, D.M., Sochalski, J., Silber, J.H. (2002) Hospital Nurse Staffing and Patient Mortality,
Nurse Burnout, and Job Dissatisfaction. JAMA October 23/30, 2002-Vol 288, No. 16
11. EHR Optimization: A Prescription for Clinician Burnout. Tactics to promote clinician wellness. Webcast accessed September 4, 2019 from https://www.advisory.com/research/health-care-it- advisor/events/webconferences/2019/2019-health-care-it-advisor-virtual-summit/ehr-optimization-a- prescription-for-clinician-burnout/ondemand
12. Moss M., Good V.S., Gozal D., Kleinpell R., Sessler C.N. An Official Critical Care Societies Collaborative Statement:
Burnout Syndrome in Critical Care Health Care Professionals: A Call for Action. Am. J. Crit. Care. 2016;25:368–376. doi:
10.4037/ajcc2016133.
13. Wright A.A., Katz I.T. Beyond Burnout—Redesigning Care to Restore Meaning and Sanity for
Physicians. N. Engl. J. Med. 2018;378:309–311. doi: 10.1056/NEJMp1716845.
14. Shanafelt TD, Balch CM, Dyrbye L, et al. Special Report: Suicidal Ideation Among American Surgeons. Arch Surg.
2011;146(1):54–62. doi:10.1001/archsurg.2010.292
15. Lee R.T., Seo B., Hladkyj S., Lovell B.L., Schwartzmann L. Correlates of physician burnout across regions and specialties: A meta-analysis. Hum. Resour. Health. 2013;11:48. doi: 10.1186/1478-4491- 11-48.
16. Brown S.D., Goske M.J., Johnson C.M. Beyond substance abuse: Stress, burnout, and depression as causes of physician impairment and disruptive behavior. J. Am. Coll. Radiol. 2009;6:479–485. doi: 10.1016/j.jacr.2008.11.029.
17. Miller C. What is the Price of Physician Stress and Burnout? {(accessed on 1 August 2018)]; Available online: http://www.medicaleconomics.com/medical-economics/news/what-price-physician-stress-and-burnout.
18. West C.P., Tan A.D., Shanafelt T.D. Association of resident fatigue and distress with occupational blood and body fluid
exposures and motor vehicle incidents. Mayo Clin. Proc. 2012;87:1138–1144. doi: 10.1016/j.mayocp.2012.07.021.
19. Shanafelt T.D., Sloan J.A., Habermann T.M. The well-being of physicians. Am. J. Med. 2003;114:513
–519. doi: 10.1016/S0002-9343(03)00117-7.
20. Bianchi R., Schonfeld I.S., Laurent E. Burnout-depression overlap: A review. Clin. Psychol. Rev.
2015;36:28–41. doi: 10.1016/j.cpr.2015.01.004.
21. Asai M., Morita T., Akechi T., Sugawara Y., Fujimori M., Akizuki N., Nakano T., Uchitomi Y. Burnout and psychiatric morbidity among physicians engaged in end-of-life care for cancer patients: A cross- sectional nationwide survey in Japan. Psychooncology. 2007;16:421–428. doi: 10.1002/pon.1066.
22. Oreskovich M.R., Kaups K.L., Balch C.M., Hanks J.B., Satele D., Sloan J., Meredith C., Buhl A., Dyrbye L.N.,
Shanafelt T.D. Prevalence of alcohol use disorders among American surgeons. Arch. Surg. 2012;147:168–174. doi:
10.1001/archsurg.2011.1481.
23. Carter, S. 2012. Emotions are Contagious-Choose Your Company Wisely. Second hand emotions: the good, the bad,
and the ugly. Accessed September 30, 2019 https://www.psychologytoday.com/ us/blog/high-octane-
women/201210/emotions-are-contagious-choose-your-company-wisely
24. Blog: Reflected on the Mind. The Ripple Effect (Emotional Contagion in Groups). March 2013. Accessed October 1, 2019
http://reflectd.co/2013/03/25/the-ripple-effect-emotional-contagion- transferring-moods-to-others/
25. Dunford, Benjamin B.1
; Boss, Wayne R.2; Boss, Alan D.
3; Zara, George A.
4; Grooms, Richard W. Jr.
5 Can Entire
Departments Be Burned Out? A Conservation of Resources Perspective on Burnout Contagion, Journal of Healthcare
Management: July-August 2014 - Volume 59 - Issue 4 - p 305-306
26. IHS Markit, 2019. Prepared for Association of American Medical Colleges. The Complexities of
Physician Supply and Demand: Projections from 2017-2032.
27. U.S. Bureau of Labor Statistics (2018). Employment outlook for bachelor’s-level occupations. Accessed on May 23, 2019
https://www.bls.gov/careeroutlook/2018/article/bachelors-degree- outlook.htm#Healthcare%20and%20science
28. U.S. Department of Health and Human Services. The Future of Nursing Workforce: National and State-level Projections 2012-2025 (2014). Access October 28, 2019 https://bhw.hrsa.gov/sites/ default/files/bhw/nchwa/projections/nursingprojections.pdf
29. Nurse life (2018). RNnetwork 2018 Portrait of a Modern Nurse Survey. Access October 29, 2019
https://rnnetwork.com/blog/rnnetwork-2018-portrait-of-a-modern-nurse-survey/
30. American Association of Colleges of Nursing Fact Sheets 2019. Accessed November 1 https://
www.aacnnursing.org/News-Information/Nursing-Shortage-Resources/About
31. U.S. Department of Health and Human Services. The Future of Nursing Workforce: National and State-level Projections 2012-2025, Talking points. Accessed May 23 https://www.aacnnursing.org/ Portals/42/News/Nursing-Shortage/HRSA-Nursing-Workforce-Projections.pdf?ver=2017-12-11- 115743-493
32. American Association of Colleges of Nursing Fact Sheet: Nursing Shortage (2019). Accessed November 1 https://www.aacnnursing.org/Portals/42/News/Factsheets/Nursing-Shortage- Factsheet.pdf
33. Advisory Board (2019). The Experience-Complexity Gap. Accessed August 20 https:// www.advisory.com/research/nursing-executive-center/resources/2019/the-experience-complexity- gap?
WT.mc_id=Email|Q319|RESEARCH+DOM|NEC|ResRep|ExpCompGap|83632|&elq_cid=3889656&x
_id=003C000002QTVmuIAH
34. Health Affairs Blog How should we prepare for the wave of retiring baby boomer nurses? (2017).
Accessed October 1, 2019 https://www.healthaffairs.org/do/10.1377/hblog20170503.059894/full/
35. Shanafelt, Tait D. et al. Relationship Between Clerical Burden and Characteristics of the Electronic Environment with
Physician Burnout and Professional Satisfaction. Mayo Clinic Proceedings, Volume 91, Issue 7, 836 – 848
36. EHR Optimization: A Prescription for Clinician Burnout. Tactics to promote clinician wellness. Webcast accessed
September 4, 2019 https://www.advisory.com/research/health-care-it-advisor/ events/webconferences/2019/2019-
health-care-it-advisor-virtual-summit/ehr-optimization-a- prescription-for-clinician-burnout/ondemand
37. Hendrich, A., Chow, M. P., Skierczynski, B. A., & Lu, Z. (2008). A 36-hospital time and motion study: how do medical-surgical nurses spend their time?. The Permanente journal, 12(3), 25–34. doi:10.7812/tpp/08-021
38. EHR Optimization: A Prescription for Clinician Burnout. Tactics to promote clinician wellness. Webcast accessed September 4, 2019 https://www.advisory.com/research/health-care-it-advisor/ events/webconferences/2019/2019-health-care-it-advisor-virtual-summit/ehr-optimization-a- prescription-for-clinician-burnout/ondemand
39. Reith T P (December 04, 2018) Burnout in United States Healthcare Professionals: A Narrative
Review. Cureus 10(12): e3681. DOI 10.7759/cureus.3681
40. Topaz, M., Ronquillo, C., Peltonen, L. M., Pruinelli, L., Sarmiento, R. F., Badger, M. K., Ali, S., Lewis, A., Georgsson, M., Jeon, E., Tayaben, J. L., Kuo, C. H., Islam, T., Sommer, J., Jung, H., Eler, G. J., Alhuwail, D., & Lee, Y. L. (2017). Nurse Informaticians Report Low Satisfaction and Multi-level Concerns with Electronic Health Records: Results from an International Survey. AMIA ... Annual Symposium proceedings. AMIA Symposium, 2016, 2016–2025.
41. How disparate EHR systems, lack of interoperability contribute to physician stress, burnout. The evolution of the
patchwork EHR landscape has been complex, and one expert traces the problem back to meaningful use. https://www.healthcareitnews.com/news/how-disparate-ehr-systems-lack- interoperability-contribute-physician-stress-burnout. Accessed October 3, 2019
42. Ancker, J. S., Edwards, A., Nosal, S., Hauser, D., Mauer, E., Kaushal, R., & with the HITEC Investigators (2017). Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC medical informatics and decision making, 17(1), 36. https:// doi.org/10.1186/s12911-017-0430-8
43. Harrington, L. Future Model for Nursing Documentation: Extinction. Nurse Leader VOLUME 17, ISSUE 2, P113-116,
APRIL 01, 2019 DOI:https://doi.org/10.1016/j.mnl.2018.12.005
44. McHugh, M.D., Kutney-Lee, A.,Cimiotti, J.P., Sloane, D.M., Aiken, L.H. Nurses’ Widespread Job
Dissatisfaction, Burnout, And Frustration With Health Benefits Signal Problems For Patient Care. Health Aff (Millwood) . 2011 February ; 30(2): 202–210. doi:10.1377/hlthaff.2010.0100. Accessed September 11, 2019
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3201822/pdf/nihms285341.pdf
45. Roberts, R. K., & Grubb, P. L. (2014). The consequences of nursing stress and need for integrated solutions. Rehabilitation nursing: the official journal of the Association of Rehabilitation Nurses, 39 (2), 62–69. doi:10.1002/rnj.97. Accessed May 24, 2019 https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC4664060/
46. Swensen, Stephen MD; Kabcenell, Andrea RN; Shanafelt, Tait MD (2016). Physician-Organization Collaboration Reduces Physician Burnout and Promotes Engagement: The Mayo Clinic Experience. Journal of Healthcare Management: March 2016 - Volume 61 - Issue 2 - p 105–127
47. Dyrbye LN, Shanafelt TD. Physician burnout: a potential threat to successful health care reform.
JAMA. 2011;305(19):2009–2010. doi:10.1001/jama.2011.652
48. Grayson, R. (2018). Creating the Framework for a healthy Practice Environment. JONA, October
2018, vol. 48 no. 10, 469-470
49. Cordo, J., Hill-Rodriquez, D. (2017). The Evolution of a Nursing Professional Practice Model Through Leadership
Support of Clinical Nurse Engagement, Empowerment and Shared Decision Making. Nurse Leader, October 2017, vol.
15 no 5, 325-330
50. Swensen,S.J., Shanafelt, T. An Organizational Framework to Reduce Professional Burnout and Bring Back Joy in Practice. The Joint Commission Journal on Quality and Patient Safety 2017; 43:308–313
51. Rushton, C.H., Batcheller, J., Schroeder, K., Donohue, P. Burnout and Resilience among Nurses Practicing in High-intensity Settings. Am J Crit Care September 2015 vol. 24 no. 5 412-420
52. Dempsey, C., Reilly, B., (January 31, 2016) "Nurse Engagement: What are the Contributing Factors for Success?"
OJIN: The Online Journal of Issues in Nursing Vol. 21 No. 1, Manuscript 2.
53. Darban, F., Balouchi, A., Narouipour, A., Safarzaei, E., & Shahdadi, H. (2016). Effect of Communication Skills Training on the Burnout of Nurses: A Cross-Sectional Study. Journal of clinical and diagnostic research : JCDR, 10(4), IC01–
IC04. doi:10.7860/JCDR/2016/19312.7667
54. Perlo, J., Feeley, D. Why Focusing on Professional Burnout is Not Enough. Journal of Healthcare Management: March-April 2018 - Volume 63 - Issue 2 - p 85-89. doi: 10.1097/JHM-D-18-00003. Accessed May 24, 2019
55. Choromanski, L. (2011). Nursing domain of CI governance: recommendations for health IT adoption and optimization.
CIN: Computers, Informatics, Nursing February 2011 Vol x issue 2 p 69 – 71.
56. Collins, S.A., et al. J Am Med Inform Assoc 2015;22:697–706. doi:10.1093/jamia/ocu001)
57. American Nursing Association. (2011). Nursing informatics: Scope and standards of practice. Silver Spring, MD:
American Nurses Association
58. KLAS Arch Collaborative. Accessed Dec 16, 2019 https://klasresearch.com/arch-collaborative.
59. Rosenbloom, S.T et al. Cognitive factors influencing perceptions of clinical documentation tools. Journal of Biomedical
Informatics Volume 40, Issue 2, April 2007, Pages 106-113
60. Cochran K., Freeman R., Moore E., ANA on the Frontline. Health IT for Nursing: What now? Accessed Nov 21, 2019
https://www.americannursetoday.com/healthit-nursing/.
61. Cochran K., Freeman R., Moore E., ANA on the Frontline: Nurses transforming the EHR. October
2018, Volume 13, Number 10
62. Phansalkar, S. et al. Drug—drug interactions that should be non-interruptive in order to reduce alert fatigue in
electronic health records. Journal of the American Medical Informatics Association, Volume 20, Issue 3, May 2013,
Pages 489–493
63. Reaction Data 2019. Accessed December 15 https://www.reactiondata.com/report/physician-
About Cerner
It’s our mission to relentlessly seek breakthrough
innovation that will shape health care of tomorrow. And
we believe that what we do doesn’t just impact health
care – it impacts the world. It’s why, more than ever,
health care is too important to stay the same.™
Contact us for more information • [email protected]
• cerner.com
2800 Rock Creek Pkwy. Kansas City, MO 64117
2326895071 _Clinician Burnout: Causes, Consequences and Strategies_v2/January2021
© Cerner Corporation. All rights reserved. ©Cerner Corporation. All rights reserved. All other trademarks referenced herein are
the property of their respective owners.