depth of anesthesia monitoring in cardiac surgery - oma.org · •ge healthcare (helsinki, finland)...
TRANSCRIPT
Depth of Anesthesia
Monitoring in Cardiac
Surgery
Adam Dryden MD, FRCPC
University of Ottawa Heart Institute
Depth of Anesthesia
Monitoring in Cardiac
Surgery
Because it’s not all about the heart.
“The anesthetist and surgeon could have before them on tape or screen a continuous record of the electric activity of both heart and brain.”
Disclosures
None

Objectives
• Review the general principles of monitoring
• Highlight the commercially available monitors
• Determine whether depth of anesthesia monitoring can
allow us to prevent awareness
• Evaluate whether titrating anesthesia to a processed
EEG value can promote positive outcomes
• Share our experience with processed EEG at the Ottawa
Heart Institute

GENERAL PRINCIPLES OF
MONITORING
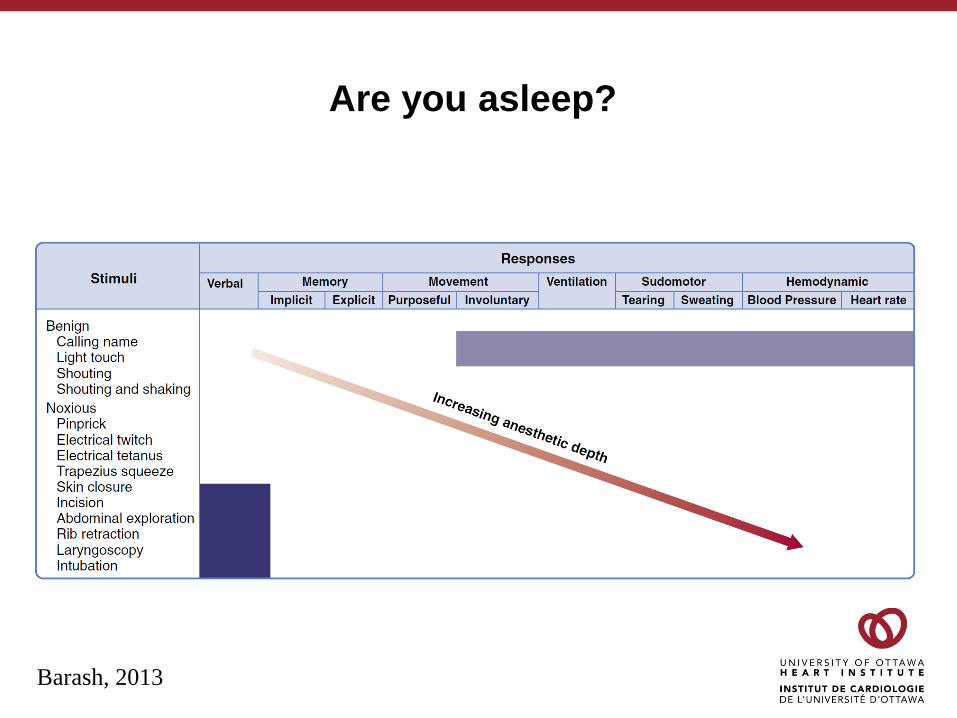
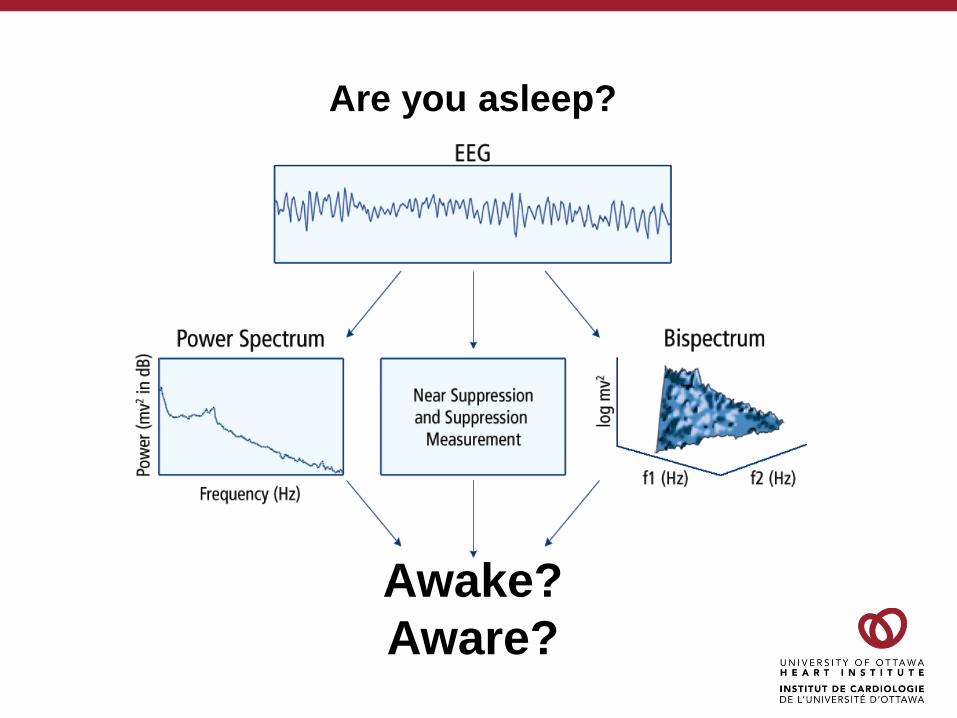
Are you asleep?
Barash, 2013

Are you asleep?
Purdon et al, 2015

General Principles of Monitoring
Awake?
Aware?
Are you asleep?
Awake?
Aware?
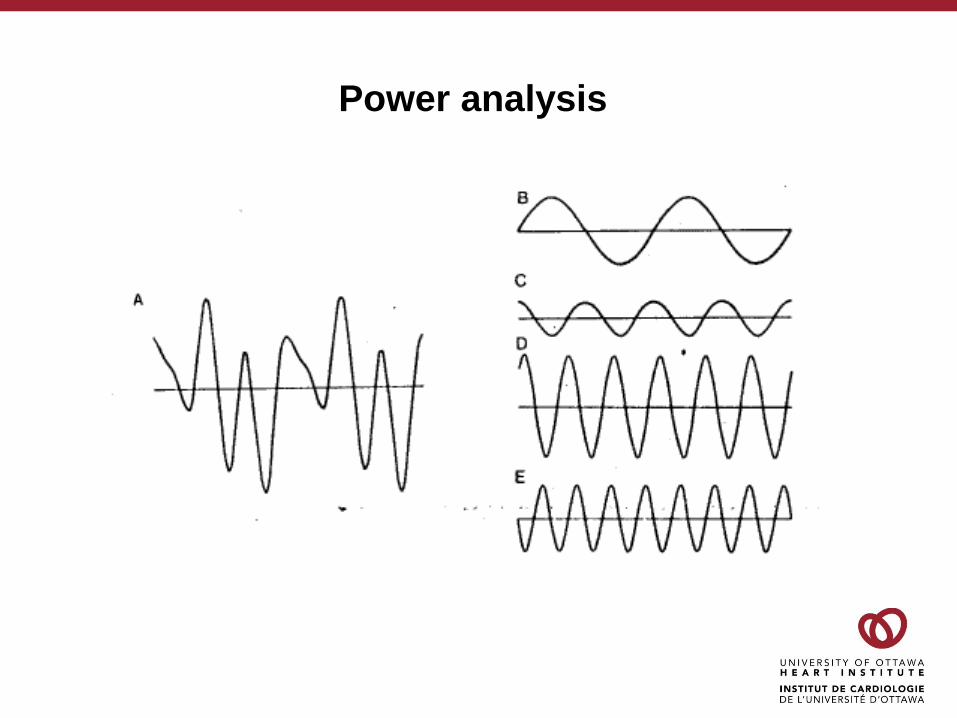
Power analysis

Power analysis
a b gqd
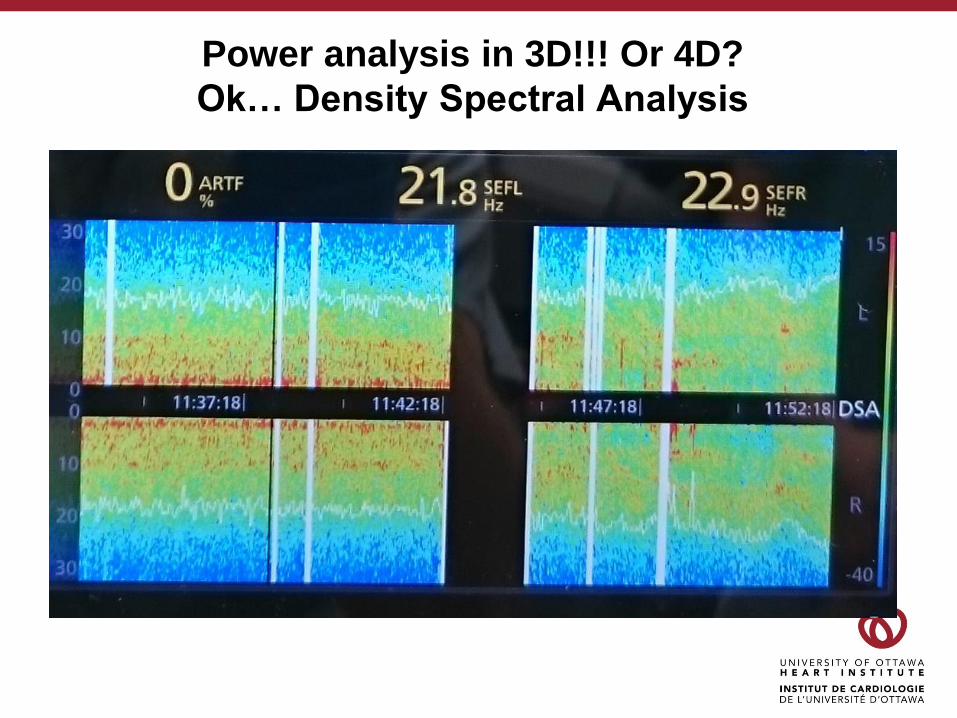
Power analysis in 3D!!! Or 4D?
Ok… Density Spectral Analysis
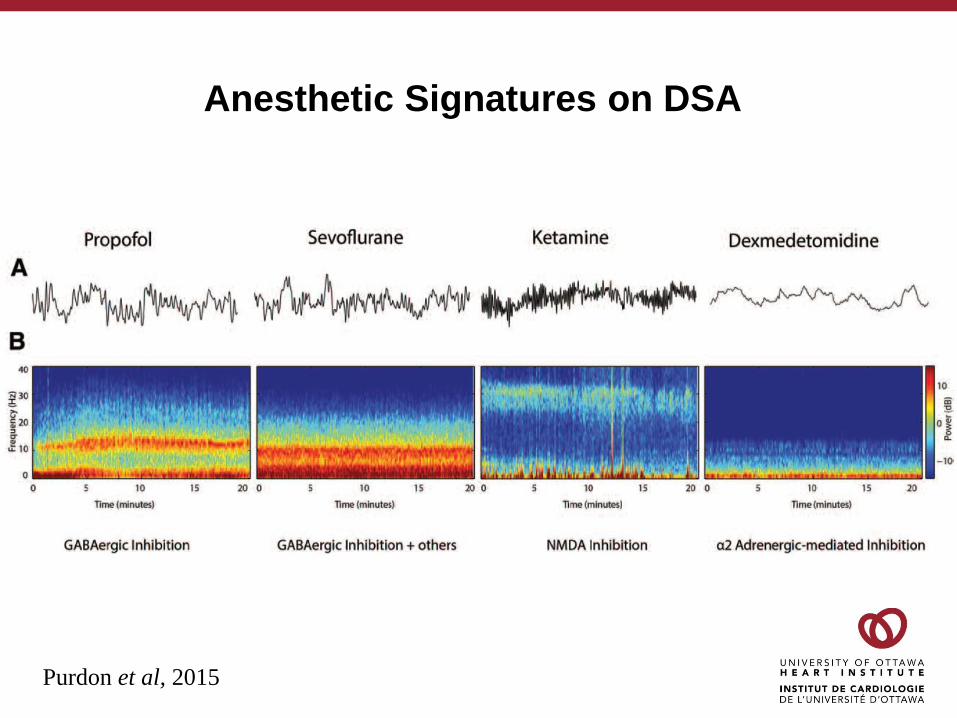
Anesthetic Signatures on DSA
Purdon et al, 2015

Limitations of (Processed) EEG
• Muscular activity
• Medical devices
• Pacemakers, electrocautery, surgical navigation systems, forced air
warmers
• Changes in cerebral metabolism
• Cardiac arrest, hypovolemia, hypotension, hypoglycemia,
hypothermia
• Seizures (or other abnormal EEG states)
• Medication limitations
• Ketamine, nitrous oxide, etomidate, ephedrine
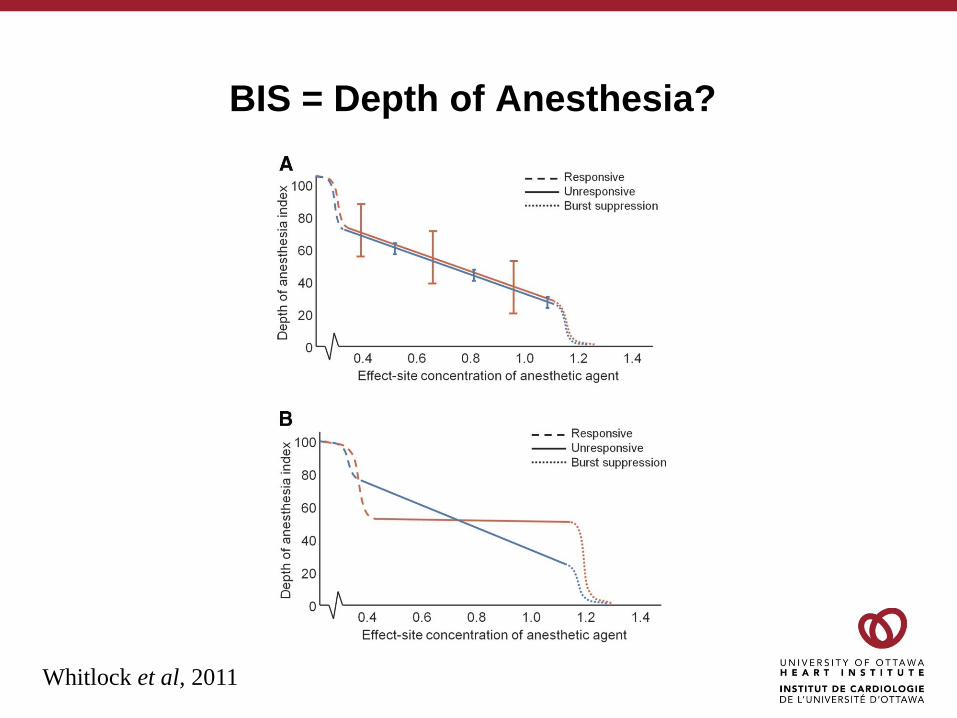
BIS = Depth of Anesthesia?
Whitlock et al, 2011
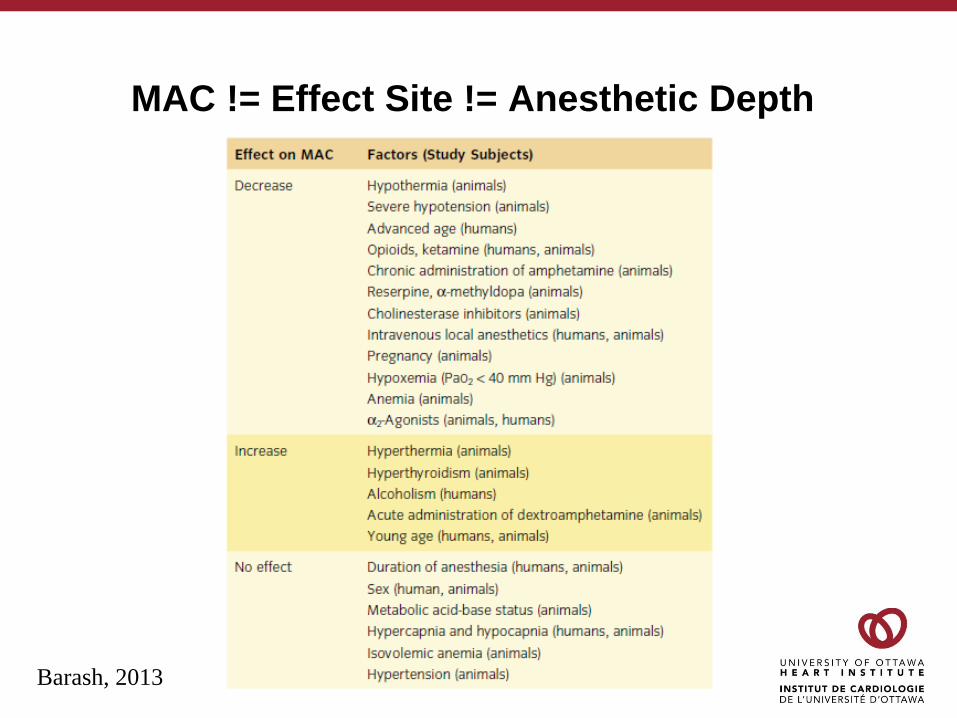
MAC != Effect Site != Anesthetic Depth
Barash, 2013

COMMERCIALLY AVAILABLE
MONITORS
Commercially Available Monitors
• Bispectal Index
• Covidien (Boulder, CO)
• Sedline
• Masimo (Irvine, CA)
• State Entropy
• GE Healthcare (Helsinki, Finland)
• Narcotrend
• Narcotrend-Gruppe (Hannover, Germany)
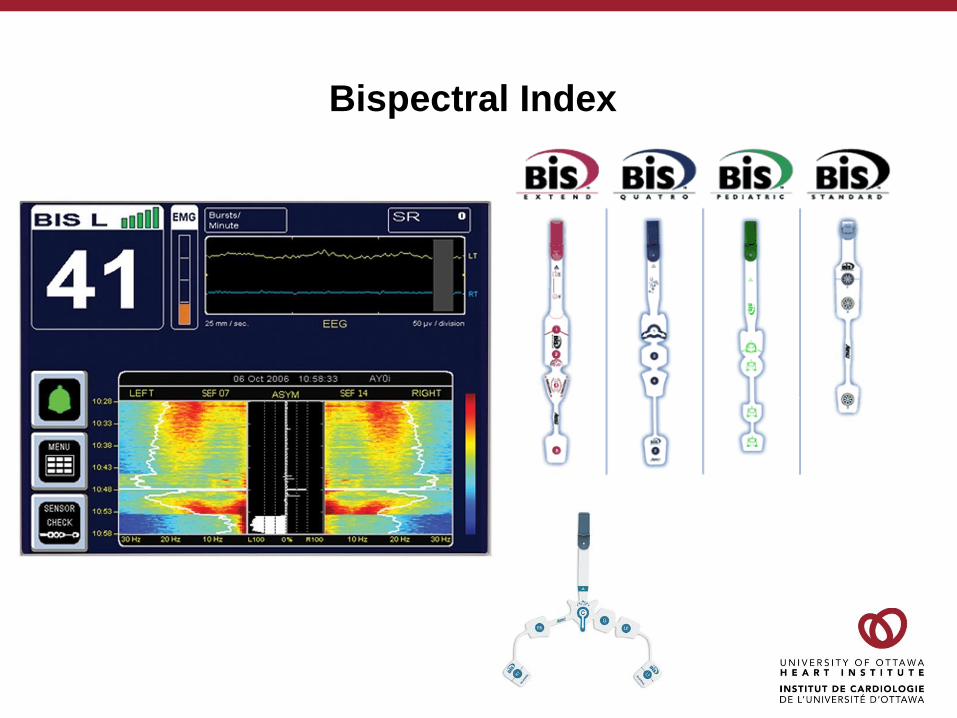
Bispectral Index

Sedline
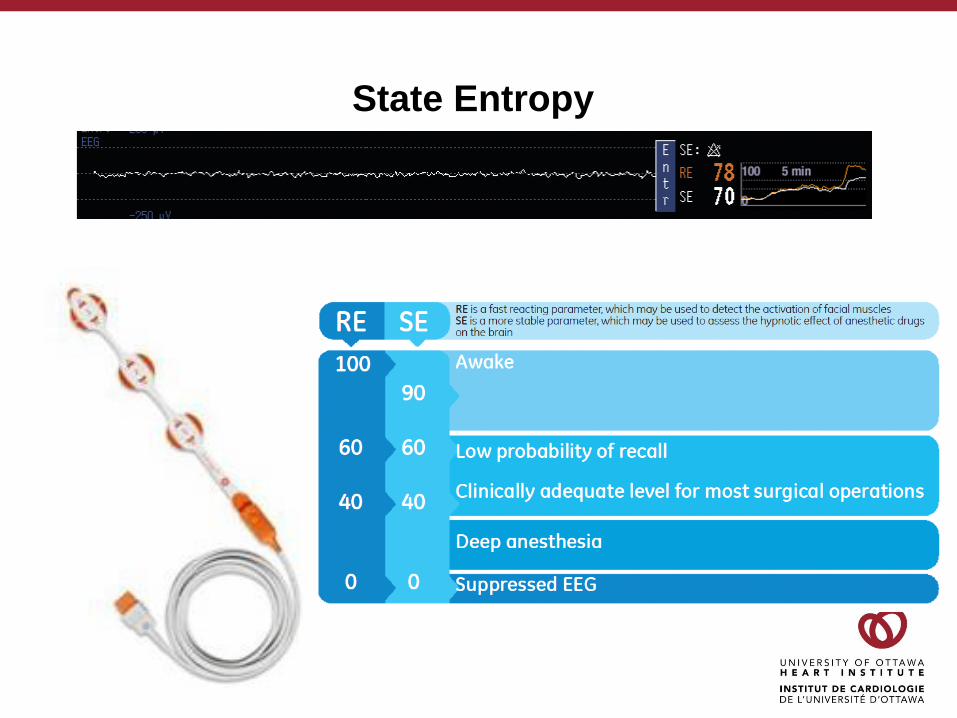
State Entropy

Narcotrend

PREVENTING AWARENESSFirst… Do No Harm.

Awareness
• Incidence is likely 1-2/1000
• Cardiac surgical procedures
• Obstetrical surgical procedures
• ASA III or IV
• Use of neuromuscular blocking agents
• ? Older
• ? Longer case
Sebel et al, 2004
Pollard et al, 2007

B – Aware
• Awareness: BIS 0.17% vs Routine 0.91%
• NNT of 138
• Anesthetic technique differences
•Less midazolam in the BIS group (2mg vs 2.5mg)
•Lower target plasma propofol concentration (2mg/L vs 2.4mg/L)
• No significant differences in nearly all post operative parameters and
complications
Myles et al, 2004
BAG - RECALL
• Goal was to determine whether BIS guided anesthetic management
was superior to end tidal anesthetic concentration (ETAC) for
awareness prevention
•Alarms used to guide therapy
• BIS was not superior to ETAC for preventing awareness
•BIS 0.24% compared to ETAC 0.07%
• No difference in median BIS
• No difference in median ETAC
Avidan et al, 2011
MACS
• Patients with no particular risk for awareness were included
• Very large (n=21,601) effectiveness study
• Planned for 30,000 patients – terminated for futility at interim endpoint
• Based on randomization, practitioners received alerts
• MAC < 0.5 (age adjusted)
• BIS > 60
Mashour et al, 2012

• Significant differences
when analyzed by intention
to treat vs post hoc
grouping
• Technical malfunction
MACS
Mashour et al, 2012
The Holy Grail of Cochrane
• Decreases the risk of awareness
in high risk patients
• But ETAC may be as effective
• No clinically relevant difference in
discharge readiness
• Less anesthetic use
• Especially consistent and relevant
for TIVA
• Impact of BIS on outcome was not
evaluated
Punjasawadwong et al, 2014
PROMOTING OUTCOMES
The Holy Grail of Cochrane, Round 2
• Non Cardiac Surgery
• Probably reduces risk of
postoperative delirium in first 7
days
• NNT – 17
• Moderate quality evidence
• No support for other outcomes
• All cause mortality
• Length of stay
Punjasawadwong et al, 2018

B – Aware
• Long term follow-up was done with included patients
•Median follow-up time of 4.1 years
• No difference in post-30 day death rates in the BIS
monitored compared to routine care
• Patients who had BIS < 40 for more than 5 minutes were
less likely to be alive at follow-up (HR=0.66, p=0.003)
Leslie et al, 2010
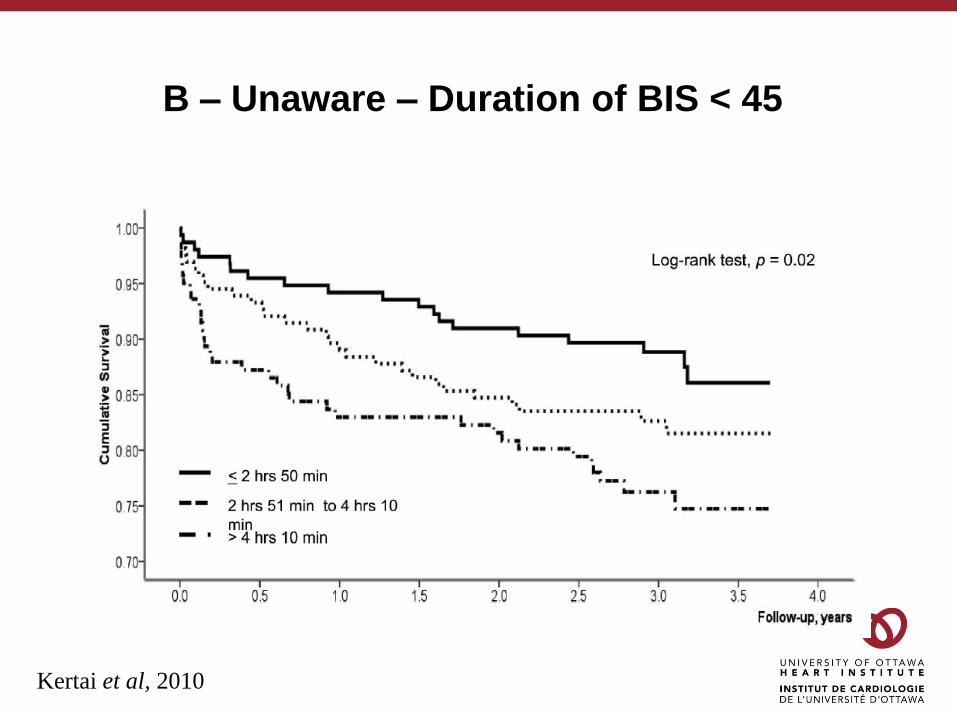
B – Unaware – Duration of BIS < 45
Kertai et al, 2010

Burst Suppression and Delirium
• A single centre prospective observational study
• 81 patients enrolled with identical anesthetic management
•Divided into delirious and non-delirous groups
• No difference in mean BIS values
• No other statistically significant risk factors identified
• Burst suppression duration was associated
• Burst suppression ratio was associated
Soehle et al, 2015
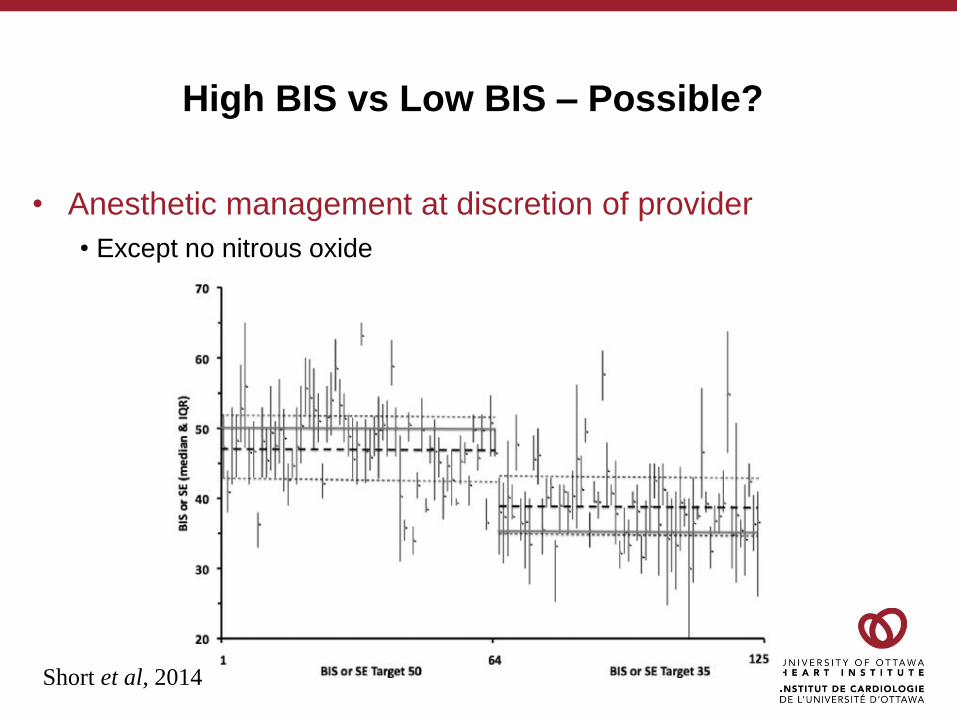
High BIS vs Low BIS – Possible?
• Anesthetic management at discretion of provider
• Except no nitrous oxide
Short et al, 2014

BIS AND THE OTTAWA HEART
INSTITUTE
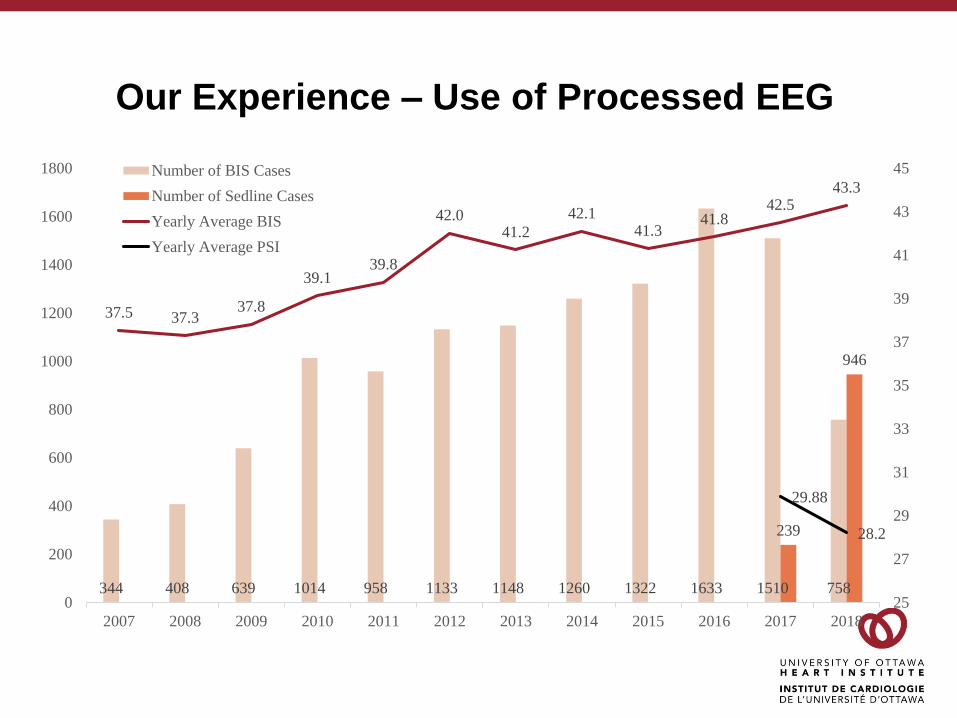
Our Experience – Use of Processed EEG
344 408 639 1014 958 1133 1148 1260 1322 1633 1510 758
239
946
37.5 37.337.8
39.139.8
42.041.2
42.141.3
41.842.5
43.3
29.88
28.2
0
200
400
600
800
1000
1200
1400
1600
1800
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
25
27
29
31
33
35
37
39
41
43
45Number of BIS Cases
Number of Sedline Cases
Yearly Average BIS
Yearly Average PSI
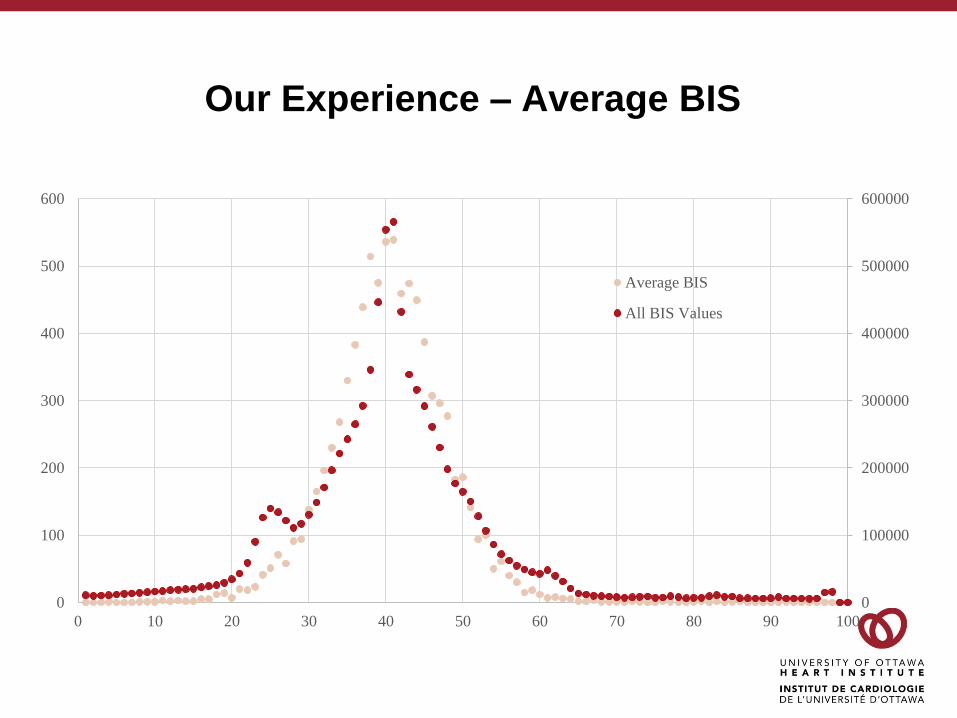
Our Experience – Average BIS
0
100000
200000
300000
400000
500000
600000
0
100
200
300
400
500
600
0 10 20 30 40 50 60 70 80 90 100
Average BIS
All BIS Values

Summary
• Depth of anesthesia is not a number
• The use of depth of anesthesia monitors, in high risk
patients, can prevent awareness
• Preventing excessive anesthetic depth is an area of very
active investigation
My Conclusions, Predictions and Bias
• The threshold value for “deep anesthesia” is suspect…
•Burst suppression/suppression ratio may prove to be useful signal
• Low numerical depth of anesthesia indicates frailty
• The expected low BIS in a critically ill patient
• The unexpected low BIS in a “well” appearing patient
• Excessive anesthetic depth is harmful
• Neurologic specific outcomes
• Outcomes related to vasoactive agent use
• Will be easier to demonstrate in vulnerable patients
• Sedation and anesthetic depth perioperatively is as, or
more important than intraoperatively

Questions
References1. Avidan MS, Jacobsohn E, Glick D, Burnside BA, Zhang L, Villafranca A, et al. Prevention of intraoperative awareness in a high-risk surgical population. N Engl J
Med. 2011;365(7):591-600.
2. Barash PG. Clinical anesthesia. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2013.
3. Kertai MD, Pal N, Palanca BJ, Lin N, Searleman SA, Zhang L, et al. Association of perioperative risk factors and cumulative duration of low bispectral index with
intermediate-term mortality after cardiac surgery in the B-Unaware Trial. Anesthesiology. 2010;112(5):1116-27.
4. Leslie K, Myles PS, Forbes A, Chan MT. The effect of bispectral index monitoring on long-term survival in the B-aware trial. Anesth Analg. 2010;110(3):816-22.
5. Mashour GA, Shanks A, Tremper KK, Kheterpal S, Turner CR, Ramachandran SK, et al. Prevention of intraoperative awareness with explicit recall in an
unselected surgical population: a randomized comparative effectiveness trial. Anesthesiology. 2012;117(4):717-25.
6. Maheshwari A, McCormick PJ, Sessler DI, et al. Prolonged concurrent hypotension and low bispectral index ('double low') are associated with mortality, serious
complications, and prolonged hospitalization after cardiac surgery. Br J Anaesth. 2017;119(1):40-49
7. Myles PS, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled
trial. Lancet. 2004;363(9423):1757-63.
8. Nitzschke R, Wilgusch J, Kersten JF, Trepte CJ, Haas SA, Reuter DA, et al. Bispectral index guided titration of sevoflurane in on-pump cardiac surgery reduces
plasma sevoflurane concentration and vasopressor requirements: a prospective, controlled, sequential two-arm clinical study. Eur J Anaesthesiol.
2014;31(9):482-90.
9. Pollard RJ, Coyle JP, Gilbert RL, Beck JE. Intraoperative awareness in a regional medical system: a review of 3 years' data. Anesthesiology. 2007;106(2):269-
74.
10. Punjasawadwong Y, Phongchiewboon A, Bunchungmongkol N. Bispectral index for improving anaesthetic delivery and postoperative recovery. Cochrane
Database Syst Rev. 2014;6:CD003843.
11. Punjasawadwong Y, Chau-In W, Laopaiboon M, Punjasawadwong S, Pin-On P. Processed electroencephalogram and evoked potential techniques for
amelioration of postoperative delirium and cognitive dysfunction following non-cardiac and non-neurosurgical procedures in adults. Cochrane Database Syst
Rev. 2018;5:CD011283.
12. Purdon PL, Sampson A, Pavone KJ, Brown EN. Clinical Electroencephalography for Anesthesiologists: Part I: Background and Basic Signatures.
Anesthesiology. 2015;123(4):937-60.
13. Sebel PS, Bowdle TA, Ghoneim MM, Rampil IJ, Padilla RE, Gan TJ, et al. The incidence of awareness during anesthesia: a multicenter United States study.
Anesth Analg. 2004;99(3):833-9.
14. Short TG, Leslie K, Campbell D, Chan MT, Corcoran T, O'Loughlin E, et al. A pilot study for a prospective, randomized, double-blind trial of the influence of
anesthetic depth on long-term outcome. Anesth Analg. 2014;118(5):981-6.
15. Sigl JC, Chamoun NG. An introduction to bispectral analysis for the electroencephalogram. J Clin Monit. 1994;10(6):392-404.
16. Soehle M, Dittmann A, Ellerkmann RK, Baumgarten G, Putensen C, Guenther U. Intraoperative burst suppression is associated with postoperative delirium
following cardiac surgery: a prospective, observational study. BMC Anesthesiol. 2015;15:61.
17. Whitlock EL, Torres BA, Lin N, Helsten DL, Nadelson MR, Mashour GA, et al. Postoperative delirium in a substudy of cardiothoracic surgical patients in the
BAG-RECALL clinical trial. Anesth Analg. 2014;118(4):809-17.
18. Whitlock EL, Villafranca AJ, Lin N, Palanca BJ, Jacobsohn E, Finkel KJ, et al. Relationship between bispectral index values and volatile anesthetic
concentrations during the maintenance phase of anesthesia in the B-Unaware trial. Anesthesiology. 2011;115(6):1209-18.
Selected References
Short TG, Leslie K, Campbell D, Chan MT, Corcoran T, O'Loughlin E, et al. A pilot study for a
prospective, randomized, double-blind trial of the influence of anesthetic depth on long-
term outcome. Anesth Analg. 2014;118(5):981-6.
Whitlock EL, Torres BA, Lin N, Helsten DL, Nadelson MR, Mashour GA, et al. Postoperative
delirium in a substudy of cardiothoracic surgical patients in the BAG-RECALL clinical trial.
Anesth Analg. 2014;118(4):809-17.
Kertai MD, Pal N, Palanca BJ, Lin N, Searleman SA, Zhang L, et al. Association of
perioperative risk factors and cumulative duration of low bispectral index with
intermediate-term mortality after cardiac surgery in the B-Unaware Trial. Anesthesiology.
2010;112(5):1116-27
Purdon PL, Sampson A, Pavone KJ, Brown EN. Clinical Electroencephalography for
Anesthesiologists: Part I: Background and Basic Signatures. Anesthesiology.
2015;123(4):937-60.