folyadékterápia: krisztalloid vagy kolloid? · 500 1000 250 v o 2 (m l / m i n) do2 (ml/min) ......
TRANSCRIPT

Folyadékterápia:krisztalloid vagy kolloid?
Molnár Zsolt Aneszteziológiai és Intenzív Terápiás Intézet
Szegedi Tudományegyetem

Élettan

DO2= (SV•P) • (Hb•1.39•SaO2+0.003•PaO2) ~ 1000ml/min
VO2 = CO • (CaO2 - CvO2) ~ 250 ml/min (ScvO2~70-75%)
Folyadék Vér Oxigén
Analgézia, szedáció
Az oxigén adósság

500 1000
250
VO
2 (m
l/min
)
DO2 (ml/min)
Sokk
Kompenzáló mechanizmusok
Kritikus pont

A folyadék fontos…

…életeket menthet,
Mortalitás: 46.5 vs. 30.5% (p=0.009)

…de árthat is: SOAPVincent JL, et al. Crit Care Med 2006; 34: 344–353

Annyit adjunk, amennyire szükség van!Bungaard-Nielsen M, et al. ACTA Anaesthesiol Scand 2009; 53: 843-51
Mit adjunk:
Krisztalloidot vagy Kolloidot?

Mortalitás:Lássuk az evidenciát!

SAFE
Finfer S et al. SAFE study. N Eng J Med 2004; 350: 2247
20.9% 21.1%
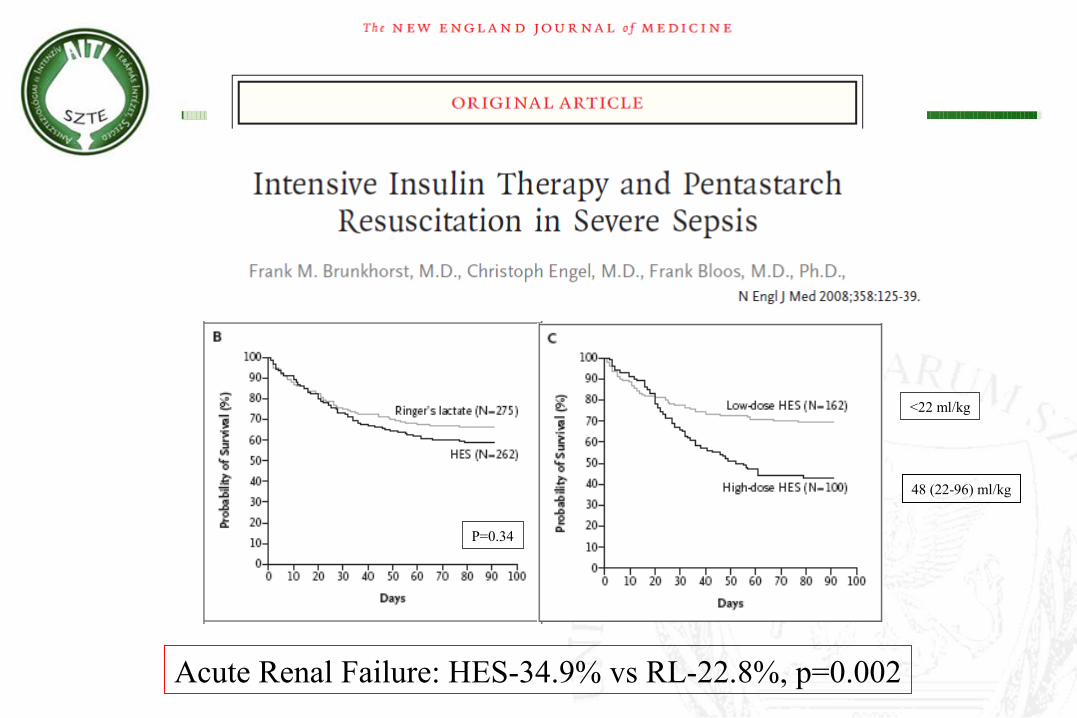
P=0.34
<22 ml/kg
48 (22-96) ml/kg
Acute Renal Failure: HES-34.9% vs RL-22.8%, p=0.002

• Patients with severe sepsis assigned to fluid resuscitation with HES 130/0.4 had an increased risk of death at day 90 and were more likely to require renal-replacement therapy, as compared with those receiving Ringer’s acetate.
• In patients in the ICU, there was no significant difference in 90-day mortality between patients resuscitated with 6% HES (130/0.4) or saline. However, more patients who received resuscitation with HES were treated with renal-replacement therapy.
HES is bad for you…
Molnár ‘99
Myburh JA et al. 2012; DOI: 10.1056/NEJMoa1209759
Perner A et al. 2012; DOI: 10.1056/NEJMoa1204242
„6S”
„CHEST”

„HES-ítélet” - 2012
Vége a szintetikuskolloid történetnek?
Dellinger RP et al. Intensive Care Med 39. doi: 10.1007/s00134-012-2769-8

Krisztalloidot vagy Kolloidot adjunk?

• Crystalloids:– Robert Lewins – 1832
• INJECTION OF SALINE SOLUTIONS IN EXTRAORDINARY QUANTITIES INTO THE VEINS IN CASES OF MALIGNANT CHOLERA
– Sydney Ringer – 1885
– Alexis Hartmann (1898-1964)
• Albumin– Pearl Harbor - 1941
Mérföldkövek
Molnár ‘99
A szemipermeabilis membránok
J Physiol May 5, 1896 19 (4) 312-326

TBW ~ 40L
Interstitial I.v.
I. c. E.c.
Coll
Cryst.
5%D1/82/85/8
1/43/4
1/1
Megoszlás – kompartment modell
V:R=1:1; 1:4Fact or fiction?

Hogyan működik az élettana klinikai gyakorlatban?

SAFE
Finfer S et al. SAFE study. N Eng J Med 2004; 350: 2247
Alb:1184 ml
Saline:1565 ml25%<
Folyadékterápia indokációja:
„The treating clinician judged that fluid resuscitation was required”

Perner A et al. 2012; DOI: 10.1056/NEJMoa1204242
„Trial fluid…was used when ICU clinician
judged [it] was needed”
HES:1500 ml
RA:1500 mlNS<

Myburh JA et al. 2012; DOI: 10.1056/NEJMoa1209759
20%< S
„Trial fluid was administered…as determined by the treating clinician
and supported by at least one objectivephysiological criterion”

Myburh JA et al. 2012; DOI: 10.1056/NEJMoa1209759
HR<90
MAP~75
CVP~9
Lac~2
• Közös vonások:• Indication of fluid-bolus was based on „intuition”
(reflects everyday practice)• Rather than invasive hemodynamic indeces
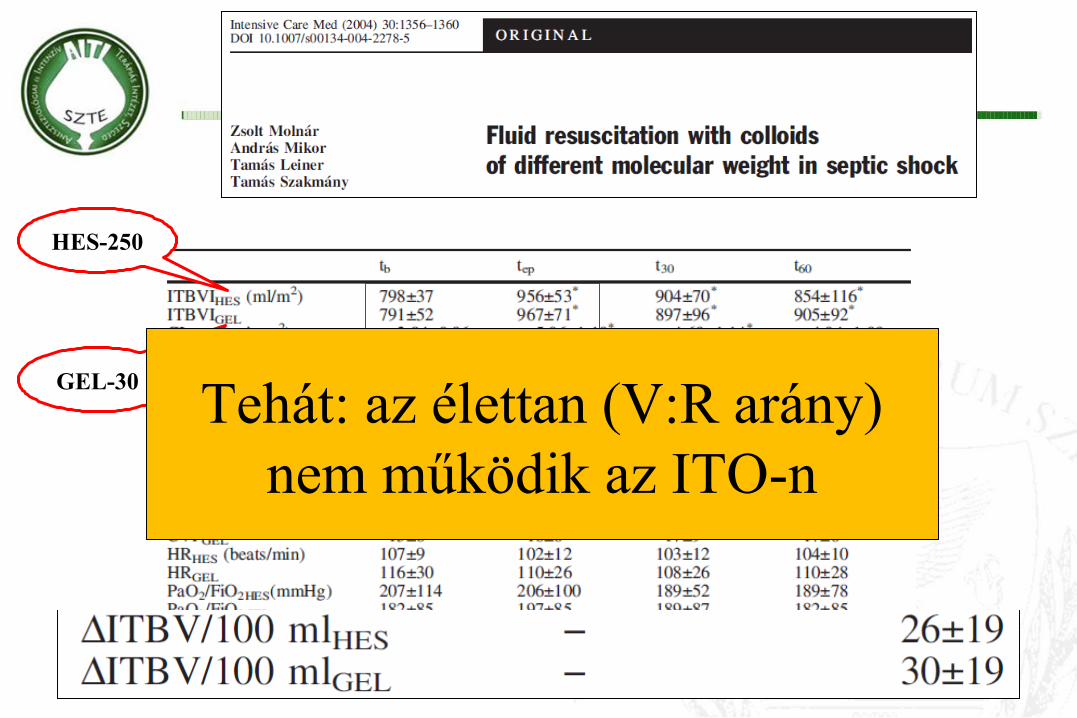
HES-250
GEL-30 Tehát: az élettan (V:R arány) nem működik az ITO-n

Mi a helyzet „egészségesekben”?

Acta Anaesthesiol Scand 2012; 56: 291–297
Decrease by 60%
Bleeding: 150 ± 33 ml/eventBlood:HES = 1:1

Crit Care Med. 2010 58(2):1-7
10 healthy adults1000 ml fluid/60 min
4x

Mit tanultunk eddig?
• „Működik” egészségesekben
• Mintha nem működne szeptikus betegekben1. Kolloid extravazáció?2. Valóban hypovolémiásak voltak ezek a betegek?
?
Válasz az első kérdésre:A titok nyitja a mikrocirkuláció
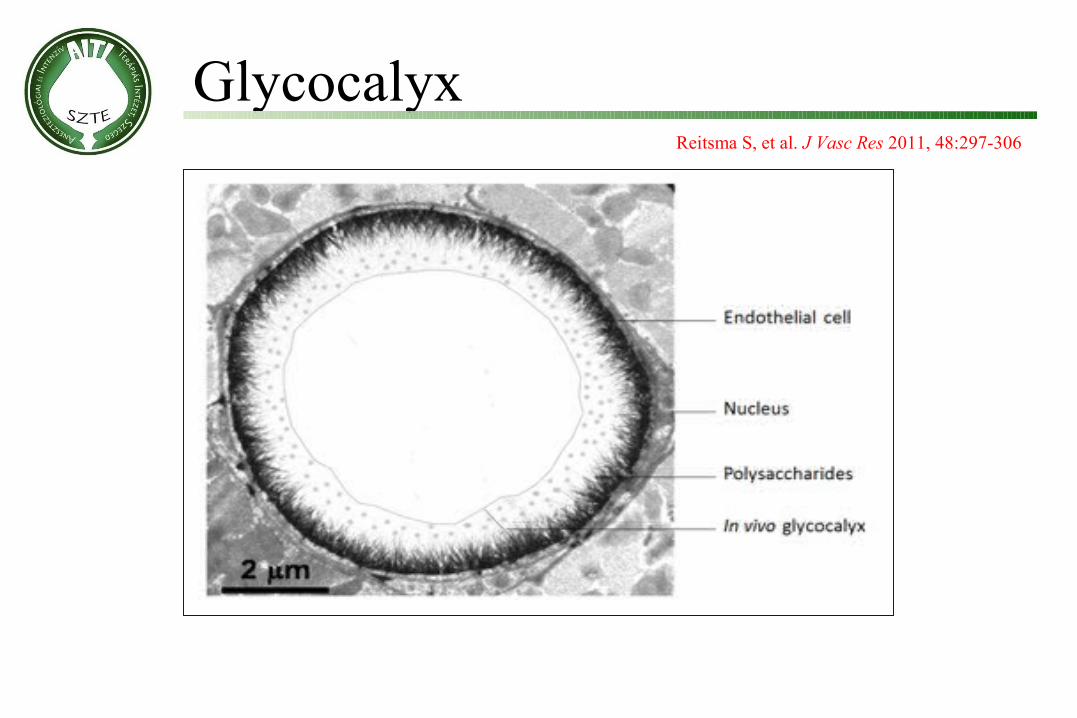
Reitsma S, et al. J Vasc Res 2011, 48:297-306
Glycocalyx

Bernard M. et al. Circulation Research. 2003; 92: 592-594
HypervolemiaBruegger D, et al. Am J Physiol Heart Cicr Physiol
2005; 289: H1993-1999
Severe sepsisChappel D, et al. Curr Opin Anaesthesiol
2009; 22: 155-62
SIRS
Glycocalyx

• Patients with severe sepsis assigned to fluid resuscitation with HES 130/0.4 had an increased risk of death at day 90 and were more likely to require renal-replacement therapy, as compared with those receiving Ringer’s acetate.
• In patients in the ICU, there was no significant difference in 90-day mortality between patients resuscitated with 6% HES (130/0.4) or saline. However, more patients who received resuscitation with HES were treated with renal-replacement therapy.
HES is bad for you?
Molnár ‘99
Myburh JA et al. 2012; DOI: 10.1056/NEJMoa1209759
Perner A et al. 2012; DOI: 10.1056/NEJMoa1204242
Igen:• Glycocalix sérült
• Extravazáció - toxicitás
Második kérdés:Valóban hypovolémiásak voltak ezek a
betegek?

Mi a fontosabb?
Mikor infundáljunk?Vagy:
Mit infundáljunk?

Invazív hemodinamikai monitorozás
• Otto Frank (1865-1944):• Élettanász (Lipcse)• Zur Dynamik des Herzmuskels, Z Biol 32
(1895) 370
• Ernest Starling (1866-1927):• UCL• Starling erők, hormonok, stb
Úttörők
Molnár ‘99

• Otto Frank, Ernest Starling – 1914: „Law of the heart”– „Within physiological limits, the force of contraction is directly
proportional to the initial length of the muscle fiber”
Molnár ‘99
The goal of resuscitationSV: CO-monitoring
EDV: ?
Hemodynamics
Starling EH. The Linacre Lecture on the Law of the Heart. London; 1918Starling EH. J R Army Med Corps. 1920; 34: 258-262
Stro
ke v
olum
e (m
l)End diastolic volume (ml)

.
normal heartnormal heart
failing heartfailing heart
preload responsiveness
preload unresponsiveness
Stroke volume
Ventricular preload
Statikus paraméterek (CVP, PAOP, GEDV) nem jelezhetik, a folyadék-válaszkészséget
„One size does not fit all!”
Courtesy of Prof. Jean-Loius Teboul

Molnár ‘99 PPmax PPmin
PPPPmaxmax - PP - PPminmin
(PP(PPmax max ++ PPPPminmin) /2) /2PPV =PPV =
(Courtesy of Jean-Louis Teboul)
IPPV = series of Valsalva-maneuvers
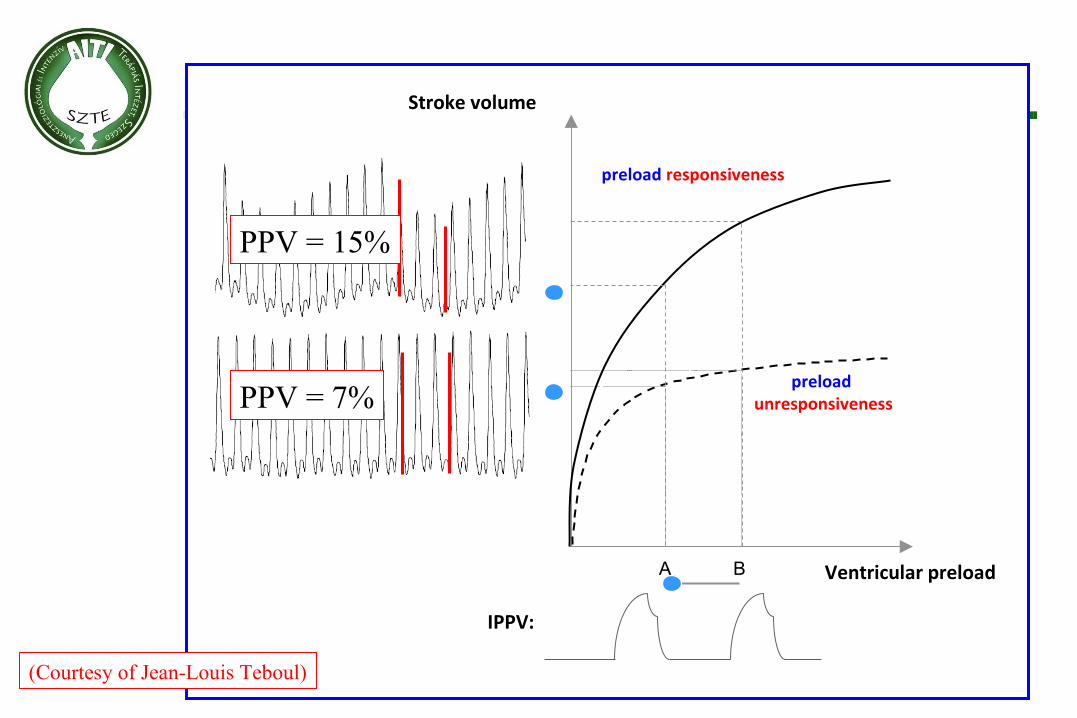
A B Ventricular preload
Stroke volume
preload responsiveness
preload unresponsiveness
(Courtesy of Jean-Louis Teboul)
IPPV:
PPV = 15%
PPV = 7%
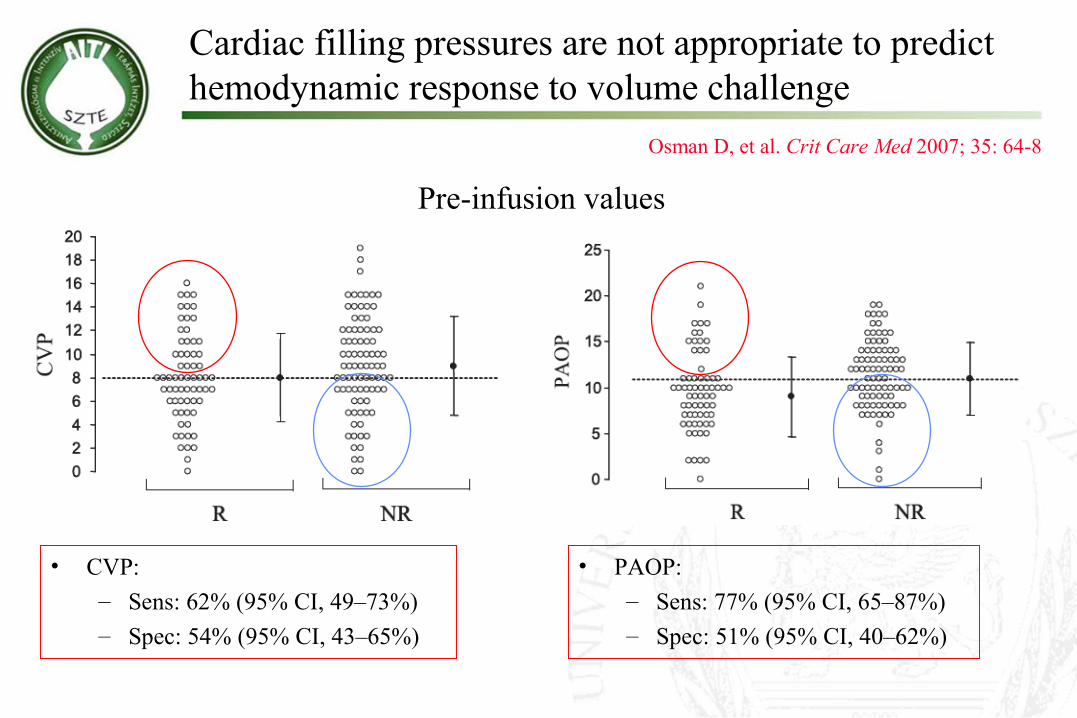
Osman D, et al. Crit Care Med 2007; 35: 64-8
Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge
• CVP:– Sens: 62% (95% CI, 49–73%)– Spec: 54% (95% CI, 43–65%)
Pre-infusion values
• PAOP:– Sens: 77% (95% CI, 65–87%)– Spec: 51% (95% CI, 40–62%)


Tánczos K, Németh M, Molnár ZAnn. Up. in Int. Care and Em. Med. 2014, pp. 355-65
Solve the hemodynamic puzzle first!2014
2014

Input: ScvO2, CVP, CI, GEDVI, SVV, MAP
Hypovolemic patients Normovolemic patients

Your wish…
Fluid therapy – in just 24 hours!
…won’t come true!

A legnagyobb tanulság...
Auguste Rodin: The Thinker

A hiba az élettanban van?
Nem, bennünk, aki nem-, vagy félre-értjük az adatainkat!

Come to Budapest – 18-20. September!
www.sepseast.euFREE registration for junior
doctors (age<29)!