oregon caregiver training · this report was written by the oregon caregiver training ......
TRANSCRIPT

OREGON CAREGIVER TRAINING
WORK GROUP REPORT

1
ACKNOWLEDGEMENTS
This report was written by the Oregon Caregiver Training Workgroup, a collaborative project of the Governor’s Commission on Senior Services and
the Oregon Disabilities Commission.
Thank you to the many stakeholders who provided input, analysis, content and hard work in creating this report. We specifically thank the Oregon Department of Human Services, Aging and People with Disabilities for
providing staff support.
Published June 2014

2
TABLE OF CONTENTS
Executive Summary
Key Recommendations
Introduction
Background and Process
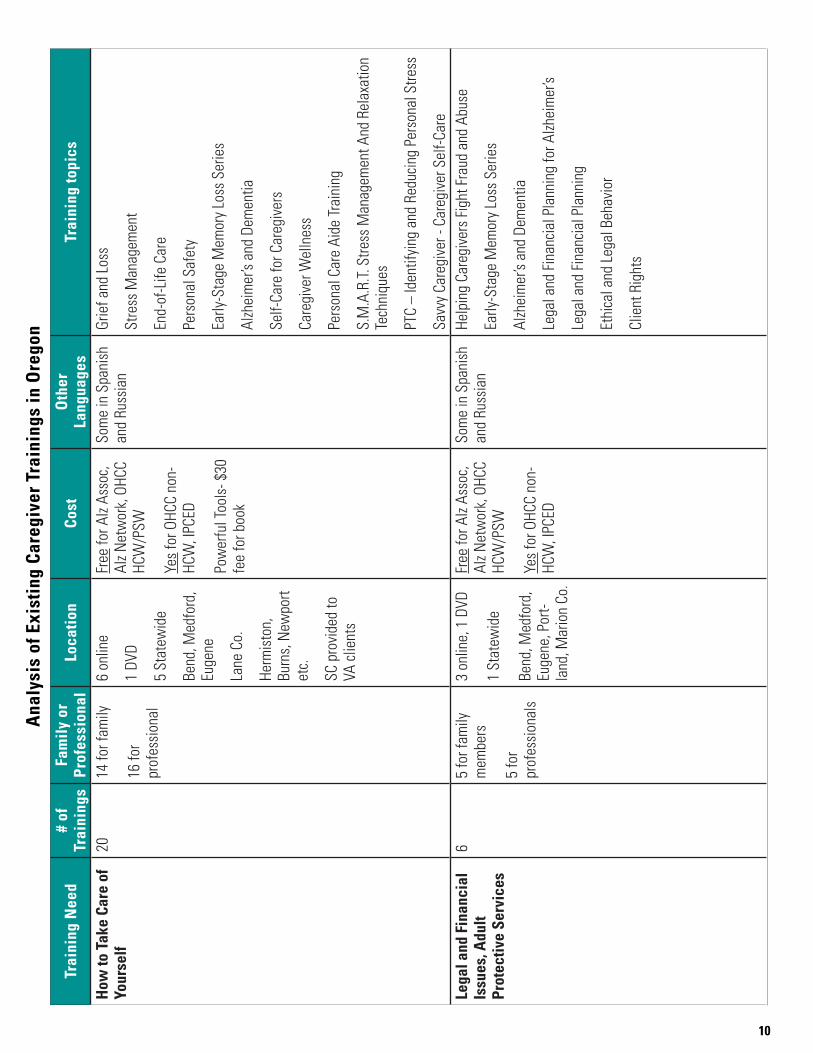
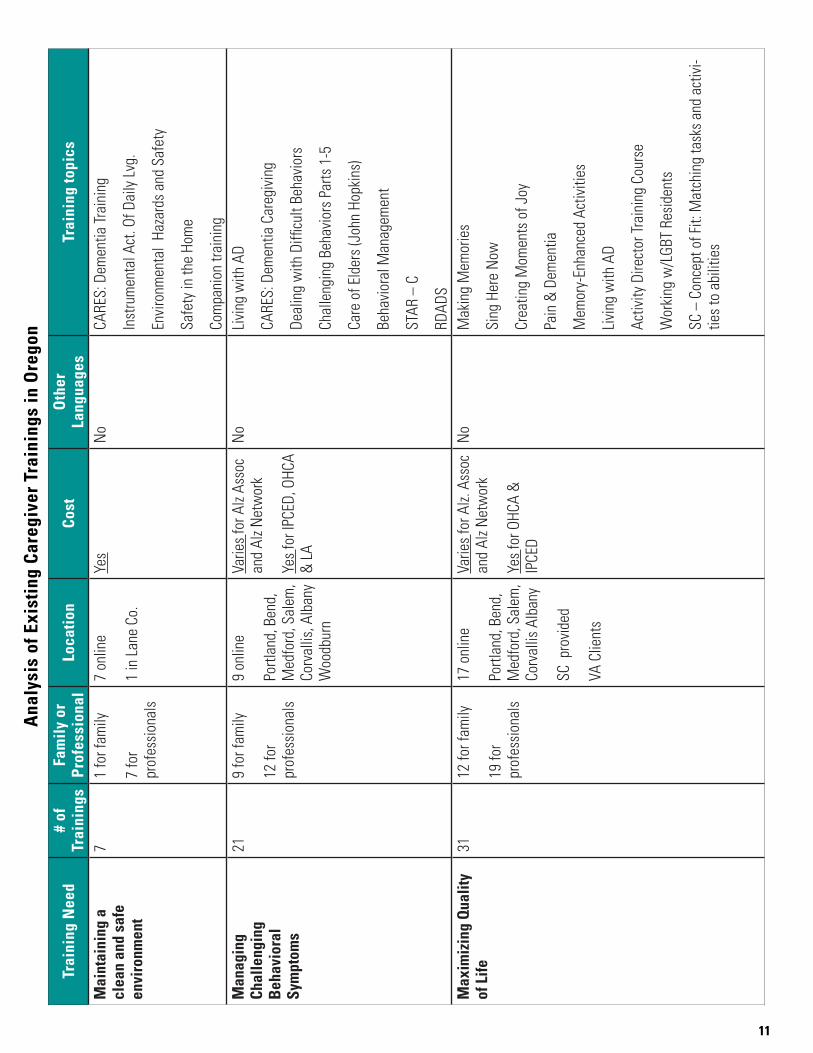
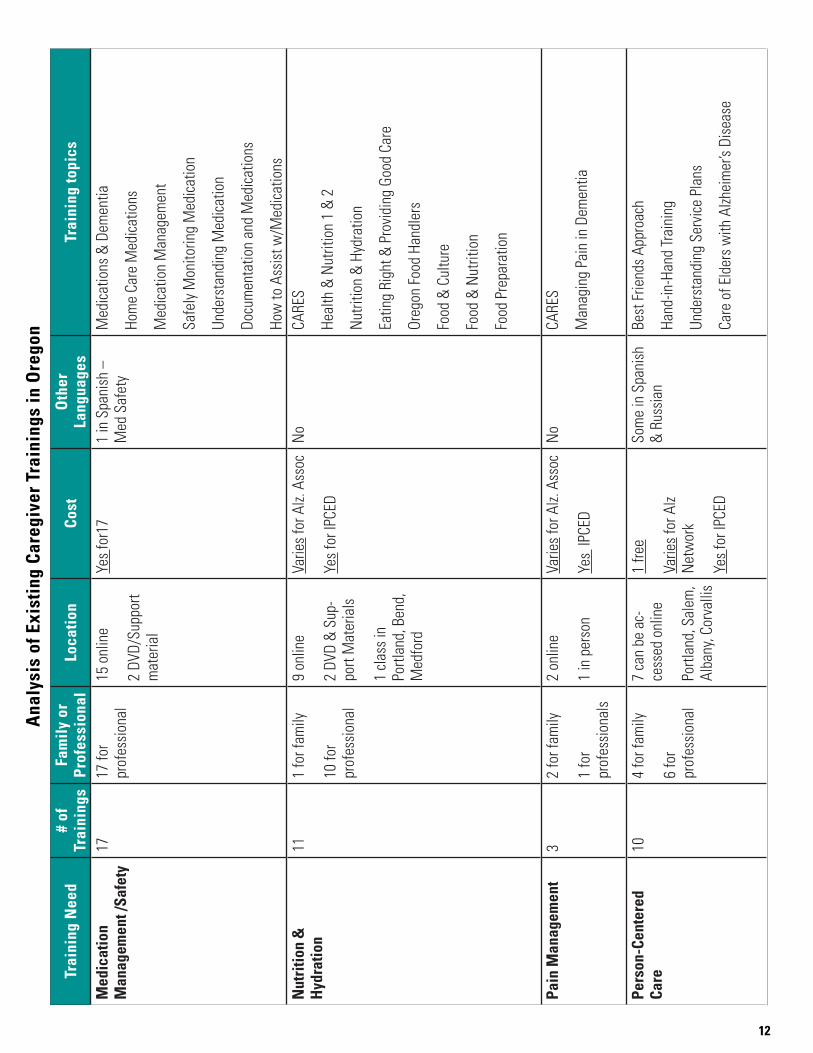
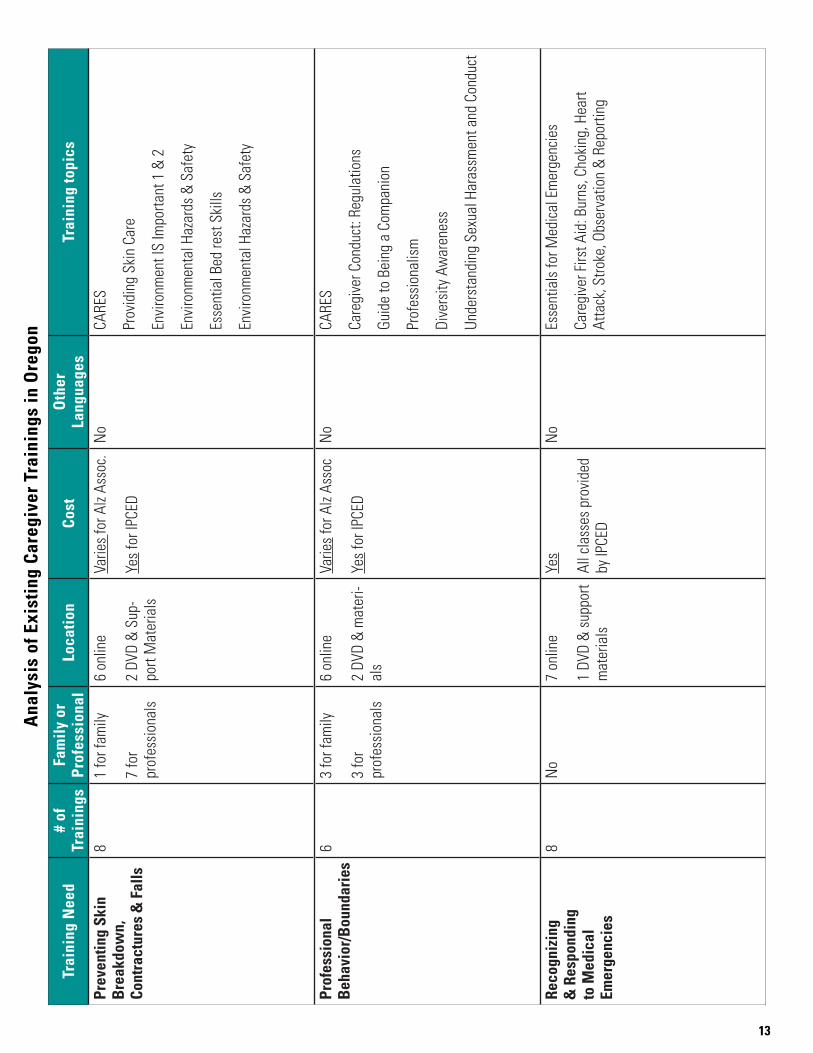
Analysis of Existing Caregiver Trainings in Oregon
Analysis
Recommendations
Appendix
3
4
5
6
7
15
19
22
3
OREGON CAREGIVER TRAINING WORK GROUP REPORT
Executive Summary
Oregon’s Health Care Transformation effort is focused on the “Triple Aim” of better care, better health, and lower costs. Caregiving is emerging as a risk factor for poor health and higher costs, and interventions exist to reduce the potential negative health impact on caregivers while improving the quality of care provided to the person or people for whom they are caring.
Many Oregonians require another person to provide daily care and help with activities a majority of us take for granted, such as eating, bathing, and getting dressed. The people receiving care may require it for a few months, a few years, or a lifetime, for many reasons (such as an injury, a physical disability, or a progressive disease). According to research by AARP, each year, over 460,000 unpaid caregivers in Oregon provide about $5.5 billion worth of care.1
The impact of caregiving on a caregiver is tremendous — physically, mentally, and financially. The most recent data from the Alzheimer’s Association shows that each year in Oregon, unpaid caregivers for people with dementia have $100 million in higher health care costs.2 Professional caregivers also face significant job stress in positions that are not well paid, leading to a high rate of job turnover, which is detrimental to the people receiving care.
Training can help improve care, reduce health care costs, improve the health of caregivers, and reduce turnover of professionals. Unfortunately, caregivers face barriers that prevent them from accessing beneficial education and training. The goal of this report is to make recommendations to ensure all caregivers in Oregon who can benefit from training are able to receive it. A valuable byproduct of the work group that wrote this report was the creation of a catalog of trainings that might be useful to many individuals, organizations, and agencies when looking for training — or when establishing public policy in regard to improving long-term care in Oregon.
1 http://assets.aarp.org/rgcenter/ppi/ltc/i51-caregiving.pdf2 http://www.alz.org/documents_custom/facts_2014/alz_ff_oregon.pdf
4
Key Recommendations
• Develop trainings to address unmet needs
o Businesses and nonprofits that provide trainings for caregivers should consider this list as a jumping-off point for the development of trainings that meet the unmet need..
o Government granting bodies, such as the Innovations Fund board, might want to use this list as a consideration for their grant process.
• Increase access to Oregon Home Care Commission trainings
o The Oregon Home Care Commission should begin a process to determine how to make its trainings more available to the general public while ensuring home-care and personal-support workers have full access to all required trainings.
• More aggressive promotion of existing trainings
o The ADRC should be promoted as the central place for Oregonians to find trainings. In addition, every training provider should be listed in the ADRC’s resource database.
o Hospitals, health systems, and medical professionals should be prepared to provide information about what training would be useful, as well as where to find it.
• Expand access to trainings statewide
o Increase the focus on developing Web-based trainings for those with Internet access.
o Respite programs need to be developed and expanded, including a revived Lifespan Respite Program.
o Investigate the use of public-access television and cable on-demand programming to air training videos.
• Ensure family caregivers are informed about caregiving and how to choose a useful training.
o Develop a simple brochure that lists what a caregiver might need help with and what to consider when looking for training.
This brochure should be made available in all medical offices, ADRCs, senior and community centers, libraries, and any other relevant locations, and it should be included in any packet of information medical providers give families following a diagnosis that may lead to someone serving as a family caregiver.
These recommendations are intended to be doable actions that will lead to a greater level of training of caregivers in Oregon. Some need to be implemented by nonprofits, some by government agencies, and some by businesses, and others might require legislative action. By following these recommendations, we assert that the quality of caregiving will improve in Oregon, caregivers’ lives will improve, and health care costs of caregivers will decline.

5
Introduction
Many Oregonians require another person to provide daily care that a majority of us take for granted. Caregivers help with many “instrumental activities of daily living” (IADLs), such as housework, managing money, and shopping. Additionally, caregivers help with “activities of daily living” (ADLs), such as bathing, eating, dressing, and toileting. The people receiving care may require it for a few months, a few years, or a lifetime, for many reasons (such as an injury, a physical disability, or a progressive disease). According to research by AARP, each year, over 460,000 unpaid caregivers in Oregon provide about $5.5 billion worth of care.3 The Alzheimer’s Association estimates that in Oregon unpaid care just for people with Alzheimer’s disease is valued at more than $2.4 billion per year.4
To provide the best care for people who require it, caregivers need education and training on best practices. This training might be about how to perform ADLs effectively, but it might also be on communication, legal issues, or maintaining a safe environment. Caregivers have many needs that training can meet, which will ultimately help care recipients live a better life.
Training can also directly benefit the caregiver. The impact of caregiving on a caregiver is tremendous — physically, mentally, and financially. The most recent data from the Alzheimer’s Association shows that each year in Oregon, unpaid caregivers for people with dementia have $100 million in higher health-care costs.5 Thus, training will help family caregivers live healthier and happier lives.
In regard to professional caregivers, training can lead to lower turnover rates and higher quality of care. Since 2011, entry-level home care aides in Washington State must complete 75 hours of basic-level training before they can be hired. Chesterfield Health Services, a home health-care provider in Seattle, invests heavily in training and advancement opportunities for its workforce. Stella Ogiale, Chesterfield’s founder and CEO, says it is important to train and empower workers to move up the health-career ladder to improve their professionalism if they choose to remain in home care. This investment has paid off, as demonstrated by high satisfaction rates for clients and home health-care providers, as well as low turnover rates.6
A 2011 study in Washington also pointed to the impact of career advancement and training on turnover among home-care workers. A survey of former home-care workers asked what they felt was most important to recruit new home-care workers. The results mirrored the results of a 20-year-old study that showed interventions to improve salary, benefits, hours, increased training, and support for retention in aggregate reduced turnover between 11 percent and 44 percent.7
The goal of this report is to make recommendations to ensure all caregivers in Oregon who can benefit from training are able to receive it. A valuable byproduct of the work group was the creation of a catalog of trainings that might be useful to many individuals, organizations, and agencies when looking for training — or when establishing public policy in regard to improving long-term care in Oregon.
3 http://assets.aarp.org/rgcenter/ppi/ltc/i51-caregiving.pdf4 http://www.alz.org/documents_custom/facts_2014/alz_ff_oregon.pdf5 Ibid6 http://phinational.org/consulting/resources/best-practices/chesterfield7 http://seiu775.org/files/2012/02/Why-They-Leave-Report1.pdf
6
Background
The Oregon Caregiver Training Work Group started at a retreat for the Governor’s Commission on Senior Services (GCSS) in the fall of 2012. The GCSS members recognized the need for caregiver training to improve the quality of care provided in the home and in long-term care settings, and they decided to start addressing this issue by gathering and analyzing data. At the time, the idea dovetailed closely with recommendations in the State Plan for Alzheimer’s Disease and Related Dementias in Oregon (SPADO), which was released in July 2012. SPADO was a broad coalition effort to determine how stakeholders in Oregon could help address the needs of individuals impacted by Alzheimer’s. The SPADO report identified caregiver training as an area for improvement.
The initial GCSS committee working on this idea recognized that caregiver training was not exclusive to aging or Alzheimer’s; the committee reached out to the Oregon Disabilities Commission (ODC) to create a jointly chaired work group on broad caregiver-training issues. The Oregon Caregiver Training Work Group was formed with Sherry Stock, executive director of the Oregon Brain Injury Alliance, representing ODC and Jon Bartholomew, public policy director of the Alzheimer’s Association Oregon Chapter, representing GCSS, and multiple stakeholders were invited to participate. The State Unit on Aging provided staff support for the work group. See Appendix A for a full list of individuals who served on the work group.
Oregon legislators passed Senate Bill 21 during the 2013 legislative session, which established a process by which the Oregon Department of Human Services (DHS) will convene stakeholders to discuss improvements to the long-term care system in Oregon. The Caregiver Training Work Group’s efforts are in sync with the goals of SB 21, and they will be relevant to the implementation of the law.
Process
During the work group’s initial meeting, the members determined the scope of the work needed to be done, as well as the process for doing it. We determined first that we would be focused on family caregivers and professionals who are not licensed. (A separate work group on dementia training for licensed professionals was created via the implementation of SPADO.) We also clarified that we would be looking at all caregiving in Oregon rather than caregiving for a particular condition or age range.
The work group determined our charge would be to:
• Determine what caregiver needs can be met by training
• Determine what trainings exist
• Determine where needs aren’t met by existing training
• Recommend solutions to close those gaps
The first step in achieving our goals was to brainstorm and categorize a set of caregivers’ needs. From that list, the work group members provided information about known trainings in Oregon to create a catalog. In this process, discussion arose regarding the difference between “training” and “education,” as the former can mean something formal and specific with a demonstration of proficiency. We decided to include anything that would be helpful in improving individuals’ caregiving skills, regardless of the level of formality.
A spreadsheet of caregiver trainings was created with input from work group members and others whom we reached out to. Erika Sessions from the Institute for Professional Care Education created a pivot table of this spreadsheet, which greatly assisted with the analysis of the data.
In January 2014, a work group subcommittee analyzed the data and brought the findings back to the larger work group to discuss recommendations. The subcommittee consisted of Jean Yamamoto from SEIU, Jan Karlen from DHS, and Suanne Jackson from the State Unit on Aging. The report was compiled by Jon Bartholomew, with editing assistance from his staff and work group members.

7
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
Act
iviti
es o
f Dai
ly
Livi
ng20
13 fo
r fam
ily
20 fo
r pr
ofes
sion
als
9 on
line
1 w
ebin
ar o
n de
man
d
5 DV
D
4 Sa
lem
, Co
rval
lis, A
lban
y
1 La
ne C
o.
5 st
atew
ide
4 Fr
ee
Varie
s fo
r Alz
Asso
c an
d OH
CA
Free
for O
HCC
HCW
/PSW
Yes
for O
HCC
non-
HCW
and
IPCE
D
Som
e Sp
anis
h an
d Ru
ssia
nDe
men
tia C
areg
ivin
g
Diffi
cult
Beha
vior
s
Carin
g fo
r the
Car
egiv
er
Pers
onal
Car
e Sk
ills
IADL
Bath
ing
and
Groo
min
g
Dura
ble
Med
ical
Equ
ipm
ent
End
of L
ife C
are
Bas
ic D
isea
se
Info
rmat
ion/
Pr
ogre
ssio
n
3121
for f
amily
30 fo
r pr
ofes
sion
als
20 o
nlin
e
5 DV
D
5 St
atew
ide
Portl
and,
Ben
d,
Med
ford
, Eu
gene
, Sal
em,
Corv
allis
, Alb
any
Free
9 w
ith A
lz As
soc,
Alz
Net
wor
k,
for O
HCC
HCW
/PS
W
Varie
s 4
for A
lz As
soc,
OHC
A
Yes
for O
HCC
non-
HCW
and
IPCE
D
Som
e Sp
anis
h an
d Ru
ssia
nLi
ving
with
, und
erst
andi
ng, c
arin
g fo
r, re
sear
ch
on A
lzhei
mer
’s, d
emen
tia
chro
nic
dise
ases
, hea
rt he
alth
y, di
abet
es
Com
mun
icab
le d
isea
ses
Deve
lopm
enta
l dis
abili
ties
care
HIV/
AIDS
Park
inso
n’s d
isea
se s
ympt
oms
Apha
sia
Blin
dnes
s an
d lo
w v
isio
nB
ehav
iors
as
Com
mun
icat
ion
117
for f
amily
9 fo
r pr
ofes
sion
als
6 on
line
1 DV
D
1 St
atew
ide
Mar
ion
Co.,
Corv
allis
SG -p
rovi
ded
to
VA fa
mili
es
Free
for A
lz N
etw
ork,
OHC
C HC
W/P
SW
Varie
s fo
r Alz.
Ass
oc
Yes
for O
HCC
non-
HCW
& IP
CED
Som
e Sp
anis
h an
d Ru
ssia
nDe
men
tia C
areg
ivin
g
Hand
ling
Diffi
cult
Situ
atio
ns, B
ehav
iors
Chal
leng
ing
Beha
vior
s
Savv
y Ca
regi
ver (
SG) –
Bas
ic C
omm
unic
atio
n Te
chni
ques
/ D
evel
opin
g st
rate
gies
for
com
mon
beh
avio
ral p
robl
ems
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n

8
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
Bod
y M
echa
nics
82
for f
amily
8 fo
r pr
ofes
sion
als
6 on
line
3 DV
D/Su
ppor
t m
ater
ial
1 La
ne C
o
1 St
atew
ide
Varie
s fo
r Alz
Asso
c
Free
for O
HCC
HCW
/PSW
Yes
for O
HCC
non-
HCW
, IPC
ED, a
nd
Lane
CC
Som
e in
Spa
nish
an
d Ru
ssia
nDe
men
tia C
areg
ivin
g
Prom
otin
g an
d M
aint
aini
ng G
ood
Mob
ility
Body
Mec
hani
cs a
nd B
ack
Safe
ty
Safe
Lift
ing
and
Tran
sfer
s
How
to h
elp
som
eone
who
use
s w
heel
chai
r, w
alke
r, ca
ne, c
rutc
hes
Esse
ntia
l Bed
rest
Ski
lls
Pers
onal
Car
e Ai
de Tr
aini
ng
Prot
ectin
g ag
ains
t spr
ains
and
stra
ins
Care
Tra
nsiti
ons
33
for f
amily
2 on
line
Yes
for I
PCED
Pow
erfu
l Too
ls: $
30
fee
for b
ook
No
Mak
ing
the
Mov
e-Tr
ansi
tions
to C
are
Jour
ney
from
Gui
lt to
Joy
Pow
erfu
l Too
ls (P
TC)–
Mas
terin
g Ca
regi
ving
De
cisi
ons
Com
mun
icat
ion
Skill
s28
13 fo
r fam
ily
26 fo
r pr
ofes
sion
als
17 o
nlin
e
5 st
atew
ide
Bend
, Med
ford
, Eu
gene
, Mar
ion
Co.,
Corv
allis
, La
ne C
o.
PT p
rovi
ded
in
man
y lo
catio
ns
stat
ewid
e
Free
for A
lz As
soc,
Al
z Net
wor
k, O
HCC
HCW
/PSW
Varie
s fo
r Alz.
As
soc,
OHC
A
Yes
for O
HCC
non-
HCW
, IPC
ED, L
ane
CC PTC,
$30
fee
for
book
Som
e in
Spa
nish
an
d Ru
ssia
nCh
alle
ngin
g Be
havi
ors
Livi
ng w
ith A
lzhei
mer
’s Se
ries
Dem
entia
Car
egiv
ing
Com
mun
icat
ion
Skill
s fo
r Car
egiv
ers
Carin
g fo
r the
Car
egiv
er
Ther
apeu
tic C
omm
unic
atio
n
Com
mun
icat
ing
with
peo
ple
who
hav
e Ap
hasi
a/De
men
tia/H
earin
g Lo
ss
Inte
rper
sona
l Com
mun
icat
ion
Confl
ict R
esol
utio
n
Wor
king
Toge
ther
Cust
omer
Ser
vice
Pow
erfu
l Too
ls (P
TC) –
Com
mun
icat
ing
Feel
ings
, Nee
ds a
nd C
once
rns/
Com
mun
icat
ing
in C
halle
ngin
g Si
tuat
ions
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n
9
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
Cultu
ral C
ompe
tenc
y4
4 fo
r pr
ofes
sion
als
3 on
line
1 St
atew
ide
Varie
s fo
r Tsa
i Co
mm
s
Yes
for I
PCED
Chin
ese
Unde
rsta
ndin
g Cu
ltura
l Diff
eren
ces
Food
and
Cul
ture
Deve
lopi
ng C
ultu
ral C
ompe
tenc
e
Cultu
ral C
ompe
tenc
y
Dive
rsity
Aw
aren
ess
Fire
Saf
ety
and
N
on-m
edic
al
Emer
genc
y
71
for f
amily
7 fo
r pr
ofes
sion
als
5 on
line
1 DV
D &
Sup
-po
rt M
ater
ials
1 St
atew
ide
1 La
ne C
o.
Free
for
OHC
C HC
W/P
SW
Yes
for I
PCED
, OHC
C no
n-HC
W, L
ane
CC
Som
e in
Sp
anis
h an
d Ru
ssia
n
Pers
onal
Saf
ety
Fire
Saf
ety
and
Emer
genc
ies
Resp
ondi
ng to
Wea
ther
Resp
ondi
ng to
Em
erge
ncie
s
Pers
onal
Car
e Ai
de Tr
aini
ngH
and
Was
hing
and
In
fect
ion
Cont
rol
51
for f
amily
5 fo
r pr
ofes
sion
als
3 on
line
1 DV
D
1 La
ne C
o.
1 St
atew
ide
Varie
s fo
r OHC
A
Free
for O
HCC
HCW
/PSW
Yes
for O
HCC
non-
HCW
, Lan
e CC
, IP
CED
Som
e in
Sp
anis
h an
d Ru
ssia
n
Infe
ctio
n Co
ntro
l and
Blo
od-B
orne
Pat
hoge
ns
Pers
onal
Car
e Ai
de Tr
aini
ng
Prev
entin
g Di
seas
e Tr
ansm
issi
on
How
to A
cces
s Re
sour
ces,
Dru
g-Fr
ee W
orkp
lace
107
for f
amily
8 fo
r pr
ofes
sion
al
6 on
line
1 DV
D &
sup
port
mat
eria
ls
1 St
atew
ide
Bend
, Med
ford
, Eu
gene
, Mar
ion
Co.
Free
for A
lz As
soc,
Al
z Net
wor
k, O
HCC
HCW
/PSW
Yes
for O
HCC
non-
HCW
, IPC
ED
Som
e in
Sp
anis
h an
d Ru
ssia
n
Subs
tanc
e Ab
use
Awar
enes
s
Getti
ng S
tarte
d w
ith A
lzhei
mer
’s
Early
-Sta
ge M
emor
y Lo
ss S
erie
s
Alzh
eim
er’s
and
Dem
entia
Livi
ng w
ith A
lzhei
mer
’s Se
ries
New
Hea
lth E
xcha
nge
and
How
it W
orks
Help
ing
Fam
ilies
Cop
e
Wor
king
with
Chi
ldre
n an
d Fa
mili
es
Deve
lopm
enta
l Dis
abili
ties:
Abi
lity
Awar
enes
s
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n
10
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
How
to T
ake
Care
of
Your
self
2014
for f
amily
16 fo
r pr
ofes
sion
al
6 on
line
1 DV
D
5 St
atew
ide
Bend
, Med
ford
, Eu
gene
Lane
Co.
Herm
isto
n,
Burn
s, N
ewpo
rt et
c.
SC p
rovi
ded
to
VA c
lient
s
Free
for A
lz As
soc,
Al
z Net
wor
k, O
HCC
HCW
/PSW
Yes
for O
HCC
non-
HCW
, IPC
ED
Pow
erfu
l Too
ls- $
30
fee
for b
ook
Som
e in
Spa
nish
an
d Ru
ssia
nGr
ief a
nd L
oss
Stre
ss M
anag
emen
t
End-
of-L
ife C
are
Pers
onal
Saf
ety
Early
-Sta
ge M
emor
y Lo
ss S
erie
s
Alzh
eim
er’s
and
Dem
entia
Self-
Care
for C
areg
iver
s
Care
give
r Wel
lnes
s
Pers
onal
Car
e Ai
de Tr
aini
ng
S.M
.A.R
.T. S
tress
Man
agem
ent A
nd R
elax
atio
n Te
chni
ques
PTC
– Id
entif
ying
and
Red
ucin
g Pe
rson
al S
tress
Savv
y Ca
regi
ver -
Car
egiv
er S
elf-C
are
Lega
l and
Fin
anci
al
Issu
es, A
dult
Prot
ectiv
e Se
rvic
es
65
for f
amily
m
embe
rs
5 fo
r pr
ofes
sion
als
3 on
line,
1 D
VD
1 St
atew
ide
Bend
, Med
ford
, Eu
gene
, Por
t-la
nd, M
ario
n Co
.
Free
for A
lz As
soc,
Al
z Net
wor
k, O
HCC
HCW
/PSW
Yes
for O
HCC
non-
HCW
, IPC
ED
Som
e in
Spa
nish
an
d Ru
ssia
nHe
lpin
g Ca
regi
vers
Fig
ht F
raud
and
Abu
se
Early
-Sta
ge M
emor
y Lo
ss S
erie
s
Alzh
eim
er’s
and
Dem
entia
Lega
l and
Fin
anci
al P
lann
ing
for A
lzhei
mer
’s
Lega
l and
Fin
anci
al P
lann
ing
Ethi
cal a
nd L
egal
Beh
avio
r
Clie
nt R
ight
s
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n
11
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
Mai
ntai
ning
a
clea
n an
d sa
fe
envi
ronm
ent
71
for f
amily
7 fo
r pr
ofes
sion
als
7 on
line
1 in
Lan
e Co
.
Yes
No
CARE
S: D
emen
tia Tr
aini
ng
Inst
rum
enta
l Act
. Of D
aily
Lvg
.
Envi
ronm
enta
l Ha
zard
s an
d Sa
fety
Safe
ty in
the
Hom
e
Com
pani
on tr
aini
ngM
anag
ing
Chal
leng
ing
Beh
avio
ral
Sym
ptom
s
219
for f
amily
12 fo
r pr
ofes
sion
als
9 on
line
Portl
and,
Ben
d,
Med
ford
, Sal
em,
Corv
allis
, Alb
any
Woo
dbur
n
Varie
s fo
r Alz
Asso
c an
d Al
z Net
wor
k
Yes
for I
PCED
, OHC
A &
LA
No
Livi
ng w
ith A
D
CARE
S: D
emen
tia C
areg
ivin
g
Deal
ing
with
Diffi
cult
Beha
vior
s
Chal
leng
ing
Beha
vior
s Pa
rts 1
-5
Care
of E
lder
s (J
ohn
Hopk
ins)
Beha
vior
al M
anag
emen
t
STAR
– C
RDAD
SM
axim
izin
g Q
ualit
y of
Life
3112
for f
amily
19 fo
r pr
ofes
sion
als
17 o
nlin
e
Portl
and,
Ben
d,
Med
ford
, Sal
em,
Corv
allis
Alb
any
SC p
rovi
ded
VA C
lient
s
Varie
s fo
r Alz.
Ass
oc
and
Alz N
etw
ork
Yes
for O
HCA
&
IPCE
D
No
Mak
ing
Mem
orie
s
Sing
Her
e N
ow
Crea
ting
Mom
ents
of J
oy
Pain
& D
emen
tia
Mem
ory-
Enha
nced
Act
iviti
es
Livi
ng w
ith A
D
Activ
ity D
irect
or Tr
aini
ng C
ours
e
Wor
king
w/L
GBT
Resi
dent
s
SC –
Con
cept
of F
it: M
atch
ing
task
s an
d ac
tivi-
ties
to a
bilit
ies
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n
12
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
Med
icat
ion
M
anag
emen
t /Sa
fety
1717
for
prof
essi
onal
15
onl
ine
2 DV
D/Su
ppor
t m
ater
ial
Yes
for1
71
in S
pani
sh –
M
ed S
afet
y M
edic
atio
ns &
Dem
entia
Hom
e Ca
re M
edic
atio
ns
Med
icat
ion
Man
agem
ent
Safe
ly M
onito
ring
Med
icat
ion
Unde
rsta
ndin
g M
edic
atio
n
Docu
men
tatio
n an
d M
edic
atio
ns
How
to A
ssis
t w/M
edic
atio
nsN
utri
tion
&
Hyd
ratio
n 11
1 fo
r fam
ily
10 fo
r pr
ofes
sion
al
9 on
line
2 DV
D &
Sup
-po
rt M
ater
ials
1 cl
ass
in
Portl
and,
Ben
d,
Med
ford
Varie
s fo
r Alz.
Ass
oc
Yes
for I
PCED
No
CARE
S
Heal
th &
Nut
ritio
n 1
& 2
Nut
ritio
n &
Hyd
ratio
n
Eatin
g Ri
ght &
Pro
vidi
ng G
ood
Care
Oreg
on F
ood
Hand
lers
Food
& C
ultu
re
Food
& N
utrit
ion
Food
Pre
para
tion
Pain
Man
agem
ent
32
for f
amily
1 fo
r pr
ofes
sion
als
2 on
line
1 in
per
son
Varie
s fo
r Alz.
Ass
oc
Yes
IPCE
D
No
CARE
S
Man
agin
g Pa
in in
Dem
entia
Pers
on-C
ente
red
Care
104
for f
amily
6 fo
r pr
ofes
sion
al
7 ca
n be
ac-
cess
ed o
nlin
e
Portl
and,
Sal
em,
Alba
ny, C
orva
llis
1 fre
e
Varie
s fo
r Alz
Net
wor
k
Yes
for I
PCED
Som
e in
Spa
nish
&
Rus
sian
Best
Frie
nds
Appr
oach
Hand
-in-H
and
Trai
ning
Unde
rsta
ndin
g Se
rvic
e Pl
ans
Care
of E
lder
s w
ith A
lzhei
mer
’s Di
seas
e
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n
13
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
Prev
entin
g Sk
in
Bre
akdo
wn,
Co
ntra
ctur
es &
Fal
ls
81
for f
amily
7 fo
r pr
ofes
sion
als
6 on
line
2 DV
D &
Sup
-po
rt M
ater
ials
Varie
s fo
r Alz
Asso
c.
Yes
for I
PCED
No
CARE
S
Prov
idin
g Sk
in C
are
Envi
ronm
ent I
S Im
porta
nt 1
& 2
Envi
ronm
enta
l Haz
ards
& S
afet
y
Esse
ntia
l Bed
rest
Ski
lls
Envi
ronm
enta
l Haz
ards
& S
afet
y
Prof
essi
onal
B
ehav
ior/B
ound
arie
s6
3 fo
r fam
ily
3 fo
r pr
ofes
sion
als
6 on
line
2 DV
D &
mat
eri-
als
Varie
s fo
r Alz
Asso
c
Yes
for I
PCED
No
CARE
S
Care
give
r Con
duct
: Reg
ulat
ions
Guid
e to
Bei
ng a
Com
pani
on
Prof
essi
onal
ism
Dive
rsity
Aw
aren
ess
Unde
rsta
ndin
g Se
xual
Har
assm
ent a
nd C
ondu
ct
Reco
gniz
ing
& R
espo
ndin
g to
Med
ical
Em
erge
ncie
s
8N
o7
onlin
e
1 DV
D &
sup
port
mat
eria
ls
Yes
All c
lass
es p
rovi
ded
by IP
CED
No
Esse
ntia
ls fo
r Med
ical
Em
erge
ncie
s
Care
give
r Firs
t Aid
: Bur
ns, C
hoki
ng, H
eart
Atta
ck, S
troke
, Obs
erva
tion
& R
epor
ting
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n
14
Trai
ning
Nee
d#
of
Trai
ning
sFa
mily
or
Prof
essi
onal
Loca
tion
Cost
Oth
er
Lang
uage
s Tr
aini
ng to
pics
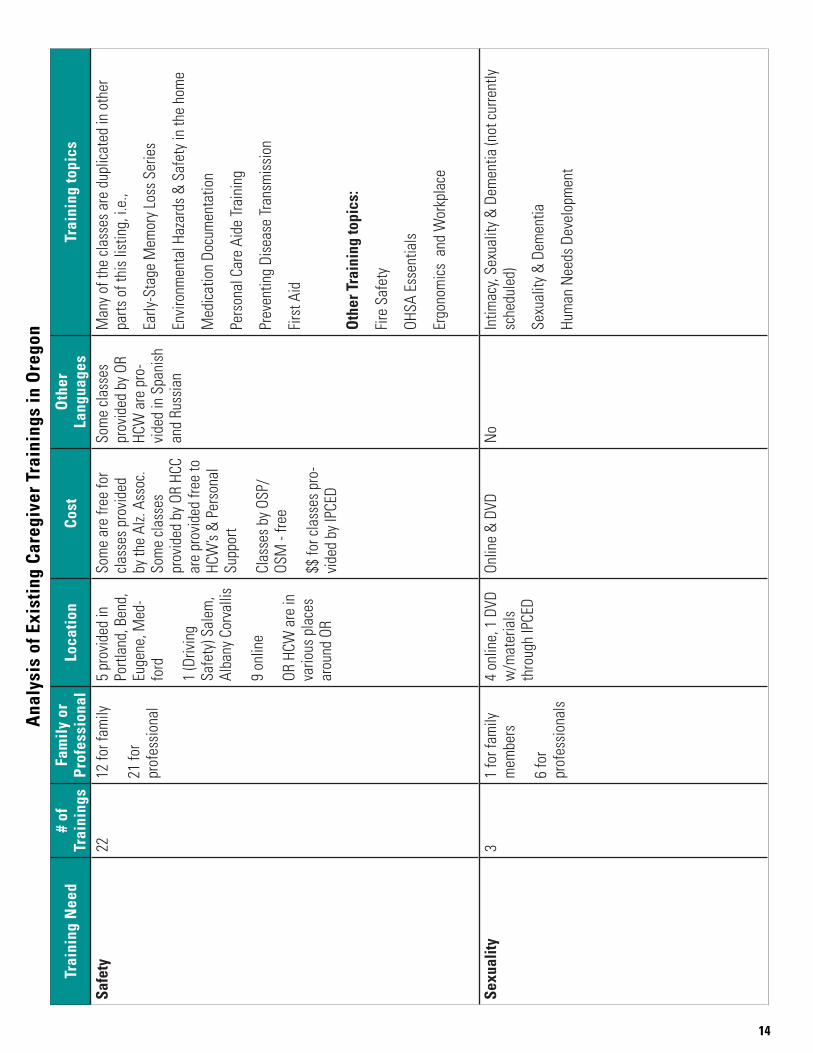
Safe
ty22
12 fo
r fam
ily
21 fo
r pr
ofes
sion
al
5 pr
ovid
ed in
Po
rtlan
d, B
end,
Eu
gene
, Med
-fo
rd
1 (D
rivin
g Sa
fety
) Sal
em,
Alba
ny C
orva
llis
9 on
line
OR H
CW a
re in
va
rious
pla
ces
arou
nd O
R
Som
e ar
e fre
e fo
r cl
asse
s pr
ovid
ed
by th
e Al
z. As
soc.
So
me
clas
ses
prov
ided
by
OR H
CC
are
prov
ided
free
to
HCW
’s &
Per
sona
l Su
ppor
t
Clas
ses
by O
SP/
OSM
- fre
e
$$ fo
r cla
sses
pro
-vi
ded
by IP
CED
Som
e cl
asse
s pr
ovid
ed b
y OR
HC
W a
re p
ro-
vide
d in
Spa
nish
an
d Ru
ssia
n
Man
y of
the
clas
ses
are
dupl
icat
ed in
oth
er
parts
of t
his
listin
g, i.
e.,
Early
-Sta
ge M
emor
y Lo
ss S
erie
s
Envi
ronm
enta
l Haz
ards
& S
afet
y in
the
hom
e
Med
icat
ion
Docu
men
tatio
n
Pers
onal
Car
e Ai
de Tr
aini
ng
Prev
entin
g Di
seas
e Tr
ansm
issi
on
Firs
t Aid
Oth
er T
rain
ing
topi
cs:
Fire
Saf
ety
OHSA
Ess
entia
ls
Ergo
nom
ics
and
Wor
kpla
ce
Sexu
ality
31
for f
amily
m
embe
rs
6 fo
r pr
ofes
sion
als
4 on
line,
1 D
VD
w/m
ater
ials
th
roug
h IP
CED
Onlin
e &
DVD
No
Intim
acy,
Sexu
ality
& D
emen
tia (n
ot c
urre
ntly
sc
hedu
led)
Sexu
ality
& D
emen
tia
Hum
an N
eeds
Dev
elop
men
t
Ana
lysi
s of
Exi
stin
g Ca
regi
ver T
rain
ings
in O
rego
n
15
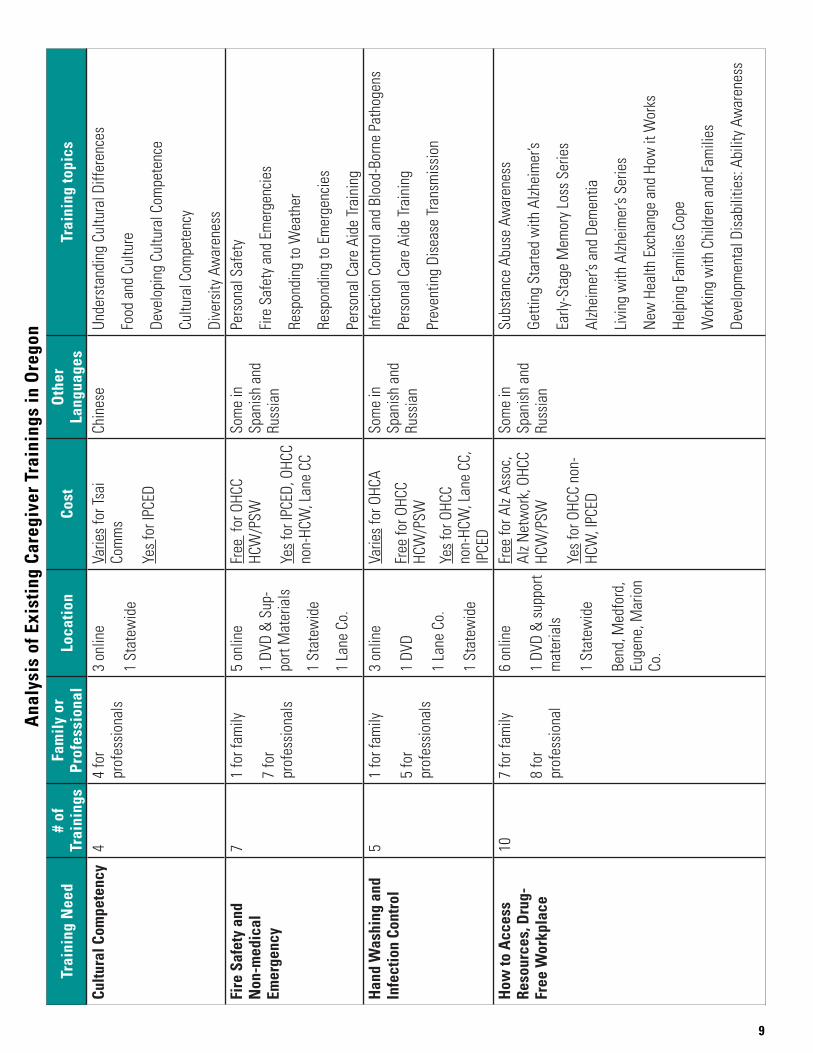
Analysis
This is a review of the “pivot table” and is based only on information provided by different entities participating in the work group at a certain point in time. Other trainings likely exist, for both family caregivers and professionals, but are not listed in this table. These other trainings may be offered in local communities by AAAs, health care entities such as health care systems, hospice/home health agencies, in-home care agencies, individual trainers, online resources, etc.
Many of the trainings in the table are listed under multiple categories and duplicated, as the courses often cross over areas of focus. For example, the Alzheimer’s and Dementia Series, the Early-Stage Memory Loss Series, the Dementia Caregiving training, and the Personal Care Aide training appear in multiple categories. This is also the case with the training need of “Safety,” in which many of the topics are also listed under “Maintaining a Clean and Safe Environment,” “Medication Management,” and “Preventing Skin Breakdown, Contractures and Falls.”
Two questions we considered cannot be answered at this time because we do not have data to analyze them. These questions pertain to the following issues:
• Certainneedshavetrainingsavailable,butpeoplearen’tawareofthem.
• Needsmaynotbemetbecausepeoplecan’tleavetheirlovedonealone,butthereisanassumptionthatfamily caregivers have difficulty attending trainings because of cost and/or not being able to find reliable care for their loved one.
Needs met with number of trainings available?
Training “needs” best addressed (meaning five or more trainings are available) for family caregivers are:
• Activities of Daily Living
• Basic Disease Information/Progression
• Behaviors as Communication
• Communication Skills
• How to Access Resources
• How to Take Care of Yourself
• Legal and Financial Issues/Adult Protective Services
• Managing Challenging Behaviors
• Maximizing Quality of Life and Safety
Training “needs” somewhat addressed (meaning three or four trainings are available) for family caregivers:
• Care Transitions
• Pain management (also listed under Maximizing Quality of Life)
• Person-centered care
• Professional Behavior/Boundaries Note: There is an assumption that person-centered planning is also addressed in other topics, such as Managing Challenging Behaviors and Maximizing Quality of Life.
16
Training “needs” best addressed (meaning five or more trainings are available) for professional caregivers:
• Activities of Daily Living
• Basic Disease Information/Progression
• Behaviors as Communication
• Body Mechanics
• Communication Skills
• Fire Safety and Non-Medical Emergencies
• Hand Washing and Infection Control
• How to Access Resources
• How to Take Care of Yourself
• Legal and Financial Issues/Adult Protective Services
• Managing Challenging Behaviors
• Maximizing Quality of Life
• Nutrition/Hydration
• Safety
Somewhat addressed (meaning three or four trainings are available) for professional caregivers:
• Cultural Competency
• Preventing skin breakdown
• Recognizing and responding to medical emergencies
• Person-centered planning
• Professional Behavior/Boundaries
Note: There is an assumption that person-centered planning is also addressed in other topics, such as Managing Challenging Behaviors and Maximizing Quality of Life.
17
Needs that have too little training available?
Training “needs” that seem to be the least addressed for family caregivers are:
• Body Mechanics
• Fire Safety and Non-Medical Emergencies
• Hand Washing and Infection Control
• Medication Management
• Nutrition/Hydration
• Pain Management
• Preventing skin breakdown, contractures and falls
• Recognizing and Responding to Medical Emergencies
• Sexuality
Training “needs” that seems to be the least addressed for professionals:
• Care Transitions
• Pain Management (or at least the signs and symptoms to watch for) —also listed under Maximizing Quality of Life
Lack of training in languages other than English
The Oregon Home Care Commission (OHCC) offers some classes at some locations in Spanish and Russian. Lane Community College also has written materials in Spanish. Tsai Communications offers one communication in Chinese. Classes in other languages are lacking.
18
Geographic locations where classes are offered
For Family Caregivers:
• Most classroom or in-person classes are offered through the Alzheimer’s Association Oregon Chapter at its offices, which are in Portland, Bend, Eugene, and Medford. The Alzheimer’s Network, which services Marion, Polk, Linn, and Benton counties, also provides in-person classes in Salem, Albany, and Corvallis.
• The Alzheimer’s Association also provides online classes.
• The majority of classes for professionals are offered online or through DVD with supporting materials.
o Only one online training entity provided information about its classes.
• For OHCC home-care and personal-support workers, trainings are available throughout the state: in Portland, Eugene, Hermiston, Burns, Newport, St. Helens, Prineville, etc. Family caregivers can also attend these trainings, but they must pay a fee.
Limitations/Barriers:
• Not all trainings are available in rural areas that would be easy for many caregivers to access
• Cost can be a factor, especially for family caregivers who have limited funds to pay for online or in-person training
• Family caregivers often require respite to be available for a training, and in many locations, respite is either not available or more expensive than the caregiver can afford
• For caregivers whose primary language is not English, limited classes are available in other languages
19
Recommendations
Develop trainings to address unmet needs
This report has identified ten needs for family caregivers and two needs for professionals that lack sufficient training opportunities. Businesses and nonprofits that provide trainings for caregivers should consider this list as a jumping-off point for the development of trainings that meet the unmet need. Further, government granting bodies, such as the Innovations Fund board, might want to use this list as a consideration for their grant process.
Of particular need for both family and professional caregivers is training on care transitions; many types of care transitions challenge a caregiver’s preparedness to provide services. Caregivers might gradually take on more tasks as needs change, and they should be aware of the built-up stress that comes with increasing the workload. Caregivers might be thrust into this role because of the occurrence of a sudden illness in which they find themselves performing medical or nursing procedures, monitoring conditions, managing illness-related behaviors, or navigating the health-care system. In addition to having the knowledge, skills, and ability to perform direct care, caregivers must be prepared emotionally and physically for the transitions.
Transitions between care settings create another level of training needs for caregivers. As medical settings discharge to home with expectations of follow-up care in the home and complicated regimens, caregivers need resources to help with this process. Before leaving the hospital, caregivers need clear instructions on medications, what to expect in recovery, what “red flags” to look for and what to do, when to make a follow-up appointment, and many other details about special diets, rehab needs, and other service needs.
Increase access to Home Care Commission trainings
The Oregon Home Care Commission (OHCC) offers a broad set of training topics and provides them in many locations around Oregon. In addition, the OHCC provides training in Russian and Spanish. But these trainings are primarily promoted to home-care and personal-support workers, which the Commission is constitutionally and statutorily charged to provide. The public, adult foster home providers, agencies, and others are participating in OHCC trainings (if there is still capacity) but for a fee, which may be cost prohibitive for many family caregivers. The Legislature has determined that the OHCC should collect fees from all participants who are not home-care or personal-support workers but has also supported increasing access to caregiver training. We recommend that the OHCC begin a process to determine how to make its trainings more available to the general public. The commission should explore the following ideas:
• Reduce the fee for family caregivers or using a “voucher” program for caregivers with financial need
• Look at new ways to promote the trainings to the public in the regions where capacity exists
• Use technology to provide trainings via the internet
• Any other ideas that would expand access to OHCC trainings to the general public
20
More aggressive promotion of existing trainings
The public is unaware of many caregiver trainings available in Oregon. We recommend several methods to ensure more people are aware of what is available in their community.
The ADRC should be promoted as the central place for Oregonians to find trainings. In addition, every training provider should be listed in the ADRC’s resource database.
• All providers of training, e.g. organizations (such as the Alzheimer’s Association), health systems, home health agencies, the Home Care Commission, the VA, and businesses, should be encouraged to have their training opportunities listed in the ADRC resource database.
• The ADRC’s media campaign should include the fact that it has information about available trainings for caregivers. The ADRC should also expand its advertising and outreach to ensure it is known as the place to find information about caregiver training.
• ADRC staff should receive ongoing training on how to identify when a caregiver could benefit from training, as well as what trainings would be appropriate and available in the caregiver’s area.
Hospitals, health systems, and medical professionals are often the first place to identify when someone may require caregiver training; frequently, it is at the point of diagnosis they will know a family will need help. Medical professionals should be prepared to provide information about what training would be useful, as well as where to find it.
• Oregon CCO innovator agents should identify and share best practices regarding how to identify potential caregivers in need of training and how to provide information to them.
• All medical professionals should be made aware of the ADRC as a primary resource for caregivers to access information about training.
• Organizations for medical professionals (e.g., Oregon Medical Association, Oregon Nurses Association, Oregon Academy of Family Physicians, etc.) should include a workshop on caregiver needs and how to connect caregivers with training at their annual conventions.
Expand access to trainings statewide
Many resources are available to caregivers in the major metropolitan areas of Oregon, but traveling even a short distance to attend a training might be prohibitive for many caregivers. This impact is magnified when few or no trainings are available in a 100-mile radius from the caregiver’s home. We recommend several ways to improve access to training.
Technology is a useful tool for some caregivers —but not all. For those who have a computer and broadband Internet access, training providers should make better use of webinars. Providers that already offer online training should consider special promotion of those options if people are not widely aware of them. This recommendation also applies to any government-supported training. Innovations Fund resources could be employed to support the development of technology infrastructure of nonprofit training providers, and Oregon Long Term Care Quality Fund resources could be used to increase Web-based training for professional caregivers.
The need for respite is a critical barrier to caregivers who seek training. Even if a training is offered a few blocks away and for free, family caregivers often can’t leave the person for whom they are providing care. Providing some respite care is critical for many caregivers to receive training that would help them provide better care and improve their own quality of life. We recommend expanding respite programs throughout Oregon, possibly by reviving the
21
Lifespan Respite Care Program, which would require adequate and reliable funding.
An often overlooked yet simple method for providing training across the state is to use the media; cable providers offer on-demand programming, as well as public-access TV stations, many of which will air what their local communities ask. Organizations and agencies could create trainings in a format appropriate for television and record them on a DVD, which they could provide to the public-access station. Cable companies are often looking to add programming to their on-demand services, and if they are provided content for free, they may include it in their offerings.
This recommendation requires further research, but it has the potential to expand the availability of training to anyone with cable television service.
Ensure family caregivers are informed about caregiving and how to choose a useful training.
Realizing that you are becoming a caregiver can be terrifying; most people do not plan or expect to be caregivers, and they will enter into the role unwillingly and unprepared. Further, not only do they not know what to expect, they might not seek helpful training because they don’t know where to begin or how to select a training that would be useful for them.
We recommend the creation of a simple brochure that lists what a caregiver might need help with and what to consider when looking for a training. It would be a generic document about caregiving that could be supplemented by information specific to the situation (e.g., Alzheimer’s disease, brain injuries, autism, etc.). The brochure should be made available in all medical offices, ADRCs, senior and community centers, libraries, and any other relevant locations. Additionally, it should be included in any packet of information medical providers give families following a diagnosis that may lead to someone serving as a family caregiver.
22
List of Oregon Caregiver Training Work Group Participants
Jon Bartholomew, Alzheimer’s Association Oregon Chapter and Governor’s Commission on Senior ServicesBarbara Bieg, Governor’s Commission on Senior ServicesAllison Bookman, Volunteers of AmericaChris Bouneff, NAMI OregonJeff Brandon, Governor’s Commission on Senior ServicesPeggy Brey, Oregon Association of Area Agencies on Aging and DisabilitiesPatty Brost, Governor’s Commission on Senior ServicesSharon Brothers, Institute for Professional Care EducationKevin Call, Adeo In Home CareMargaret Cervenka, Leading AgeLeah Christensen, VARuth Cohen, AARPPetronella Donovan, Independent Adult Care Home AssociationNicole Easley, Marquis CompaniesStacey Franklin, VARep. Vic Gilliam,Lee Girard, Multnomah CountyJenna Hahn, Oregon Geriatrics SocietyAmy Hoffman, Alzheimer’s Network of OregonLeslie Houston, Home Care CommissionJeannette Hulse, Oregon Department of Human Services, Aging and People with DisabilitiesSuanne Jackson, State of Oregon, State Unit on AgingMary Jaeger, Oregon Long Term Care OmbudsmanJan Karlen, DHSBeth Kessler, Oregon Council on Developmental DisabilitiesJennifer Lawrence, VAAllison Lindauer, OHSUAnnie Lupei, Independent Adult Care Home AssociationRuth McEwen, Oregon Disabilities CommissionLoriann McNeill, Multnomah CountyAnn McQueen, Oregon Department of Human Services, Aging and People with DisabilitiesSen. Laurie Monnes-Anderson,Elizabeth O’Neill, State of Oregon, State Unit on AgingDiane Roberts, Oregon Association for Home CareMary Ruhl, OHSUPam Ruona, Oregon Health Care AssociationRandy Samulson, HASL Center for Independent LivingMary Scott, Mennonite VillageBandana Shrestha, AARPSerena Smith, Partnerships in Community Living Becki Sparre, Brain Injury Association of OregonSherry Stock, Brain Injury Association, Oregon Disabilities CommissionKirt Toombs, Eastern Oregon Center for Independent LivingMolly Trauten, Marie Smith Center Lori Watt, State of Oregon, State Unit on AgingJean Yamamoto, SEIU Local 503
Appendix