pseudo tumour of the and polyarteritis - …jcp.bmj.com/content/jclinpath/12/5/419.full.pdf ·...
TRANSCRIPT

J. clin. Path. (1959), 12, 419.
PSEUDO TUMOUR OF THE ORBIT ANDPOLYARTERITIS NODOSA
BY
E. W. WALTONFrom the Department of Pathology, King's College, Durham University, in the Royal Victoria Infirmary,
Newcastle upon Tyne
(RECEIVED FOR PUBLICATION DECEMBER 14, 1958)
Pseudo tumour of the orbit, or chronicgranuloma as it is frequently called, is a fairlycommon clinical condition. Though most casesare of unknown aetiology, a few prove to bemanifestations of systemic disease. The purposeof this paper is to report a case where the clinicaldiagnosis of pseudo tumour of the orbit was madeand polyarteritis nodosa, suspected during life,was confirmed at necropsy.
Case ReportW. 0. Y., a bus conductor, aged 53 years, was first
seen on August 29, 1955. For two months he hadhad shooting pains in the left temple with frequentheadache. A month later the vision of the left eyedeteriorated and he was told the eye bulged forwards.He then had two brisk epistaxes. On examinationthe right eye was normal; the left showed 5 mm.proptosis, limitation of all movements, and absenceof the direct light reflex, though the consensual reflexwas present. A dense central scotoma wasdemonstrated on the left side, yet the fundus appearednormal. The pulse was 76 per minute, blood pressure150/90 mm. Hg. Radiological examination showedopacity of the left posterior ethmoidal region with asuggestion of bone destruction. A blood count wasnormal apart from slight anaemia (haemoglobin12.7 g. per 100 ml.), and the plasma proteins showedreversal of the A/G ratio (total 6.6 g. per 100 ml.,albumin 2.8 g., globulin 3.8 g.). Blood Wassermannand Kahn reactions were negative. The urinecontained a trace of albumin but no abnormal cellsand the blood urea was 66 mg. per 100 ml.Exploration of the ethmoidal and sphenoidal air cellsrevealed thick mucus only: a biopsy of the thickenedmucosa showed a granulomatous lesion of chronic,non-specific type with marked endarteritis but nomicro-organisms.
Despite treatment with penicillin, he did notimprove. and within some five weeks was blind in theleft eye. The pupil was fixed, the veins wereengorged, and optic atrophy had developed.Orbitonometry showed a progressive increase in the
proptosis and in the consistency of the orbitalcontents. Exenteration of the orbit was performedon October 13 (sixth week). A hard pale mass wasfound in the posterior ethmoidal air cells, penetratingthe superior and inferior orbital fissures to surroundthe optic nerve. The histological report on the biopsywas:
"The specimen shows a granulomatous lesiondescribed as pseudo tumour of the orbit. As similarmaterial was removed from the ethmoid, it is likelythat the lesion originates there. Lesions of theabove type have been described in association withperiarteritis nodosa. Is there evidence of systemicdisease in this patient ? " (Dr. R. 0. K. Schade).After the operation the headaches ceased but
recurred two weeks later on the right side. Blurringof vision appeared and a dense central scotomawas demonstrated, similar to that which previouslydeveloped in the left eye. A course of x-ray therapywas given to the posterior orbit in an endeavour toarrest the disease, but the patient's general conditionbegan to worsen; he developed a swingingtemperature and became very apathetic. OnNovember 28 signs of peritonitis appeared and atlaparotomy a gangrenous, perforated appendix wasremoved. His condition rapidly deteriorated and hedied the following day. There was no terminal risein blood pressure.
NecropsyThe body was wasted. The left orbit was lined
by an apparently healthy graft. Apart from therecent surgical incision in the abdomen there wasnothing else of note externally.
Skull.-The dura in the anterior cranial fossaeand over the vertex was diffusely thickened anda purulent pachymeningitis was present, localizedto these areas. The right orbit, the frontal,maxillary, and anterior and middle ethmoidalsinuses appeared normal. The bone over both thesphenoidal and the left posterior ethmoidal sinuseswas elevated and thinned; these air cells contained
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from
E. W. WALTON
a smooth, fleshy mass of yellowish material,homogeneous and adherent to bone. Pus waspresent in the nasal cavity. The brain, pituitary,and middle ears were normal. The mucosa ofthe nasopharynx and soft palate was congested;otherwise the mouth, tonsils, fauces, and pharynxwere healthy.Chest.-The lungs were heavy and on section
showed areas of early bronchopneumonia: thebronchial tree and main pulmonary vessels werenormal. The heart was of normal size. Thecoronary arteries, especially the descending branchof the left vessel, were tortuous and showed manynodular thickenings which on section were smallaneurysms, filled with recent thrombus. The aortaand its main branches were normal apart fromatheroma.Abdomen.-A recent fibrinous peritonitis was
present. Numerous mucosal erosions were presentin the bowel, especially in the ileum andrectosigmoid. The liver was of normal size andthe parenchyma was mottled and congested:numerous ante-mortem thrombi were present inmajor branches of the portal vein and in nodositiesof the hepatic artery (Fig. 1). The spleen weighed300 g. and was extensively infarcted (Fig. 2). Thekidneys together weighed 520 g. Multiple recentinfarcts were present in each and the cortices wereextensively swollen and blurred. Many of themain branches of each renal artery containedthrombus (Fig. 3). Jnfarcts were present in eachtestis (Fig. 4).The gastroduodetial, left spermatic, and left
gastric arteries and major branches of the splenic,hepatic, renal, and superior mesenteric arterieswere grossly nodular, the aneurysms all containingante-mortem thrombus. The other main vesselswere healthy. All other organs and tissues werenormal. Bacteriological examination of materialfrom the paranasal sinuses was negative.
HistologyReview of the biopsies from the left orbit
and ethmoidal sinuses shows in each a chronicgranuloma of non-specific type. In the orbit thegranuloma tightly ensheaths the optic nerve andhas replaced much of the orbital fat. The densecellular infiltrate consists largely of macrophages,plasnia cells, lymphocytes, and neutrophilpolymorphs: eosinophil polymorphs are quitefrequent, but there is no epithelioid cell reactionand the infrequent giant cells are of foreigni bodytype. The infiltrate, perivascular in places (Fig. 5),has in most areas fused to form a solid mass. Thelyrnphocytes are in places arranged into pseudo
follicles without germ centres. At the periphery,the lesion invades the orbital muscles. Manyvessels, both arterioles and venules, show peri-vascular infiltration but are otherwise normal.The ethmoidal mucosa is greatly thickened by
fibrous tissue and patchily infiltrated by cells ofsimilar type but fewer in number than in theorbital granuloma. There are no giant cells andno focal granulomata. The arteries show fibrosisof all layers with reduplication of elastica andnarrowing of the lumen. No defects of elasticaare present, and the lesions, though reminiscent,are not diagnostic of polyarteritis nodosa. Similarchanges are seen in the necropsy specimens fromthe sphenoidal and left ethmoidal air cells. Nomicro-organisms are seen in sections from eachgranuloma stained by the Ziehl-Neelsen, Gram,and P.A.S. methods. Areas of myelin degenerationare presertt in the right optic and oculomotornerves; there is infarction in the ocular muscle.but no granuloma is present on this side.The necropsy material shows vascular lesions
(Figs. 6-11) in many organs and tissues (Table 1).
TABLLE ISITES OF LESIONS
GranulomaLeft orbit
ethmoidal sinusesBoth sphenoidal
ArteritisRecent
Coronary, gastroduodenal, leftgastric and left spermaticarteries
Branches of splenic, hepatic,renal, and mesenteric arteries
Right optic nerveRight orbital fatDura materEpiglottis, trachea, stomach,
ileum, rectum, liver, pan-creas, spleen, kidney, epidi-dymis
InfarctionHeartSpleenPancreasKidneyTestesRight ocular muscles
Acute inflammationPachymeningitisTracheitis, bronchitis, andbronchopneumonia
Proctitis
OldRight optic nerveRight ethmoidal sinusesNasal septum, tongue,
vocal cord, thyroid, liver,pancreas, kidney, spermaticcord, seminal vesicles
Brachial plexusSciatic nerve
Small and medium-sized arteries are principallyinvolved though occasional affected arterioles andeven capillaries are seen in the spleen and kidneys.Veins are not affected though thrombi are presentin small veins in the liver, kidney, and lacrimalglands. The lesions are focal and often segmental
420
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from
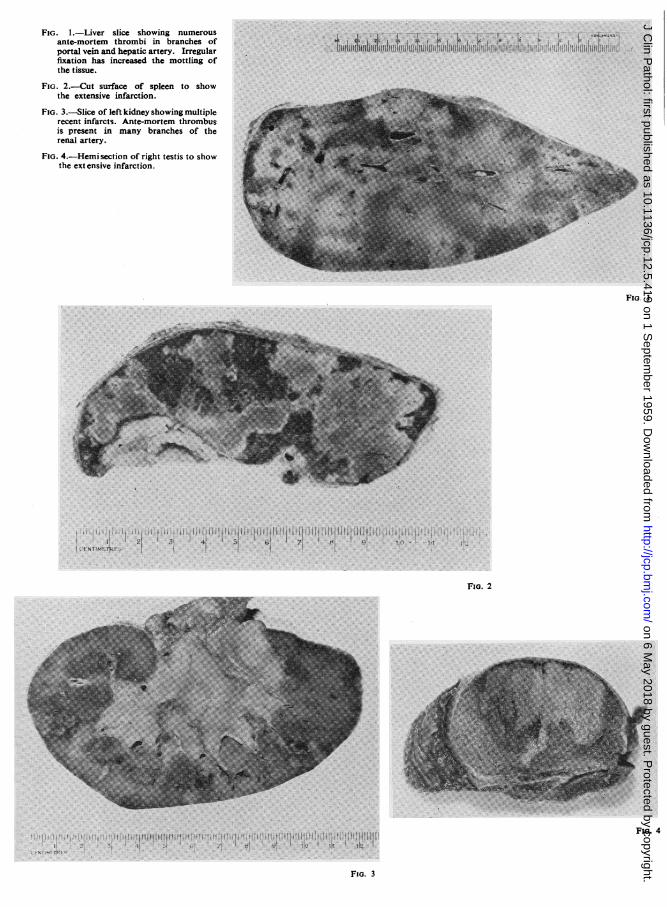
FIG. 1.-Liver slice showing numerousante-mortem thrombi in branches ofportal vein and hepatic artery. Irregularfixation has increased the mottling ofthe tissue.
FIG. 2.-Cut surface of spleen to showthe extensive infarction.
FIG. 3.-Slice of left kidney showing multiplerecent infarcts. Ante-mortem thrombusis present in many branches of therenal artery.
FIG. 4.-Hemi section of right testis to showthe ext ensive infarction.
Fso. I
21 7I~~~~~~i
FIG. 2
Fio. 4
it
FiG. 3
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from
jp:Ai,V t
wsv
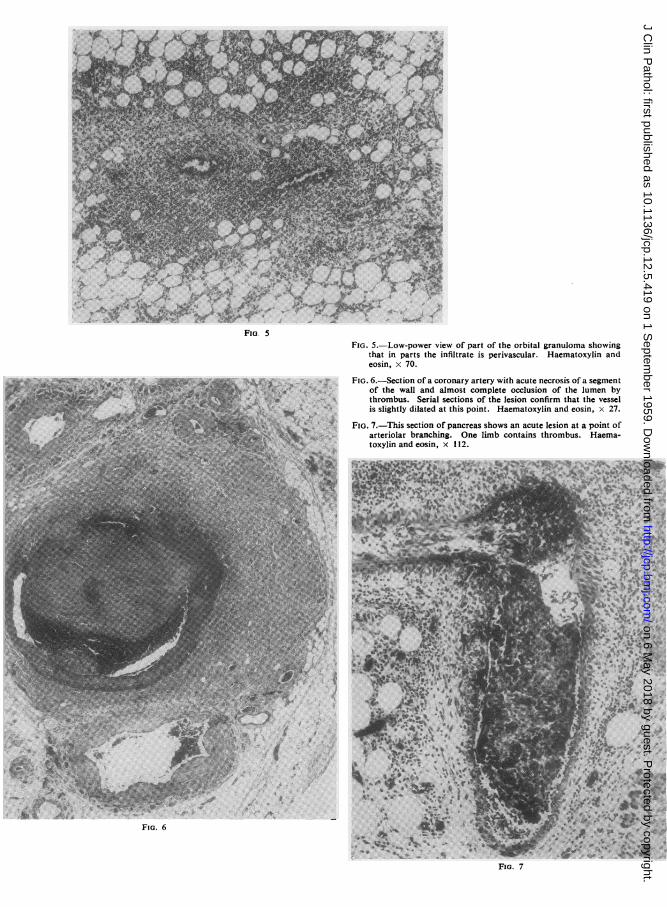
Fla. 5FIG. 5.-Low-power view of part of the orbital granuloma showing
that in parts the infiltrate is perivascular. Haematoxylin andeosin, x 70.
FIG. 6.-Section of a coronary artery with acute necrosis of a segmentof the wall and almost complete occlusion of the lumen bythrombus. Serial sections of the lesion confirm that the vesselis slightly dilated at this point. Haematoxylin and eosin, x 27.
FIG. 7.-This section of pancreas shows an acute lesion at a point ofarteriolar branching. One limb contains thrombus. Haema-toxylin and eosin, x 112.
FIG. 6
FIG. 7
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from
.ft
An AiA.A*~ *W ~ lk O
.X ilp
,;. w 4,,D je j.
N
~~~~~~~~~~~k
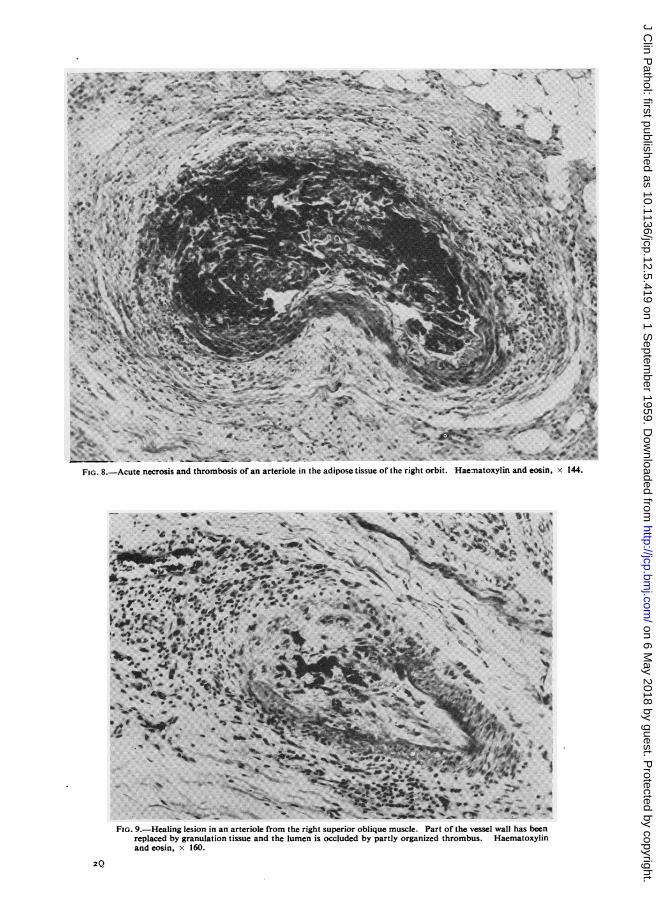
FI.8-ct erssadtrmoi fanatroei h dps iseo h igtobt araoyi n oi,x14
\ %; > - _ tIl o., , ... ,~~~~Mb
, e .. -
;4W> sb , tt r ... 4 # _ ,w:t~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.......
FIG. 9.-Healing lesion in an arteriole from the right superior oblique muscle. Part of the vessel wall has beenreplaced by granulation tissue and the lumen is occluded by partly organized thrombus. Haematoxylinand eosin, x 160.
2Q
i0
R
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from
* *
::s. - --...,. .......1
;
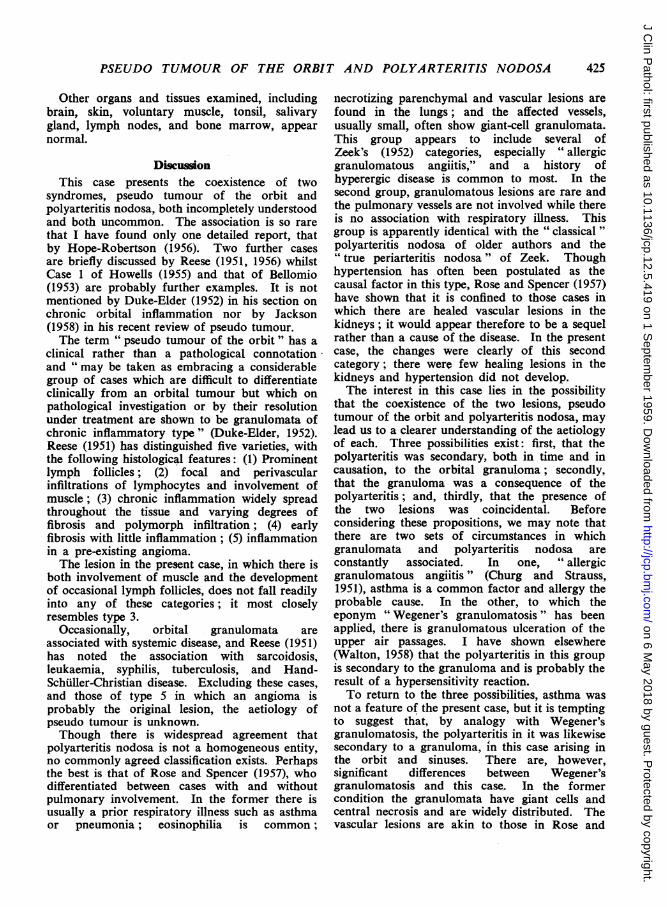
FIG. 11.-Serial sectiorelastica. Weig
A.4~~~ ~ ~ ~ ~ ~ ~~~~.
numroucaillrie.Hemtoxli anaoi,x15
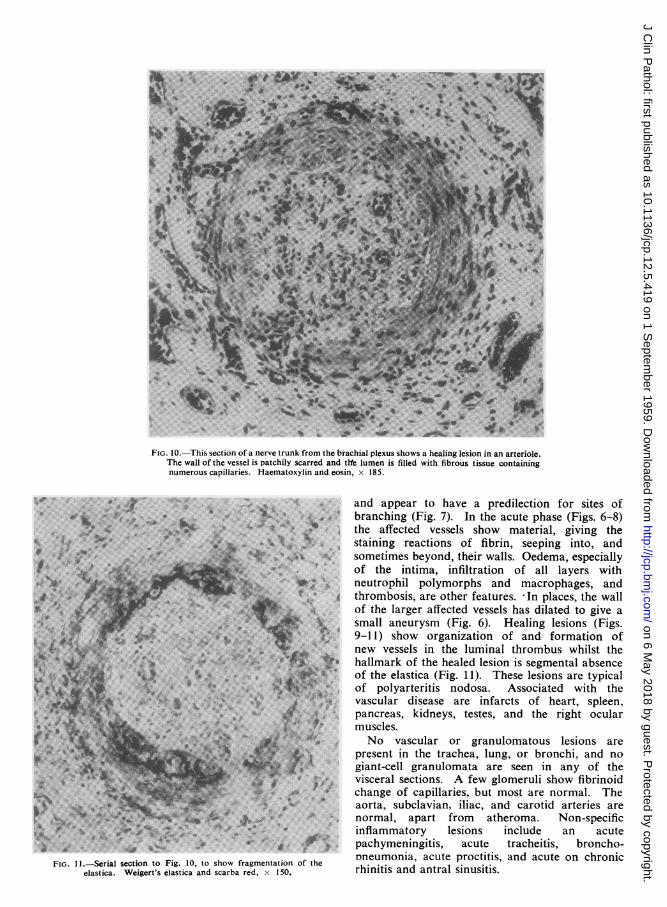
FG10. Thi sectio ofanretrnroh bachia aplexus showa healigvesapedioninranteareioe
L.* * branching (Fig. 7). In the acute phase (Figs. 6-8)jl^lFr= X.eS* r ....... ithe affected vessels show material, giving the
i*g + *\ =* - ^ staining reactions of fibrin, seeping into, andu* ~ ~~~~~ *.e*>"s ¢ sometimes beyond, their walls. Oedema, especially:E_ 'e;......... . §P, ^of the intima, infiltration of all layers with
^ %; W>vi neutrophil polymorphs and macrophages, and|9u''s - P _ t Ba gthrombosis, are other features. ln places, the wall°tXPU vY X X of the larger affected vessels has dilated to give a*
g . \ ~~~~~small aneurysm (Fig. 6). Healing lesions (Figs.ssj@ v g = w ~9-11) show organization of and formation of
inJ,,=snew vessels in the luminal thrombus whilst the-TeFF S^ **P;> t hallmark of the healed lesion is segmental absence%804R M|egel. of the elastica (Fig. 11). These lesions are typical
xx** 3< F X t ^ of polyarteritis nodosa. Associated with the*6 #* t.w.....#.>;; 't X svascular disease are infarcts fhat peny
$* ' 8Xffai ''. s# 'pancreas, kidneys, testes, and the right ocular#.,iS: [SB s2 muscles.|2*ci9;@ ; z x< 2Kw No vascular or granulomatous lesions are.....e .. .'T«present in the trachea, lung, or bronchi, and no
|t gf2-M ~~~~giant-cell granulomata are seen in any of the#~~~~~ * , ,'3 visceral sections. A few glomeruli show fibrinoid*4^ ,v^+ change of capillaries, but most are normal. The
iiit * * s ~~~aorta, subclavian, iliac, and carotid arteries are$g~ v> * w *normal, apart from atheroma. Non-specific
*t.Z*jK.* ^ 2 ;^ inflammatory lesions include an acute.i~~~~9t* f pachymeningitis, acute tracheitis, broncho-toig.10tohowfrgmetatonof he oneumonia, acute proctitis, and acute on chronic
.ert's elastica~and scarba red, 150 rhinitis and antral sinusitis.,IF. a-- ;.M CWO. -sW1- va.s/-
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from
PSEUDO TUMOUR OF THE ORBIT AND POLYARTERITIS NODOSA
Other organs and tissues examined, includingbrain, skin, voluntary muscle, tonsil, salivarygland, lymph nodes, and bone marrow, appearnormal.
DiscuLionThis case presents the coexistence of two
syndromes, pseudo tumour of the orbit andpolyarteritis nodosa, both incompletely understoodand both uncommon. The association is so rarethat I have found only one detailed report, thatby Hope-Robertson (1956). Two further casesare briefly discussed by Reese (1951, 1956) whilstCase 1 of Howells (1955) and that of Bellomio(1953) are probably further examples. It is notmentioned by Duke-Elder (1952) in his section onchronic orbital inflammation nor by Jackson(1958) in his recent review of pseudo tumour.The term " pseudo tumour of the orbit " has a
clinical rather than a pathological connotationand " may be taken as embracing a considerablegroup of cases which are difficult to differentiateclinically from an orbital tumour but which onpathological investigation or by their resolutionunder treatment are shown to be granulomata ofchronic inflammatory type" (Duke-Elder, 1952).Reese (1951) has distinguished five varieties, withthe following histological features: (1) Prominentlymph follicles; (2) focal and perivascularinfiltrations of lymphocytes and involvement ofmuscle; (3) chronic inflammation widely spreadthroughout the tissue and varying degrees offibrosis and polymorph infiltration; (4) earlyfibrosis with little inflammation; (5) inflammationin a pre-existing angioma.The lesion in the present case, in which there is
both involvement of muscle and the developmentof occasional lymph follicles, does not fall readilyinto any of these categories; it most closelyresembles type 3.
Occasionally, orbital granulomata areassociated with systemic disease, and Reese (1951)has noted the association with sarcoidosis,leukaemia, syphilis, tuberculosis, and Hand-Schuiller-Christian disease. Excluding these cases,and those of type 5 in which an angioma isprobably the original lesion, the aetiology ofpseudo tumour is unknown.Though there is widespread agreement that
polyarteritis nodosa is not a homogeneous entity,no commonly agreed classification exists. Perhapsthe best is that of Rose and Spencer (1957), whodifferentiated between cases with and withoutpulmonary involvement. In the former there isusually a prior respiratory illness such as asthmaor pneumonia; eosinophilia is common;
necrotizing parenchymal and vascular lesions arefound in the lungs; and the affected vessels,usually small, often show giant-cell granulomata.This group appears to include several ofZeek's (1952) categories, especially " allergicgranulomatous angiitis," and a history ofhyperergic disease is common to most. In thesecond group, granulomatous lesions are rare andthe pulmonary vessels are not involved while thereis no association with respiratory illness. Thisgroup is apparently identical with the " classical "polyarteritis nodosa of older authors and the" true periarteritis nodosa " of Zeek. Thoughhypertension has often been postulated as thecausal factor in this type, Rose and Spencer (1957)have shown that it is confined to those cases inwhich there are healed vascular lesions in thekidneys; it would appear therefore to be a sequelrather than a cause of the disease. In the presentcase, the changes were clearly of this secondcategory; there were few healing lesions in thekidneys and hypertension did not develop.The interest in this case lies in the possibility
that the coexistence of the two lesions, pseudotumour of the orbit and polyarteritis nodosa, maylead us to a clearer understanding of the aetiologyof each. Three possibilities exist: first, that thepolyarteritis was secondary, both in time and incausation, to the orbital granuloma; secondly,that the granuloma was a consequence of thepolyarteritis; and, thirdly, that the presence ofthe two lesions was coincidental. Beforeconsidering these propositions, we may note thatthere are two sets of circumstances in whichgranulomata and polyarteritis nodosa areconstantly associated. In one, " allergicgranulomatous angiitis" (Churg and Strauss,1951), asthma is a common factor and allergy theprobable cause. In the other, to which theeponym "Wegener's granulomatosis " has beenapplied, there is granulomatous ulceration of theupper air passages. I have shown elsewhere(Walton, 1958) that the polyarteritis in this groupis secondary to the granuloma and is probably theresult of a hypersensitivity reaction.To return to the three possibilities, asthma was
not a feature of the present case, but it is temptingto suggest that, by analogy with Wegener'sgranulomatosis, the polyarteritis in it was likewisesecondary to a granuloma, in this case arising inthe orbit and sinuses. There are, however,significant differences between Wegener'sgranulomatosis and this case. In the formercondition the granulomata have giant cells andcentral necrosis and are widely distributed. Thevascular lesions are akin to those in Rose and
425
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from

E. W. WALTON
Spencer's (1957) first group, small vessels in thelung being especially involved. In the case underdiscussion, no giant cells were found in the lesions,the granulomata were present only in the orbitand paranasal sinuses, the lungs were not affected,and the vascular lesions, involving mainly vesselsof medium size, clearly come into Rose andSpencer's second category. Furthermore, noclinical evidence of hypersensitivity was noted.There is thus no convincing evidence that thevascular lesions were caused by the orbitalgranuloma.More likely is the second possibility that the
orbital and sinusoidal lesions were a result of thepolyarteritis, being the sequel of confluence ofnumerous perivascular infiltrates. In the case ofpolyarteritis nodosa with chronic orbital myositisdescribed by Bellomio (1953), inflammatorylesions of the orbital muscles were thought by theauthor to be the direct result of polyarteritis. InHope-Robertson's (1956) case an interval of twoand a half years elapsed between the diagnosis ofpseudo tumour of the orbit and the demonstrationat necropsy of polyarteritic lesions. In thepresent case, re-examination of serial sectionsfrom the orbital and sinusoidal biopsies showedno vascular lesions of the kind at necropsy. Thisproposition is therefore no more than surmise andvery possibly the coexistence of the two lesionsis mere coincidence. Nevertheless, it seemsjustifiable to suggest, on the basis of this case,that in cases of orbital granuloma, especially in
the presence of symptoms and signs of widespreaddisease, a vasculitis should be considered as apossible aetiological factor.
SummaryA case is reported in which the presenting
clinical picture was that of pseudo tumour of theorbit. At necropsy, polyarteritis nodosa, suspectedduring life because of the perivascular nature ofthe orbital granuloma, was confirmed. Thebearing this rare association has on the aetiologyof pseudo tumour, the relationship with Wegener'sgranulomatosis, and the classification andaetiology of necrotizing arteritis are brieflydiscussed.
I am indebted to Mr. H. Vernon Ingram forpermission to publish this case, to Mr. A. E. Youngand Mr. J. W. Corkhill for the illustrations, and toProfessor J. B. Duguid, Professor A. C. Lendrum,Dr. R. 0. K. Schade, Dr. 1. Rannie, and Dr. W. W.Park for advice and encouragement.
REFERENCESBellomio, S. (1953). Riv. ital. Tracoma, 5, 103.Churg, J., and Strauss, L. (1951). Amer. J. Path., 27, 277.Duke-Elder, S. (1952). Text-book of Ophthalmology, Vol. 5, p. 5448.
Henry Kimpton, London.Hope-Robertson, W. J. (1956). Trans. ophthal. Soc. N.Z., 8, 56.Howells, G. H. (1955). J. Laryng., 69, 309.Jackson, H. (1958). Brit. J. Ophthal., 42, 212.Reese, A. B. (1951). Tumors of the Eye, p. 522. Paul B. Hoeber,
New York.-(1956). Atlas of Tumor Pathology, Section X, Fascicle 38:
Tumors of the Eye and Adnexa, p. 204. Armed Forces Instituteof Pathology, Washington, D.C.
Rose, G. A., and Spencer, H. (1957). Quart. J. Med. n.s., 26, 43.Walton, E. W. (1958). Brit. nwed. J., 2, 265.Zeek, P. M. (1952). Amer. J. ctin. Path., 22, 777.
426
on 6 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.12.5.419 on 1 Septem
ber 1959. Dow
nloaded from