polyarteritis nodosa and congenital pyloric hypertrophy … · j. clin. path. (1960), 13, 291....
TRANSCRIPT
J. clin. Path. (1960), 13, 291.
POLYARTERITIS NODOSA AND CONGENITAL PYLORICHYPERTROPHY IN A 3-MONTH-OLD INFANT
BY
T. R. SAVAGE AND J. F. SMITH*From Wanstead Hospital, Essex, and the Bernhard Baron Institute of Pathology,
London Hospital, E.]
(RECEIVED FOR PUBLICATION FEBRUARY 12, 1960)
A case of polyarteritis nodosa in the first year of life with the clinical picture dominated bypyrexia, an initial upper respiratory element, episodes of tachycardia, and sudden death three weeksafter the onset is described. The necropsy showed evidence of polyarteritis nodosa, myocarditis,and valvulitis as well as congenital pyloric hypertrophy. Clinical manifestations of the latter hadpreceded the final illness and the two diseases were not thought to be related.The previous 19 cases reported in the first year of life are reviewed, and support is given for the
concept that at this age a rash, pyrexia, upper respiratory manifestations, and progressive heartfailure or sudden death are characteristic clinical manifestations and that the heart is often the siteof the major lesions at necropsy.The possible role of hypersensitivity is discussed. There was no evidence for it in the present case.
Polyarteritis nodosa is uncommon in infancy;references to 19 cases diagnosed as such in thefirst year of life have been found; there are afew others we have not been able to check (thecases of Ruger, 1944, and Wright, 1948). Ofthose checked all except the ones reported byDe Pascale (1955) and Legros (1944) have provedfatal. These authors reported cases in which themain manifestations of the disease were in theskin, and it is possible that they were not dealingwith examples of true polyarteritis nodosa butrather that group described as " allergic " vascu-litis by McCombs, Patterson, and McMahon(1956) in which recovery is common. Many ofthe fatal cases had features indicating involve-ment of the skin, upper respiratory tract, and heartduring life and maximal lesions in the coronaryarteries at necropsy. In the infant reported inthis paper such features were preceded by clinicalsymptoms of congenital pyloric hypertrophywhich was also found at necropsy. Furthermore,a diffuse myocarditis and valvulitis similar to thatof severe acute rheumatism formed part of thepathological picture.
Case ReportC.Q., a boy, had weighed 9 lb. 7 oz. at birth, the
pregnancy and labour being normal. The father hadhad pulmonary tuberculosis which was reported cured*Present address: University College Hospital Medical School.
University Street, London, W.C.1.
in 1946. There was no other family history of illnessand none of allergy. The infant was breast fed andat the age of 9 weeks was admitted to hospital witha history of constipation and increasing vomiting afterfeeds for two weeks; in the preceding four days everyfeed had been returned. A provisional diagnosis ofhypertrophic pyloric stenosis was made. On examina-tion the baby was well nourished and hydrated.There was visible peristalsis, but no pyloric tumourwas palpated and there were no other physical signs.The vomiting ceased during administration of atropinemethyl nitrate which was continued for several days.
In the absence of a pyloric tumour a diagnosis offeeding difficulty was made and he was dischargedhome after three days. The infant remained well andcontinued to gain weight until the age of 12 weeks,when a cough, purulent nasal and conjunctivaldischarge, and bilateral cervical lymph node enlarge-ment developed. After five days he was againadmitted to hospital; pyrexia, mostly 100-103° F.,swinging at times, was present during the remainderof his life, a further two and a half weeks; the liverwas palpable to two fingerbreadths.
Investigations.-No pathogens were isolated fromnose and throat swabs or from faeces. The cerebro-spinal fluid was clear; cells 16/c.mm. (50% lympho-cytes, 500% endothelial cells); protein 30 mg. /100 ml.,sugar 55 mg. /100 ml.; culture sterile. A blood countshowed Hb 70% ; red cells 4.3 million; white cells32,000 (neutrophils 85%, eosinophils 5%, lymphocytes7%, monocytes 3%, reticulocytes 0.2%); blood urea35 mg./100 ml. A blood culture showed a coagulase-negative staphylococcus (regarded as a contaminant).There was no agglutination with S. typhi, paratyphi,
on June 30, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.13.4.291 on 1 July 1960. D
ownloaded from
T. R. SAVAGE and J. F. SMITH
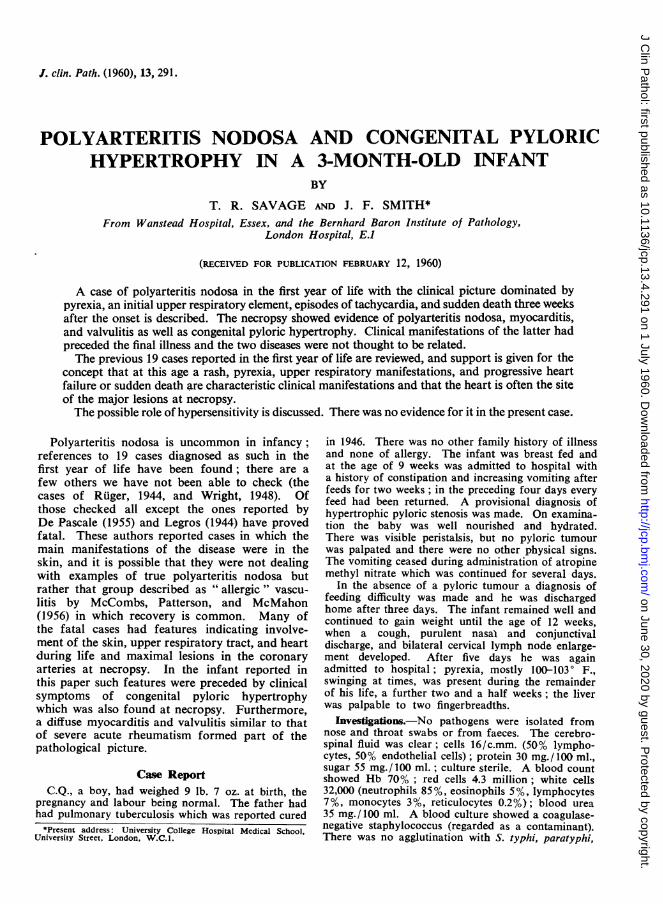
FIG. I.-F:hotograph of heart. At 1, 2, and 3 aneurysms of thecoronaries containing thrombus are seen in section. At 4, abranch of the coronary is cut across as it runs down the surfaceof the ventricle; the thickened wall causes the vessel to standout as a cord.
and typhi murium. A direct Coombs test was nega-tive. The Mantoux test at 1:100 was negative. Areport on iliac marrow (Dr. H. Caplin) read:
I. . . the main feature was intense granulocytosiswith a preponderance of metamyelocytes andjuvenile polymorphs. Nucleated red cells appearedscanty, the myeloid-erythroid ratio being approxi-mately 30: 1. The appearances were in keepingwith a pronounced reaction to pyogenic infection."Urine contained no protein or sugar; a few leuco-
cytes and epithelial cells were found in the depositand a culture showed coagulase-negative staphylo-coccus (regarded as a contaminant).
Radiogrophs of the chest and the whole skeletonwere normal. An electrocardiogram with a rate of180 per min. approximately and with right axisdeviation was interpreted as indicative of sinus tachy-cardia only.
Progress and Treatment.-A single injection ofcrystalline penicillin, 100,000 units, was given onadmission, then chloramphenicol, 250 mg. by mouthsix hourly for three days; and then streptomycin,100 mg. 12 hourly, and penicillin, 100,000 units fourhourly, both intramuscularly, for a further threedays. Six days after this, terramycin, 70 mg. sixhourly by mouth, was given for 48 hours. None ofthese drugs had any effect on the pyrexia. The onlyother drug given was atropine methyl nitrate, 3 dropsbefore feeds during the first five days of this secondadmission.
A sudaminal type of rash appeared on the upperlimbs three days after admission and was presentintermittently during the rest of the illness on alllimbs. The liver remained palpable, the apical pulserate was 160-180 on two occasions, the complexionwas sallow but without jaundice. Feeding was satis-factory and stools were normal. Dr. KennethTallerman kindly agreed to accept responsibility forthe care of the baby and he was transferred to theLondon Hospital where he suddenly collapsed anddied 60 hours after admission. In that time thelaboratory findings remained unchanged; a chest filmwas normal and a blood culture sterile.Necropsy Report.-The findings may be summar-
ized as acute heart failure, myocarditis, polyarteritisrodosa, and congenital pyloric hypertrophy. Bodyweight 154 lb.Heart (2 oz.).-Scattered nodular aneurysms of the
circumflex branch of the left and terminal part ofthe right coronary artery were present; they had abluish-red, projecting surface and on section containedrecent thrombus (Fig. 1), the latter extending for a fewcentimetres on either side of the dilatation. The wallof the right coronary artery was slightly thickened (upto 0.05 cm.) proximal to the thrombus. Most of thefree margin of the mitral valve and a segment (1.5cm. long) of the tricuspid valve were slightly
4-
WAV
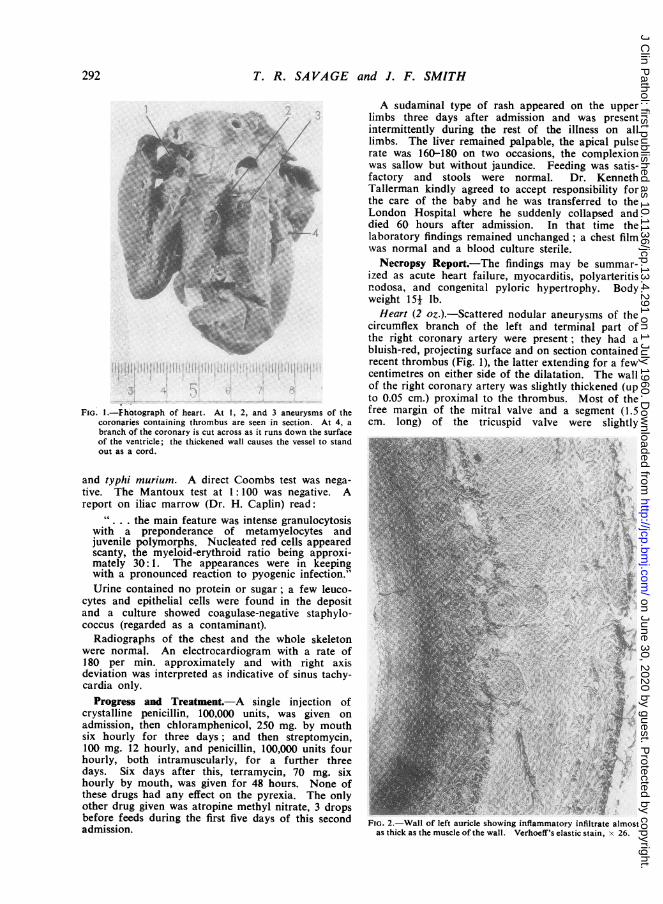
FIG. 2.-Wall of left aurscle showing inflammatory infiltrate almostas thick as the muscle of the wall Verhoeff's elastic stain, x 26
292
on June 30, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.13.4.291 on 1 July 1960. D
ownloaded from
vi n
Ae~~~~ ~ ~~~~~~~~~'
A. ~ ~ t 4$
............ 7L.N '
4. S~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.A.$'?:$4~~~~~~~s'~~~ ~~- -,~~~~ 4*~~~ ~ ~ 4 ,'r~~~~~~~i
MEL~~ ~ ~ ~ ~ ~
.4'V~~~~~~~~~c~~~g.~~~~~~~~~¾ ~ ~ ~ ~ ~ ~ .VS~
r~~~~~~~~~~~~~~~~~~~
p. or~~Op4 N ¾-~_. M
~~~~~~~~~~4 O
Ago.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
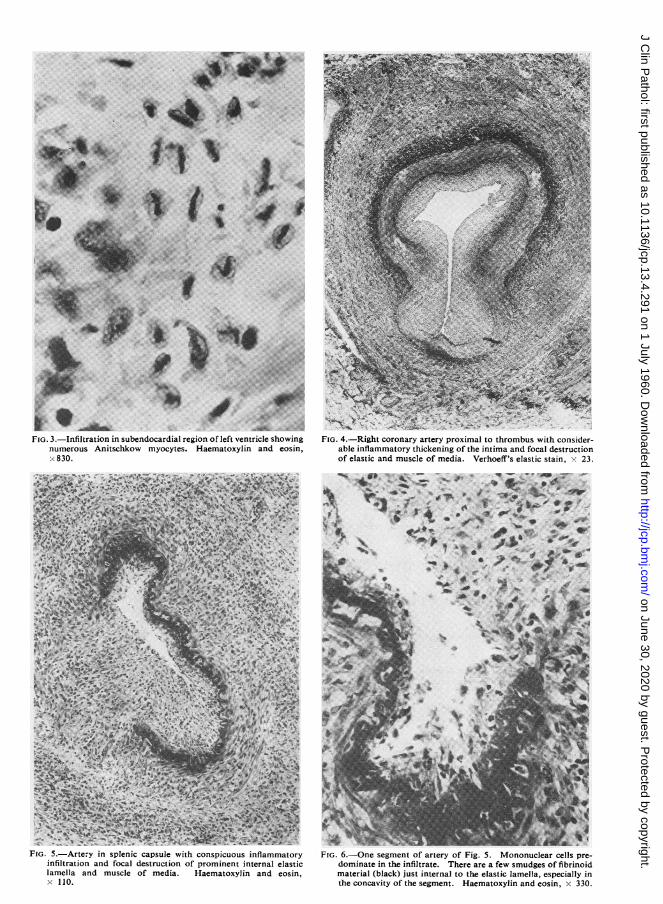
' .' -gFIG. 5.-Artery in splenic capsule with conspicuous inflammatory
infiltration and focal destruction of prominent internal elasticlamella and muscle of media. Haematoxylin and eosin,x 110.
r*¢<~~~~ ~~~~~~~~~~~~~~~~~~~~~~~~~~
FIG. 6.-One segment of artery of Fig. 5. Mononuclear cells pre-dominate in the infiltrate. There are a few smudges of fibrinoidmaterial (black) just internal to the elastic lamella, especially inthe concavity of the segment. Haematoxylin and eosin, x 330.
on June 30, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.13.4.291 on 1 July 1960. D
ownloaded from
T. R. SAVAGE and J. F. SMITH
thickened; pinhead haematomas were also present inthese, one at the root of the tricuspid, one near itsfree edge, and %a third near the free edge of themitral. Themyocardium was firm and greyish brownwith a slightly streaky appearance on the fresh cutsurface in some areas of the left ventricle.
Other Organs.-The kidneys were congested; thelungs slightly congested. The muscle of the pyloricend of the stomach was conspicuously thickened (0.5cm.), but there was no stenosis.
Microscopical Examination.-This was undertakenon tissues from all the cardiac chambers, mitral andtricuspid valves, coronary arteries, liver, spleen,kidneys, alimentary tract, endocrines, several lymph-atic glands, the submandibular salivary gland, bothlungs, cerebellum, pons, basal ganglia, and lefttemporal lobe.There was an extensive inflammatory infiltration
in the heart which was maximal in and around thewalls of the larger coronary arteries, in the endo-cardium of the left auricle (Fig. 2), and at the root ofthe mitral valve but was also conspicuous in patchesin the subendocardial region of the left ventricle andto a less extent in the right auricle and ventricle.The walls of small coronary arteries were in generalspared, but the endothelium of a few veins wasinfiltrated. The mitral valve was infiltrated fromroot to free margin but the tricuspid only at the root.Histiocytes and lymphocytes were very numerous inall sites; polymorphonuclear leucocytes abundant inmost sites, numerous eosinophil leucocytes in only afew sites. In some areas there were scattered fibro-blasts and some delicate, newly formed collagenfibrils. In the subendocardial region of the leftventricle Anitschkow myocytes were abundant (Fig.3) and in several areas some were large withtwisted hyperchromatic nuclei reminiscent of the cellsfound in Aschoff bodies; an occasional histiocytewas seen in mitosis. In the myocardium the infil-trate was perivascular for the most part, buta few small groups of cells were found betweenmuscle fibres. In some areas the connective tissueat the site of infiltration stained poorly and in a fewthere was slight fragmentation, but fibrinoid changewas only seen in one small area in the epicardiumanterior to the interventricular septum. The infiltra-tion was thus somewhat like that of acute rheumatism,but the cellular types were even more pleomorphicthan in that condition.
In the larger coronary arteries the infiltration wasoften associated with partial destruction of the elasticlamellae and of muscle of the media; in some thethickening of the intima was very conspicuous (Fig. 4),but in none was there fibrinoid material in the wall.At the sites of aneurysms there was great focalthinning of the media and recent thrombus in thelumen.A similar arteritis involved one vessel in the splenic
capsule (Figs. 5 and 6) and two in the capsules of thesuprarenals. In the splenic one there was focaldestruction of the internal elastic lamella, patches of
fibrinoid internal to it, and conspicuous cellularthickening of the intima; in the suprarenal vessels theinternal elastic lamellae had a fibrinoid layer closelyapposed to their inner aspect, but appeared to beintact. The adventitia was conspicuously thickened bycellular infiltration, and this encroached in places intothe media.
In the section of the upper lobe of the left lungfocal infiltrations of the walls of large pulmonaryarteries and veins mainly by polymorphonuclearleucocytes and lymphocytes, were associated withintimal intraluminal projections and focal partialdestruction of the elastic of the wall in the arteries.In this and also in the section of the right upper lobechronic inflammation of the walls of a few bronchiwas present. In the kidney there was adventitialinfiltration of an artery in the lower cortex.The only other histological abnormalities were
inflammation of the leptomeninges, of the capsuleand periportal regions of the liver, of the sinuses ofthe lymph glands and around a few small veins inthe thyroid.Reasons for Diagnosis.-Destructive and inflamma-
tory lesions of large branches of the coronary arteriesand of smaller ones in the suprarenal and spleniccapsules were present, the former being accompaniedby aneurysm formation and thrombosis, the lattershowing focal fibrinoid change. These justify adiagnosis of polyarteritis nodosa. The presence ofslighter but definite lesions in pulmonary arteries andveins makes its nosological place uncertain if theclassification of Zeek (1952) is used. This and thesignificance of the myocarditis will be considered inthe discussion. The congenital pyloric hypertrophyis regarded as a coincidental and unrelated finding.
DiscusionIt is convenient to summarize five of the cases
reported of polyarteritis nodosa occurring ininfancy, and to give very brief details of others,in order to illustrate the variety of clinical andpathological manifestations before consideringthe significance of the peculiar features of thepresent case.Krzyszkowski (1899) described a 22-month-old
baby with an indefinite skin rash, slight oedemaof the eyelids and extremities, and pyrexia. Aclinical diagnosis of scarlet fever or syphilis wasmade and death occurred 11 days after the onset.Necropsy showed small thrombosed aneurysms ofthe coronary arteries which were characteristicof polyarteritis nodosa on microscopic examina-tion. Although bronchopneumonia, enteritis, andnephritis were also described, arterial lesions werenot found outside the heart.
Scott and Rotondo (1944) described a 9-month-old female in whom a rash developed after thefifth dose of sulphathiazole (0.5 g. every fourhours was given for pharyngitis with pyrexia).
294
on June 30, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.13.4.291 on 1 July 1960. D
ownloaded from
POLYARTERITIS NODOSA AND CONGENITAL PYLORIC HYPERTROPHY 295
Pyuria and oedema of the face and limbs werelater manifestations, while radiographs indicatedcardiac hypertrophy and an inflammatory processat the base of the right lung. The child diedsuddenly five weeks after the initial symptoms ata time when clinical improvement was thought tobe occurring. At necropsy, thrombosed aneurysmswere present in the coronary arteries of theenlarged heart. Microscopy indicated these to bedue to polyarteritis nodosa, which was also foundin the kidneys, liver, and uterus.
Fager, Bigler, and Simonds (1951) reported a
4-month-old male infant who had an illnessresembling virus pneumonia initially. Pyrexiawas persistent despite treatment with penicillin,streptomycin, aureomycin, and sulphonamides.There was no rash, but in the terminal stages therespiratory and cardiac symptoms and signssuggested a myocarditis. At necropsy thromboseddilated coronary arteries in the enlarged heartwere recanalized and there were infarcts in spleenand kidneys; the left renal artery was thrombosed.Microscopy indicated polyarteritis nodosa in theseorgans and focal myocarditis.
Adelson (1951) described a male infant in whomthe illness began at the age of 15 weeks withpyrexia, slight cough, and moderate cervicalgland enlargement which persisted throughout an
illness of 22 days. Sensitivity to penicillin, whichhad been used initially, was strongly suggestedby the development of a rash following itsadministration on two separate occasions. Thefinal episode of screaming, gasping, and cyanosisin which death occurred was sudden andunexpected. At necropsy there was conspicuous
nodular "beading," narrowed lumina, and aneu-
rysmal dilatation of coronary arteries withthrombosis in the circumflex. The histologyshowed characteristic changes of polyarteritis inthe heart and other organs.
Martelle (1955) did not classify his case of"coronary thrombosis in a 5-month-old infant"as an example of polyarteritis although the clinicaland pathological features were similar to those ofmany recorded examples. The illness started at4 months with fever, vomiting, loose stools, anda dry skin. The baby was treated with penicillinand appeared to recover satisfactorily. Two weekslater there was a two-day episode of irritability,anorexia, and vomiting without pyrexia. The babyrecovered, but when 5 months old he had anotherepisode in which sudden death occurred. Atnecropsy the enlarged heart showed aneurysmaldilatation and thrombosis of all the coronary
arteries. Microscopical examination showed
severe arteritis, involving chiefly the coronaries,but also the aorta and extensive myocarditis andendocarditis. The latter affected the left auriclebut not apparently the valves; and althoughdistinct Aschoff bodies were not present " thegrouping of some of the mononuclear cells wassuggestive, as well as their individual appearance."Areas of muscle necrosis were not thought suffi-cient to account for the myocarditis.Of the other cases recorded it is worth while
noting that marked pulmonary arteritis was afeature in the newborn infant described byElwood (1955) and in the case of Liban, Shamir,and Schorr (1954).Johansmann and Zeek (1954) described a 7-day-
old baby in whom scattered arterial lesions werethought to correspond to that type of polyarteritisnodosa which she refers to as the classical one andin which hypertension may be an important patho-genic factor. This example had also a thrombosedaneurysm of a ductus arteriosus and extensiveinfarction of the right kidney. The latter wasassociated with thrombosis of a branch of therenal artery but not with arteritis.The infant described by Bohman (1954) was
unique in that the illness began after pertussisprophylaxis had been given, but the coursesuggested that a septic process, starting insubcutaneous abscesses, was more important inpathogenesis. In Thinnes' (1924) case the onlysymptom was abdominal pain four hours beforedeath and at necropsy histological evidence ofpolyarteritis was present in the heart and kidneys.The two cases described by Wilmer (1945)occurred in the first month of life; both had asevere illness, one with skin lesions, and extensivelesions were found in the heart, kidneys, uterus,and other viscera. The 9-month female infantreported by Diaz-Rivera and Miller (1946) fellinto the skin, upper respiratory, cardiac group,as did that of Sinclair and Nitsch (1949). In bothof these sulphonamide drugs had been given, inthe latter penicillin also.The case reported by Korb (1957) had a clinical
picture suggestive of nephritis and sepsis, andpolyarteritis was only diagnosed on microscopicexamination; that of Rose (1957) had aneurysmsof branches of the aorta as well as coronaryinvolvement.Munro-Faure (1959) has reported an infant with
marked coronary involvement and reviewed aseries which overlaps extensively with the oneconsidered here. Her paper is called " Necro-tizing Arteritis of the Coronary Vessels." Shehas therefore not included examples of poly-
on June 30, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.13.4.291 on 1 July 1960. D
ownloaded from
T. R. SA VAGE and J. F. SMITH
arteritis in which the coronaries were not involvedand has included two cases in which the authors,Crocker, Sobin, and Thomas (1957), consideredthe diagnosis of polyarteritis nodosa but were notprepared to make it. Before reading her paper we
had noted the frequent involvement of the skinin life and of the coronary arteries at necropsyin this group.
In her somewhat more selected series this pointcomes out clearly, and we would support the con-
tention that there is a group of cases in infants in
which an arteritis is maximal in the coronariesand the illness is frequently characterized byfleeting macular skin eruptions, fever, leucocytosis,conjunctivitis, and pharyngitis, and in which deathoccurs either as a result of progressive heartfailure or suddenly and unexpectedly. Cervicaladenitis and cough were common but not quite so
frequent in this group. If the features of thepyloric hypertrophy are regarded as a separateprocess the present case obviously illustrates many
features of what might be called the upper
respiratory, skin, cardiac group. Of the 18 cases
discussed here, eight fall easily into this group andlesions of the coronaries were present to some
extent in 16 (88%). In the Ill cases of poly-arteritis recently reviewed by Rose (1957), whichincluded mainly adult material, 48°, had coronary
lesions. In none of these infantile cases was therethe prolonged uraemia, hypertension, or peripheralneuritis which characterize an appreciable numberof adult cases.
There remain for consideration the significanceof the myocarditis and valvulitis in our case andthe possible role of hypersensitivity in the patho-genesis. The myocarditis was probably respon-
sible for the episodes of tachycardia during life,and a similar correlation has been noted in otherinfantile cases. Extensive myocarditis, however,is uncommon in this age group, endocarditis was
only noted in the case of Martelle (1955), whilethe valvulitis of the present case was unique.The presence of these features suggests that
our case might be classified as an example ofrheumatic carditis with polyarteritis. Such havebeen described in the past by Neale and Whitfield(1934) and Friedberg and Gross (1934) in childrenand adults but not in infants. The only infantwhich could be so classified in addition to our
own is that of Martelle (1955). Clinical manifes-tations of rheumatism outside the heart and theassociation with a streptococcal infection whichhave been a feature of rheumatic carditis withpolyarteritis were lacking in the infantile cases.
At this age, furthermore, acute rheumatism is
almost unknown.
We do not therefore wish to press this pointnor the interwoven one of the possibility of ahypersensitive reaction in the pathogenesis. Thiswould involve a detailed discussion of present-dayviews on the role of hypersensitivity in poly-arteritis which was originally emphasized soclearly by Rich (1947) and more sharply definedin Zeek's (1952) concept of "hypersensitivityangeiitis." Our case does not fit into this categoryand the concept has not been confirmed in thesurvey of Rose and Spencer (1957). And althoughthe present example yields no clear evidence ofa hypersensitive reaction to any of the drugsgiven, one is left with the impression that themorphological changes are more easily explainedin terms of such a process than in any other way.That antibodies can form in the early months oflife is indicated by the investigations of Sako(1947) and Sako, Treuting, Witt, and Nichamin(1945), and the case of Adelson (1951) suggestsstrongly that anaphylactic hypersensitivity candevelop actively at this period. It is possible thatin these early months there may be considerablevariation in the speed and degree of loss of theimmunological tolerance of foetal life andoccasional unusual manifestations of reaction toantigenic stimulation.
We are indebted to Dr. Eric Frankel and Dr.Kenneth Tallerman for allowing us to describe a caseunder their care. and to Professor Dorothy Russellfor advice about the pathology.
REFERENCES
Adelson, L. (1951). J. Pediat., 39, 346.Bohman, M. (1954). Ac tac pacedijit. (UUppsalu), 43. 374.Crocker, D. W.. Sobin, S., and Thomas, W. C. (1957). Ainer. J. Pat/h
33, 819.De Pascale, A. (1955). M!inervri pedliat. (Toril;o), 7, 1217.Diaz-Risera. R. S., and Miller, A. J. (1946). Anni1. inlteitni. AcIed.. 24,
420.Elwood, J. S. (1955). A.-I.A. Arch. Path., 60, 179.Fager, D. B., Bigler, J. A., and Simonds, J. P. (1951). J. Pediat.,
39, 65.Friedberg, C. K.. and Gross, L. (1934). Arch. interni. Mecl., 54, 170.Johansmann, R. J., and Zeek, P. (1954). Ab. llA. A.rch. Paith.. 58. 207.Korb, G. (1957). Z. ges. inn. MXed., 12, 605.Krzyszkowski, J. (1899). Quoted by Wilmer (1945).Legros, J. (1944). Arch. fran( Pediat., 2. 112.Liban, E., Shamir, Z., and Schorr, S. (1954). Aner. .J. Dis. Chiltl.,
88, 210.Martelle, R. R. (1955). J. Peliat., 46, 322.McCombs, R. P., Patterson, J. F., and McMahon, H. E. (1956).
New Enzgl. J. Aled., 255. 251.Munro-Faure, H. (1959). Pediatrics, 23, 914.Neale, A. V., and Whitfield, A. G. W. (1934). B-it. miied. J., 2, 104.Rich, A. R. (1947). Harver Lect., 1946-1947, 42, 106.Rose, G. A. (1957). Brit. mtied. J., 2, 1148.
and Spencer, H. (1957). Quart. J. Mted. (n.s.), 26, 43.R(iger, I. (1944). Kinidetirztl. P-as., 15, 99.Sako. W. (1947). J. Pediat., 30, 29.
Treuting, W. L., Witt, D. B., and Nichamin. S. J. (1945). J.Amier. nied. Ass., 127, 379.
Scott, E. P., and Rotondo, C. C. (1944). J. Pe/int., 25, 306.Sinclair, W., and Nitsch, E. (1949). Amner. Heat-t J., 38, 898.Thinnes, P. (1924). Franhfurt Z. Path., 30, 104.Wilmer, H. A. (1945). Bull. Johns Hopk. Hosp.. 77, 275.Wright, 1. S. (1948). Quoted by Korb in Vacscular Diseases in Cliflicac
Practice. Year Book Publishers, Chicago.Zeek, P. M. (1952). Amec. J. clin. Path., 22, 777.
296
on June 30, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.13.4.291 on 1 July 1960. D
ownloaded from