south west healthcare warrnambool€¦ · south west healthcare warrnambool ... interpretation. ......
TRANSCRIPT
SOUTH WEST HEALTHCARE
WARRNAMBOOL
ADVANCED LIFE SUPPORT
LEARNING PACKAGE
Prepared by:
J. Brown, ICU
Last revised February, 2010.
C. Joseph, Nursing Education.
2
CONTENTS: Page: Objectives 3-5 Basic Life Support 6-8 Choking and airway obstruction 8-9 Defibrillation in ALS 9-11 Automated External Defibrillators 12 Temporary external pacing 13-16 Medications used in ALS 17-23 Treatment of arrhythmias 23-26 Correcting reversible causes 26 References 27
3
OBJECTIVES: 1. Demonstrate / describe what constitutes effective BLS:
• Assessment of airway
• Breathing
• Circulation / Compressions
• Demonstrate the above on manikin 2. Give the rationale for early defibrillation, early access to the emergency response system and early BLS.
3. Recognises those rhythms that require defibrillation and those that do not. 4. Describe the protocol for the use of a defibrillator in both the manual and Automated External Defibrillator (AED) mode. 5. Give the rationale for the use of and indications for delivering either a single shock or a series of 3 rapid stacked shocks. 6. Demonstrate techniques which provide access to appropriate skin sites for placement / attachment of the defibrillator electrodes and:
• Describe when it might be necessary to dry the skin
• Demonstrate preparation of defibrillator electrodes for attachment to the skin.
• Describe the technique to avoid trapping of air between the electrodes and the skin.
• Attach the electrodes to the skin at appropriate sites in a manner that facilitates safe and effective defibrillation.
4
7. Demonstrate electrode placement on either a manikin which generates an ECG signal, or to a separate ECG signal generator, including:
• Turning on defibrillator / attaching electrode cable to defibrillator.
• The technique for initiating analysis of the ECG signal in the AED mode.
• The technique for charging the defibrillator.
• When AED mode in use, deliver first shock when prompted to do so.
• The delivery of a shock after giving a warning for bystanders to stand clear.
• The provision of further shocks and Basic Life Support (BLS) according to SWH protocol and by prompts from the AED, including the prompt that a non-shockable rhythm is present. The participant should demonstrate preparation of AED, attachment of the electrodes to manikins chest etc. in a two minute time frame. The participant must also demonstrate how to operate the AED in the manual mode (Critical Care and Emergency trained staff only).
8. Demonstrate appropriate responses to perfusing and non-perfusing rhythms on a manikin that generates various rhythms for interpretation. In the case of the manual biphasic defibrillator, the participant must demonstrate use, response to rhythms, select joules, charge, defibrillate and demonstrate use and understanding of all buttons on the defibrillator. 9. Describe the possible complications of external defibrillation. 10. Describe the safety precautions of defibrillation, including the importance of the “stand clear” command.
5
11. Describe the possible problems which may arise during the use of the defibrillator and how to respond to such problems. 12. Demonstrate a maintenance check of and basic fault finding in a defibrillator:
• Checking leads for damage.
• Turning on the defibrillator to check for potential function.
• Checking the presence of paper in the paper drive and that the electronic data collection module is in place.
13. Outline troubleshooting of the defibrillator when there is failure to discharge or failure to defibrillate..
14. State the steps in the ALS algorithm and the points at which medications are appropriate. 15. Choose the most appropriate drug or drugs in light of:
• The point that has been reached in the ALS algorithm.
• The cardiac rhythm.
• The duration of the arrest.
• The patient’s serum electrolyte levels and acid-base status.
• The patient’s response to drugs, which have already been administered.
• The patient’s history and previous medication exposure.
• Identify the need to exclude reversible causes and identify these causes.
16. State the initial dose of the selected drug, different modes of administration including the use of minijets, time to onset of action, likely duration of effect, subsequent doses, maximum doses, side effects and management of side effects.
6
BASIC LIFE SUPPORT
Definition: The preservation and restoration of life by the establishment of and/or maintenance of airway, breathing and circulation and related emergency care.
D - Danger:
• The area should be assessed for any signs of danger for the patient and/or bystanders. Remove the source of danger if possible.
R - Response:
• Check the patient for a response, touch and shout!
• Call for help, call a Code Blue, dial 33, and state patient location.
• Note the time of the event.
A - Airway:
• Check patency of the airway, look inside the airway for any signs of obstruction, clear or suction the airway if required.
• Insert Guedel airway if required, measure from patients ear to lip.
B - Breathing:
• Look, listen and feel for any spontaneous respirations.
• Perform the head tilt/chin lift (not in infants).
• Administer two good breaths with Laerdal bag. Ventilation oxygenates the patient.
• Assist Doctors to intubate the patient if required.
7
C - Circulation:
• Check for a carotid pulse, located at the corner of the mouth and half way down the neck. Do not spend more than 10 seconds trying to locate the pulse.
• For a witnessed or monitored arrest a precordial thump should be administered.
• Attach FR2 automatic defibrillator if on general ward and follow prompts from the machine.
• If in ICU, ED or OR attach the HeartStart XL defibrillator.
• It is important to continue CPR when the patient has no output, as this helps cellular perfusion and the circulation of drugs. Avoid interruptions to CPR, if interruptions occur, for example ALS interventions, 2 minutes of uninterrupted CPR must be performed before performing any further interventions.
• Check for output during CPR by palpating either the carotid or femoral pulse.
• Reassess the patient’s rhythm and for signs of spontaneous output every 2 minutes.
COMPRESSION/VENTILATION RATIOS:
• Adult ratio: 30:2 compressions / ventilations for one or two operators, aiming for a rate of 100 compressions/ minute.
• Paediatric ratio (all ages except newborn): 15:2 compressions / ventilations for one or two operators.
• Newborn ratio (first minutes to hours after birth): 3:1 compressions / ventilations for one or two operators, providing a rate of 120 compressions and 40 – 60 breaths /minute. Note the newborn period is the first minutes to hours after birth.
Compression techniques:
• Compress the centre of the patient’s chest with the heel of both hands. It is now recommended by the Australian Resuscitation Council (ARC) to use both hands for adults and children except in infants and newborns.
8
• The compression should be 1/3 of the depth of the chest for all patients, which is 4-5cm.
• Compressions for infants (<1 year) should be with two fingers.
For further reading refer to the
SWH Resuscitation Policy, accessed through Clinical Guidelines on the intranet.
Or visit the Australian Resuscitation Council (ARC) website at http://www.resus.org.au
_____________________________________________________
MANAGEMENT OF FOREIGN BODY AIRWAY OBSTRUCTION - (CHOKING)
A foreign body airway obstruction (FBAO) is a life threatening emergency. Chest thrusts, back blows or abdominal thrusts are effective for FBAO in conscious adults and children >1 year of age. Some injuries have been reported with the use of abdominal thrusts therefore the ARC no longer recommends the use of lateral chest thrusts. Assess Severity The simplest way to assess the severity of a FBAO is to assess whether the cough is effective or ineffective. Effective Cough (mild obstruction): The victim with an effective cough should be reassured and encouraged to keep coughing to expel the foreign body. Ineffective Cough (severe airway obstruction): Conscious Victim:
• Perform up to 5 sharp back blows with the heel of one hand in the middle of the back between the shoulder blades.
• Check to see if each back blow has cleared the obstruction. An infant may be placed in a head down position prior to giving the back blows.
9
• If the back blows are unsuccessful the rescuer should perform 5 chest thrusts, checking to see if each thrust has relieved the obstruction. To perform chest thrusts identify the same compression point as for CPR and give 5 thrusts. The infant should be placed in a head down supine position. If the obstruction is still not relieved continue alternating 5 back blows with 5 chest thrusts.
Unconscious Victim:
• The finger sweep can be used in the unconscious victim with an airway obstruction if the foreign body is visible. A Code Blue should be activated and CPR commenced immediately if the victim is unconscious and the rescuer is unable to remove the foreign body.
_____________________________________________________
ADVANCED LIFE SUPPORT
Defibrillation in advance cardiac life support: Research has shown that early defibrillation in cardiac arrest for patients presenting with VF and pulseless VT dramatically increases the chance of survival. A direct current passed through the patient’s chest can produce simultaneous depolarisation of myocardial cells leading to organised electrical activity. Research has shown survival decreases by 5.5% per minute without the initiation of defibrillation, BLS and ALS. SWH has Philips HeartStart XL defibrillators, located in ICU, Acute Care, E.D and the Operating Theatre. These can be used in manual and semi-automatic modes. The remainder of the hospital has Philips FR2 automatic defibrillators that may also be operated in manual mode (by Critical Care or Emergency trained SWH staff). All the defibrillators are bi-phasic meaning the electrical energy travels back and forth between the adhesive pads. This reduces the impedence of the chest wall allowing fewer joules to be used.
10
Note: The latest ARC Guidelines (2006) recommend that energy levels for adults should be set at 200J for all shocks, unless relevant clinical data for a specific defibrillator suggests that an alternative energy level provides adequate shock success. It is recommended by Philips that the HeartStart XL and FR2 defibrillators be set for adults at 150J for all shocks, therefore SWH protocol stipulates the use of 150J based on these recommendations.
Procedure for applying defibrillator pads:
• The adhesive pads should be rolled onto the patient’s skin to avoid trapping of air.
• If the patient’s skin is moist then attempt to dry off.
• Do not operate the defibrillator if in contact with water.
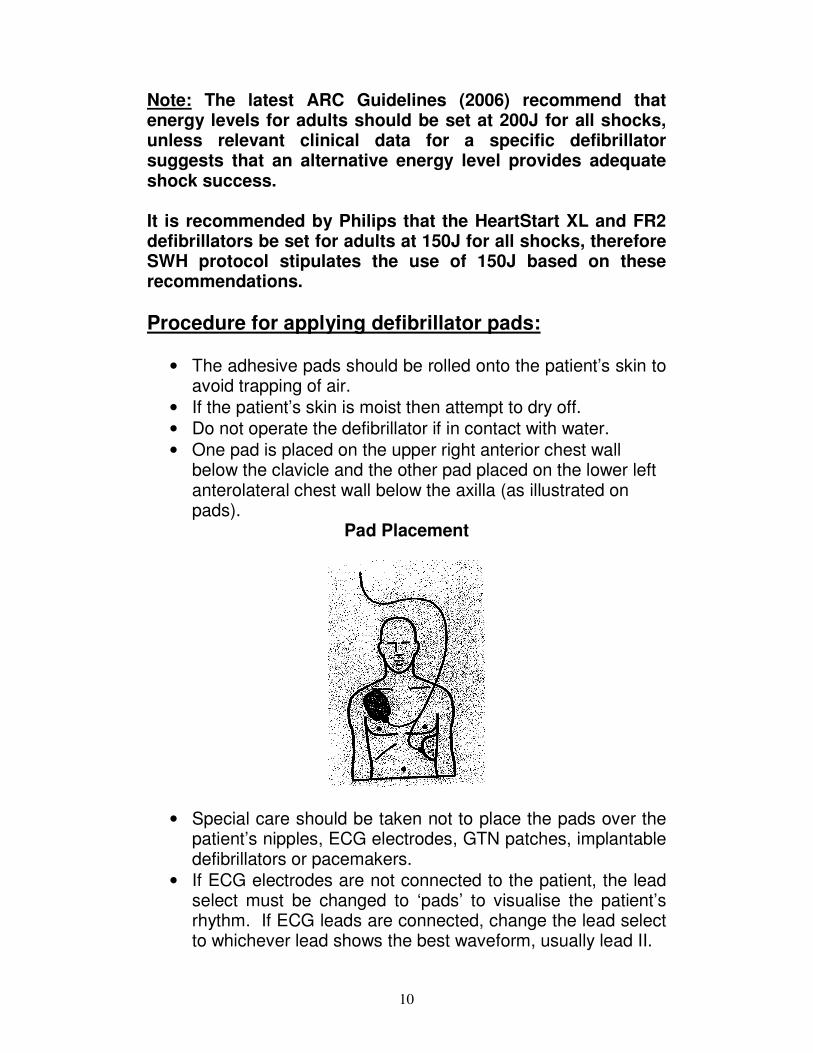
• One pad is placed on the upper right anterior chest wall below the clavicle and the other pad placed on the lower left anterolateral chest wall below the axilla (as illustrated on pads).
Pad Placement
• Special care should be taken not to place the pads over the patient’s nipples, ECG electrodes, GTN patches, implantable defibrillators or pacemakers.
• If ECG electrodes are not connected to the patient, the lead select must be changed to ‘pads’ to visualise the patient’s rhythm. If ECG leads are connected, change the lead select to whichever lead shows the best waveform, usually lead II.
11
• Ensure that the patient is not in contact with any metal fixtures, eg: bed rails.
• Call loudly “stand clear” when shock is to be delivered and visualise that no person is in contact with the patient before delivering the shock.
• Oxygen should be pointed away from the patient to prevent arching.
• The adhesive defibrillator pads can deliver up to 50 shocks before they need to be replaced.
Troubleshooting failure to defibrillate:
?
• Are the pads connected to the defibrillator?
• If some time has lapsed between the charge and defibrillation, then the defibrillator may have dumped the load.
• Is the synchronise button on? The synchronise feature is only used for elective cardioversions.
• Have the joules been selected?
• Is the defibrillator battery flat?
• If all the above is NAD, apply a new set of pads.
12
AUTOMATIC EXTERNAL DEFIBRILLATORS (AED) AED (FR2) defibrillators are located on all ward emergency trolleys throughout the hospital. The AED is programmed to deliver a shock of 150J. Ward staff are educated to attach the AED in an arrest situation as part of the BLS protocol, and defibrillate if instructed to do so by the FR2. Staff who have completed the ALS competency and are critical care trained are able to override the AED and use it in the manual mode to defibrillate patients if they wish to do so. Otherwise the FR2 should remain in the automatic mode. Refer to the manual or a trainer in your ward or department for instructions on how to operate the AED in the manual mode. The HeartStart XL can be operated in both the manual and AED mode. SWH protocol allows ALS trained staff to choose which mode they will use, however the benefits of using the AED make it the preferred mode to use. The benefits are as follows: In AED mode the defibrillator will analyse the rhythm and advise if a shock is to be delivered. Once the defibrillator has delivered a shock or has advised CPR, the pause button should be pressed to enable the defibrillator to count down two minutes of CPR. The patient’s rhythm will automatically be re-analysed once two minutes time has lapsed.

13
TEMPORARY EXTERNAL PACING The HeartStart XL defibrillators are capable of performing temporary external (transcutaneous) pacing.
Indications:
• Patients that may require pacing include bradycardias that do not respond to drug therapy, causing haemodynamic compromise or asystole.
• External pacing may also be required whilst temporary transvenous pacing is being arranged.
Modes:
There are two available modes of pacing; demand and fixed.
• In the demand mode the pacer delivers paced pulses when the patient’s heart rate is lower than the set rate. This mode is selected when the patient has some spontaneous beats, eg: heart blocks or bradycardias.
• The fixed mode allows the pacer to deliver paced pulses at a set rate to be used when the patient has no spontaneous electrical activity. The demand mode is used whenever possible.
14
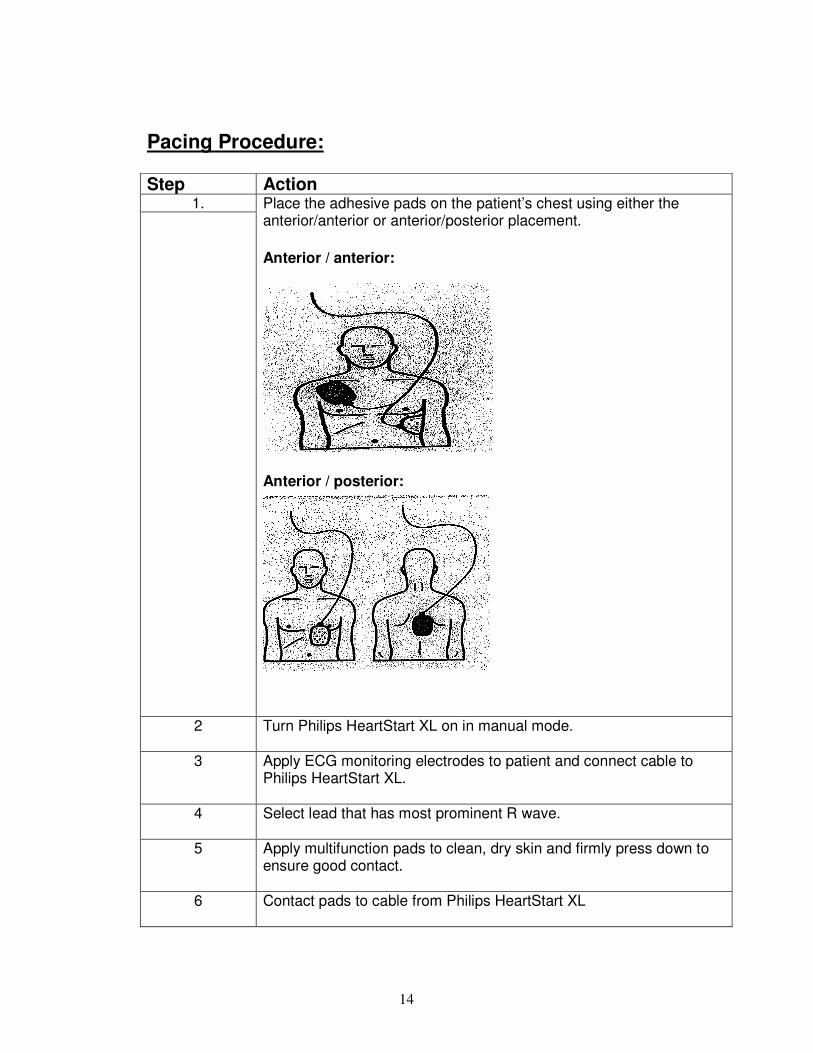
Pacing Procedure: Step Action
1.
Place the adhesive pads on the patient’s chest using either the anterior/anterior or anterior/posterior placement.
Anterior / anterior:
Anterior / posterior:
2 Turn Philips HeartStart XL on in manual mode.
3 Apply ECG monitoring electrodes to patient and connect cable to Philips HeartStart XL.
4 Select lead that has most prominent R wave.
5 Apply multifunction pads to clean, dry skin and firmly press down to ensure good contact.
6 Contact pads to cable from Philips HeartStart XL

15
7 Press “PACER” key to turn pacing mode on
8 Dot markers should appear in the middle of the QRS complexes if the
patient’s intrinsic rate is greater than the pacer rate. This signifies that sensing is occurring.on ECG monitoring (see above diagram of pacing dialogue box). If dots are not present, adjust ECG size (amplitude) or select another lead.
9 Press “MODE” key to change between Demand and Fixed Pacing Mode. Demand Mode is the preferred mode of pacing.
10 Press “RATE” key using arrows to set / adjust pacing rate. The Pacer defaults to a rate of 70 when turned on. Set the rate 10 higher than the patient’s intrinsic rate to check sensing and capture.
11 Press “OUTPUT” key using arrows to set amount of energy delivered to achieve myocardial capture. The output default setting is 30mA, but can be adjusted between 10 – 200mA. The output should be increased until every beat is capturing (this is the pacing threshold). A wide QRS complex will identify capture. Set the output at 10% greater than the pacing threshold. The least amount of mA should be used.
12 Press “Start/Stop” button to commence pacing.
16
Action cont: 13 Observe for commencement of electrical capture and check that
mechanical capture is occurring by palpating patient pulse and ensuring adequate BP.
14 Document all pacing settings, time pacing commenced, patient cardiac rhythm, BP and peripheral pulses on observation chart and in nursing notes. Perform 12 lead ECG.
15 Administer ordered analgesia / sedation to promote patient comfort.
NOTE: Safety precautions: Defibrillation during external pacing: CPR during external pacing: Complications of external pacing
• Do not leave patient unattended whilst temporary transcutaneous cardiac pacing is in progress.
• If required, defibrillation can be initiated whilst in pacing mode.
o There is no need to switch pacing off o Charge defibrillator as normal and deliver the
shock. o The pacer will need to be turned on again after
defibrillation to reinitiate pacing (the previous settings will be restored).
• CPR can be safely performed without electrical risk to the operator providing the following precautions are taken:
o Do not place hands over pacing pads o Wear rubber gloves
• Complications may include micro-shock, skin breakdown, muscle twitching and pain.
17
MEDICATIONS USED IN ADVANCED LIFE SUPPORT
IV access: Administration of medications intravenously is preferable in the event of cardiac arrest. An intravenous cannula must be inserted into a large peripheral vein. If there is no visible peripheral access then the external jugular vein should be considered. Lower limb veins should be avoided due to lack of venous return. Intravenous administration of drugs should be followed by a flush of 30mls of compatible fluid and external cardiac compressions. A normal saline infusion may be commenced to aid in flushing of medications.
Minijets: Minijets of adrenaline, atropine, lignocaine and calcium chloride are available for use at SWH. If you are unfamiliar with the use of minijets please see one of the ALS assessors for further instruction. Expired minijets are available in the education centre for training.
Endotracheal drug administration: Endotracheal administration may be considered if intravenous access cannot be obtained. Adrenaline, atropine and lignocaine can all be administered via the endotracheal route.
Method:
• The ETT must be suctioned prior to administration.
• Insert a clean suction catheter down the ETT and instil the medication via the catheter.
• Administer twice the intravenous dose diluted to 10mls of normal saline or water.
• This is to be followed by at least two vigorous ventilations.
• In the paediatric patient intraosseous administration may also be considered. The same dose is administered as the intravenous dose.
18
Nurse-initiated medications for ALS: Adrenaline, Atropine and Amiodarone are first line drugs that may be administered during a cardiac arrest by nurses at SWH, whom have undertaken the Advanced Life Support education package and been deemed competent.
MEDICATIONS USED IN ADVANCED LIFE SUPPORT:
Adrenaline (Epinephrine) A naturally occurring catecholamine with alpha and beta effects, leading to peripheral vasoconstriction via its alpha-adrenergic action, directing blood to the myocardium and brain.
Indications: • Ventricular Fibrillation / pulseless Ventricular Tachycardia
after initial shocks have failed.
• Asystole, pulseless electrical activity (PEA)
Dose: Initial adult dose is 1mg (1ml of 1:1,000 or 10mls of 1:10,000) This dose may be repeated every three minutes during CPR. An infusion of adrenaline may be required after return of circulation. Adrenaline by infusion should be delivered by a dedicated central line as soon as possible. Adrenaline must not be mixed with sodium bicarbonate.
Adverse effects:
• Tachyarrhythmia’s
• Severe hypertension post resuscitation
• Tissue necrosis.
19
Amiodarone Amiodarone is an antiarrhythmic drug that has effects on sodium, potassium and calcium channels. It also has alpha and beta-adrenergic blocking properties.
Indications: • First line anti-arrhythmic for failed defibrillation of VT/VF.
• Prophylaxis of recurrent VF/VT.
Dose: • Initial bolus dose is 300mg diluted to 20mls of 5% dextrose
and administered over 3 minutes. An additional dose of 150mg may be considered. This may be followed by an infusion of 15mg/kg over 24 hours.
Adverse effects: Hypotension, bradycardia and heart block.
Atropine
A parasympathetic antagonist that blocks the action of the vagus nerve on the heart.
Indications: • Bradycardia leading to haemodynamic compromise
• Asystole.
Dose: Unconscious patients: 1.0 mg bolus that may be repeated every 3-5 mins, up to a total of 3mg. Conscious patients: 0.6mg bolus that may be repeated every 3-5 mins, up to a total of 3mg.
Adverse effects: Tachycardia, excitement, delirium, urinary retention, dilated pupils, hyperthermia in large doses. __________________________________________________
20
MEDICATIONS THAT MAY BE USED IN ADVANCED LIFE SUPPORT BY ORDER OF A MEDICAL OFFICER:
Lignocaine An anti-arrhythmic drug acting as a sodium channel blocker.
Indications: • Second line anti-arrhythmic for failed defibrillation of VT/VF.
• Also used as a prophylactic for recurrent VT/VF.
Dose: 1mg/kg bolus initially. An additional dose of 0.5mg/kg may be considered. A lignocaine infusion may be considered once there is a return of spontaneous circulation.
Adverse effects: Slurred speech, altered consciousness, muscle twitching, seizures, bradycardia, hypotension, heart block and asystole.
Isoprenaline A beta sympathomimetic agonist, with positive inotropic and chronotropic actions.
Indications: Bradycardias not responding to atropine.
Dose: Initial dose is 20mcg, which may be repeated every two minutes until adequate perfusion is achieved. To prepare isuprel dilute 200mcg/ml into 10mls of Normal Saline so that each ml contains 20mcg.
Adverse Effects: Tachycardia, hyper/hypotension, angina, nausea, headaches and flushing.
21
Adenosine Suppresses the conduction through the atrioventricular node, interrupting re-entry tachycardia.
Indications: SVT causing haemodynamic compromise (must be administered quickly as it has a short half life).
Dose: 1st dose 3.0mg, 2nd dose 6.0mg, and 3rd dose 12.0mg.
Adverse effects: Flushing, dyspnoea, chest pain and AV blocks.
Potassium Potassium is an electrolyte essential for membrane stability. Hypokalaemia can lead to ventricular arrhythmias, especially when associated with hypomagnesaemia and digoxin therapy.
Indications: Persistent ventricular arrhythmias especially when associated with documented hypokalaemia.
Dose: Bolus of 5mmol of potassium chloride.
Adverse effects: Hyperkalaemia may lead to bradycardia, hypotension and possibly asystole, extravasation and tissue necrosis.
Magnesium Magnesium is an electrolyte essential for membrane stability. Hypomagnesaemia can lead to myocardial hyperexcitability particularly in the presence of hypokalaemia and digoxin therapy.
Indications: • Torsades de pointes,
• Cardiac arrest associated with digoxin toxicity,
• Failure to revert VF/VT,
• Documented hypokalaemia,
• Documented hypomagnesaemia.
22
Dose: 5mmol bolus, which may be repeated once. This may be followed by an infusion of 20mmol over 5 hours.
Adverse effects: • Excessive use may lead to muscle weakness and respiratory
failure.
• Hypotension, bradycardia, and flushing.
Calcium Calcium is essential for normal muscle activity and nerve conduction. It increases myocardial nerve excitability and contractility and increases peripheral resistance.
Indications: Hyperkalaemia, hypocalcaemia, overdose of calcium-channel blocking agents.
Dose: 5-10mls of 10% calcium chloride given as a bolus.
Adverse effects: Possible increase in myocardial and cerebral injury by mediating cell death, tissue necrosis and extravasation.
Sodium Bicarbonate Alkalising solution.
Indications: • Hyperkalaemia,
• Treatment of documented metabolic acidosis,
• Overdose with tricyclic antidepressants, and
• Prolonged arrest. Early efficient CPR and adequate ventilation usually negates the need for sodium bicarbonate.
Dose: 1mmol/kg over 2-3 minutes. This may be repeated if required, and as guided by arterial blood gases.
23
Adverse Effects:
• Due to the risk of alkalosis, hyperosmolality and hypernatraemia, sodium bicarbonate is not part of initial routine therapy.
• Intracellular acidosis may develop or worsen,
• Sodium bicarbonate and adrenaline or calcium when mixed together may inactivate each other, precipitate and block the IV line.
____________________________________________________
TREATMENT OF ARRHYTHMIAS
For further reading refer to the SWH Resuscitation Policy and the ARC Guidelines, accessed at
www.resus.org.au
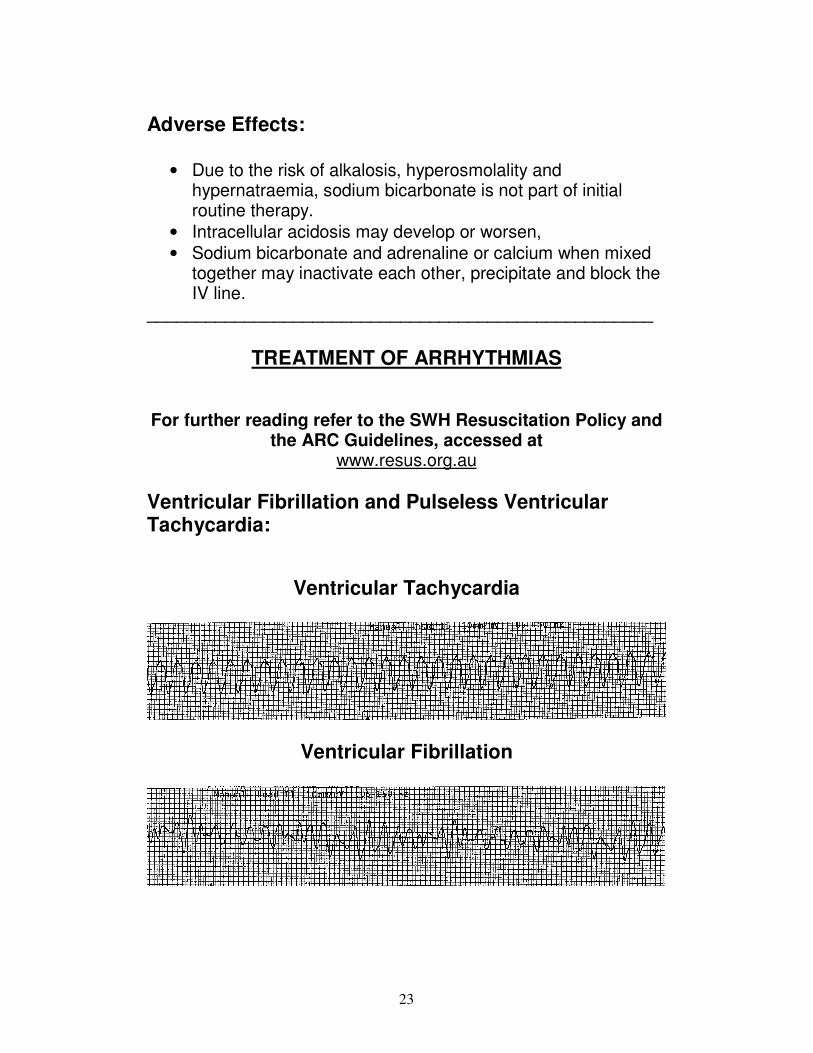
Ventricular Fibrillation and Pulseless Ventricular Tachycardia:
Ventricular Tachycardia
Ventricular Fibrillation

24
For pulseless VT and VF it is advised that only 1 shock of 150J is delivered. If the arrest (VT/VF) has been witnessed by a rescuer then 3 stacked shocks of 150J should be administered. The rhythm should be quickly checked between the stacked shocks to ensure the patient is still in a shockable rhythm.
• After defibrillation immediately perform 2 minutes of CPR.
• During CPR consider the administration of adrenaline.
• Administer adrenaline 1mg followed by at least 2 minutes of CPR.
• Check patient’s rhythm; if the patient remains in a shockable rhythm defibrillation is repeated as a single shock (150J) and followed by adrenaline and CPR. Further doses of 1mg of adrenaline may be repeated every 3 minutes, until return of a spontaneous rhythm.
• Amiodarone may also be administered after defibrillation, if adrenaline and CPR have failed.
• Correct reversible causes.
• Consider inducing hypothermia following VF arrest; refer SWH Hypothermic Therapy following Cardiac Arrest Policy.
Torsades de Pointes
• First line treatment for Torsades is Magnesium.
• Administer Magnesium 5mmol, followed by 2 minutes of CPR if the patient is pulseless. Magnesium 5mmol may be repeated once, followed by an infusion of 20mmol over 5 hours.
• Defibrillation (1 single shock of150J) may be considered if magnesium fails to revert the patient and the patient is pulseless.
• Continue CPR until the return of a spontaneous rhythm.
• Correct reversible causes.
25
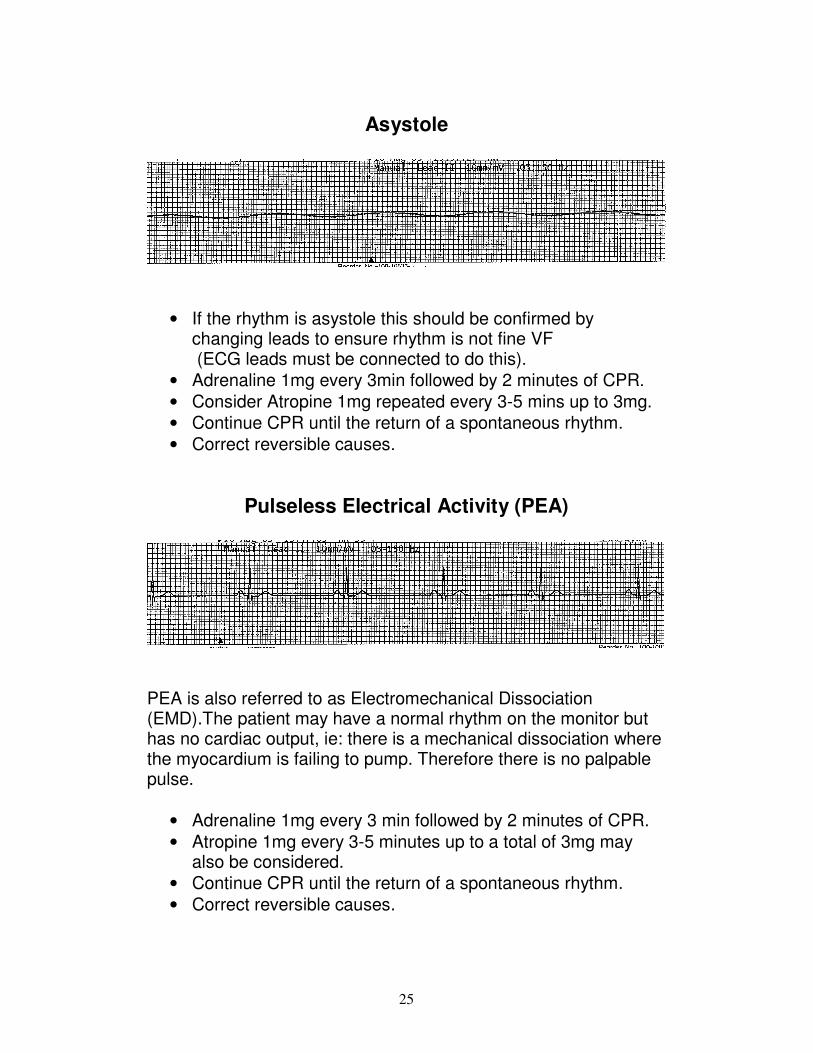
Asystole
• If the rhythm is asystole this should be confirmed by changing leads to ensure rhythm is not fine VF (ECG leads must be connected to do this).
• Adrenaline 1mg every 3min followed by 2 minutes of CPR.
• Consider Atropine 1mg repeated every 3-5 mins up to 3mg.
• Continue CPR until the return of a spontaneous rhythm.
• Correct reversible causes.
Pulseless Electrical Activity (PEA)
PEA is also referred to as Electromechanical Dissociation (EMD).The patient may have a normal rhythm on the monitor but has no cardiac output, ie: there is a mechanical dissociation where the myocardium is failing to pump. Therefore there is no palpable pulse.
• Adrenaline 1mg every 3 min followed by 2 minutes of CPR.
• Atropine 1mg every 3-5 minutes up to a total of 3mg may also be considered.
• Continue CPR until the return of a spontaneous rhythm.
• Correct reversible causes.
26
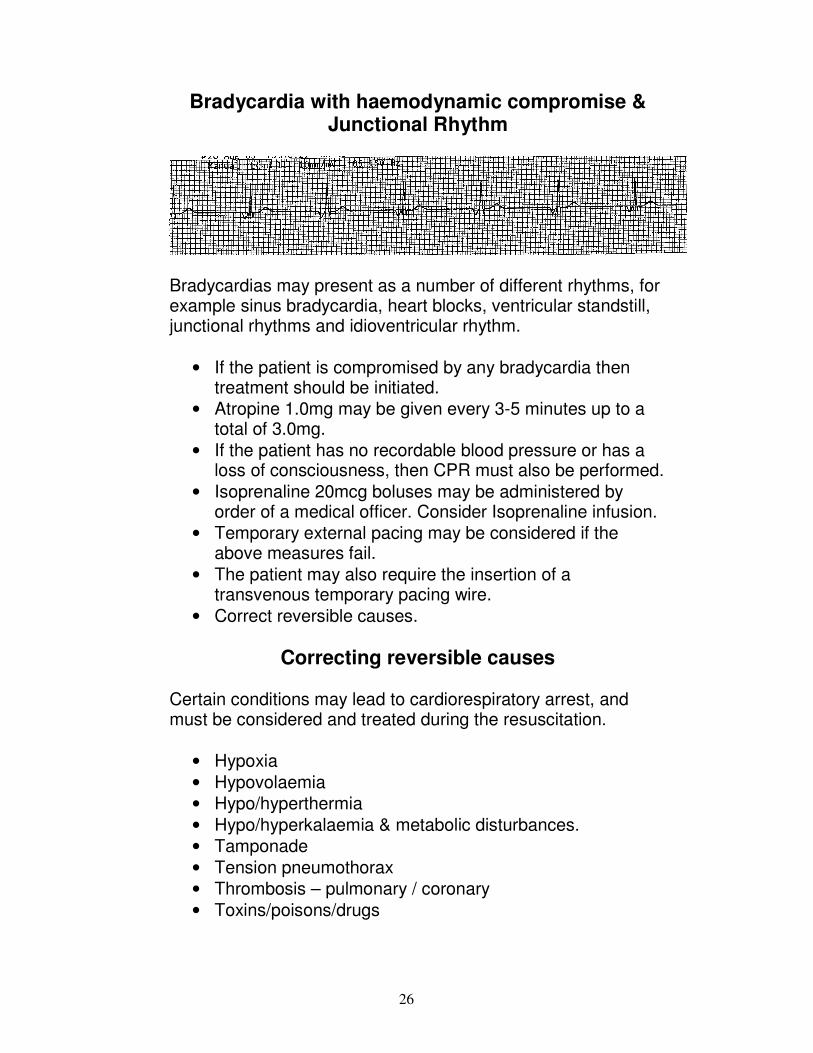
Bradycardia with haemodynamic compromise & Junctional Rhythm
Bradycardias may present as a number of different rhythms, for example sinus bradycardia, heart blocks, ventricular standstill, junctional rhythms and idioventricular rhythm.
• If the patient is compromised by any bradycardia then treatment should be initiated.
• Atropine 1.0mg may be given every 3-5 minutes up to a total of 3.0mg.
• If the patient has no recordable blood pressure or has a loss of consciousness, then CPR must also be performed.
• Isoprenaline 20mcg boluses may be administered by order of a medical officer. Consider Isoprenaline infusion.
• Temporary external pacing may be considered if the above measures fail.
• The patient may also require the insertion of a transvenous temporary pacing wire.
• Correct reversible causes.
Correcting reversible causes Certain conditions may lead to cardiorespiratory arrest, and must be considered and treated during the resuscitation.
• Hypoxia
• Hypovolaemia
• Hypo/hyperthermia
• Hypo/hyperkalaemia & metabolic disturbances.
• Tamponade
• Tension pneumothorax
• Thrombosis – pulmonary / coronary
• Toxins/poisons/drugs
27
REFERENCES Advanced Life Support Revision and Update Packages, (2003). The Royal Melbourne Hospital. Australian Resuscitation Council Guidelines (2006). Drug Protocols. (2003). Cardiology Department, The Royal Melbourne Hospital. Heartstream AED’s Technical Reference Manual, Philips Medical Systems. Heartstart XL Technical Reference Manual, Philips Medical Systems. Intensive Care Advanced Life Support Competencies Learning Package. (2000). St. Vincent’s Hospital, Melbourne. International Liaison Committee on Resuscitation. (2005). Part 4: Advanced life support. Resuscitation, 67, 213-247. SWH Advanced Life Support Competency Assessment Education Package. (2004). SWH Temporary Transcutaneous Pacing Protocol. (2008).