the monocyte monolayer assay (mma) · the monocyte monolayer assay (mma): an adjunct to...
TRANSCRIPT
Ghislain Noumsi MD,SBB(ASCP)CM
Molecular ImmunoHematologist
Scientific Support Services
LifeShare Blood Centers
Shreveport, LA
The Monocyte Monolayer Assay (MMA):
An Adjunct to Compatibility Testing
Objectives
Review the mechanism of RBC destruction
by alloantibody
Describe the MMA technique
Analyze the MMA impact as secondary
crossmatch method for patients with RBC
alloantibody(ies)
Blood bank response
to blood request
Request and specimen
received
Initial
investigation
Interpretation and
additional test
Crossmatch
Blood delivered
Patient transfused
No reaction (hemolysis)

Sometimes
things are more
complicated!!!
Any decision can have a direct impact on
the patient prognosis
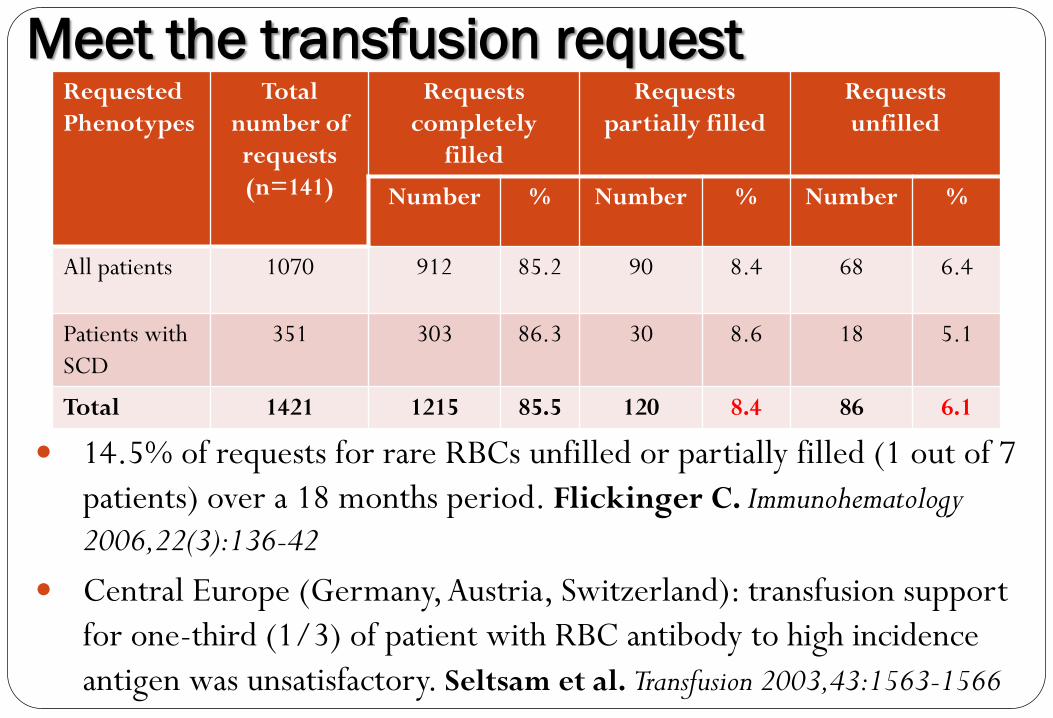
Meet the transfusion request Requested
Phenotypes
Total
number of
requests
(n=141)
Requests
completely
filled
Requests
partially filled
Requests
unfilled
Number % Number % Number %
All patients 1070 912 85.2 90 8.4 68 6.4
Patients with
SCD
351 303 86.3 30 8.6 18 5.1
Total 1421 1215 85.5 120 8.4 86 6.1
14.5% of requests for rare RBCs unfilled or partially filled (1 out of 7
patients) over a 18 months period. Flickinger C. Immunohematology
2006,22(3):136-42
Central Europe (Germany, Austria, Switzerland): transfusion support
for one-third (1/3) of patient with RBC antibody to high incidence
antigen was unsatisfactory. Seltsam et al. Transfusion 2003,43:1563-1566
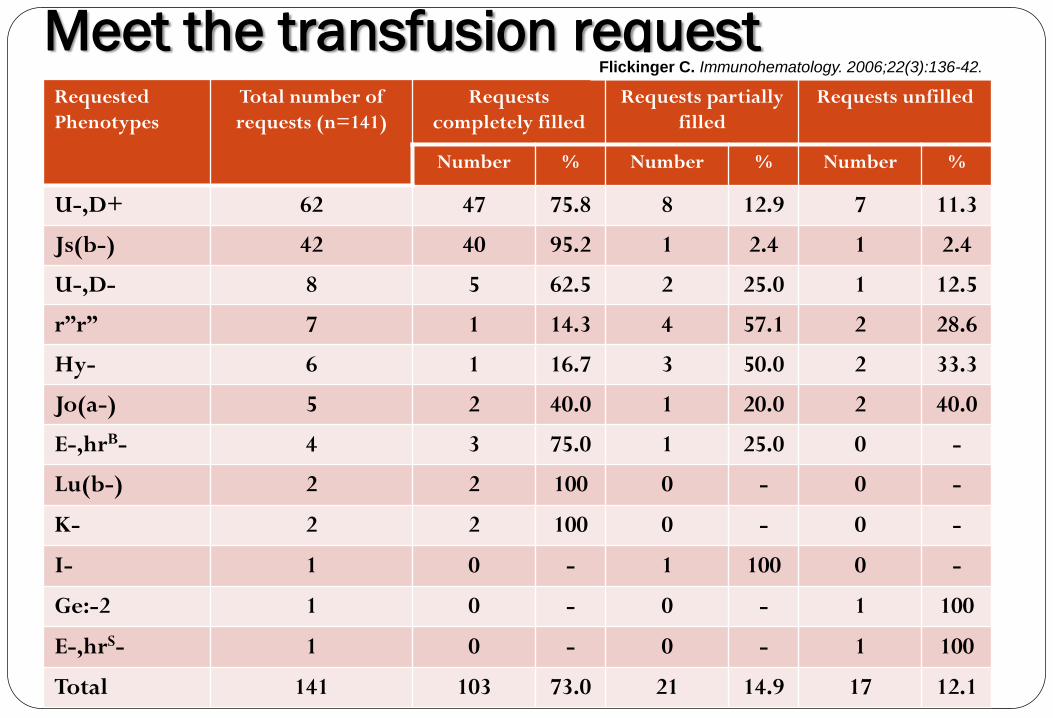
Meet the transfusion request Requested
Phenotypes
Total number of
requests (n=141)
Requests
completely filled
Requests partially
filled
Requests unfilled
Number % Number % Number %
U-,D+ 62 47 75.8 8 12.9 7 11.3
Js(b-) 42 40 95.2 1 2.4 1 2.4
U-,D- 8 5 62.5 2 25.0 1 12.5
r”r” 7 1 14.3 4 57.1 2 28.6
Hy- 6 1 16.7 3 50.0 2 33.3
Jo(a-) 5 2 40.0 1 20.0 2 40.0
E-,hrB- 4 3 75.0 1 25.0 0 -
Lu(b-) 2 2 100 0 - 0 -
K- 2 2 100 0 - 0 -
I- 1 0 - 1 100 0 -
Ge:-2 1 0 - 0 - 1 100
E-,hrS- 1 0 - 0 - 1 100
Total 141 103 73.0 21 14.9 17 12.1
Flickinger C. Immunohematology. 2006;22(3):136-42.
What is the clinical significance of my
antibody(ies)?
“A clinically significant RBC antibody is defined as an
antibody that is frequently associated with HDFN,
with hemolytic transfusion reactions, or with a
notable decrease in the survival of transfused
RBCs”. AABB Technical Manual. 16th Ed. P466
In vivo: RBCs are considered incompatible if their
survival is curtailed by the presence of clinically
significant alloantibody
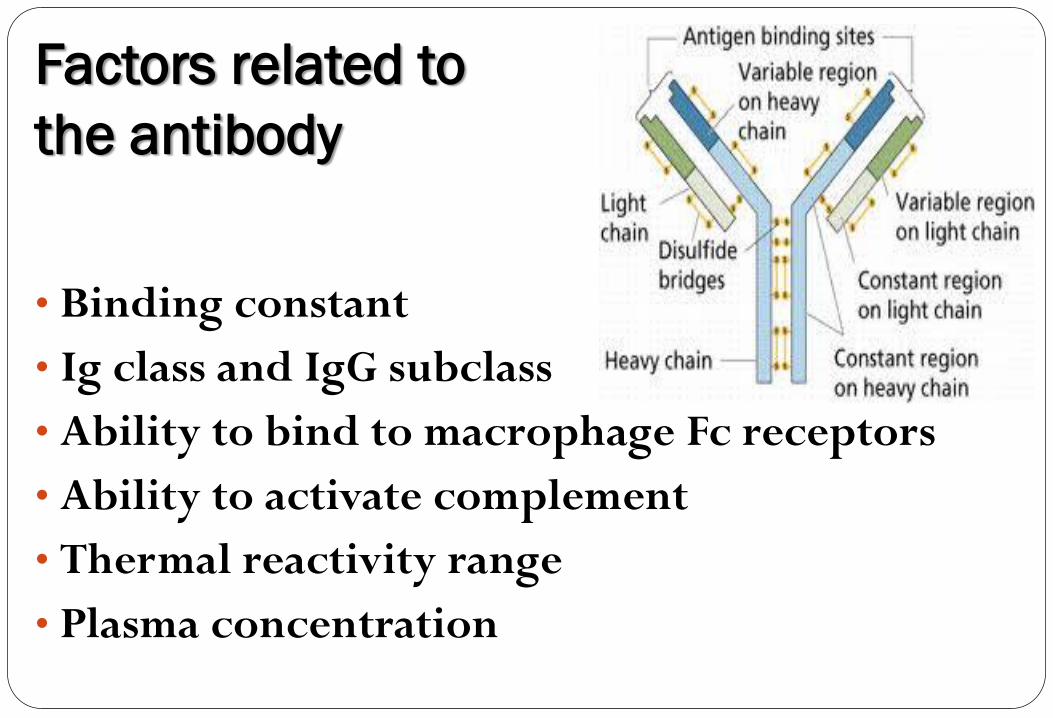
Factors related to
the antibody
• Binding constant
• Ig class and IgG subclass
• Ability to bind to macrophage Fc receptors
• Ability to activate complement
• Thermal reactivity range
• Plasma concentration

Factors related to the
antigen
• Antigenic determinant “epitope”
• Distribution in the body
• Abudance of sites on the red cell
• Appearance on the fetus RBC and placenta (in
case of evaluation of risk of HDFN)
• Association with complement activation
• Other: antigen expression and modification
during storage; number of RBC transfused…etc
Factors affecting the antigen-antibody
bond formation
Spatial complementarity between antigen
and antibody: “Lock and Key” concept
Weak non-specific intermolecular forces
including: electrostatic charges (ionic
groups), hydrogen bonds, hydrophobic
(non-polar) bonds, Van der Waals forces
The equilibrium (association) constant of
the Ag-Ab formation
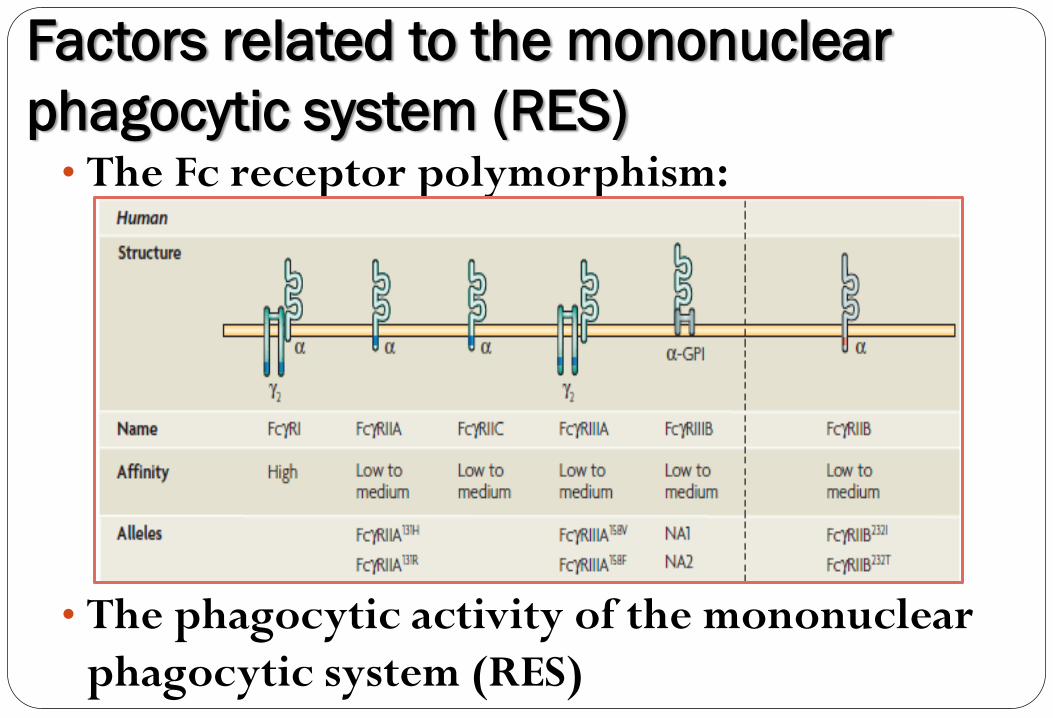
Factors related to the mononuclear
phagocytic system (RES) • The Fc receptor polymorphism:
• The phagocytic activity of the mononuclear
phagocytic system (RES)
Where do we go
from here ?
Do we just STOP ?
One element missing in
the above pathogenesis
process can result in normal
survival of antigen positive RBCs !!!
The Monocyte Monolayer Assay (MMA)
In vitro assay
Predict the outcome of transfused
antigen positive RBCs to patients
with corresponding antibody
Predict the risk of HDFN in
maternal alloimmunization with
feto-maternal incompatibility
Early development
• Stevens JO, Braley JF, Schanfield MS. Detection
of clinically significant IgG antibodies by an in vitro
human peritoneal macrophage phagocytosis assay. Transfusion
1976; 16:523
• Arndt PA, Garratty G. A retrospective analysis of
the value of monocyte monolayer assay results for
predicting the clinical significance of blood group
alloantibodies. Transfusion 2004;44:1273-81
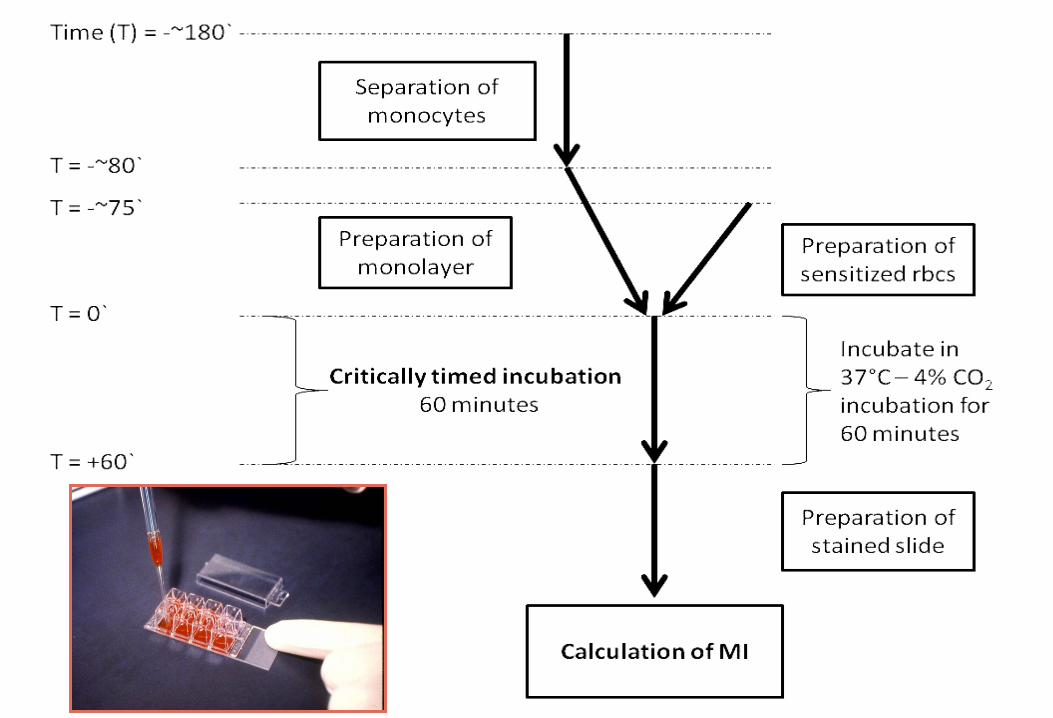
MMA
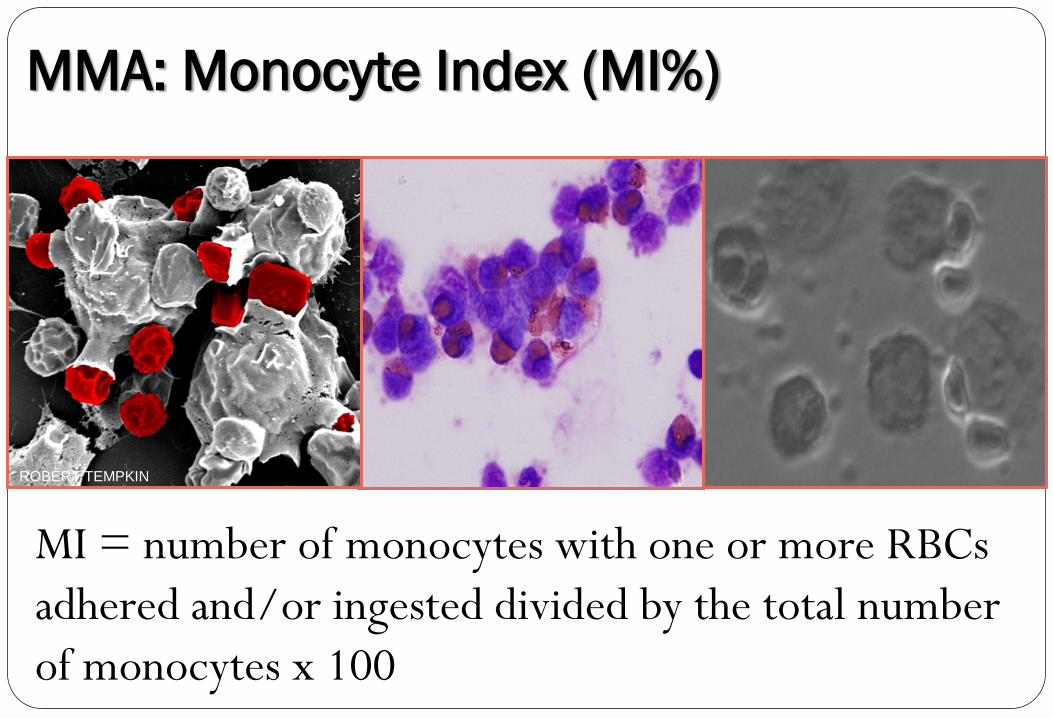
MMA: Monocyte Index (MI%)
MI = number of monocytes with one or more RBCs
adhered and/or ingested divided by the total number
of monocytes x 100
ROBERT TEMPKIN
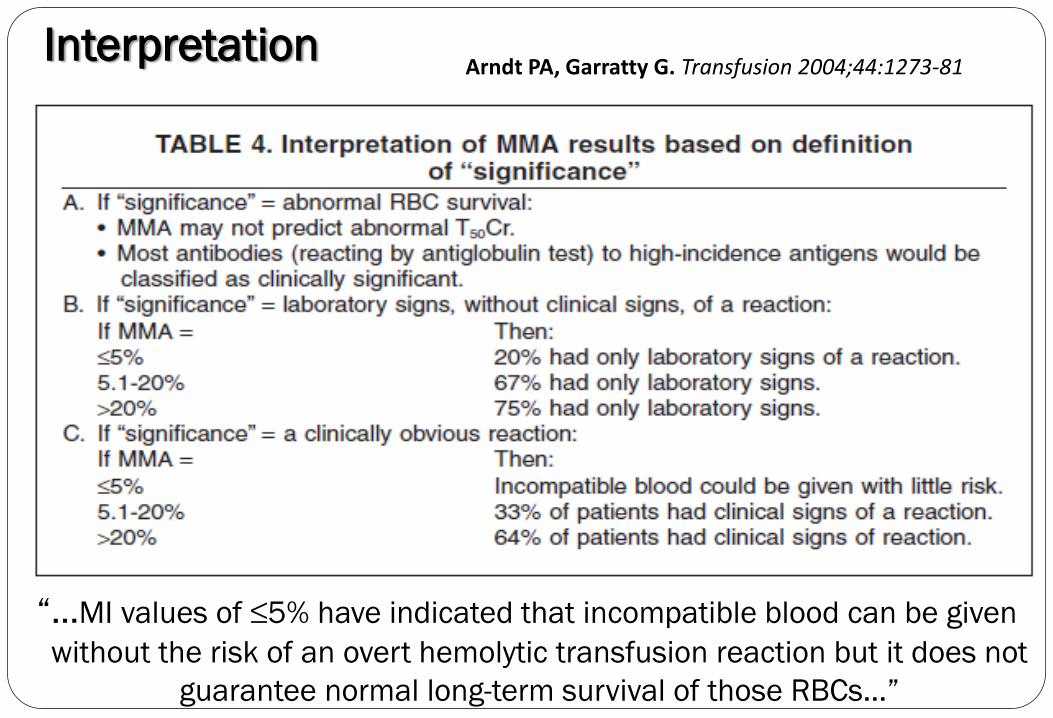
Interpretation
“…MI values of ≤5% have indicated that incompatible blood can be given
without the risk of an overt hemolytic transfusion reaction but it does not
guarantee normal long-term survival of those RBCs…”
Arndt PA, Garratty G. Transfusion 2004;44:1273-81
Can MMA be used as a secondary
crossmatch technique for patients with
unusual antibodies presentation ?
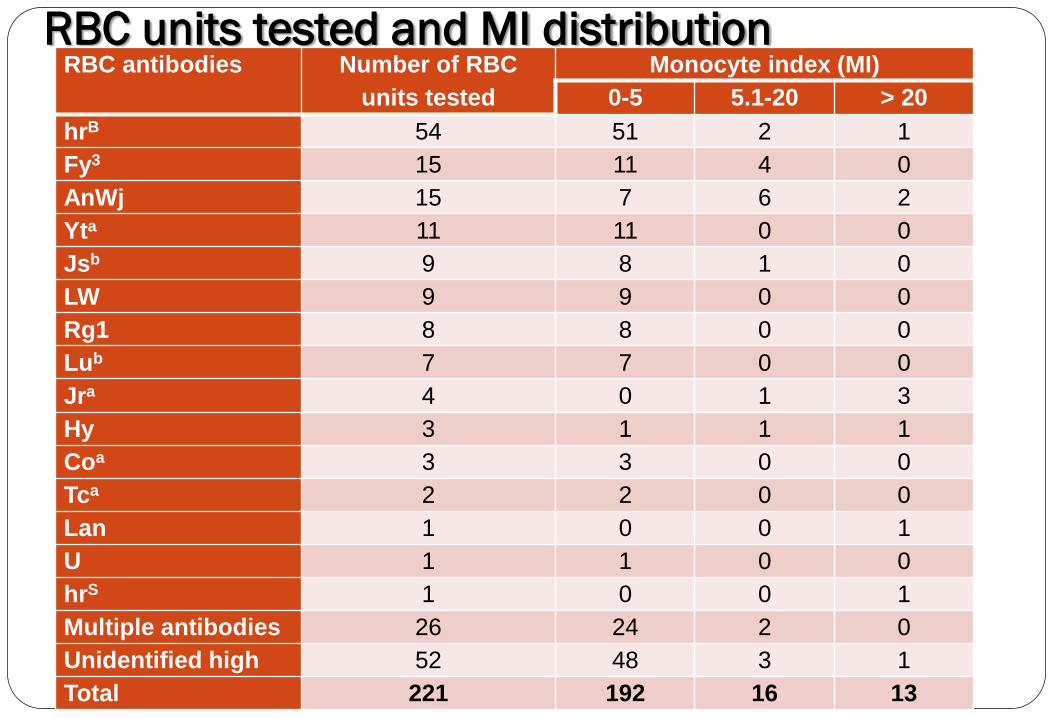
RBC units tested and MI distribution RBC antibodies Number of RBC
units tested
Monocyte index (MI)
0-5 5.1-20 > 20
hrB 54 51 2 1
Fy3 15 11 4 0
AnWj 15 7 6 2
Yta 11 11 0 0
Jsb 9 8 1 0
LW 9 9 0 0
Rg1 8 8 0 0
Lub 7 7 0 0
Jra 4 0 1 3
Hy 3 1 1 1
Coa 3 3 0 0
Tca 2 2 0 0
Lan 1 0 0 1
U 1 1 0 0
hrS 1 0 0 1
Multiple antibodies 26 24 2 0
Unidentified high 52 48 3 1
Total 221 192 16 13
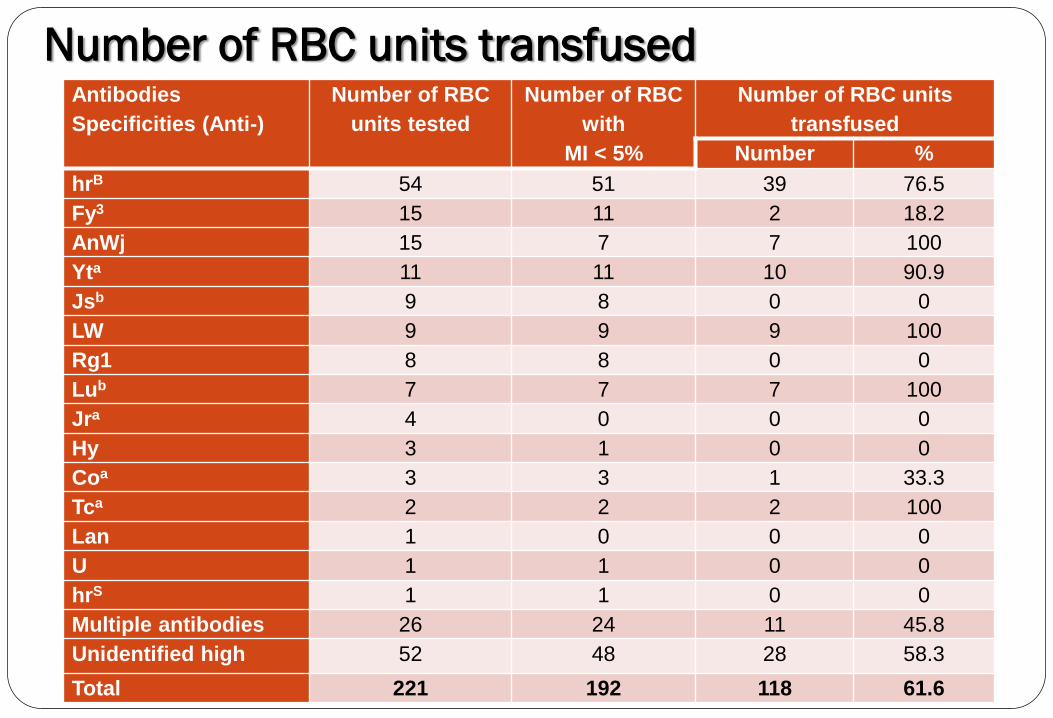
Number of RBC units transfused Antibodies
Specificities (Anti-)
Number of RBC
units tested
Number of RBC
with
MI < 5%
Number of RBC units
transfused
Number %
hrB 54 51 39 76.5
Fy3 15 11 2 18.2
AnWj 15 7 7 100
Yta 11 11 10 90.9
Jsb 9 8 0 0
LW 9 9 9 100
Rg1 8 8 0 0
Lub 7 7 7 100
Jra 4 0 0 0
Hy 3 1 0 0
Coa 3 3 1 33.3
Tca 2 2 2 100
Lan 1 0 0 0
U 1 1 0 0
hrS 1 1 0 0
Multiple antibodies 26 24 11 45.8
Unidentified high 52 48 28 58.3
Total 221 192 118 61.6
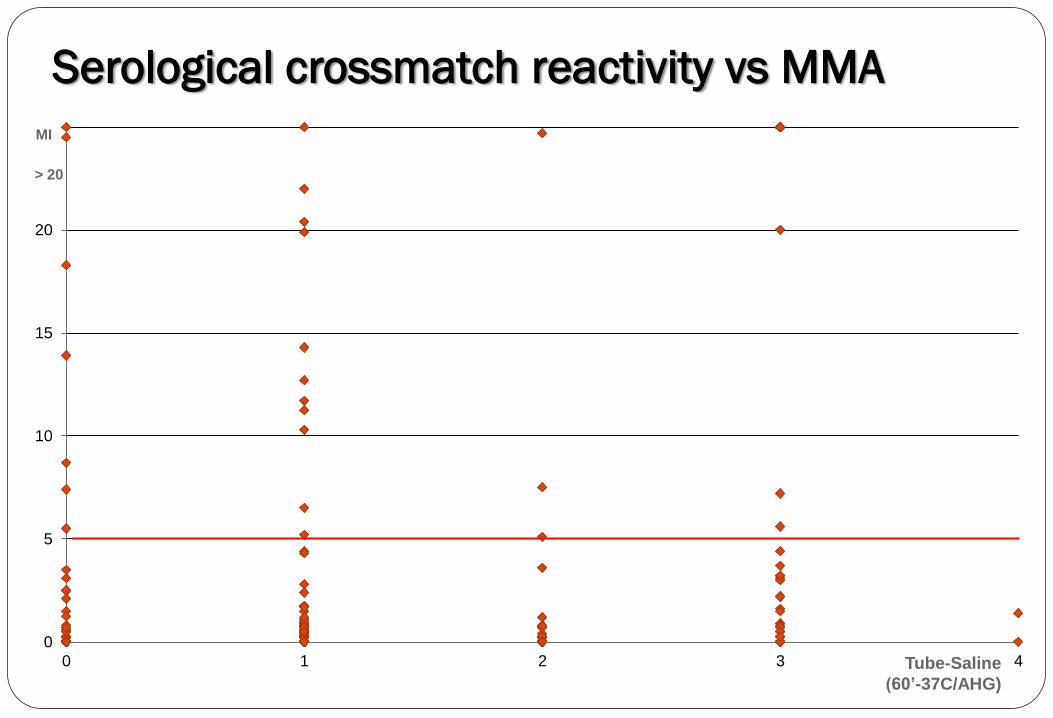
> 20
0
5
10
15
20
25
0 1 2 3 4
MI
Tube-Saline
(60’-37C/AHG)
Serological crossmatch reactivity vs MMA
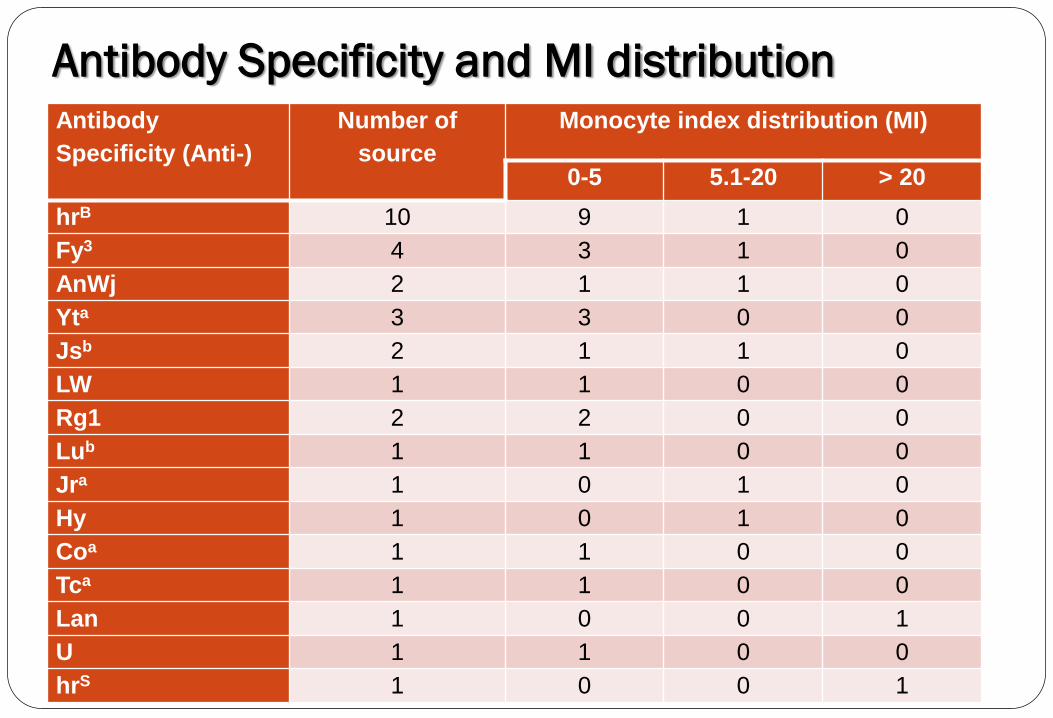
Antibody Specificity and MI distribution Antibody
Specificity (Anti-)
Number of
source
Monocyte index distribution (MI)
0-5 5.1-20 > 20
hrB 10 9 1 0
Fy3 4 3 1 0
AnWj 2 1 1 0
Yta 3 3 0 0
Jsb 2 1 1 0
LW 1 1 0 0
Rg1 2 2 0 0
Lub 1 1 0 0
Jra 1 0 1 0
Hy 1 0 1 0
Coa 1 1 0 0
Tca 1 1 0 0
Lan 1 0 0 1
U 1 1 0 0
hrS 1 0 0 1

PREDICTING THE CLINICAL SIGNIFICANCE OF 51 RBCs ALLOANTIBODIES USING MONOCYTE
MONOLAYER ASSAY (MMA): A 5 YEAR REVIEW NOUMSI GT, BILLINGSLEY K, MOULDS JM, MOULDS JJ
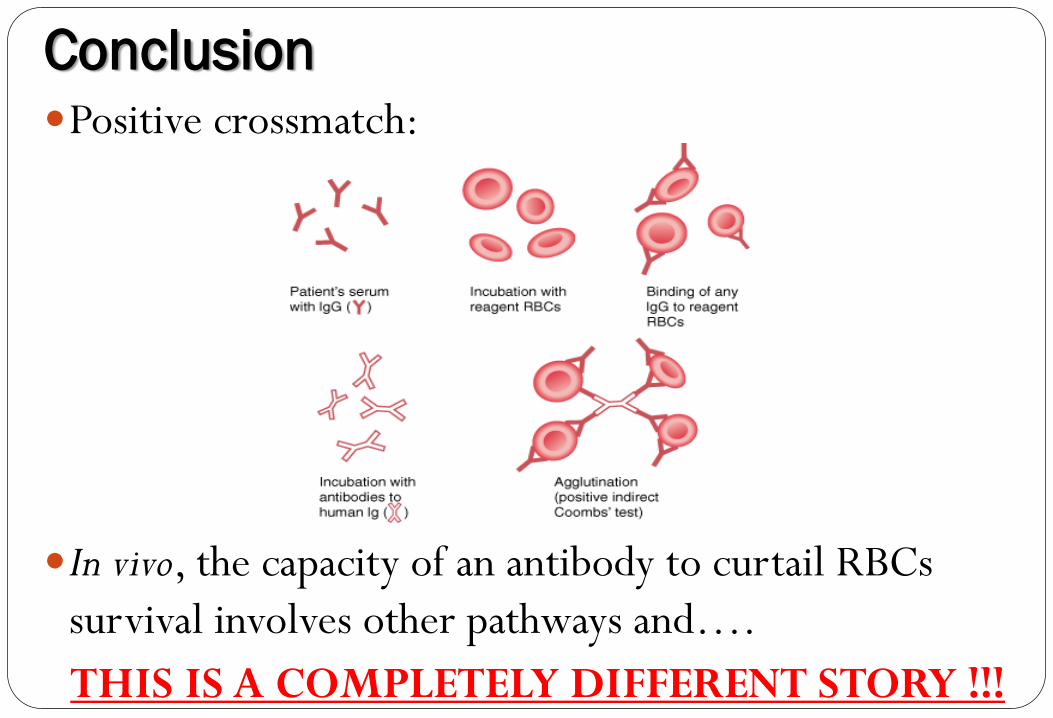
Conclusion Positive crossmatch:
In vivo, the capacity of an antibody to curtail RBCs
survival involves other pathways and….
THIS IS A COMPLETELY DIFFERENT STORY !!!
When all RBCs
seems to be
crossmatch
incompatible
think MMA
you may be
SURPRISED !!!

Thank you !!!