the use of medical expulsion therapy for distal ureteral calculi heidi roloson pa-s lock haven...
TRANSCRIPT

The use of Medical The use of Medical Expulsion Therapy for distal Expulsion Therapy for distal ureteral calculi ureteral calculi
Heidi Roloson PA-SLock Haven University

PICOPICOIn patients over 18 suffering from
ureteral calculi of 10 mm or less, is medical expulsion therapy with alpha-antagonist plus routine pain management superior to routine pain management alone in decreasing symptom duration, time to stone expulsion and increasing the stone passage rate.

Ureteral calculiUreteral calculi
Lifetime prevalence is approximately 7-12% in Americans◦Recurrence probability of 50% in 5
yearsMales>females3rd and 4th decade of lifeHealth care costs from 1994-2000
◦Over $2.1 billionPain, risk of invasive procedures,
lost days at work

Ureteral CalculiUreteral Calculi
Result of metabolic, environmental and nutritional mechanisms◦Occur when normally soluble material
supersaturates the urine resulting in the formation of crystals
◦Calcium, struvite, uric acid and cystine

Current TreatmentCurrent TreatmentWatchful waiting for spontaneous
expulsion along with analgesics for pain control for calculi <5mm
Dependent on the size and location of the stone◦Distal ureteral stones <5 mm: 71%-100%◦Distal ureteral stones 5-10mm: 25%-46%
Can take up to 40 daysComplications: urinary infection,
hydronephrosis, repeat colic events
Current Current Treatment Treatment
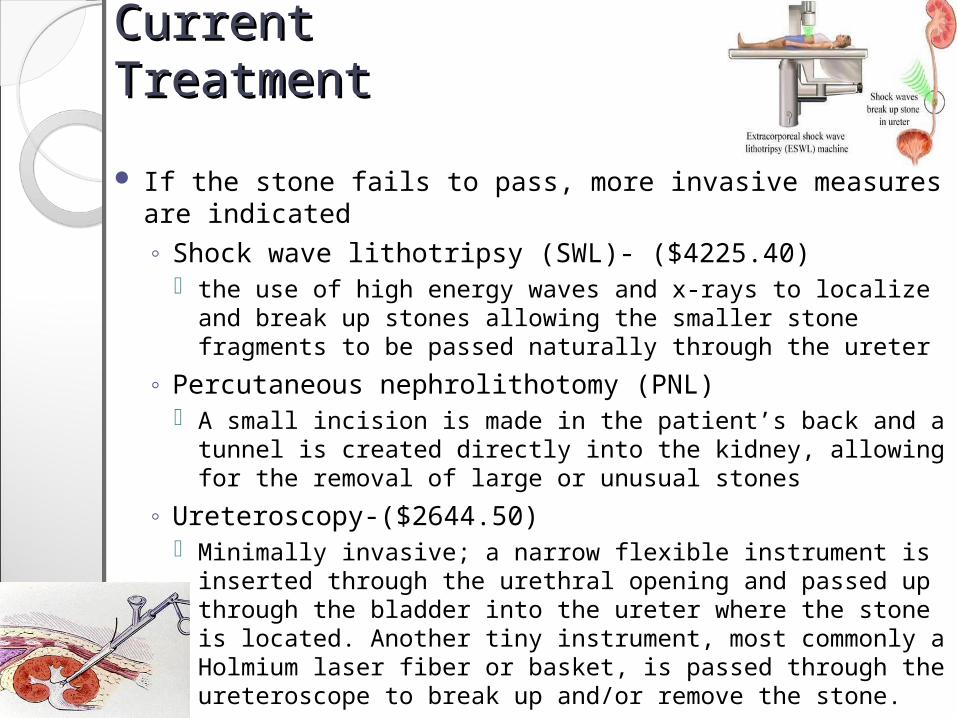
If the stone fails to pass, more invasive measures are indicated◦ Shock wave lithotripsy (SWL)- ($4225.40)
the use of high energy waves and x-rays to localize and break up stones allowing the smaller stone fragments to be passed naturally through the ureter
◦ Percutaneous nephrolithotomy (PNL) A small incision is made in the patient’s back and a tunnel is
created directly into the kidney, allowing for the removal of large or unusual stones
◦ Ureteroscopy-($2644.50) Minimally invasive; a narrow flexible instrument is inserted
through the urethral opening and passed up through the bladder into the ureter where the stone is located. Another tiny instrument, most commonly a Holmium laser fiber or basket, is passed through the ureteroscope to break up and/or remove the stone.

Medical Expulsion Therapy Medical Expulsion Therapy (MET)(MET)The use of pharmaceutical
agents to aid in the spontaneous expulsion of urethral calculi
Goals◦Improve stone passage rates◦Decrease the time to stone passage◦Decrease patient’s pain and colic
episodes◦Decrease health care costs, and lost
days at work

Medical Expulsion TherapyMedical Expulsion Therapy
Alpha-adrenergic receptor antagonists
Calcium channel blockersCorticosteroids

Physiology of the UreterPhysiology of the UreterContains α-adrenergic receptors
◦Highest concentration in the distal portion
Stimulation of these receptors results in increased force of ureteral contractions and the frequency of ureteral peristalsis
Adrenergic alpha-1-antagonists◦Inhibit basal tone, peristaltic frequency,
and the ureteral contractions◦Allows for antegrade stone propagation

AlalysisAlalysisDellabella et al. compared the expulsive
efficacy of different agents on distal ureteral calculi greater than 4 mm◦ spasmolytic agent: phloroglucinol 80 mg
Stone passage rate: 63.3% Time to passage: 5 days
◦an alpha blocker: tamsulosin 0.4 mg Stone passage rate: 97.1% Time to passage: 3 days
◦Calcium channel blocker: nifedipine 30 mg Stone passage rate: 77.1% Time to passage: 5 days
AnalysisAnalysisLiterature review performed by Beach et
al28 day trial Patients receiving tamsulosin 0.4mg
plus pain management◦Expulsion rate: 79.3-100%◦Average time to expulsion: 2.7-7.9 days
Patients receiving pain management alone◦Expulsion rate: 35-75%◦Average time to expulsion: 4.6-20 days
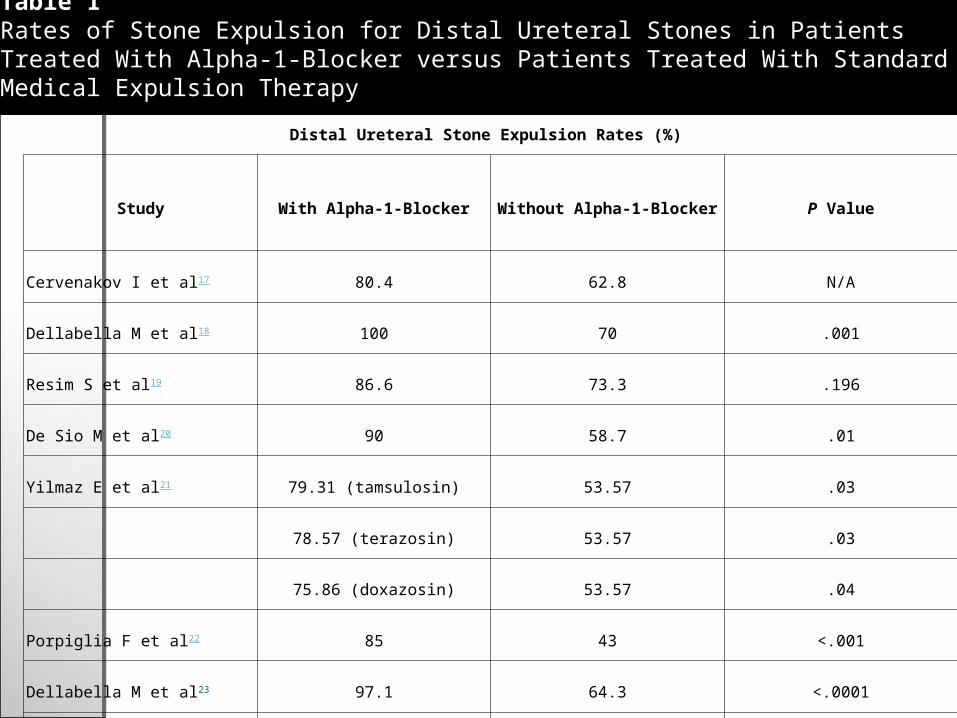
Distal Ureteral Stone Expulsion Rates (%)
Study With Alpha-1-Blocker Without Alpha-1-Blocker P Value
Cervenakov I et al17 80.4 62.8 N/A
Dellabella M et al18 100 70 .001
Resim S et al19 86.6 73.3 .196
De Sio M et al20 90 58.7 .01
Yilmaz E et al21 79.31 (tamsulosin) 53.57 .03
78.57 (terazosin) 53.57 .03
75.86 (doxazosin) 53.57 .04
Porpiglia F et al22 85 43 <.001
Dellabella M et al23 97.1 64.3 <.0001
Table 1Rates of Stone Expulsion for Distal Ureteral Stones in Patients Treated With Alpha-1-Blocker versus Patients Treated With Standard Medical Expulsion Therapy Without Alpha-1-Blocker

Distal Ureteral Stone Expulsion Times
Study With Alpha-1 Blocker Without Alpha-1 Blocker P Value
Dellabella M et al18 65.7 h 111.1 h .02
De Sio M et al20 4.4 d 7.5 d .005
Yilmaz E et al21 6.31 d (tamsulosin) 10.54 d .04
5.75 d (terazosin) 10.54 d .03
5.93 d (doxazosin) 10.54 d .03
Porpiglia F et al22 7.9 d 12 d .02
Dellabella M et al23 72 h 120 h <.0001
Table 2Time to Stone Expulsion for Distal Ureteral Stones in Patients Treated With Alpha-1-Blocker Versus Patients Treated With Standard Medical Expulsion Therapy Without Alpha-1-Blocker
Rev Urol. 2006; 8(Suppl 4): S35–S42
Rev Urol. 2006; 8(Suppl 4): S35–S42

Corticosteriod in addition to Alpha Corticosteriod in addition to Alpha BlockerBlockerThe use of corticosteroids are thought to
additionally aid in the expulsion when added to an alpha blocker by reducing ureteral edema which could cause secondary obstruction for stone passage
Dellabella et al. divided patients suffering from distal ureteral stones into two groups.◦ tamsulosin 0.4 mg daily
Expulsion rate: 90% Time to expulsion: 5 days
◦ corticosteroid deflazacort 30 mg in addition to tamsulosin 0.4 mg daily Expulsion rate: 96.7% Time to expulsion : 3 days
◦ They did not observe any differences between the groups in relation to the use of analgesics in order to control renal colic pain.

SWL and Alpha-BlockersSWL and Alpha-BlockersAlpha-blockers have been in addition
studied as an adjunct therapy along with shock wave lithotripsy (SWL).
48 patients suffering for distal ureteral stones of 6-15 mm in size
underwent SWL along with treatment of◦Tamsulosin 0.4mg plus oral hydration or
Stone Expulsion rate: 70.8%◦oral hydration alone
Stone Expulsion rate: 33.3%
Calcium Channel BlockersCalcium Channel BlockersUreteral smooth muscle contraction is
mediated by calcium channels
Theorized that CCBs will decrease spontaneous contractions of the ureter by blocking the calcium influx necessary for smooth muscle contraction, which may allow normal peristalsis to move the stone through the ureter.
In a study done by Borghi et al. it was found that patients receiving nifedipine had a significantly higher percentage of passing stones and a decreased time to expulsion compared to patients receiving placebo.

Patient CriteriaPatient Criteriapatient’s age and stone size were fairly uniform
in all trials
Patients with complications such as hydronephrosis, urinary tract infection (UTI), diabetes, hypotension, or declining renal function were excluded.
Adverse effects were not commonly encountered and were consistent with the known adverse effect profiles of the drugs. ◦ These included hypotension, dizziness, and asthenia. ◦ This low incidence of side effects could be due to the
fact that many trials excluded patients who were likely to experience the particular effects of the medications being administered.

Conclusion Conclusion Studies show that alpha blockers are
highly effective in ◦increasing the expulsion rate of ureteral
stones◦reducing the time to stone passage ◦decreasing the amount of pain medication
needed during passage of stones◦decrease hospitalization rates and the
need for more invasive procedures. ◦cost effective
typical course of the alpha antagonists ranging from $27.95 to $57.38

Conclusion (cont.)Conclusion (cont.)Stone size is considered one of the main factors
determining the possibility of spontaneous passage.
The use of α-antagonists has been shown to
augment stone passage rates of moderately sized, distal ureteral stones of 5-10 mm◦ Patients with stones less than 5 mm were found to be
just as likely to spontaneously pass the stone as patients receiving an alpha blocker, although the MET may aid in deceasing the patients overall discomfort and can lead to a decrease in the amount of analgesics needed.
◦ In patients suffering from calculi larger than 10 mm, the calculi may be too large to spontaneously pass even with the aid of an alpha blocker and an anti-inflammatory. These patients may show better benefits from combined procedures such as shock wave lithrotripsy and MET or ureteroscopy.
Conclusion (cont.)Conclusion (cont.)More invasive measures should be
indicated if:◦obstruction persists ◦the stone fails to progress towards
passage ◦in the setting of worsening pain.

ApplicationApplicationMET looks most promising for the future
treatment of urethral calculi of less than 10 mm located in the distal ureter
Patient selection for expulsive therapy should be derived from the entry criteria of the available studies
To avoid potential increased risk of kidney damage, expulsive therapy should be avoided in patients with ◦ hydronephrosis, UTI, a single kidney, hypotension,
and those patients already on antihypertensive therapy
The length of therapy should mirror the two to four week course duration used in the available trials
May be administered with in conjunction with corticosteroids and or NSAIDs, which can reduce ureteral edema and improve the ability for a patient to spontaneously pass a ureteral stone.

ApplicationApplicationThe use of alpha blockers for the
purposes of facilitating stone passage, however, is investigation and off label.
It is thought that MET can be suggested as first choice treatment for distal ureterolithiasis without complications due to its excellent expulsive efficiency, good pain control and patient satisfaction.

Works CitedWorks Cited Beach, M. A., & Mauro, L. S. (2006). Pharmacologic Expulsive Treatment of Ureteral
Calculi. The Annals of Pharmacotherapy , 40 (7), 1361-1368. Best, S. L., & Nakada, S. Y. (2008, May). Using Drugs to Expel Stones. Retrieved from
Renal and Urology News: http://www.renalandurologynews.com/Using-Drugs-to-Expel-Stones/article/110900/
Buehler, G., Mills, A. M., & Chen, E. H. (2007). Does the Addition of Tamsulosin to Outpatient Analgesic Therapy Enhance Spontaneous Stone Passage in Patients With Uncomplicated disal Ureteral Stones? Annals of Emergency Medicine , 50 (5), 564-568.
Dellabella, M., Milanese, G., & Muzzonigro, G. (2005). Medical-Expulsive Therapy for Distal Ureterolithiasis: Randomized Prospective Study on Role of Corticosteroids used in Conbination with Tamsulosin-Simplified Treatment Regimen and Health-Related Quality of Life. Urology , 66, 712-715.
Dellabella, M., Milanese, G., & Muzzonigro, G. (2005). Randomized Trial of the Efficacy of Tamsulosin, Nifedipine and Phloroglucinol in Medical Expulsive Therapy for Distal Ureteral Calculi. The Journal of Urology , 174, 167-172.
Lipkin, M., & Shah, O. (2006). The Us of Alpha-Blockers for the Treatment of Nephrolithiasis. Reviews in Urology , 8 (4), 35-42.
Micali, S., Grande, M., Sighinolfi, M. C., De Stefani, S., & Bianchi, G. (2007). Efficacy of Expulsive Therapy using nifedipine or tamsulosin, both associated with ketoprofene, after shock wave lithotripsy of ureteral stones. Journal Urological Research , 35, 133-137.
Naja, V., Agarwal, M. M., Mandal, A. K., Singh, S. K., Mavuduru, R., Kumar, S., et al. (2008). Tamsulosin Facilitates Earlier Clearance of Stone Fragments and Reduces Pain After Shockwave Lithotripsy for Renal Calculi: Results From an Open-Label Randomized Study. Urology , 72 (5), 713-719.
Singh, A., Alter, H. J., & Lettlepage, A. (2007). A Systematic Review of Medical Therapy to Facilitate Passage of Ureteral Calculi. Annals of Emergency Medicine , 50 (5), 552-563.