thursday gs 6 majewski - c.ymcdn.com€¦ · the ominous octet of type 2 diabetes per ralph a....
TRANSCRIPT

9/23/2014
1
Update on Medications
to Treat Type 2 Diabetes
Wisconsin Academy of
Physician Assistants Fall Conference
October 9, 2014
Kathryn G. Majewski, MSHS, PA-C
Gundersen Health System – La Crosse Endocrinology Department
Disclaimer
• No conflicts of interests.
• No financial relationships with any
commercial interests.
• ADA & AACE info used with permission.
“Update”
• Currently for type 2 diabetes medications, we have 12 classes of agents:
– 16 oral agents
– 14 insulin options
– 5 other injectable options
– Plus numerous combination products
– & many more coming down the pipeline
• But we only have 45 minutes…
The Ominous Octet of Type 2 Diabetesper Ralph A. DeFronzo, MD – U of TX-San Antonio
Diabetes 58:4 (2009):773-795.
The Ominous Octet
Pancreas
• Beta cell dysfunction & failure
• Decreased insulin production
Small intestine
• Decreased incretin effect
Adipose
• Increased lipolysis, increased free fatty acid production
• Further impairs insulin secretion
Kidneys
• Increased reabsorption of glucose
Muscle
• Decreased glucose uptake
Brain
• Neurotransmitter dysfunction
• Affects appetite & weight
Liver
• Increased hepatic glucose production (stimulated by increased free fatty acids)
Islet-alpha cells
• Increased glucagon secretion
• Responsible for high fasting glucose levels
Diabetes 58:4 (2009):773-795.
With this in mind
• Choose meds that would address multiple
issues
• The natural history of diabetes is such that
over time it becomes more challenging to
control.
• Most people will require multi-drug therapy,
often from the time of diagnosis.
• Why not start sooner?
9/23/2014
2
Step-therapy for DM-2
The Foundation: Therapeutic Lifestyle Changes
Healthy food / beverage choices; regular activity; weight loss
Monotherapy – usually metformin
Dual drug therapy
metformin + GLP-1/DDP-4/TZD/?
Triple drug therapy
Insulin
+/- orals, GLP-1
It’s an UPDATE, so
we’ll start with the newest meds
SGLT-2sSodium-glucose co-transporter 2 inhibitors
Actions:
• Inhibits SGLT-2 in proximal convoluted tubule, reducing reabsorption of filtered glucose
• Lowers renal threshold for glucose
• Increases urinary excretion of glucose
• Causes osmotic diuresis
At present, 3 options (more to follow):
• canagliflozin (Invokana)
• dapagliflozin (Farxiga)
• empagliflozin (Jardiance)
SGLT-2s work here
Diabetes 58:4 (2009):773-795.
SGLT-2s
Advantages:
• Low risk of hypoglycemia –works only with hyperglycemia
• Lose about 400 calories per day via urine glucose– 4-6 pound wt loss
• Decreases BP by about 5 points on average– Diuretic effect
• Can be used early or late in the disease process
Disadvantages:
• May increase LDL by 4-8 points
• Don’t use with eGFR <45 (canaglifozin, empagliflozin) or < 60 (dapagliflozin)
• Increased risk of genital fungal infections & UTI, especially in those prone to such infxns
• Hypotension in elderly, with dehydration, etc.
• Increased urination & thirst, maybe constipation
• Increased risk of hyperkalemiawith canagliflozin, especially in CKD patients
SGLT-2s
Contradictions:
• eGFR < 60 (dapagliflozin)
• eGFR < 45 (canaglifozin, empagliflozin)
• Need to monitor creatinine & eGFR in folks using SGLT-2s– May cause slight increase
in creatinine & slight decrease in eGFR, especially in the elderly
Precautions:
• eGFR 45-59 (canaglifozin, empagliflozin)
• Use of loop diuretic– Reduce dose of loop
• Elderly
• Low systolic BP
• Issues re: dehydration– Athletes, outdoor work,
elderly, cognitively challenged, etc
• Pregnancy category C

9/23/2014
3
SGLT-2s
• Could be a good option for truck drivers with
CDL but will test positive for urine glucose, so
need to send documentation re: this when
they get their DOT physical.
GLP-1 receptor agonists
AKA incretin mimetics• About 60% of post-meal insulin secretion is due to
effects of incretins. These effects are diminished in people with DM-2 & pre-diabetes.
Actions:
• Stimulates GLP-1 receptors, which enhances glucse-dependent insulin secretion
• Inhibits post-prandial glucagon release, so reduces heptatic glucose output
• In CNS, reduces appetite, promotes earlier satiety
• Slows gastric emptying
• Therefore weight loss
GLP-1 receptor agonists
AKA incretin mimetics
• 5 options available, all with pen devices:
• exenatide (Byetta) – twice daily injection before meals
• liraglutide (Victoza) – once daily injection regardless of meals
• exenetide extended-release (Bydureon) – once weekly injection (new pen device)
• albiglutide (Tanzeum) – once weekly injection
• dulaglutide (Trulicity) – once weekly injection (just approved by FDA – not yet in stores as of 9-22-14)
GLP-1 receptor agonists
Advantages:
• Low risk of hypoglycemia
• Appetite suppression
• Weight loss
• “I never knew before what it felt like to be full.”
• A motivator for further weight loss / healthier lifestyle
Disadvantages:
• Requires injection
• GI side effects are common– Nausea, diarrhea
– Usually transient
– Usually manageable
– May require dose adjustment
• Requires more education
• Pregnancy category C
GLP-1 receptor agonists
Contraindications:
• Gastroparesis
• Chronic nausea, vomiting,
motility issues
• History of pancreatitis
• CrCl < 30
• Hx of medullary thyroid
carcinoma or MEN-2
– Black box warning re: risk
of thyroid tumors in rats
Precautions:
• Risk factors for
pancreatitis
• Chronic diarrhea
• Chronic abdominal pain
• Active peptic ulcer
GLP-1 receptor agonists work here
Diabetes 58:4 (2009):773-795.

9/23/2014
4
DPP-4 inhibitors: dipeptidyl peptidase-
4 inhibitors or incretin enhancers
Actions:
• Incretins have very short half-life – < 2 minutes in circulation
• DPP-4 inhibitors prolong the half-life of endogenous incretins by inhibiting their degradation
• Thereby increases post-prandial insulin secretion & decreases glucagon secretion
• Glucose-dependent action
DPP-4 inhibitors
Options:
• sitagliptin (Januvia)
• saxagliptin (Onglyza)
• linagliptin (Tradjenta)
• alogliptin (Nesina)
• All once-daily oral agents
• In stage 3 trials, a once-a-week version
DPP-4 inhibitors
Advantages:
• Oral, once daily
• Low risk of hypoglycemia
• Weight neutral
• No GI side effects
• Pregnancy category B
Disadvantages:
• Requires dose adjustment for renal disease with eGFR < 60
– Except linagliptin
• Post-marketing reports of hepatic failure with alogliptin, increased liver enzymes with sitagliptin
DPP-4 inhibitors
Contraindications:
Precautions:
• Hx of pancreatitis
• Risk factors for pancreatitis
• Potential slight increase risk of CHF, seen in 2 recent studies
Precautions:
• Decrease dose of sitagliptin, saxagliptin if eGFR < 50, alogliptin if eGFR < 60
• Decrease dose of saxagliptin if also taking strong cytochrome P450 3A4/5 inhibitors (ketoconazole, clarithromycin, etc)
DPP-4 inhibitors work here Just so you know…
Because they over-lap in their functions,
you should use
EITHER a GLP-1
OR a DPP-4,
not both at the same time.

9/23/2014
5
OK, you have the new stuff.
Let’s go back to
the old stuff.
Underlying theme of DM-2
is insulin resistance
• Starts long before person meets criteria for diagnosis of DM-2 or even pre-diabetes
• Suspect it in the right person
• Screen for it regularly
• Jump on it & treat it aggressively from the start
• Remember that HTN = insulin resistance
• Remember that high triglycerides & low HDL = insulin resistance
Screen with A1c
• First measurable defect is elevated post-
prandial glucose
• Will cause rise in A1c long before rise in
fasting glucose
• An A1c > 5.7% = pre-diabetes & deserves tx
• An A1c > 6.5% = diabetes & deserves tx
• For both, tx = therapeutic lifestyle changes +
medication
By the time they meet criteria for
diagnosis of DM-2, 50% of beta
cells have been destroyed.
For good.
Be nice to your beta cells –
you only get so many.
Preserve those beta cells!
• By addressing the reason for their early demise
– Hyperglycemia
– Insulin resistance
– Over-working the beta cells
– They eventually burn out & quit working
• Help keep them working happily longer by giving metformin.
• Avoid using meds that will help them burn out sooner, like sulfonylureas.

9/23/2014
6
Metformin
Actions:
• Decreases hepatic glucose output
• Reduces gluconeogenesis & glycogenolysis
• Increases peripheral glucose uptake & utilization
• Enhances insulin sensitivity
• Decreases intestinal glucose absorption
• Does not affect insulin production
• Antiatherogenic effects (DeFronzo)
Metformin
Options:
• metformin – twice daily with meals
• metformin extended-release – once daily with a meal
• In combination pills with many other DM meds
• We generally use 500 mg tablets, as the larger once are often too large to swallow.– 500 mg daily x several days, then 1000 mg daily x
several days, then 1500, then 2000 long term
Metformin
Advantages:
• Does not cause hypoglycemia
• Weight neutral
• Generally well tolerated
• On the $4 lists
• Plays nicely with others
• Good evidence it reduces risk of progression from IGT to DM
• Pregnancy category B
Disadvantages:
• GI side effects fairly common
• Nausea, loose stools, usually mild & short term– Some metformin is better
than no metformin
• Potential B-12 deficiency
• Lactic acidosis – rare but serious
Metformin
Contraindications:
• Significant CKD– d/c if creatinine
• > 1.4 women,
• > 1.5 men
• Clinically significant CHF
• Hypoperfusion (sepsis, MI, etc)
• Dehydration (GI losses, elderly, dementia, etc)
• Significant liver disease
Precautions:
• Stop temporarily if:• Dehydration for any reason
• Surgery or procedure (colonoscopy prep)
• Need for contrast dye for imaging studies
• Hospitalization
• Gastroenteritis
Lactic acidosis secondary to metformin
Preventable! Choose the right pts for the drug.
• Rare (3 cases per 100,000 pt-yr – most of whom had underlying contraindications to metformin)
• Lactate levels >5 mmol/L• Decreased blood pH• Increased anion gap• Increased lactate/pyruvate ratio. • Electrolyte disturbances • Treatment with hemodialysis• 40% mortality
Diabetes Care July 2004 vol. 27 no. 7 1791-1793
Metformin works here
Diabetes 58:4 (2009):773-795.

9/23/2014
7
Another oldy but a goody
• For the right person, anyway…
• TZDs or thiazolidinediones
TZDs
Actions:
• Enhance insulin sensitivity in muscle & fat by increasing glucose transporter expression
• Increase glucose disposal by muscle
• Decrease glucose output from liver
Options:
• pioglitazone (Actos)
• rosiglitazone (Avandia)
• But these 2 are very different from each other
TZDsAdvantages:
• Once-daily oral
• Low risk hypoglycemia
• Pio improves lipids, lowers triglycerides, raises HDL
• Pio improves fatty liver –very common in DM-2
• Relatively safe in renal failure
• Preserves beta cell fxn
• Improves albumin excretion
• Improves vascular smooth muscle proliferation
Disadvantages:
• Takes 2-3 months to see full effect
• Fluid retention, therefore weight
gain in some
• Can push someone over the fence
into CHF - warn pt & d/c drug if wt
gain &/or edema
• Possible increased risk of fracture,
esp women 50+ yo
• Post-marketing reports of hepatic
failure – monitor if at increased risk
• Don’t use with gemfibrozil or
rifampin
• Pregnancy category C Peripheral (subQ) fat is associated with improvement of insulin sensitivity, whereas
central or visceral fat is the bad fat that is associated with insulin resistance.Vasc Health Risk Manag 2010; 6: 671-690.
Effect of pioglitazone on fat
TZDs & bladder cancer
• Recent studies have shown potential increase risk of bladder cancer
– In folks on TZD the longest & on the highest doses
• Smokers are up to 7 x higher risk of bladder cancer than non-smokers
• Risk of bladder cancer in general population of non-smokers is low
– Increasing the risk of a low risk condition is still a very low risk
• I’ll consider 15-30 mg of pio daily for non-smoker
TZDs
Contraindications:
• Class III-IV CHF
• Significant edema
• Significant liver disease
• +/- osteoporosis
• Hx of bladder cancer
Precautions:
• CHF
• Hepatic disease
• Heavy alcohol use
• Smokers
• Advanced age
9/23/2014
8
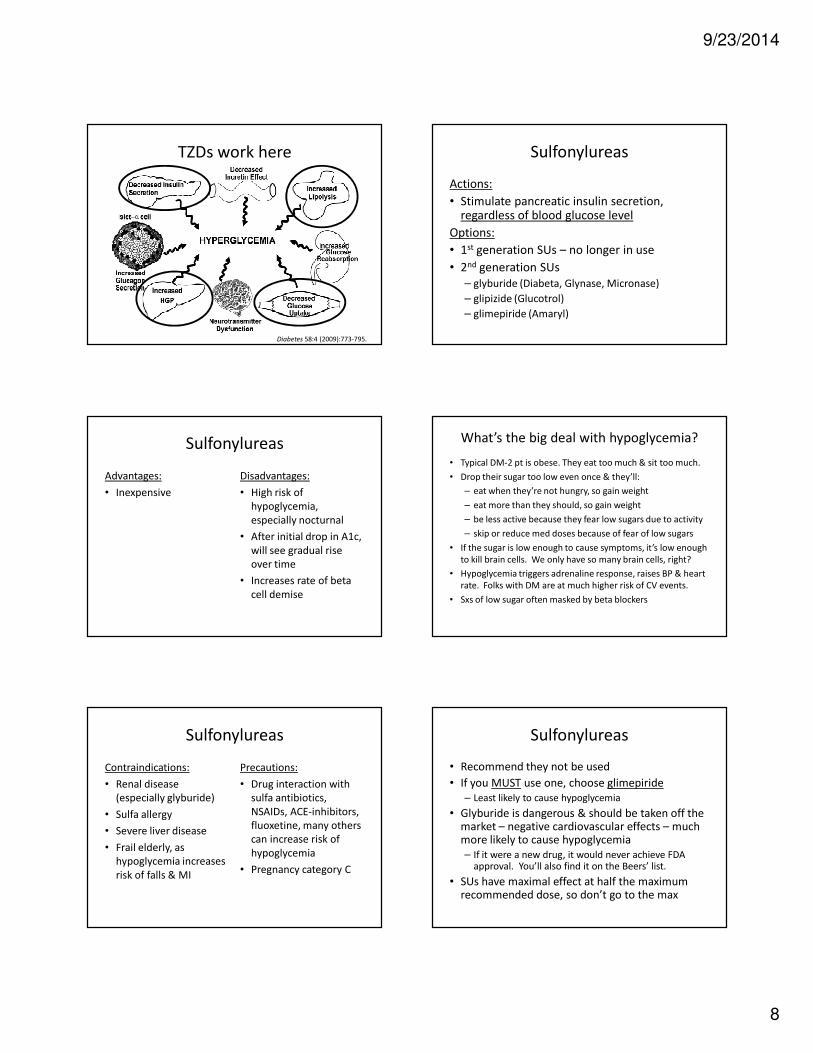
TZDs work here
Diabetes 58:4 (2009):773-795.
Sulfonylureas
Actions:
• Stimulate pancreatic insulin secretion, regardless of blood glucose level
Options:
• 1st generation SUs – no longer in use
• 2nd generation SUs
– glyburide (Diabeta, Glynase, Micronase)
– glipizide (Glucotrol)
– glimepiride (Amaryl)
Sulfonylureas
Advantages:
• Inexpensive
Disadvantages:
• High risk of
hypoglycemia,
especially nocturnal
• After initial drop in A1c,
will see gradual rise
over time
• Increases rate of beta
cell demise
What’s the big deal with hypoglycemia?
• Typical DM-2 pt is obese. They eat too much & sit too much.
• Drop their sugar too low even once & they’ll:
– eat when they’re not hungry, so gain weight
– eat more than they should, so gain weight
– be less active because they fear low sugars due to activity
– skip or reduce med doses because of fear of low sugars
• If the sugar is low enough to cause symptoms, it’s low enough
to kill brain cells. We only have so many brain cells, right?
• Hypoglycemia triggers adrenaline response, raises BP & heart
rate. Folks with DM are at much higher risk of CV events.
• Sxs of low sugar often masked by beta blockers
Sulfonylureas
Contraindications:
• Renal disease
(especially glyburide)
• Sulfa allergy
• Severe liver disease
• Frail elderly, as
hypoglycemia increases
risk of falls & MI
Precautions:
• Drug interaction with
sulfa antibiotics,
NSAIDs, ACE-inhibitors,
fluoxetine, many others
can increase risk of
hypoglycemia
• Pregnancy category C
Sulfonylureas
• Recommend they not be used
• If you MUST use one, choose glimepiride
– Least likely to cause hypoglycemia
• Glyburide is dangerous & should be taken off the market – negative cardiovascular effects – much more likely to cause hypoglycemia
– If it were a new drug, it would never achieve FDA approval. You’ll also find it on the Beers’ list.
• SUs have maximal effect at half the maximum recommended dose, so don’t go to the max
9/23/2014
9
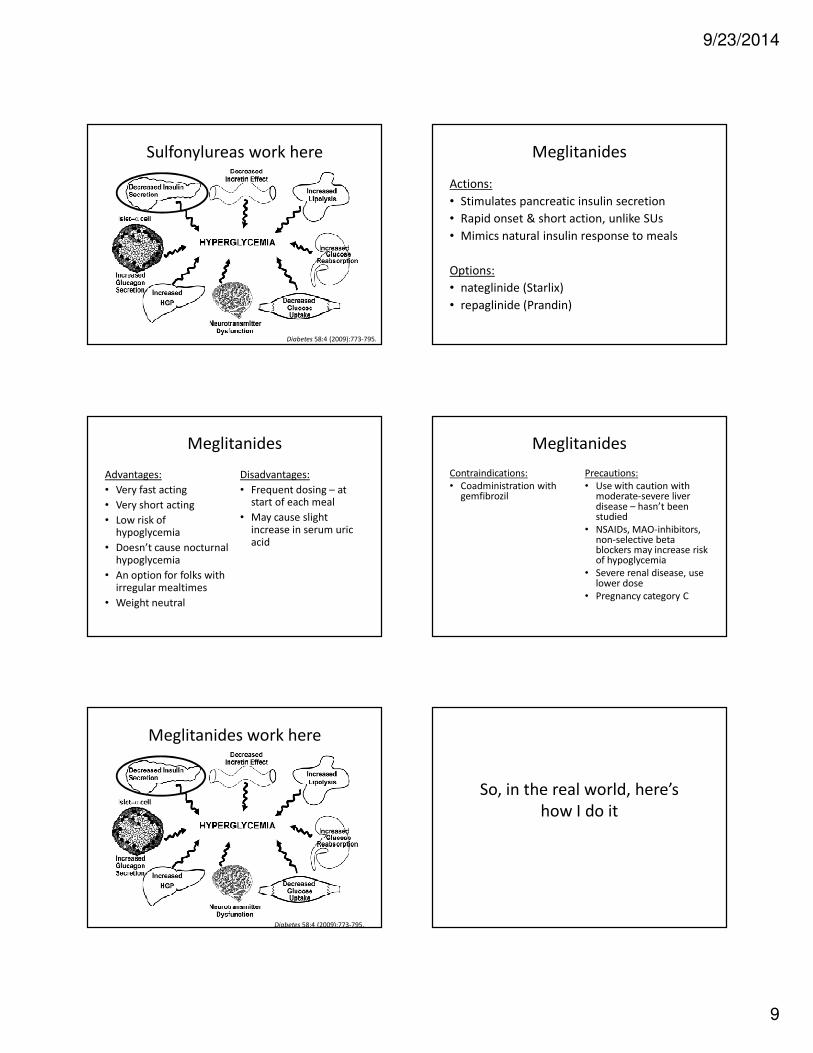
Sulfonylureas work here
Diabetes 58:4 (2009):773-795.
Meglitanides
Actions:
• Stimulates pancreatic insulin secretion
• Rapid onset & short action, unlike SUs
• Mimics natural insulin response to meals
Options:
• nateglinide (Starlix)
• repaglinide (Prandin)
Meglitanides
Advantages:
• Very fast acting
• Very short acting
• Low risk of hypoglycemia
• Doesn’t cause nocturnal hypoglycemia
• An option for folks with irregular mealtimes
• Weight neutral
Disadvantages:
• Frequent dosing – at start of each meal
• May cause slight increase in serum uric acid
Meglitanides
Contraindications:
• Coadministration with gemfibrozil
Precautions:
• Use with caution with moderate-severe liver disease – hasn’t been studied
• NSAIDs, MAO-inhibitors, non-selective beta blockers may increase risk of hypoglycemia
• Severe renal disease, use lower dose
• Pregnancy category C
Meglitanides work here
Diabetes 58:4 (2009):773-795.
So, in the real world, here’s
how I do it

9/23/2014
10
In general,
• Start with lifestyle modification – even before dxof pre-diabetes in people at higher risk
• Start metformin at time of dx of pre-DM or DM to preserve beta cell function, which has already dropped substantially
• Add a GLP-1 if they need weight loss
– Or a DPP-4 if they are normal wt or decline injectables
• Add TZD if not high risk for CHF, not smoker
• Add SGLT-2 or add basal insulin, later prandialinsulin
Official guidelines
American Diabetes Association – ADA
• Updated every January
• Lots of choices & lots of good info, but not much guidance re: meds
• http://professional.diabetes.org/ResourcesForProfessionals.aspx?cid=84160
American Association of Clinical Endocrinologists
• Updated 2013
• Focused on physiology
• Emphasizes therapies that don’t cause hypoglycemia &/or weight gain, which are major safety & compliance barriers
• https://www.aace.com/publications/algorithm
At diagnosis, AACE recommends
• If A1c is < 7.5%
– Start with metformin (& lifestyle, of course)
• If A1c is > 7.5%
– Start with metformin + another agent
• If A1c is > 9%
– If no sxs, start with dual- or triple-drug oral therapy
– If sxs, start with basal insulin, at least short term, till s/sx dehydration resolve, to protect kidneys
Add-on therapy should target a
different physiology issue
Diabetes 58:4 (2009):773-795.
Choose therapy for the individual
• First step is to consider contraindications• Metformin in CKD, pioglitazone in CHF, etc.
• Next, evaluate patient values & preferences• Desire / need for weight loss?
• Is hypoglycemia especially dangerous for that person?
• Fear of injections?
• Financial burden? Insurance issues?
• Age – be much more aggressive with younger pts
• Get patient “buy-in”. It helps a lot with compliance.
• Remember, each patient is the captain of their own health care team.
Choose goals of therapy
for that individual
• Based on their preferences, lifestyle, age, co-morbidities, risk factors, etc.
• A1c goals:
– Generally < 7%
– < 6.5% for healthy pts without concurrent illness
& at low risk for hypoglycemia
– < 7.5% for pts with cardiac disease, but only if you can do that with NO hypoglycemia
– < 8% for elderly, frail, with NO hypoglycemia
– Adjust goals over time to fit pt’s current situation

9/23/2014
11
The financial burden
• Brand name drugs almost always have a co-pay discount program
– www.(insert brand name here).com
• Hot competition in some classes, so can get co-pay fully paid by the pharma company
• These programs apply to non-govt-funded insurance plans (including the exchanges)
• Many pharma companies change rules for pt assistance programs for those in Medicare –D donut hole
A gift for you
www.fingertipformulary.com
• Choose the drug
• Choose your state
• Choose patient’s insurance plan (non-Medicare & Medicare plans)
• Shows you tier for that drug
• Gives link for plan’s full formulary
• Quick & easy to do in exam room
• Saves time/hassle, frustration & improves compliance
The bottom line:
• Start early in the disease process
• Be aggressive with therapy to preserve beta cell function
• Go at it from several different directions with medications
• Weight loss
• Weight loss
• Weight loss
• Close follow up
For your patients who will
only go the “natural” route
• SGLT-2s were derived from the bark of apple
trees
• Metformin was derived from the French lilac
plant
• GLP-1s were derived from saliva from lizards
• Obesity is not natural. Weight loss is good!
For the sake of completeness,
I am including the following
information on your handouts, but
will not have time to discuss this
during the presentation.

9/23/2014
12
Insulins
Actions:
• Insulin replacement therapy
• Reduces blood glucose
• Gives beta cells a rest to some extent
Dosing options:
• Vial & syringe
• Pen device
• Same price with most insurance plans
Insulin options
The preferred plan:• Long-acting basal insulins:
– glargine (Lantus), detemir (Levemir)
• Rapid-acting prandial insulins:– lispro (Humalog), aspart (NovoLog), glulisine (Apidra)
• U-500 R insulin for those severely insulin resistant (>200 u / day)– Be sure you know what you’re doing with it before prescribing U-500 – it’s a
completely different ball game & totally unlike standard Regular insulin.
Used less often, but somewhat less expensive – often gives wider & more frequent fluctuations in blood glucose levels, more hypoglycemia
• Intermediate-acting insulins – twice daily dosing:– NPH (Humulin N, Novolin N)
• Short-acting prandial insulins:– Regular (Humulin R, Novolin R)
• Fixed-dose combinations– 70/30, 75/25, 50/50, etc – very limited flexibility, more low sugars
Insulin options
Used less often, but somewhat less expensive – often causes wider & more frequent fluctuations in blood glucose levels, more hypoglycemia
• Intermediate-acting insulins – twice daily dosing:– NPH (Humulin N, Novolin N)
• Short-acting prandial insulins:– Regular (Humulin R, Novolin R)
• Fixed-dose combinations– 70/30, 75/25, 50/50, etc – very limited flexibility, more
low sugars
Insulins
Advantages:
• Works quickly
• Once-daily basal insulin may be enough
• Plays nicely with other DM meds
• Many options, much flexibility with dosing
Disadvantages:
• Injections / hassle
• Must be open to monitoring, reporting sugars, frequent dose adjustments
• Significant risk of hypoglycemia
• VERY user dependent
• Takes dexterity, other physical & cognitive abilities
• Requires ongoing patient education
Insulins
Contraindications:
• None, other than the
universal previous
allergic reaction to the
drug
Precautions:
• Severe hypoglycemia
• Reduce dose with
severe renal or hepatic
disease
Insulins work here – sort of
Diabetes 58:4 (2009):773-795.

9/23/2014
13
Tips for insulin therapy• Always inject in the abdomen, not the extremities, to
improve absorption & consistent effectiveness
• If dose is > 50 units, split into 2 smaller doses in 2 separate locations to improve absorption & effectiveness
• If on prandial insulin, don’t use a sliding scale that says no insulin if sugar is less than … at mealtime– Give a base dose, & go up a bit or down a bit depending
upon their pre-meal sugar, but they need SOME prandialinsulin at each meal
• The most accurate “generic” meter & strips are the Relion brands from Wal-Mart. Relion insulins are also a less expensive option for folks without insurance.
Alpha-glucosidase inhibitors
Advantages:
• Weight neutral
• Does not cause
hypoglycemia
Disadvantages:
• Dosed at start of each
meal
• Significant GI issues,
especially flatulance
• May cause diarrhea,
abdominal discomfort
• Potential very low risk
of liver toxicity
Alpha-glucosidase inhibitors
Actions:
• Competitively blocks the enzyme alpha-
glucosidase in brush border of small intestine
– Therefore slows breakdown of carbohydrate to
glucose & delays intestinal glucose absorption
Options:
• acarbose (Precose)
• miglitol (Glyset)
Alpha-glucosidase inhibitors
Contraindications:
• Inflammatory bowel
disease
• Hx of intestinal
obstruction or at risk
• Colonic ulceration
Precautions:
• Pregnancy category B
Alpha glucosidase inhibitors work in
the gut, but does not involve incretins
Diabetes 58:4 (2009):773-795.
Bile acid sequestrant
Actions:
• May reduce hepatic insulin resistance
• Therefore, reduced hepatic glucose production
• May have effect on molecular mediators of
glucose metabolism
• May reduce intestinal glucose absorption
Options:
• colesevelam (Welchol)

9/23/2014
14
Bile acid sequestrant
Advantages:
• Not systemically absorbed
• Weight neutral
• Does not cause hypoglycemia
• Lowers LDL about 20%
• May help IBS-diarrhea predominant sxs
• Safe in CKD, CHF
Disadvantages:
• Inconvenient dosing– Either 3 big pills bid or
powder mixed with liquid daily
• Can cause constipation & abdominal bloating
• Can interfere with absorption of some nutrients & some meds, esp OCPs & antibiotics
• Can increase triglycerides
Bile acid sequestrant
Contraindications:
• Triglyceride > 500
• Hx of bowel obstruction
• Hx of triglyceride-
induced pancreatitis
Precautions:
• Triglyceride > 300
• Multiple drug
interactions re:
interfering with
absorption
• Pregnancy category B
Bile acid sequestrant works in the gut
but does not involve incretins
Diabetes 58:4 (2009):773-795.
Dopamine agonist
Actions:
• Uncertain; may centrally reverse many of the
metabolic changes associated with insulin
resistance & obesity
Option:
• bromocriptine (Cycloset)
Dopamine agonist
Advantages:
• Low risk of hypoglycemia
• Weight neutral
• Lowers risk of CV events
Disadvantages:
• Common side effects:
– Nausea, vomiting
– Headache
– Hypotension, SYNCOPE
– Dizziness
– Fatigue
– Confusion
– Depression
– Agitation / hallucinations
Dopamine agonist
Contraindications:
• Antipsychotic use
• Severe psychotic
disorder
• Breastfeeding
• Syncope
• Use of ergot
medications
• Hypotensive
Precautions:
• If treating diabetes, use
much lower doses than
used for other reasons
• Start with 0.8 mg first
thing in the morning
• Pregnancy category B

9/23/2014
15
Dopamine agonist works here
Diabetes 58:4 (2009):773-795.
Amylin analog
Actions:
• Slows gastric emptying
• Therefore feeling of early satiety
• Decreases post-prandial glucagon secretion
Option:
• pramlintide (Symlin)
Amylin analog
Advantages:
• Contributes to weight
loss
Disadvantages:
• Injected prior to meals
• Hypoglycemia
• May cause nausea
Amylin analong
Contraindications:
• Hypoglycemia unawareness
• Gastroparesis
Precautions:
• if also taking insulin, reduce mealtime insulin dose by 50% to reduce risk of hypoglycemia
• Needs to be taken separated from oral meds or may impair their absorption
• Pregnancy category C
Amylin analog works here
Diabetes 58:4 (2009):773-795.