universidade federal do rio de janeiro hospital …livros01.livrosgratis.com.br/cp120268.pdf ·...
TRANSCRIPT

UNIVERSIDADE FEDERAL DO RIO DE JANEIROHOSPITAL UNIVERSITÁRIO CLEMENTINO FRAGA FILHO
FACULDADE DE MEDICINA DA UFRJINSTITUTO DE BIOFÍSICA CARLOS CHAGAS FILHO
VALÉRIA BATTISTELLA AMADO DOS SANTOS
SEGURANÇA DO TRANSPLANTE AUTÓLOGO DE CÉLULASMONONUCLEARES DA MEDULA ÓSSEA EM PACIENTES COM ACID ENTE
VASCULAR CEREBRAL ISQUÊMICO SUBAGUDO
RIO DE JANEIRO2009

Livros Grátis
http://www.livrosgratis.com.br
Milhares de livros grátis para download.

VALÉRIA BATTISTELLA AMADO DOS SANTOS
SEGURANÇA DO TRANSPLANTE AUTÓLOGO DE CÉLULAS MONONUCLEARESDA MEDULA ÓSSEA EM PACIENTES COM ACIDENTE VASCULAR CEREBRAL
ISQUÊMICO SUBAGUDO
Dissertação de Mestrado apresentada aoPrograma de Pós-Graduação em Clínica Médica,Universidade Federal do Rio de Janeiro, comorequisito parcial à obtenção do título de Mestreem Clínica Médica, com área de atuação emNeurologia
Orientadores:Charles AndréRosália Mendez-OteroGabriel Rodriguez de Freitas
Rio de Janeiro2009

B336 Battistella, Valéria Segurança do transplante autólogo de células monucleares
da medula óssea em pacientes com acidentes vascular cerebral isquêmico sub-agudo. / Valéria Battistella. – 2009 75 f.
Dissertação (Mestrado em Clínica Médica) –Universidade Federal do Rio de Janeiro, Instituto de Biofísica Carlos Chagas Filho. Hospital Clementino Fraga Filho, Rio de Janeiro, 2009.
Orientador: Charles André.
1.Clínica médica – Teses. 2. AVC isquêmico. 3.Célula Tronco. 4. Medula óssea. I. André, Charles. II. Universidade
Federal do Rio de Janeiro. Instituto de Pós-Graduação em Clínica Médica. III. Título. CDD 616

Valéria Battistella Amado dos Santos
SEGURANÇA DO TRANSPLANTE AUTÓLOGO DE CÉLULAS MONONUCLEARESDA MEDULA ÓSSEA EM PACIENTES COM ACIDENTE VASCULAR CEREBRAL
ISQUÊMICO SUBAGUDO
Dissertação de Mestrado apresentada aoPrograma de Pós-Graduação em Clínica Médica,Universidade Federal do Rio de Janeiro, comorequisito parcial à obtenção do título de Mestreem Clínica Médica, com área de atuação emNeurologia.
_____________________________________________Prof. Dr. Charles AndréUniversidade Federal do Rio de Janeiro
_____________________________________________Profª Drª Lea Miriam Barbosa da FonsecaUniversidade Federal do Rio de Janeiro
_____________________________________________Prof. Dr. Marcos Raymundo Gomes de FreitasUniversidade Federal Fluminense
_____________________________________________Prof. Dr. Maurice VincentUniversidade Federal do Rio de Janeiro
Data: ________________________________________

AGRADECIMENTOS
Agradeço a Deus, pela minha vida.
Aos meus pais, Paulo e Ieda, pelo esforço desempenhado com minha educação.
Aos meus irmãos, Wagner e Wander, e madrinha Edinéa, pelo estímulo constante aos estudos.
Ao meu marido Cesar pelo amor e companheirismo nos últimos 15 anos e à minha filha
Beatriz, simplesmente por existir.
A toda a equipe multiprofissional envolvida neste projeto, pelo carinho e dedicação em sua
realização: Daniel Mercante, Juliana Dias, Regina Goldenberg, Thais Kazai-Binswick, Bianca
Gutfien, Cláudia Lopes, Eduardo Wajnberg, Soniza Vieira e Lea Miriam Barbosa da Fonseca.
Aos meus orientadores, Charles, Rosália e Gabriel, pela atenção e orientação a mim
dispensada, nesta importante fase da vida acadêmica.

RESUMO
O Acidente vascular cerebral (AVC) permanece a principal causa de incapacidade no mundo
e há poucos estudos clínicos avaliando formas efetivas de melhorar a incapacidade residual
(CRAMER, 2008). Nos últimos anos, muitos estudos investigaram o potencial papel
restaurador de células-tronco, de diferentes fontes, em modelos animais de isquemia cerebral
(MENDEZ-OTERO; de FREITAS; MENDONÇA; ANDRÉ, 2007). Este é um estudo clínico
fase 1, para averiguar a segurança e exequibilidade do transplante autólogo de células
mononucleares da medula óssea (CMMO), em pacientes com acidente vascular cerebral
(AVC) isquêmico, em território da artéria cerebral média (ACM), ocorrido até 90 dias antes
da infusão. Dez por cento das células a serem injetadas foram marcadas com 99mtecnécio para
avaliação da cinética das CMMO após a injeção. Sete pacientes (idade entre 24 e 65 anos)
preencheram todos os critérios de inclusão. Foi realizado aspirado de medula óssea pela crista
ilíaca, sob sedação e anestesia local. As CMMO foram isoladas do aspirado utilizando
gradiente Ficoll; 10% das células foram separadas e marcadas com 99mtecnécio e reinjetadas
na ACM responsável pelo AVC (mínimo de 1 x 108 e máximo de 5 x 108 células injetadas),
por técnica de Seldinger. Imagens cintilográficas foram realizadas duas e 24 horas após o
procedimento. Eletroencefalograma foi feito nos primeiros sete dias após o transplante. Os
pacientes foram avaliados utilizando hemograma e bioquímica e avaliação de escalas
neurológicas (escala de AVC do Instituto Nacional de Saúde Americano, Escala modificada
de Rankim e Índice de Barthel), antes da infusão das CMMO e 1, 3, 7, 30, 60, e 120 dias
após. Não houve qualquer complicação ou eventos adversos ligados diretamente ao
procedimento. Em seis pacientes não houve piora evolutiva das escalas neurológicas até o
final do acompanhamento. Um paciente necessitou intervenção cirúrgica uma semana após a
infusão das CMMO (intercorrência clínica não ligada ao procedimento), apresentando novo
evento isquêmico cerebral no pós-operatório. Em todos os pacientes houve captação na
Tomografia Computadorizada de fóton único (sigla em inglês, SPECT) e nas imagens
corporais totais realizados duas horas após infusão das CMMO marcadas. Devido à meia-vida
curta do tecnécio (seis horas), nem todas as imagens realizadas 24 horas após a infusão
apresentavam atividade do radiofarmaco. Todos os pacientes permaneceram em
acompanhamento mesmo após o término do protocolo (120 dias) e dois pacientes
apresentaram crise convulsiva tônico-clônica generalizada, aproximadamente 200 dias após a
infusão. Apesar das crises convulsivas, não houve alteração nas escalas de avaliação,

comparado ao 120° dia de acompanhamento. Neste pequeno estudo piloto, fase 1, a infusão
intra-arterial de CMMO em pacientes com AVC isquêmico (fase subaguda) foi segura e
exequível. Observou-se que a fração de CMMO marcada permaneceu na área isquêmica por,
pelo menos, 24 horas em alguns pacientes. Estudos fase 2, com inclusão de maior número de
pacientes, são necessários para avaliar eficácia e segurança.

PALAVRAS-CHAVE: AVC ISQUÊMICO, CÉLULA-TRONCO, MARCAÇÃO CÉLULA-
TRONCO, CÉLULA MONONUCLEAR, MEDULA ÓSSEA.

ABSTRACT:
Stroke remains the leading cause of disability in the world. There are few clinical trials that
evaluated effective ways to enhance recovery in patients with residual disability (CRAMER,
2008). In recent years, several studies have investigated the potential restorative role of stem
cells from different sources in animal models of brain ischemia (MENDEZ-OTERO; de
FREITAS; MENDONÇA; ANDRÉ, 2007). This is a phase 1 clinical study to assess the safety
and feasibility of bone-marrow mononuclear cell (BMMC) transplantation in patients with
middle cerebral artery (MCA) territory ischemic stroke, within 90 days of stroke onset. In all
patients a portion of the infusion cells (10%) was marked with tecnecium-99-m to evaluate
the fate of BMMC after injection. Seven patients (aged 24 to 65 years) filled all the inclusion
criteria according to a protocol registered in the Research Ethics Committee, number 169/03.
Iliac-crest bone-marrow aspiration was performed under sedation and local anesthesia.
BMMC were isolated using a Ficoll gradient, and 10% of the cells were separated and labeled
with 99mTc and re-injected in the MCA responsible for the stroke (minimum: 1 x 108 and
maximum: 5 x 108 injected cells) after navigation (Seldinger technique). Single photon
emission computerized tomography (SPECT) and whole-body scan images were done two
and 24 hours after the procedure. Electroencephalogram was done within 7 days after
transplantation. Patients were evaluated with complete blood count, biochemical exams and
by neurological scales (National Institute of Health Stroke Scale, modified Rankin Scale, and
Barthel Index) before BMMC infusion and 1, 3, 7, 30, 60 and 120 days after. No patient
exhibited any complication or adverse events during the procedure. In six patients there was
no worsening in neurologic scales until the end of follow-up. One patient needed surgery (not
related to the BMMC infusion) one week after the procedure. He had a new ischemic stroke.
Whole-body scans and SPECT obtained two hours after infusion of labeled BMMCs showed
uptake in the brains of all patients. Due to the six-hour half-life of 99mTc, the brain uptake at
24h after cell infusion couldn’t be visualized in all patients. All the patients remained
monitored even after the end of follow-up (120 days) and two patients had generalized
seizures, 200 days after cell infusion. In spite of that, the scales evaluated remained the same
of the 120th day. In this small phase 1 pilot study, BMMC intra-arterial injection in patients
with sub-acute ischemic strokes proved feasible and safe. The fraction of labeled BMMC
stayed in the ischemic area for at least 24 hours in some patients. Phase II studies with more
patients are required to further evaluate efficacy and safety of BMMC transplantation in
patients with ischemic stroke.

LISTA DE FIGURAS
Figura 1: Fisiopatologia simplificada da lesão induzidapelo AVC, reparo endógeno e regeneração 17
Figura 2: Penumbra isquêmica 17
Figura 3: Paciente 1 - Imagens SPECT 2h após infusão CMMO 40
Figura 4: Paciente 1 - Imagens corpo inteiro 2h após infusão CMMO 41
Figura 5: Paciente 1 - Imagens de corpo inteiro 24h após infusão CMMO 42
Figura 6: Paciente 2 - Imagens SPECT 2h após infusão CMMO 43
Figura 7: Paciente 2 - Imagens corpo inteiro 2h após infusão CMMO 44
Figura 8: Paciente 2 - Imagens corpo inteiro 24h após infusão CMMO 45
Figura 9: Paciente 3 - Imagens SPECT 2h após infusão CMMO 46
Figura 10: Paciente 3 - Imagens corpo inteiro 2h após infusão CMMO 47
Figura 11: Paciente 3 - Imagens corpo inteiro 24h após infusão CMMO 48
Figura 12: Paciente 3 - Imagem cerebral 24h após infusão CMMO 49
Figura 13: Paciente 4 - Imagens SPECT 2h após infusão CMMO 50
Figura 14: Paciente 4 - Imagens corpo inteiro 2h após infusão CMMO 51
Figura 15: Paciente 4 - Imagens corpo inteiro 24h após infusão CMMO 52
Figura 16: Paciente 5 - Imagens corpo inteiro 2h após infusão CMMO 53
Figura 17: Paciente 5 - Imagens corpo inteiro 24h após infusão CMMO 54
Figura 18: Paciente 6 - Imagens SPECT 2h após infusão CMMO 55
Figura 19: Paciente 6 - Imagens corpo inteiro 2h após infusão CMMO 56
Figura 20: Paciente 6 - Imagens corpo inteiro 24h após infusão CMMO 57
Figura 21: Paciente 7 - Imagens cerebrais 2h após infusão CMMO 58
Figura 22: Paciente 7 - Imagens corpo inteiro 2h após infusão CMMO 59

LISTA DE QUADROS, TABELAS E GRÁFICOS
Quadro 1: Protocolo de acompanhamento 34
Tabela 1: Características gerais dos pacientes 36
Quadro 2: Celularidade do material infundido 38
Tabela 2: Escala de AVC do Instituto Nacional Americano de Saúde(sigla em inglês, NIHSS) da amostra 60
Tabela 3: Índice de Barthel dos pacientes 60
Tabela 4: Escala modificada de Rankin dos pacientes 61
Gráfico 1: NIHSS (abscissa) x Dias após infusão (ordenada) 61

LISTA DE ABREVIATURAS
99m MetaestávelACM Artéria Cerebral MédiaAIT Ataque Isquêmico TransitórioAVC Acidente Vascular CerebralCEP Comissão de Ética em PesquisaCMMO Células Mononucleares da Medula ÓsseaCONEP Comissão Nacional de Ética em PesquisaCTH Células-tronco HematopoiéticasCTM Células-tronco MesenquimaisECASS European Cooperative Acute Stroke StudyEEG EletroencefalogramaEMS European Motor ScaleESS European Stroke ScaleFC Fragment crystallizableFDA Food and Drug AdministrationFWHM Full Width at Half-maxGCSF Granulocyte Colony-stimulating FactorGRID Gadolinium Rhodamine DextranHMG HemogramaHUCFF Hospital Universitário Clementino Fraga FilhoIB Índice de BarthelMIE Membro Inferior EsquerdoMHC Major Histocompatibility ComplexMO Medula ÓsseaNIHSS National Institute of Health Stroke ScaleNINDS National Institute of Neurological Disorders and StrokeNK Natural KillerPET Positron EmissionTomographyRM Ressonância Magnéticart-PA recombinant tissue Plasminogen ActivatorSPECT Single Photon Emission Computed TomographyTC Tomografia ComputadorizadaTCA Tempo de Coagulação AtivadoTCE Traumatismo CrânioencefálicoTRM Traumatismo RaquimedularUFRJ Universidade Federal do Rio de Janeiro

SUMÁRIO
1 INTRODUÇÃO 14
2 REVISÃO CRÍTICA DA LITERATURA 16
2.1 ACIDENTE VASCULAR CEREBRAL (AVC) 16
2.2 CÉLULAS-TRONCO 19
2.2.1 Conceito 19
2.2.2 Aplicações 21
2.2.3 Estudos experimentais/ clínicos 23
2.2.3.1 Células-tronco na cardiologia 23
2.2.3.2 Células-tronco para reparo muscular e ósseo 23
2.2.3.3 Células-tronco para doenças da pele 24
2.2.3.4 Células-tronco na neurologia 24
3 OBJETIVOS 28
3.1 OBJETIVO GERAL 28
3.2 OBJETIVOS ESPECÍFICOS 28
4 PACIENTES E MÉTODOS 29
4.1 PACIENTES 29
4.2 INTERVENÇÃO 30
4.2.1 Admissão hospitalar (D0) 30
4.2.2 Aspirado da medula óssea (D1) 30
4.2.3 Separação das células 31
4.2.4 Marcação das CMMO com radioisótopo 31
4.2.5 Infusão das células 32
4.2.6 Acompanhamento durante internação (D1 a D3) 32
4.2.7 Acompanhamento após a alta hospitalar 33
4.3 ANÁLISE ESTATÍSTICA 34
4.4 MONITORIZAÇÃO DE EFEITOS ADVERSOS 34

5 RESULTADOS 35
5.1 CARACTERÍSTICAS DA AMOSTRA 35
5.2 SEGURANÇA DO PROCEDIMENTO 37
5.3 CELULARIDADE DO MATERIAL INFUNDIDO 38
5.4 IMAGENS 39
5.4.1 Paciente 1 40
5.4.2 Paciente 2 43
5.4.3 Paciente 3 46
5.4.4 Paciente 4 50
5.4.5 Paciente 5 53
5.4.6 Paciente 6 55
5.4.7 Paciente 7 58
5.5 ESCALAS DE AVALIAÇÃO 60
5.6 PARÂMETROS LABORATORIAIS 62
6 DISCUSSÃO 63
7 CONCLUSÃO 67
REFERÊNCIAS 68
ANEXOS 76

1 INTRODUÇÃO
O AVC é a terceira causa de morte em países desenvolvidos (MURRAY; LOPEZ,
1997) e a principal causa de morte em alguns países em desenvolvimento (WU et al, 2001),
incluindo o Brasil (ANDRÉ et al, 2006). O AVC permanece a principal causa de incapacidade
no mundo: pelo menos 30% dos sobreviventes a um AVC têm recuperação incompleta e
outros 20% necessitam de assistência com as atividades de vida diária (BONITA;
SOLOMON; BROAD, 1997). Embora alguns fatores no tratamento do AVC agudo, como as
Unidades de AVC e o uso dos trombolíticos, possam melhorar o prognóstico dos pacientes, há
poucos estudos clínicos avaliando formas efetivas de melhorar a incapacidade residual
(CRAMER, 2008). Nos últimos anos, muitos estudos investigaram o potencial papel
restaurador de células-tronco, de diferentes fontes, em modelos animais de isquemia cerebral
(MENDEZ-OTERO; de FREITAS; MENDONÇA; ANDRÉ, 2007). Estes estudos mostraram
que a administração de células-tronco melhora a perda funcional observada após isquemia,
tornando o transplante destas células uma abordagem atrativa para restaurar a função cerebral
após AVC em humanos.
Duas instituições brasileiras diferentes (estudos clínicos fase 1) avaliaram a segurança
do transplante autólogo de células-tronco nos primeiros dez dias após AVC isquêmico
(MENDONÇA et al, 2006; de FREITAS et al, 2006). Vinte e seis pacientes (soma dos dois
estudos) com infarto no território da ACM receberam transplante autólogo de CMMO, por via
intra-arterial. Um paciente apresentou deterioração neurológica durante arteriografia cerebral,
porém antes da injeção das células-tronco. Os pacientes tratados não exibiram piora clínica e
nem lesões novas apareceram na avaliação sequencial por Ressonância Magnética (RM) de
crânio, incluindo imagem pesada em difusão. Estes estudos sugeriram que o transplante
autólogo de CMMO, via intra-arterial, é seguro nos primeiros dez dias após AVC isquêmico.
O transplante de células-tronco, após a fase aguda de uma isquemia cerebral, apresenta
alguns obstáculos. A formação de tecido cicatricial e a restauração da barreira
hematoencefálica podem afetar de forma adversa as células implantadas. Poucos modelos de
estudos animais em AVC investigaram transplante de células-tronco, meses após o infarto
(SAVITZ et al, 2002). Entretanto, há alguns estudos clínicos fase 1 e 2 que avaliaram
pacientes com AVC isquêmico crônico e transplante de células-tronco nessa fase, incluindo
pacientes até mesmo 10 anos após o evento isquêmico (KONDZIOLKA et al, 2000, 2005;

SAVITZ et al, 2005; BANG et al, 2005) e dois desses estudos utilizaram células derivadas de
teratocarcinoma humano (KONDZIOLKA et al, 2000, 2005; SAVITZ et al, 2005) e células
porcinas (SAVITZ et al, 2005), que podem provocar respostas graves de rejeição. Bang e
colaboradores examinaram a segurança e eficácia de células-tronco mesenquimais (CTM),
autólogas, expandidas em cultura e administradas via intravenosa em dois momentos: a
primeira infusão entre quatro e cinco semanas e a segunda entre sete e nove semanas após o
início dos sintomas (BANG et al, 2005). Os cinco pacientes que receberam essas células não
apresentaram efeitos adversos e tiveram melhora clínica em três e seis meses, comparados ao
grupo controle. Nesse estudo, as células da medula óssea eram cultivadas por várias semanas
antes do transplante, o que pode aumentar o risco de contaminação. Além disso, nenhum
desses estudos avaliou a cinética das células in vivo.
Baseado no exposto acima, desenhamos um estudo clínico fase I para avaliação da
segurança e exequibilidade da infusão de células mononucleares autólogas da medula óssea,
em pacientes com AVC isquêmico ocorrido em até 90 dias antes da infusão. Em todos os
pacientes do estudo uma parte das células a serem injetadas foram marcadas com tecnécio-99-
m para avaliação da cinética das CMMO após a injeção.

2 REVISÃO CRÍTICA DA LITERATURA
2.1 ACIDENTE VASCULAR CEREBRAL (AVC):
AVC é a terceira causa de morte e é a maior causa de incapacidade em países em
desenvolvimento (ANDRÉ et al, 2006). A incidência de AVC varia entre os países e aumenta
exponencialmente com a idade. Nas sociedades ocidentais, aproximadamente 80% dos casos
são causados por isquemia cerebral focal devido à oclusão arterial e os outros 20%, causados
por hemorragias (FEIGIN et al, 2003).
A fisiopatologia tanto do AVC isquêmico quanto do hemorrágico tem sido muito
estudada. Um grande número de eventos celulares e metabólicos se segue após a injúria
cerebral (Fig. 1). Os mecanismos fisiopatológicos da isquemia cerebral e suas interações são
muito complexos. Inicialmente, a porção central da lesão com perfusão muito baixa é cercada
por uma área de disfunção causada por distúrbios iônicos e metabólicos, mas com integridade
estrutural preservada, a penumbra isquêmica (Fig. 2). Entretanto, após essa fase dramática de
injúria inicial, a lesão continua a crescer muitas horas e até dias após o início da isquemia.
Dependendo do grau de fluxo sanguíneo residual e da duração da isquemia, a penumbra irá,
eventualmente, ser incorporada ao infarto, se não ocorrer reperfusão (van der WORP; van
GIJN, 2007). Portanto, quando um vaso arterial cerebral oclui, uma complexa cascata de
eventos ocorre. Células despolarizam e edemaciam, aminoácidos excitatórios e íons potássio
são liberados, enquanto os níveis de íons cálcio intracelular elevam-se rapidamente
(excitotoxicidade). Alguns mecanismos de isquemia cerebral podem ter tanto ações benéficas
quanto deletérias: (a) inflamação e interação imune-mediada, que contribuem para a expansão
da lesão, mas também são instrumentos de contenção do crescimento da lesão e reparo; o
desfecho do AVC é modulado pela interação do cérebro lesado com o sistema imune; (b)
glutamato, que tem papel importante na excitotoxicidade, mas que também é essencial para a
função cerebral normal e reorganiza a sinaptogênese após a injúria; (c) óxido nítrico,
produzido pela óxido-nítrico sintetase em resposta à injúria e que pode aumentar o fluxo
sanguíneo neuronal, mas também resulta no aumento de radicais livres. Portanto, o contexto
celular, o tempo e a intensidade do estímulo são importantes para determinar se uma mesma
molécula está em uma via de sinalização ou destruição e reparo (ENDRES et al, 2008).

Figura 1: Fisiopatologia simplificada da lesão induzida pelo AVC, reparo endógeno eregeneração. Adaptada com permissão de Dr. Ulrich Dirnagl, do artigo “Improving outcome after stroke: overcoming the translationalroadblock. Cerebrovas Dis 2008;25:269”.
Figura 2: Penumbra isquêmica. Adaptada com permissão de Dr. Ulrich Dirnagl, do artigo “Pathobiology of ischemic stroke:an integrated view. Trend neurosci 1999;22:394”.

Baseado na duração dos sintomas, as isquemias podem ser transitórias ou permanentes
(ataque isquêmico transitório [AIT] ou AVC, respectivamente). AIT é um déficit neurológico
temporário, sem piora evolutiva, de início súbito, atribuído à isquemia focal do cérebro, retina
ou cóclea, e que dura menos que 24 horas. Entretanto, a maioria dos AITs dura de cinco a 20
minutos. Sintomas com duração maior que 24 horas são considerados AVC isquêmicos
(BILLER; LOVE; SCHNECK, 2008).
No atendimento emergencial ao paciente com sintomas sugestivos de isquemia
cerebral, o déficit neurológico deve ser investigado por um exame neurológico cuidadoso. A
escala de AVC do Instituto Nacional de Saúde Americano – NIHSS (do inglês, National
Institute of Health Stroke Scale) (BROTT et al, 1989) é a escala mais utilizada para
quantificar a gravidade do déficit. O infarto cerebral não pode ser distinguido, com certo grau
de certeza, de hemorragia intracerebral com base nos sinais e sintomas somente. Em todos os
pacientes com suspeita de AVC isquêmico, tomografia computadorizada (TC) ou RM de
crânio deve ser realizada. A TC sem contraste é suficiente, pois tem alta sensibilidade para
hemorragia intracraniana (van der WORP; van GIJN, 2007).
Tratamento trombolítico intravenoso com ativador do plasminogênio tecidual
recombinante (sigla em inglês rt-PA), iniciado nas primeiras três horas após o início dos
sintomas, é a única terapia clínica atualmente disponível para o AVC isquêmico agudo. Um
estudo de AVC multicêntrico, randomizado (National Institute of Neurological Disorders and
Stroke Recombinant Tissue Plasminogen Activator – NINDS rt-PA) utilizando 0,9 mg/Kg de
peso de rt-PA, iniciado nas primeiras três horas após o início dos sintomas, demonstrou
probabilidade 30% maior de ter incapacidade mínima ou nenhuma incapacidade em três
meses, quando comparado com placebo (THE NINDS STUDY GROUP, 1995). Dois estudos
europeus, European Cooperative Acute Stroke Study (ECASS) e ECASS II, investigaram um
tempo maior para o uso do trombolítico após o início dos sintomas (seis horas), mas estes
estudos falharam em mostrar eficácia (HACKE et al, 1995 e 1998). Em 2008 foram
publicados os resultados do ECASS III, onde era utilizado rt-PA intravenoso entre três e
quatro horas e meia após o início dos sintomas, ocorrendo modesta, mas significativa melhora
no desfecho clínico, sem níveis maiores de hemorragia intracraniana do que o relatado
previamente entre pacientes tratados nas primeiras três horas. Entretanto, o tratamento
precoce permanece essencial. A significância do efeito da trombólise é tempo-dependente. O
tempo “porta-agulha” (chegada ao hospital ao início da infusão intravenosa de rt-PA)
permanece importante e deve ser o mais curto possível para aumentar a chance de um

desfecho melhor (HACKE et al, 2008). Portanto, devido ao curto tempo para o tratamento,
poucos pacientes recebem esta terapia.
Reduzir o risco de eventos aterotrombóticos futuros, em pacientes com história de
AVC isquêmico, tem um papel importante na terapêutica. Devem-se utilizar agentes
antiplaquetários, inibidores da 3-hidroxi-3metilglutaril coenzima-A redutase (estatinas) e anti-
hipertensivos, bem como adoção de alterações no estilo de vida (LUTSEP, 2009).
Conforme revisado por Mendez-Otero, numerosos estudos pré-clínicos e clínicos têm
sido realizados nas últimas décadas, em busca de um agente neuroprotetor para tratar os
pacientes com AVC isquêmico (MENDEZ-OTERO et al, 2007). Neuroproteção é qualquer
estratégia ou combinação de estratégias que antagonizam, interrompem ou diminuem a
sequência de eventos bioquímicos e moleculares da lesão que, caso não realizados, levariam à
injúria isquêmica irreversível (GINSBERG, 2008). Entretanto, nenhuma das drogas testadas,
até o momento, embora efetivas em estudos animais, foi eficaz em seres humanos e, portanto,
novas estratégias devem ser desenvolvidas para evitar morte neuronal e/ou restauração da
função cerebral lesada, após um AVC (MENDEZ-OTERO; de FREITAS; MENDONÇA;
ANDRÉ, 2007 e SHUAIB et al, 2007).
2.2 CÉLULAS-TRONCO:
2.2.1 Conceito:
Células-tronco são células autorrenováveis, não-diferenciadas, capazes de produzir
grande número de células diferenciadas. A característica que distingue as várias populações
de células-tronco é seu potencial para gerar diversos tipos de células especializadas. Em
outras palavras, as células-tronco podem ter características totipotenciais, pluripotenciais,
bipotenciais ou unipotenciais. O zigoto é um exemplo de células totipotenciais, pois tem
capacidade de gerar outro organismo. As células embrionárias (derivadas diretamente da
massa celular interna do embrião pré-implantação no estágio de blastocisto) representam a
população de células pluripotenciais, porque elas podem gerar todos os tecidos de um
organismo, mas não outro organismo (pois não geram a placenta e nem folhetos
extraembrionários). Usualmente, as células-tronco pluripotentes são definidas como células
que dão origem às três camadas germinativas: ectoderma (pele, tecido neural), mesoderma
(sangue, tecido adiposo, cartilagem, osso ou músculo) e endoderma (células do sistema
respiratório e digestivo). Células multipotentes são capazes de diferenciar-se em tipos

celulares múltiplos, mas dentro de certa linhagem (Ex: células-tronco hematopoiéticas,
diferenciando-se em hemácias, leucócitos e plaquetas), ou seja, com potencial mais limitado
(exemplo: sangue do cordão umbilical). O mioblasto representa um precursor de uma célula
unipotente. Ele é capaz de gerar somente um tipo celular (FILIP et al, 2008).
Células-tronco que têm pluripotência similar ou igual às células-tronco embrionárias
também podem ser derivadas de células germinativas, isto é, células germinativas
embrionárias, células de carcinoma embrionário (de tumores testiculares adultos) e células de
linhagem germinativa derivadas de células-tronco espermatogoniais ou de células de
superfície de ovários adultos. As células-tronco persistem na vida adulta, mas o dogma tem
sido se estas células-tronco adultas são mais restritas em sua capacidade de diferenciar e,
também, se são somáticas ou órgão-específicas (BELLEHSEN; NAGLER; LEVI-
SCHAFFER, 2008).
As células-tronco adultas multipotentes (células indiferenciadas) residem com células
diferenciadas nos seus tecidos de origem, com nomenclatura correlacionada. As células
progenitoras e as células-tronco adultas têm um papel reparativo, repondo as células e
mantendo ciclo normal dos órgãos regenerativos, como o sangue, pele ou tecido intestinal
(FARIN et al, 2009). As células do estroma mesenquimal adulto são células multipotentes e
indiferenciadas, as quais residem, primariamente, na medula óssea e têm potencial de
diferenciar-se em múltiplos fenótipos esqueléticos, como osteoblastos, condrócitos,
adipócitos, células do estroma, fibroblastos e, possivelmente, tendões. No corpo humano, elas
podem ser vistas como reservatórios disponíveis de células reparadoras, capazes de mobilizar-
se, proliferar-se e diferenciar-se ao tipo celular apropriado em resposta a sinais específicos
(CAPLAN, 2007).
Um nicho de células-tronco pode ser definido como um sítio específico ou reservatório
definido, composto não somente de células de suporte, mas também de glicoproteínas da
matriz organizadas em uma matriz funcional tridimensional. O contato entre esses elementos
permite interações moleculares e sinalizadoras que são cruciais para a regulação da
quiescência das células-tronco, autorrenovação, diferenciação e proliferação, bem como
fatores que influenciam a mobilização e homing da progenitora. A regulação da
autorrenovação e diferenciação das células-tronco adultas é crucial para a manutenção da
homeostase tecidual. Portanto, a estrutura do nicho não somente providencia um ambiente
propício à célula-tronco, mas também determina o estado apropriado regulado por
mecanismos intrínsecos e moleculares (MORRISON; SPRADLING, 2008). Células-tronco
adultas e seus nichos têm sido identificados em diferentes tipos de tecidos em mamíferos,

incluindo o sistema hematopoiético, sistema epitelial, sistema intestinal e sistema nervoso (LI;
XIE, 2005).
Em estado de repouso, a grande maioria das células-tronco hematopoiéticas (CTH) é
quiescente, com somente uma fração dessas células entrando em um estado cíclico para
proliferar e dar origem às “células-filhas”, que ir-se-ão proliferar e diferenciar como
progenitoras de linhagens de células sanguíneas maduras. Tem sido estimado que bilhões de
células sanguíneas sejam produzidas, a cada hora, em um organismo humano adulto saudável,
durante a vida e, na maioria das circunstâncias, essa enorme produção é balanceada por perda
celular programada, mantendo o número de células circulantes relativamente constante.
Entretanto, quando ocorre estresse sistêmico como infecção, sangramento agudo ou
quimioterapia, as CTH são recrutadas a responder com proliferação extensa, para manter
progenitores suficientes, suprindo a necessidade das células sanguíneas (BRYDER; ROSSI;
WEISSMAN, 2006).
2.2.2 Aplicações:
Transplante de CTH refere-se a qualquer procedimento onde células hematopoiéticas
serão fornecidas para um receptor, com a intenção de repovoar ou substituir o sistema
existente, em parte ou no total. Tradicionalmente, o transplante de CTH é realizado após um
regime de alta dose de quimioterapia, com ou sem irradiação, para ablação da medula óssea e
das células tumorais. Células-tronco colhidas são, então, transfundidas para repovoar a
medula e restaurar a competência hematológica e imunológica. O transplante de CTH repõe o
termo antigo utilizado “transplante de medula óssea” para indicar a gama de fontes de células
doadoras disponíveis: medula óssea, células-tronco periféricas e sangue do cordão umbilical.
As células-tronco podem ter origem no próprio paciente (autólogas), num gêmeo idêntico –
singênica - ou em um doador – halogênica (JAGANNATHAN et al, 2008).
O uso de terapias imunes e celulares para tratar doenças hematológicas vem sendo
estabelecido. Nos últimos 50 anos, o transplante de células hematopoiéticas desenvolveu-se
em terapia curativa para uma variedade de estados de falência da medula óssea, malignidades
hematológicas, imunodeficiências e erros inatos do metabolismo. Observação do efeito tumor
contra enxerto vem providenciando fundamento para o tratamento de malignidades
hematológicas com infusão de leucócitos do doador que exploram a resposta halogênica dos
linfócitos T do doador, e experimentos com infusão de outras populações celulares efetoras
halogênicas como as células natural killer (NK). Durante esta era, investigadores têm feito

acentuado progresso para doadores alternativos para transplante e medidas para prevenir e
tratar doença enxerto contra hospedeiro e infecções (McGLAVE, 2008).
As CTH possuem propriedades únicas que têm permitido, no contexto do transplante
de medula óssea, ser o único tipo de célula-tronco no uso clínico rotineiro. Primeiro: embora a
maioria das CTH normalmente residam no espaço extravascular na medula óssea, também
possuem incrível habilidade de retornar a seus nichos após injeção na circulação venosa. Esta
habilidade de recircular parece estar ligada às propriedades naturais das CTH, pois elas
migram entre a medula óssea, o sangue, a linfa e órgãos extramedulares em condições
fisiológicas. Portanto, as CTH podem ser injetadas endovenosamente ao invés de diretamente
na medula do recipiente, tornando seu uso clínico relativamente fácil. Segundo: aumentando a
propriedade circulatória das CTH usando agentes farmacológicos como fator estimulador das
colônias de granulócitos (sigla em inglês, GCSF) pode-se obter, rotineiramente, CTH do
sangue periférico de doadores saudáveis ao invés de obtê-las da medula óssea (procedimento
mais invasivo). Finalmente, CTH expressam uma combinação única de marcadores de
superfície celular que permitem sua purificação (BHATTACHARYA; EHRLICH;
WEISSMAN, 2008).
Um grande número de barreiras clínicas, entretanto, permanece, dificultando o uso
rotineiro do transplante de medula óssea para o tratamento das doenças hematológicas, como
toxicidade do regime usual pré-transplante autólogo de CTH e complicações da doença
enxerto contra hospedeiro (HAROUSSEAU, 2007).
Indicações estabelecidas (JAGANNATHAN et al, 2008):
- Doenças malignas:
a) Mieloma Múltiplo;
b) Linfoma não – Hodgkin;
c) Linfoma de Hodgkin;
d) Leucemia Mielóide Aguda;
e) Síndrome Mielodisplásica;
f) Leucemia Linfoblástica Aguda;
g) Leucemia Mielóide Crônica;
h) Leucemia Linfocítica Crônica;
i) Neuroblastoma, tumores de células germinativas e outras malignidades sólidas.
- Doenças não-malignas:
(A) Talassemia;
(B) Anemia falciforme

(C) Anemia aplástica
(D) Algumas desordens genéticas e imunológicas.
2.2.3 Estudos experimentais/ clínicos:
O uso de populações de células progenitoras e de células-tronco diferentes de CTH
para reparar tecidos de origem, bem como outros tecidos, está em intensa fase de
investigação.
2.2.3.1 Células-tronco na cardiologia: a ideia de reparar o tecido cardíaco usando diferentes
tipos de células-tronco tem levado a diferentes estudos experimentais. Esforços são feitos para
restaurar a função do coração lesado com transplante de células-tronco não-residentes, como
cardiomiócitos fetais, células-tronco embrionárias, células musculares esqueléticas, CTM
derivadas da medula óssea ou células-tronco derivadas do tecido adiposo (LAFLAMME;
MURRY, 2005). Diferentemente das células-tronco embrionárias, não há evidência
convincente que células de tecidos pós-natal outros que não o coração, possam gerar
cardiomiócitos funcionais in vivo. Estudos clínicos têm sugerido que somente 1,3 a 2,6% das
células-tronco derivadas da medula óssea ficam retidas no coração. Benefícios funcionais
também podem ser mediados através da secreção parácrina de fatores de crescimento ou
citocinas, as quais podem, indiretamente, promover a sobrevida dos cardiomiócitos,
mobilização de células progenitoras endógenas ou neovascularização (ROSENZWEIG,
2006).
2.2.3.2 Células-tronco para reparo muscular e ósseo: a capacidade regenerativa da
musculatura esquelética é atribuída às células-tronco musculares, também conhecidas como
células satélite. Atualmente é bem aceito que as CTM constituem uma fonte de progenitores
de tecidos derivados do mesoderma, como osso, cartilagem e gordura. Essas CTM
multipotentes podem ser isoladas baseadas nas suas propriedades plásticas e de aderência e
podem ser expandidas em culturas, de forma relativamente fácil. O reconhecimento de seu
potencial terapêutico é um avanço importante na terapia celular: está bem estabelecido seu
uso no reparo tecidual ósseo (reparo de defeitos ósseos segmentares de tamanho crítico em
animais, restaurar cicatrização de fraturas de ossos longos nos seres humanos ou tratar ossos
de crianças com osteogênese imperfeita), pouco se sabendo a respeito das vias de sinalização
e determinantes moleculares envolvidos na diferenciação miogênica das CTM (GARCIA-
CASTRO et al, 2008).

2.2.3.3 Células-tronco para doenças da pele: terapias celulares com queratinócitos têm sido
praticadas com sucesso. Reconstituição da barreira epidérmica funcional com regeneração da
derme papilar tem sido realizada com camadas epidérmicas autólogas em pacientes com
queimaduras de pele, bem como em outras doenças de pele (PROSPER; VERFAILLIE,
2008).
O uso de células-tronco como material básico na engenharia tecidual tem o potencial
de melhorar desfechos clínicos tanto em cicatrização de feridas e em terapia genética para
doenças cutâneas e sistêmicas. Estudos de engenharia tecidual de pele têm mostrado que
células-tronco epidérmicas podem fornecer uma fonte superior de células-tronco
multipotentes para engenharia tecidual. Entretanto, avanços na engenharia tecidual de pele são
necessários para a aplicação clínica (CHARRUYER; GHADIALLY, 2009).
2.2.3.4 Células-tronco na neurologia: o ponto-chave no tratamento das doenças
neurológicas é que o processo de lesão neuronal é frequentemente irreversível, porque os
neurônios do cérebro e da medula espinhal são incapazes de regenerar espontaneamente
(EINSTEIN; BEN-HUR, 2008).
Embora tenha sido sugerido que possa haver transdiferenciação das CTM em células
de linhagem neural in vitro , nenhum grupo ainda observou que as CTM dão origem a
neurônios completamente diferenciados e funcionais. A maioria dos dados atuais indica que
fatores bioativos (neurotrofinas e fatores de crescimento), secretados pelas CTM, em resposta
ao ambiente local, são os responsáveis pelos efeitos restauradores das CTM (LI; CHOPP,
2009).
a) No traumatismo crânio-encefálico (TCE): modelos experimentais demonstraram
que as CTM derivadas de ratos doadores transplantadas no cérebro de roedores, intracerebral
(MAHMOOD et al, 2002), intra-arterial (LU et al, 2001a) ou intravenoso (LU et al, 2001b) -
com TCE induzido por contusão, melhorou significativamente o desfecho neurológico. Um
estudo Fase I, que avaliará a infusão intravenosa de células autólogas, mononucleares,
derivadas da medula óssea de crianças após TCE grave, está em andamento (NCT 00254722).
b) Na lesão de medula espinhal: uma das terapias celulares que vem sendo estudada
para lesões na medula espinhal é o transplante de células gliais do bulbo olfatório na tentativa
de restabelecer conexões através da cicatriz glial. Nesta terapia, o objetivo não é o de
substituir neurônios perdidos, mas permitir o crescimento axonal através da cicatriz de glia.
(MENDEZ-OTERO et al, 2007). Estudos publicados em traumatismo raqui-medular (TRM)

têm encontrado efeitos positivos na administração local de células-tronco derivadas da medula
óssea, comparado à administração endovenosa (SYKOVA et al, 2006).
c) Na Doença de Parkinson: modelos de parkinsonismo têm sido estudados mais
extensivamente do que qualquer outra doença neurológica degenerativa (MEZEY, 2007).
Transplante de células-tronco derivadas da medula óssea melhorou a função motora em
modelo animal de Doença de Parkinson (LI et al, 2001).
d) Células-tronco em AVC isquêmico: estudos experimentais têm demonstrado que o
transplante de CTM facilitam os mecanismos de neuro-restauração endógenos, incluindo
redução da apoptose (CHEN et al, 2003a), e promoção do remodelamento glial, neuronal (LI
et al, 2005 e SHEN et al, 2007), e vascular (CHEN et al, 2003b), não sendo esses eventos
mutuamente exclusivos. Uma revisão recente mostrou que muitos estudos evidenciaram, em
modelos animais variados de AVC isquêmico, melhora na recuperação funcional dos animais.
Foram utilizadas CTM e/ou células da medula óssea (MEZEY, 2007).
Baseado nesses resultados, Bang e colaboradores examinaram a segurança,
exequibilidade e eficácia da terapia celular usando CTM autólogas, expandidas em cultura,
em pacientes com AVC isquêmico. Concluíram que, em pacientes com infarto cerebral grave,
a infusão endovenosa de CTM autólogas parece ser segura e exequível e pode melhorar a
recuperação funcional do paciente (BANG et al, 2005).
Outro estudo clínico, fase I, observou pacientes com AVC isquêmico agudo (entre três
e dez dias após o início dos sintomas), realizando infusão intra-arterial (via artéria femoral) de
células mononucleares autólogas da medula óssea, com resultados preliminares demonstrando
segurança e exequibilidade (de FREITAS et al, 2006).
Dados limitados existem a respeito do uso de células exógenas em pacientes que
tiveram AVC isquêmico. A segurança e viabilidade do transplante intracerebral de células
neuronais culturadas foi estabelecido em dois estudos utilizando neurônios da Layton Bio
Science – LBS (KONDZIOLKA et al, 2000 e 2005). Entretanto, apesar de haver melhora no
déficit motor dos pacientes, traduzindo-se em melhora na capacidade de algumas atividades
de vida diária, o estudo fase 2 não encontrou evidência de benefício significativo na função
motora, que era o objetivo primário do estudo (KONDZIOLKA et al, 2005).
Investigadores de Boston avaliaram a segurança do transplante de células fetais suínas
através de cirurgia estereotáxica em cinco pacientes na fase crônica (três meses a dez anos
antes) do AVC isquêmico acometendo os gânglios da base (SAVITZ et al, 2005). As células

foram retiradas da eminência gangliônica lateral, que são derivadas do striatum primitivo.
Para evitar rejeição, as células foram tratadas antes do transplante com um fragmento F (ab’)2
contra o Complexo Maior de Histocompatibilidade (sigla em inglês, MHC) classe I sem a
região Fragment crystallizable (Fc). Os três primeiros pacientes não apresentaram efeitos
colaterais em um acompanhamento de quatro anos. O quarto paciente teve piora progressiva
da hemiparesia esquerda. A RM de crânio mostrou captação de contraste no lobo frontal
direito. Biópsia desse local mostrou necrose e inflamação sugestivas de infarto e o paciente
foi tratado com corticóide com boa reposta. Um comitê de avaliação independente considerou
o evento como sendo um infarto por uma oclusão venosa provavelmente secundária à
cirurgia. O quinto paciente teve crises convulsivas parciais complexas e generalizadas
atribuídas à hiperglicemia. A RM de crânio mostrou captação de contraste no lobo frontal
direito e na área de isquemia. Devido a esses efeitos adversos o estudo foi interrompido pelo
Food and Drug Administration - FDA (MENDEZ-OTERO et al, 2007).
Muitos ensaios utilizaram fatores tróficos para estudar a diminuição da incapacidade
dos pacientes com AVC isquêmico. Dentre eles, predominam os que utilizaram granulocyte
colony stimulating factor (G-CSF). Um estudo randomizado e cego de Shyu e colaboradores
(2006) avaliou a segurança e eficácia da administração subcutânea de G-CSF (15µg/Kg/dia)
por cinco dias, iniciando nos sete primeiros dias após o evento isquêmico, em 10 pacientes
com AVC no território da artéria cerebral média e com a escala de AVC do Instituto Nacional
de saúde americano (sigla em inglês NIHSS) entre 9 e 20. Os sete pacientes que receberam G-
CSF tiveram maior percentual de melhora neurológica entre avaliação inicial e 12 meses do
que os três pacientes do grupo controle (p. ex. 59% vs. 36% de melhora no NIHSS, p < 0,05).
Foram utilizadas quatro escalas nesta avaliação: NIHSS, Escala de AVC Européia (sigla em
inglês, ESS), Subescala Motora da ESS (sigla em inglês, EMS) e Índice de Barthel (sigla em
inglês, BI). Além disso, exame de tomografia por emissão de pósitrons (sigla em inglês, PET)
com fluordeoxiglicose mostrou melhora do metabolismo cerebral na área cortical peri-infarto
dos pacientes tratados em comparação com os pacientes do grupo controle. De forma
interessante, houve correlação entre o metabolismo cerebral avaliado pelo PET e a função
motora medida através da escala motora da ESS. Outro dado relevante foi que os pacientes
que receberam G-CSF no primeiro dia (D1) pós-AVC parecem ter tido maior recuperação do
que os que receberam numa fase mais tardia.
Baseado nos estudos experimentais e clínicos acima, desenhamos um estudo clínico
fase I para avaliação da segurança e exequibilidade da infusão de células mononucleares
autólogas da medula óssea, em pacientes com AVC isquêmico em território da artéria cerebral

média, com até 90 dias após o início dos sintomas. Estudamos, também, a cinética destas
células através de marcação com radioisótopo, abordagem ainda não feita no campo da
neurologia. A evolução, clínica e laboratorial, foi avaliada durante o seguimento do estudo,
sendo todos os eventos registrados e descritos.

3 OBJETIVOS
3.1 OBJETIVO GERAL
Avaliar a segurança e a exequibilidade do transplante autólogo de células
mononucleares marcadas da medula óssea em pacientes com AVC isquêmico no território da
artéria cerebral média, em até 90 dias após o AVC.
3.2 OBJETIVOS ESPECÍFICOS
• Descrever a cinética das células mononucleares autólogas derivadas da medula
óssea marcadas com radiotraçador, duas e 24 horas após infusão na artéria
cerebral média.
• Avaliar modificação dos parâmetros clínicos através de escalas de avaliação
motora e funcional e medir a variação de parâmetros hematológicos e
bioquímicos na corrente sanguínea ao longo do seguimento.
• Descrever os eventos adversos observados durante o seguimento.

4 PACIENTES E MÉTODOS
4.1 PACIENTES:
Este é um estudo clínico fase 1, unicêntrico, realizado no Hospital Universitário
Clementino Fraga Filho (HUCFF). O protocolo e o Termo de Consentimento Livre e
Esclarecido (TCLE) foram aprovados pela Comissão de Ética em Pesquisa do HUCFF (CEP
169/03) e pela Comissão Nacional de Ética em Pesquisa (Protocolo de Pesquisa nº 10385 –
CONEP), sob o título “Terapia celular pelo transplante autólogo de células-tronco de medula
óssea em pacientes com acidente vascular cerebral isquêmico”. Também foi registrado no
portal www.clinicaltrials.gov (NCT00473057). O TCLE foi obtido de todos os participantes.
Pacientes entre 18 e 75 anos de idade eram elegíveis para o estudo se tivessem as
seguintes características:
(1) AVC isquêmico em território da ACM, evidenciado por TC ou por RM, dentro de 90 dias
após os sintomas;
(2) recanalização da ACM envolvida, avaliada por estudo de Doppler transcraniano ou por
angio-ressonância de crânio;
(3) uma pontuação entre 4 e 17 no NIHSS;
(4) Assinatura do TCLE.
Foram excluídos pacientes que preenchessem qualquer dos seguintes critérios:
(a) dificuldade em obter acesso vascular para procedimento percutâneo;
(b) estenose de carótida maior que 50% ao estudo de Doppler (ipsilateral ao AVC);
(c) piora neurológica (maior do que 4 pontos no NIHSS) antes da injeção, devido a edema ou
hemorragia intracerebral;
(d) trombofilias ou doenças hematológicas primárias;
(e) desordens neurodegenerativas;
(f) AVC prévio com Escala modificada de Rankin maior que 2;
(g) trombo intracardíaco;
(h) desordens autoimunes;
(i) sepsis (de acordo com critérios definidos pela Sociedade de Terapia Intensiva e Colégio
Americano de Médicos Torácicos, de 1992);
(j) história de neoplasia ou outra doença associada que tivesse impacto na sobrevida do
paciente a curto prazo;

(k) qualquer condição que, no julgamento dos investigadores, poderia colocar o paciente sob
risco;
(l) desordens ósseas que pudessem aumentar o risco do procedimento de coleta de aspirado da
medula óssea;
(m) insuficiência hepática;
(n) insuficiência renal (creatinina sérica maior que 2 mg/mL);
(o) instabilidade hemodinâmica ou respiratória;
(p) AVC lacunar;
(q) gravidez;
(r) participação em outro ensaio clínico.
4.2 INTERVENÇÃO:
4.2.1 Admissão hospitalar (D0):
Os pacientes foram admitidos na véspera do procedimento, sendo esse considerado o
D0 de protocolo. Neste dia, o paciente foi submetido à avaliação clínica e visita pré-
anestésica. Foi realizada hidratação venosa com solução salina (1000 mL em infusão
contínua, 12 horas antes e 12 horas após o final da intervenção).
O uso prévio de medicações para hipertensão arterial sistêmica e diabetes era suspenso
apenas no dia da intervenção, devido ao jejum prolongado (cerca de 10 horas), retornando
após a infusão das CMMO.
4.2.2 Aspirado da medula óssea (D1):
Antes do encaminhamento ao centro cirúrgico, foram coletadas amostras de sangue
para exames laboratoriais e obtenção de soro autólogo para suspensão das CMMO. No centro
cirúrgico, os pacientes foram submetidos à sedação venosa, objetivando Escala de RASS -3
(ELY et al, 2003). As células foram obtidas com o paciente em decúbito ventral, após
anestesia local, através de aspirado de medula da crista ilíaca póstero-superior (cerca de 20
aspirações, sendo 10 em cada crista ilíaca), obtendo-se um volume total de 100 mL.
Procedimento este, realizado por um hematologista, conforme protocolo utilizado pelo
Serviço de Hematologia do HUCFF, baseado em um protocolo Iugoslavo (BATINIC et al,
1990). Após observação na Unidade de Recuperação Pós-Anestésica, o paciente foi
encaminhado ao quarto.

4.2.3 Separação das células:
O material proveniente da aspiração era, então, encaminhado ao Laboratório de
Marcação de Células e Moléculas do Serviço de Medicina Nuclear do HUCFF em 20 seringas
heparinizadas contendo 5 mL de aspirado de medula óssea (MO) em cada. Após filtração de
coágulos, gordura e espículas ósseas, foi iniciada a separação de células por centrifugação
(400xg) em gradiente de Ficoll-Hypaque. O anel contendo as CMMO foi diluído em albumina
a 5% e soro autólogo em um total de 20 mL, esperando-se uma contagem de 5 – 10 x 107
células (PERIN et al, 2003). Da solução contendo as CMMO, foram retiradas pequenas
alíquotas para:
� contagem celular;
� imunofenotipagem por citometria de fluxo em aparelho BD FACSCanto™ classe 1,
realizada no Laboratório de Terapia Celular do Instituto Nacional de Cardiologia de
Laranjeiras;
� culturas (germes comuns e fungos), encaminhadas ao Laboratório de Bacteriologia do
HUCFF;
� marcação celular com radioisótopo.
4.2.4 Marcação das CMMO com radioisótopo:
Uma alíquota (10%) da solução final contendo as CMMO foi incubada com 500 µl de
cloreto estanoso (SnCl2) em solução fisiológica de cloreto de sódio (NaCl 0,9%) por 10
minutos em temperatura ambiente, conforme técnica desenvolvida no Laboratório de
marcação de células e moléculas (LMCM) /UFRJ, para marcação com 99mtecnécio
(GUTFILEN et al, 1999). A seguir, as células foram incubadas por mais 10 minutos com 45
mCi de 99mTecnécio. Após centrifugação (500 x g por cinco minutos), o sobrenadante foi
removido e lavado novamente com solução salina. A viabilidade das células marcadas foi
avaliada pelo teste de exclusão vital com azul de trypan (CARVALHO et al, 2008; CORREA
et al, 2007). A eficiência da marcação (%) foi calculada pela atividade no precipitado (pellet)
dividida pela soma da radioatividade no precipitado mais o sobrenadante, multiplicado por
100. A viabilidade das células foi superior a 93% em todos os casos. As células marcadas
foram agregadas ao restante da suspensão de CMMO, sendo a solução (volume final: 10 mL)
transferida para uma seringa e encaminhada à Unidade de Hemodinâmica. O procedimento de
separação e marcação das células ocorreu em, aproximadamente, quatro horas. Todos os
procedimentos foram realizados em condições estéreis, em capela de fluxo laminar.

4.2.5 Infusão das células:
Esta solução foi injetada lentamente na artéria cerebral média do próprio paciente
(autóloga), ipsilateral ao AVC, através da técnica de Seldinger, via cateter introduzido na
artéria femoral, por um único hemodinamicista, especializado em arteriografia cerebral. A
técnica utilizada foi a coaxial de rotina, com punção de artéria femoral com cateter guia de
diâmetro 6 french (Envoy-Cordis, Miami, Fla ou Guider-Soft tip- Boston Scientific-Target
Therapeutics- Fremont, Califórnia), posicionado em nível cervical com infusão contínua de
solução salina. Os pacientes foram anticoagulados com heparina endovenosa para obter um
tempo de coagulação ativado (TCA) duas a três vezes o nível normal e todo o procedimento
foi monitorizado por arteriografia cerebral. Um microcateter de diâmetro interno maior (SL
1018 Boston Scientific – Target Therapeutics, Fremont, California) foi introduzido até a
porção M1 da ACM e a infusão foi realizada em, aproximadamente, 10 minutos. Pacientes
receberam entre 1,25 x 108 e 5 x 108 CMMO, e o procedimento demorou, em média, uma
hora. Anestesia local e sedação leve (Escala de RASS -1), esta procedida por anestesiologista
do Serviço de Hemodinâmica, foi realizada durante o procedimento.
4.2.6 Acompanhamento durante internação (D1 a D3):
Os pacientes foram submetidos à cintilografia de corpo inteiro e à tomografia
computadorizada com emissão de fóton único (sigla em inglês SPECT) no Serviço de
Medicina Nuclear do HUCFF, utilizando câmera Xeleris (General Electric Medical Systems,
Milwaukee, Wisconsin), duas e vinte e quatro horas após a infusão das CMMO, para avaliação
da localização das mesmas. Imagens de corpo inteiro (anterior e posterior) foram adquiridas
por 20 minutos, usando um explorador de duas cabeças de alta resolução e colimador de baixa
energia. As imagens planares foram adquiridas por 10 minutos, matriz 256 x 256, incidência
anterior, lateral direita e esquerda e posterior. O SPECT foi realizado com dois detectores de
rotação opostos com colimadores de alta resolução e baixa energia. O equipamento utilizado
para reconstrução da imagem (software e hardware) foi uma estação de trabalho processadora
GE-Xeleris, para reconstrução das imagens do SPECT. Projeções foram coletadas em 24
minutos, com cada detector usando rotação de 180° para completar 360° numa órbita circular
do crânio do paciente, em decúbito dorsal. Os volumes das imagens foram reconstruídos
usando o algoritmo OSEM com alisamento axial e filtro Butterworth com ordem de 5 e ponto
de corte 0,45. Volumes de imagens consistiram de 64 x 64 x 64 voxel cada um medindo 4,38
mm³. O detector de distância variou de 14 a 20 cm durante a rotação, resultando em resolução

espacial completa com full width at half-max (FWHM), de aproximadamente 12 mm. Para
cada paciente, a captação no cérebro, fígado, baço, pulmões, bexiga e corporal total foram
avaliados após a injeção celular em imagens planares. A percentagem de captação nos
hemisférios direito e esquerdo foi quantificada em imagens de SPECT para todos os
pacientes.
Avaliação clínica e laboratorial foi realizada após os exames cintilográficos e 48h após
a infusão das CMMO, onde os pacientes, estando em condições de alta, eram liberados do
hospital. Estas avaliações tinham o objetivo de detectar possíveis complicações imediatas do
procedimento. Também foram utilizadas escalas de avaliação motora e funcional: NIHSS,
Índice de Barthel (IB) e Escala modificada de Rankin (EmR).O Quadro 1 detalha todo o
protocolo de acompanhamento.
4.2.7 Acompanhamento após a alta hospitalar:
As avaliações de seguimento foram realizadas em 7, 30, 60, 90 e 120 dias após a
infusão das CMMO, por meio das escalas clínicas supracitadas e de testes laboratoriais de
rotina (hemograma completo e bioquímica), os quais eram realizados no laboratório de
análises clínicas do HUCFF. Um eletroencefalograma (EEG) foi realizado nos primeiros sete
dias após a infusão das CMMO, pelo Serviço de Neurologia do HUCFF.
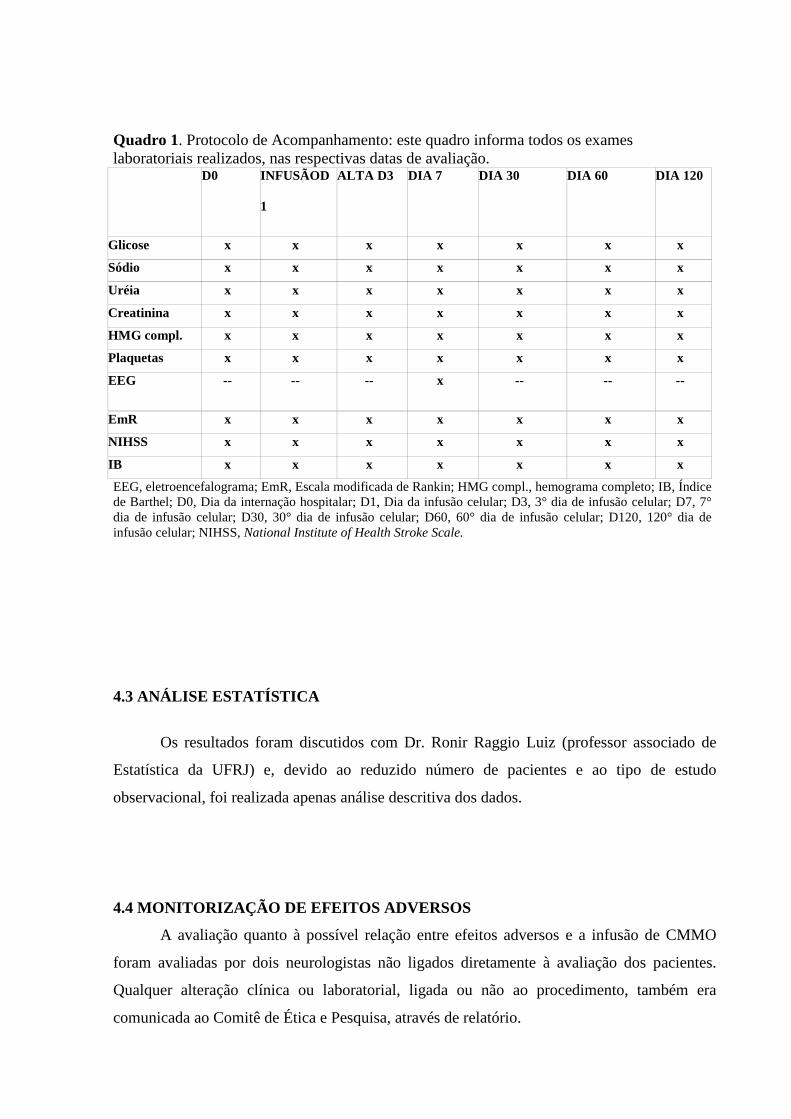
Quadro 1. Protocolo de Acompanhamento: este quadro informa todos os exameslaboratoriais realizados, nas respectivas datas de avaliação.
D0 INFUSÃOD
1
ALTA D3 DIA 7 DIA 30 DIA 60 DIA 120
Glicose x x x x x x x
Sódio x x x x x x x
Uréia x x x x x x x
Creatinina x x x x x x x
HMG compl. x x x x x x x
Plaquetas x x x x x x x
EEG -- -- -- x -- -- --
EmR x x x x x x x
NIHSS x x x x x x x
IB x x x x x x x
EEG, eletroencefalograma; EmR, Escala modificada de Rankin; HMG compl., hemograma completo; IB, Índicede Barthel; D0, Dia da internação hospitalar; D1, Dia da infusão celular; D3, 3° dia de infusão celular; D7, 7°dia de infusão celular; D30, 30° dia de infusão celular; D60, 60° dia de infusão celular; D120, 120° dia deinfusão celular; NIHSS, National Institute of Health Stroke Scale.
4.3 ANÁLISE ESTATÍSTICA
Os resultados foram discutidos com Dr. Ronir Raggio Luiz (professor associado de
Estatística da UFRJ) e, devido ao reduzido número de pacientes e ao tipo de estudo
observacional, foi realizada apenas análise descritiva dos dados.
4.4 MONITORIZAÇÃO DE EFEITOS ADVERSOS
A avaliação quanto à possível relação entre efeitos adversos e a infusão de CMMO
foram avaliadas por dois neurologistas não ligados diretamente à avaliação dos pacientes.
Qualquer alteração clínica ou laboratorial, ligada ou não ao procedimento, também era
comunicada ao Comitê de Ética e Pesquisa, através de relatório.

5 RESULTADOS:
5.1 CARACTERÍSTICAS DA AMOSTRA:
As características clínicas e radiológicas dos pacientes incluídos estão na Tabela 1,
sendo todos do sexo masculino. Dois pacientes estavam em uso de anticoagulante oral, que
foi trocado por heparina de baixo peso molecular subcutânea (enoxaparina 1 mg/Kg duas
vezes ao dia), uma semana antes do procedimento. Foram incluídos sete pacientes, no período
de dezembro de 2006 a maio de 2008.

Tabela 1: Características gerais dos pacientes: esta tabela informa as característicasclínicas e radiológicas dos pacientes antes da infusão das CMMO, bem como a avaliaçãodo NIHSS, IB e EmR no dia da infusão.
Pac 1 Pac 2 Pac 3 Pac 4 Pac 5 Pac 6 Pac 7
Sexo/
Idade
M/24 M/ 65 M/ 47 M/ 65 M/ 57 M/47 M/ 60
Fator de
risco
FOP HAS/ DM/
DLP
HAS FA/ DM HAS HAS HAS/ DM
Sintomas Afasia,
Hemipl.
Disartria,
Hemipl.
Afasia,
Hemip.
Afasia,
Hemipl.
Disartria,
Hemipl.
Disartria,
Hemipl.
Disartria,
Hemipl.
Local do
infarto
Esquerdo Direito Esquerdo Esquerdo Direito Direito Direito
Mecan. do
AVC
Cardioem. Aterotr. Durante
clip.
aneurisma
Cardioem. Aterotr. Aterotr. Aterotr.
Tto
agudo
Conserv. Conserv. Conserv. rt-PA IV rt-PA IV rt-PA IV +
IA +
craniect.
Craniect.
Transf.
Hemorr.
Não Sim Não Sim Não Sim Não
D1:
NIHSS/
IB/ EmR
(dias após
o AVC)
7/ 100/ 2
(67)
9/ 35/ 4
(82)
4/ 95/ 1
(62)
13/ 25/ 5
(72)
9/ 30/ 4
(59)
13/ 10/ 5
(73)
13/ 20/ 5
(89)
Aterotr, Aterotrombótico; Cardioem, Cardioembólico; Clip, clipagem; Conserv, conservador; Craniect,Craniectomia; DLP, dislipidemia; DM, Diabetes Melitus; EmR, Escala modificada de Rankin; FA,Fibrilação atrial; FOP, Forâmen oval patente; HAS, Hipertensão arterial sistêmica; Hemip, hemiparesia;Hemipl, Hemiplegia; Hemorr, Hemorrágica; IA, Intra-arterial; IB, Índice de Barthel; IV, intravenoso; M,Masculino; Mecan, mecanismo; NIHSS, National Institute of Health Stroke Scale; Pac, Paciente; Transf,transformação; Tto, tratamento.

5.2 SEGURANÇA DO PROCEDIMENTO
Não houve efeitos adversos relacionados ao procedimento, tampouco alteração clínica
e laboratorial nos primeiros sete dias do acompanhamento. Os EEG de todos os pacientes
demonstravam ritmo difusamente lento nas respectivas áreas isquêmicas. O EEG do paciente
3, além de lentificação, demonstrou surtos de pontas, ondas agudas e ondas irregulares, na
projeção temporal esquerda (local da isquemia), mas sem expressão clínica. Apenas o
paciente 1 fazia uso regular de fenitoína (100 mg, três vezes ao dia), devido à crise convulsiva
no dia do AVC.
Na fase de avaliação pré-internação do paciente 7, observamos diminuição de pulso
arterial periférico (dorsal do pé e tibial posterior) e história de claudicação intermitente no
membro inferior esquerdo (MIE). A arteriografia cerebral para infusão das CMMO foi
realizada, portanto, através da canulização da artéria femoral direita. Durante este
procedimento, foi constatado que a ACM direita (envolvida no AVC), estava ocluída.
Entretanto, como havia muitos ramos de colaterais, optamos pela infusão das células. O
exame prévio realizado (Doppler transcraniano), para averiguação da patência da ACM, não
demonstrava oclusão. Não houve alteração clínica nem laboratorial nos primeiros sete dias
após o procedimento. Após avaliação por um cirurgião vascular (encaminhado por seu médico
clínico), o paciente foi submetido à revascularização do MIE, sob anestesia geral. Apresentou
hipotensão arterial durante o ato cirúrgico e piora do déficit motor no pós-operatório. À RM
de crânio, foi evidenciado novo evento isquêmico no território da ACM direita.
Os pacientes permaneceram em acompanhamento no Ambulatório de Neurologia do
HUCFF após o período de acompanhamento do protocolo. Dois destes (pacientes 5 e 6),
apresentaram crise convulsiva tônico-clônica generalizada após, aproximadamente, 200 dias
da infusão das CMMO. O paciente 5 foi tratado com fenitoína (100 mg, três vezes ao dia) e o
paciente 6, com duas drogas: oxcarbazepina (300 mg, três vezes ao dia) e lamotrigina (100
mg/ dia), pois apresentou alergia à fenitoína e as crises não foram controladas com uma droga
anti-epiléptica somente. Apesar das crises convulsivas, não houve alteração nas escalas de
avaliação, comparado ao D120 de acompanhamento.
Todos os pacientes foram submetidos a um método de imagem (TC ou RM de crânio)
por volta de 180 dias. À exceção do paciente 7, anteriormente descrito, nenhum apresentou
novas lesões vasculares (isquêmicas ou hemorrágicas) ou lesões expansivas.

5.3 CELULARIDADE DO MATERIAL INFUNDIDO
A média da infusão total de células na ACM foi de 3,2 x 108, variando entre 1 x 108 e
5 x 108. O Quadro 2 demonstra a celularidade de cada paciente. Os dados da celularidade do
paciente 7 não estão disponíveis até o momento.
Quadro 2: Celularidade do material infundido: este quadro demonstra a celularidade domaterial infundido, avaliada através de imunofenotipagem por citometria de fluxo emaparelho BD FACSCanto™ classe 1
Pacientes Infundidas (x108) CMMO (%) CTM (%) CTH (%)
1 5,0 x 108 66 0,15 1,10
2 1,25 x 108 65 0,27 3,39
3 3,9 x 108 69 0,09 4,68
4 4,0 x 108 73 1,73 2,51
5 3,2 x 108 73 0,07 0,67
6 1,0 x 108 58 0,04 2,02
7 4,0 x 108 x x x
CMMO, células mononucleares da medula óssea; CTH, células-tronco hematopoiéticas;CTM, células-tronco mesenquimais.

5.4 IMAGENS
As imagens de corpo inteiro, obtidas duas horas após a infusão das CMMO marcadas,
mostraram captação no cérebro de todos os pacientes. A localização das células pode ser
melhor visualizada nas imagens de SPECT do que nas imagens corporais totais. O SPECT do
paciente 2 permite pouca visualização das células marcadas porém, à quantificação realizada
pelo aparelho de cintilografia, confirmou-se a presença das mesmas em menor quantidade,
quando comparada aos outros pacientes. Houve captação distribuída no fígado, baço, pulmões
e rins em todos os pacientes. Devido à meia-vida de seis horas do 99mTecnécio, a resolução da
imagem diminuiu, de forma importante, 24h após a infusão das CMMO marcadas. Portanto, a
captação cerebral só pode ser visualizada no cérebro dos pacientes 1 e 3, enquanto que, em
todos, a captação era vista no fígado, pulmões, baço, rins e bexiga. O paciente 7 não possui
gravadas as imagens de cintilografia realizadas 24h após a infusão das CMMO.

5.4.1 Paciente 1
Figura 3: Imagens SPECT 2h após infusão CMMO
CMMO marcadas com 99mTecnécio na área isquêmica

Figura 4: Paciente 1 - Imagens corpo inteiro 2h após infusão CMMO
CMMO marcadascom 99m Tecnéciona área isquêmica
CMMO marcadascom 99m Tecnécionos pulmões
CMMO marcadascom 99mTecnécio nofígado e baço
CMMO marcadascom 99mTecnécio nasvias urinárias
Anterior Posterior
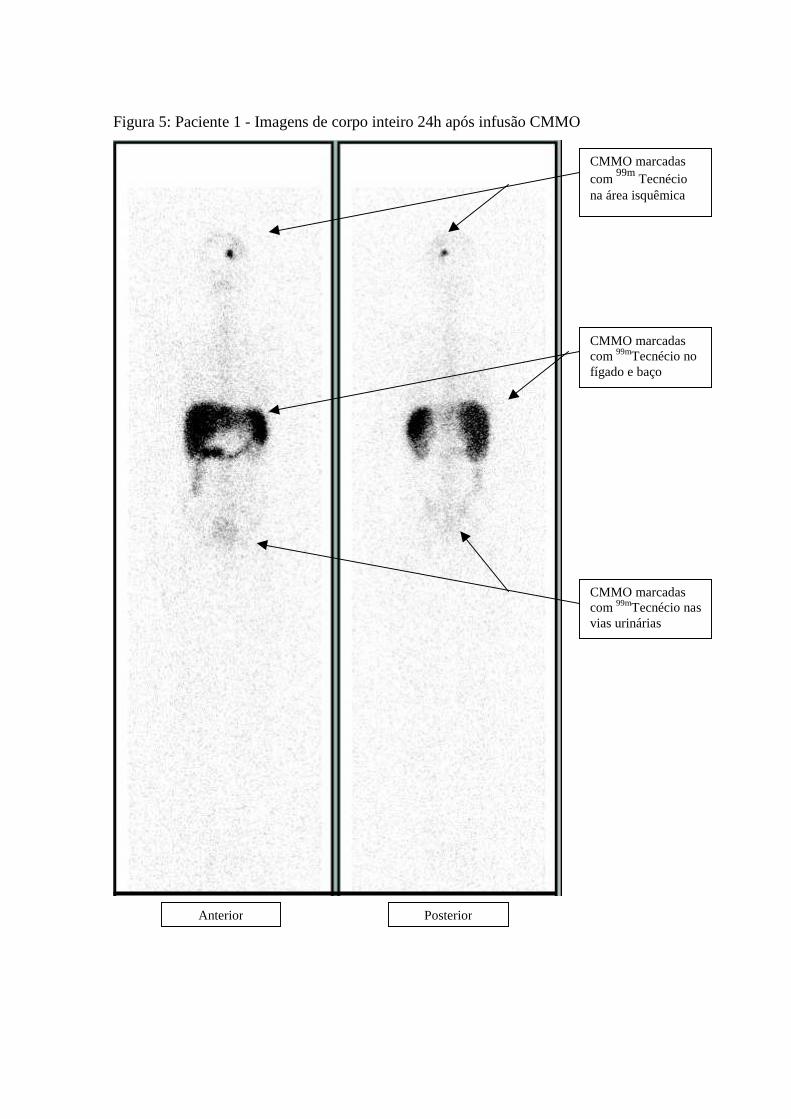
Figura 5: Paciente 1 - Imagens de corpo inteiro 24h após infusão CMMO
Anterior Posterior
CMMO marcadascom 99mTecnécio nasvias urinárias
CMMO marcadascom 99mTecnécio nofígado e baço
CMMO marcadascom 99m Tecnéciona área isquêmica

5.4.2 Paciente 2
Figura 6: Imagens SPECT 2h após infusão CMMO
CMMO marcadas com 99mTecnécio na área isquêmica

Figura 7: Paciente 2 - Imagens corpo inteiro 2h após infusão CMMO
CMMOmarcadas com99mTecnécio nasvias urinárias
CMMOmarcadas com99mTecnécio nofígado e baço
CMMOmarcadas com99mTecnécio nospulmões
CMMOmarcadas com99mTecnécio naárea isquêmica
Anterior Posterior

Figura 8: Paciente 2 - Imagens corpo inteiro 24h após infusão CMMO
CMMOmarcadascom99mTecnécionas viasurinárias
CMMOmarcadascom99mTecnéciono fígado ebaço
Anterior Posterior

5.4.3 Paciente 3
Figura 9: Imagens SPECT 2h após infusão CMMO
CMMO marcadas com 99m Tecnécio na área isquêmica

Figura 10: Paciente 3 - Imagens corpo inteiro 2h após infusão CMMO
CMMOmarcadas com99m Tecnécionas viasurinárias
CMMOmarcadas com99mTecnécio nofígado e baço
CMMOmarcadas com99mTecnécio nospulmões
CMMOmarcadas com99mTecnécio naárea isquêmica
Anterior Posterior

Figura 11: Paciente 3 - Imagens corpo inteiro 24h após infusão CMMO
CMMO marcadascom 99mTecnécionas vias urinárias
CMMO marcadascom 99mTecnéciono fígado e baço
CMMO marcadascom 99mTecnéciona área isquêmica
Anterior Posterior

Figura 12: Paciente 3 - Imagem cerebral 24h após infusão CMMO
CMMO marcadas com 99mTecnécio na área isquêmica

5.4.4 Paciente 4
Figura 13: Imagens SPECT 2h após infusão CMMO
CMMO marcadas com 99mTecnécio na área isquêmica

Figura 14: Paciente 4 - Imagens corpo inteiro 2h após infusão CMMO
CMMOmarcadas com99m Tecnécionas viasurinárias
CMMOmarcadas com99m Tecnécio nofígado e baço
CMMOmarcadas com99m Tecnécionos pulmões
CMMOmarcadas com99mTecnécio naárea isquêmica
Anterior Posterior

Figura 15: Paciente 4 - Imagens corpo inteiro 24h após infusão CMMO
CMMOmarcadas com99mTecnécio nasvias urinárias
CMMOmarcadas com99mTecnécio nofígado e baço
Anterior Posterior

5.4.5 Paciente 5
Figura 16: Imagens corpo inteiro 2h após infusão CMMO
CMMOmarcadas com99mTecnécio nasvias urinárias
CMMOmarcadas com99mTecnécio nofígado e baço
CMMOmarcadas com99mTecnécio nospulmões
CMMOmarcadas com99mTecnécio naárea isquêmica
Anterior Posterior

Figura 17: Paciente 5 - Imagens corpo inteiro 24h após infusão CMMO
CMMOmarcadas com99mTecnécio nasvias urinárias
CMMOmarcadas com99mTecnécio nofígado e baço
Anterior Posterior

5.4.6 Paciente 6
Figura 18: Imagens SPECT 2h após infusão CMMO
CMMO marcadas com 99m Tecnécio na área isquêmica

Figura 19: Paciente 6 - Imagens corpo inteiro 2h após infusão CMMO
CMMOmarcadas com99mTecnécio nasvias urinárias
CMMOmarcadas com99mTecnécio nofígado e baço
CMMOmarcadas com99mTecnécio nospulmões
CMMOmarcadas com99mTecnécio naárea isquêmica
Anterior Posterior

Figura 20: Paciente 6 - Imagens corpo inteiro 24h após infusão CMMO
CMMOmarcadas com99mTecnécio nasvias urinárias
CMMOmarcadas com99mTecnécio nofígado e baço
Anterior Posterior

5.4.7 Paciente 7
Figura 21: Imagens cerebrais 2h após infusão CMMO
CMMOmarcadas com99mTecnécio naárea isquêmica

Figura 22: Paciente 7 - Imagens corpo inteiro 2h após infusão CMMO
CMMOmarcadas com99mTecnécio nasvias urinárias
CMMOmarcadas com99mTecnécio nofígado e baço
CMMOmarcadas com99mTecnécio nospulmões
CMMOmarcadas com99mTecnécio naárea isquêmica
Anterior Posterior

5.5 ESCALAS DE AVALIAÇÃO
Todos os pacientes já ultrapassaram os 120 dias após a infusão das CMMO previstos
pelo protocolo. Somente o paciente 3 era independente nas atividades de vida diária no dia da
infusão das CMMO (IB 95 e EmR 1). No dia 120 (D120) de acompanhamento, os seis
primeiros pacientes haviam melhorado suas escalas de avaliação clínica. O sétimo paciente
manteve dependência total nas atividades de vida diária e piora na escala de AVC (NIHSS).
As tabelas 2, 3 e 4 demonstram os resultados das escalas: NIHSS, IB e EmR,
respectivamente, e o Gráfico 1 demonstra a evolução do NIHSS dos sete pacientes.
Tabela 2: NIHSS dos pacientes: esta tabela demonstra todos os valorescoletados do NIHSS, dos sete pacientes, após a infusão das CMMO,durante o protocolo de acompanhamento.
Pacientes D1 D3 D7 D30 D60 D120
1 7 6 5 5 4 4
2 9 9 8 6 6 6
3 4 3 3 3 3 3
4 13 12 12 11 9 9
5 9 6 5 3 4 1
6 13 13 12 12 12 11
7 13 13 13 15 15 15
D1, Dia da infusão celular; D3, 3° dia de infusão celular; D7, 7° dia de infusão celular; D30,30° dia de infusão celular; D60, 60° dia de infusão celular; D120, 120° dia de infusão celular;NIHSS, National Institute of Health Stroke Scale.
Tabela 3: Índice de Barthel dos pacientes: em sete pacientes, após a infusãodas CMMO, durante o protocolo de acompanhamento
Pacientes D1 D3 D7 D30 D60 D120
1 100 100 100 100 100 100
2 35 35 35 50 55 75
3 95 95 95 100 100 100
4 25 25 25 25 30 35
5 30 30 30 50 90 100
6 10 10 15 25 30 50
7 20 20 20 10 10 10
D1, Dia da infusão celular; D3, 3° dia de infusão celular; D7, 7° dia de infusão celular; D30,30° dia de infusão celular; D60, 60° dia de infusão celular; D120, 120° dia de infusão celular

Tabela 4: Escala modificada de Rankin dos pacientes: avaliada nos setepacientes após a infusão de CMMO, durante o protocolo de acompanhamento
Pacientes D1 D3 D7 D30 D60 D120
1 2 2 2 1 1 1
2 4 4 4 4 4 3
3 1 1 1 1 1 1
4 5 5 5 4 4 4
5 4 4 4 3 1 1
6 5 5 5 5 5 4
7 5 5 5 5 5 5
D1, Dia da infusão celular; D3, 3° dia de infusão celular; D7, 7° dia de infusão celular; D30,30° dia de infusão celular; D60, 60° dia de infusão celular; D120, 120° dia de infusão celular
Gráfico 1: NIHSS (ordenada) x Dia de infusão (abscissa): gráfico demonstrativo do NIHSS dos sete pacientes avaliados, durante protocolo de acompanhamento.Pacientes 1 a 7 em cores, conforme legenda ao lado do gráfico.
D1, Dia da infusão celular; D3, 3° dia de infusão celular; D7, 7° dia de infusão celular; D30,30° dia de infusão celular; D60, 60° dia de infusão celular; D120, 120° dia de infusão celular;NIHSS, National Institute of Health Stroke Scale.
0
2
4
6
8
10
12
14
16
D1 D3 D7 D30 D60 D120
1234567

5.6 PARÂMETROS LABORATORIAIS
Não houve alteração evolutiva em nenhum dos parâmetros laboratoriais colhidos
durante o acompanhamento.

6 DISCUSSÃO
Nesta série de pacientes apresentados, a infusão de CMMO mostrou ser segura e
exequível em sete pacientes com AVC isquêmico em território da ACM, em até 90 dias após
a isquemia. Não houve complicações diretas relacionadas ao procedimento. Apenas um
paciente piorou o NIHSS em dois pontos (sétimo paciente) por intercorrência clínica não
diretamente ligada ao procedimento de infusão das CMMO. Os outros seis pacientes
melhoraram suas escalas de avaliação (NIHSS, IB, EmR), no final do protocolo de
acompanhamento (Tabelas 2, 3 e 4 e Gráfico 1) e permanecem sem alterações evolutivas até o
momento.
Terapias baseadas em células-tronco representam novas e importantes estratégias para
o tratamento do AVC. Em modelos animais de isquemia, células-tronco de diferentes fontes
foram usadas com resultados promissores e diferentes mecanismos de ação têm sido sugeridos
para explicar esses benefícios funcionais (LI et al, 2000; BORLONGAN et al, 2004; SHYU et
al, 2004). Por exemplo: a introdução das células-tronco neurais/ progenitoras neurais em áreas
de perda celular pode resultar em reparação e restauração do circuito (ENGLUND et al,
2002). Alternativamente, quando as células-tronco derivadas da medula óssea (mesenquimais
ou mononucleares) são empregadas, os benefícios funcionais observados em alguns estudos
ocorrem, provavelmente, devido à liberação de citocinas e/ou fatores tróficos, os quais têm
efeito imunomodulador e/ou contribuem para a redução da apoptose na área de penumbra em
períodos mais precoces após a isquemia cerebral (GIRALDI-GUIMARÃES et al, 2009).
Além disso, tem sido sugerido que terapias baseadas nas células melhoram o processo de
reparação cerebral e plasticidade, incluindo neurogênese, angiogênese e sinaptogênese, o que
poderia explicar os benefícios observados nos modelos experimentais de AVC, até mesmo
quando as células são infundidas mais tardiamente (SAVITZ et al, 2004; CAPLAN et al,
2007; VENDRAME et al, 2005).
Até o momento, poucos estudos clínicos envolvendo terapia celular em pacientes com
AVC agudo e crônico foram publicados (KONDZIOLKA et al 2000 e 2005; SAVITZ et al,
2005; BANG et al, 2005). Não há nenhum estudo clínico em larga escala e somente dois
desses estudos envolveram o uso de células tronco autólogas, derivadas da medula óssea
(MENDONÇA et al, 2006; BANG et al, 2005). Em um deles, Bang e colaboradores
investigaram a segurança da infusão intravenosa de CTM, autólogas, derivadas da medula
óssea e expandidas in vitro, em pacientes com infarto cerebral agudo (BANG et al, 2005). O
procedimento foi seguro e exequível; os pacientes do grupo que receberam as CTM (n=5)
tiveram aumento no IB no terceiro e sexto mês após a infusão. Entretanto, as alterações no

NIHSS e na EmR não foram estatisticamente significativas. Outro ponto a ser discutido diz
respeito à preparação das células: embora exequível, tem custo elevado e é potencialmente
perigosa (risco de contaminação, principalmente). O outro estudo também foi realizado na
fase aguda do AVC (três a dez dias após o evento isquêmico) e avaliou a segurança do
transplante intra-arterial de CMMO em pacientes com infartos em território da ACM em duas
instituições brasileiras diferentes. Em uma delas, seis pacientes foram envolvidos e
receberam, aproximadamente, 3,0x108 células no território da ACM, via artéria femoral, por
técnica de Seldinger. Resultados preliminares demonstraram que o procedimento é seguro e
exequível (MENDONÇA et al, 2006; de FREITAS et al, 2006).
Com relação ao AVC na fase crônica, Savitz e colaboradores estudaram transplante
intracerebral de células fetais porcinas, em pacientes que haviam tido AVC entre três meses e
dez anos antes do estudo. Os pacientes foram submetidos a implante estereotáxico (guiado por
TC) de células fetais de porco, tratadas previamente com anticorpo para prevenir rejeição. O
estudo foi parado pelo Food and Drug Administration (sigla em inglês FDA), devido aos
eventos adversos (oclusão de veia cortical secundária à cirurgia em um paciente e convulsões
em dois pacientes – uma e três semanas após o implante (SAVITZ et al, 2005). Kondziolka e
colaboradores conduziram um estudo fase 2 (randomizado) que incluiu pacientes com tempo
médio de AVC isquêmico de três anos e meio. Eles receberam implantes estereotáxicos de
células neuronais humanas, derivadas de uma linhagem celular de carcinoma embrionário
humano e cultivadas em laboratório. O estudo foi negativo para o desfecho primário medido
(melhora no déficit neurológico motor, medido através da ESS), embora tenha havido
melhora, porém não estatisticamente significativa, em alguns pacientes. Um paciente
apresentou crise convulsiva um dia após a cirurgia, enquanto outro desenvolveu hematoma
subdural, que necessitou drenagem cirúrgica, um mês após o implante das células
(KONDZIOLKA et al, 2005). Os resultados desses dois estudos sugerem que o transplante
intracraniano tem risco potencial. No nosso estudo, a razão para se ter escolhido a dosagem
das células baseou-se no estudo de segurança descrito acima (de FREITAS et al, 2006) e a
razão para selecionar pacientes com AVC não-agudo foi baseada nos resultados de estudos
clínicos de terapia celular na fase crônica do AVC (KONDZIOLKA et al, 2000). Parece que a
janela terapêutica deve ser determinada em função da dose terapêutica e que o regime de
repetição de dose pode otimizar o benefício da recuperação (The STEPS participants, 2009).
Para entender o processo dinâmico envolvido no reparo cerebral mediado pelas
células-tronco, têm-se estudado a marcação de células in vitro com agentes de contraste na
RM. A pré-marcação das células-tronco com contrastes à base de ferro (SHAPIRO; SKRTIC;

KORETSKY, 2005) ou à base de gadolínio - Gadolinium Rhodamine Dextran – GRID
(MODO et al, 2004) permitiu visualizar, em ratos, a presença e migração das células-tronco
transplantadas para o sítio de isquemia cerebral. Entretanto, alguns pontos devem ser
observados: (a) apesar do uso de moléculas de ferro cada vez menores, sua toxicidade ainda
representa uma grande preocupação, pois, sendo um elemento essencial no metabolismo
celular, seu acúmulo produz acentuada proliferação celular (WHITNALL et al, 2006); (b)
para os dois tipos de marcação celular foram utilizados aparelhos de RM de 4,7 Tesla (T),
7,0T e 11,7T, ainda não liberados para uso clínico.
A marcação celular com radioisótopos é um método bem estabelecido que permite
monitorização sistêmica das células e tem sido aplicada em alguns estudos clínicos
envolvendo terapia celular no infarto do miocárdio (GOUSSETIS et al, 2006; HOFMANN et
al, 2005; PENICKA et al, 2007) e na fase aguda do AVC isquêmico (CORREA et al, 2007).
A segurança e a exequibilidade da injeção de CMMO na fase subaguda do AVC isquêmico,
bem como a marcação celular com 99mTecnécio ainda não haviam sido estudadas em ensaio
clínico. Estima-se que haja ruptura da barreira hematoencefálica após a isquemia, mas ainda
não há definição pela literatura do tempo levado para a sua restauração. Neste estudo
pudemos observar que, mesmo após dois meses do evento isquêmico cerebral, as CMMO
marcadas puderam ser visualizadas duas horas após a infusão, na área isquêmica de todos os
pacientes e que, pelo menos em dois pacientes, elas permaneceram na área de lesão por 24
horas. A meia-vida do 99mTecnécio é de apenas seis horas, o que permite um monitoramento
muito curto das células injetadas, porém resulta em boa resolução da imagem e menor
radiação para o paciente, quando comparado ao 111-Indium-oxina, outro radiofármaco
comumente usado (PALESTRO et al, 2009). Comprovamos o destino de parte das células
marcadas: lesão isquêmica cerebral, fígado, pulmões, baço e rins. Outros estudos devem ser
realizados, utilizando outras formas de marcação celular, como GRID por exemplo, para
avaliar o comportamento das células-tronco no cérebro humano. Entretanto, estes estudos
clínicos ainda estão longe de ocorrerem, pois, conforme descrito acima, ainda há questões de
segurança não respondidas nos ensaios experimentais.
Inicia-se também, outra importante discussão: há necessidade da patência do vaso
envolvido no AVC isquêmico (neste caso ACM), para que as CMMO atinjam a área cerebral
lesada? As imagens relacionadas ao paciente 7 levantam essa questão, pois apesar da ACM
ocluída à arteriografia, houve captação de 99mTecnécio após infusão das CMMO marcadas.
Não está claro se as convulsões tardias em dois pacientes, após o período de
acompanhamento, foram causadas por alguma reação tardia das células mononucleares

injetadas, pelo redirecionamento errático das fibras de regeneração tecidual (re-inervação
aberrante) ou pela própria presença do tecido isquêmico, fornecendo substrato anatômico.
Embora muitos fatores de risco para convulsões precoces ou tardias após o AVC tenham sido
identificados, não há um preditor claro de epilepsia pós-AVC (RYVLIN; MONTAVONT;
NIGHOGHOSSIAN, 2006). Aproximadamente cinco a dez por cento dos pacientes após
AVC isquêmico agudo têm convulsões precoces, as quais ocorrem tipicamente em 24 horas
(CAMILO; GOLDSTEIN, 2004). Já as convulsões tardias ocorrem usualmente nas primeiras
duas semanas após o AVC (BLADIN; ALEXANDROV, 2000 e GUPTA; RUBINO, 1988)
variando consideravelmente entre as séries – 3 a 67% dos casos (CAMILO; GOLDSTEIN,
2004 e LOSSIUS et al, 2005). O impacto potencial da convulsão na mortalidade do AVC e
desfecho neurológico deve ser levado em consideração, porque influencia a decisão do
tratamento após a primeira convulsão. Entretanto, este ponto ainda permanece em debate, com
dados limitados a respeito do impacto de convulsões tardias e recorrentes no desfecho
funcional (RYVLIN; MONTAVONT; NIGHOGHOSSIAN, 2006). Devido à nossa amostra
ser muito pequena, nós não podemos descartar que uma incidência de convulsão seja
explicada pelo acaso.
Alguns pontos ainda devem ser discutidos, pois apesar do uso de células-tronco
parecer seguro e exequível, muitas questões permanecem não-respondidas. Há tantas formas
potenciais de terapia celular tanto quanto tipos celulares: embrionárias, fetais, derivadas de
teratocarcinoma, células neurais culturadas, CMMO ou CTM, com as doses variando entre os
estudos. Ainda não sabemos qual a melhor via de administração das células (intravenosa,
intra-arterial, implante cerebral), pois se discute se há necessidade das células estarem
próximas ao tecido lesado para exercer seu efeito (já que o mecanismo de atuação mais aceito
atualmente é o efeito parácrino das células-tronco). O melhor tempo após o início do AVC
também não foi definido: fase aguda ou crônica do AVC? Inflamação acentuada X
fechamento da barreira hematoencefálica (KLEINIG; VINK, 2009), bem como se há
estabilidade no tempo após a infusão celular (ENGLAND; MARTIN; BATH, 2009). Estas
questões só serão respondidas após esforços para coordenar e estandardizar métodos e
parâmetros de avaliação clínica e funcional (TROUNSON, 2009).
Embora não se possa, até o momento, repopular as áreas perdidas no AVC, a
tecnologia com células-tronco é um campo promissor, que poderá impactar significativamente
o tratamento futuro do AVC isquêmico.

7 CONCLUSÃO
O transplante de CMMO é exequível e parece ser seguro em pacientes com AVC
isquêmico na fase subaguda. Houve evidência de que as CMMO marcadas com 99mTecnécio
permanecem na área afetada pela isquemia cerebral por, pelo menos, 24 horas. Não houve
modificação dos parâmetros clínicos e laboratoriais de seis pacientes ao longo do seguimento.
Estudos clínicos randomizados são necessários para estabelecer a eficácia e segurança a longo
prazo deste procedimento.

REFERÊNCIAS
ANDRÉ, C.; et al. Progressive decline in stroke mortality in Brazil from 1980 to 1982, 1990to 1992 and 2000 to 20002. Stroke, no.37,p.2784-2789. 2006
BANG, OY.; et al. Autologous mesenchymal stem cell transplantation in stroke patients. AnnNeurol, no.57, p.874-882. 2005.
BARBOSA da FONSECA, L.M.; et al. Early tissue distribution of bone-marrow mononuclearcells after intra-arterial delivery in a patient with chronic stroke. Circulation , no.120, p.539-541. 2009.
BATINIC, D.; et al. Relationship between differing volumes of bone marrow aspirates andtheir cellular composition. Bone Marrow Transplant, no.6, p.103-107. 1990.
BELLEHSEN, L.; NAGLER, A.; LEVI-SCHAFFER, F. Stem cells: what are they and whydo we need them? In: Adkinson: Middleton’s Allergy: principles and practice, 7th Edition.Philadelphia. Ed. Elsevier, 2008. p259-260.
BHATTACHARY,A. D.; EHRLICH, L.I.R.; WEISSMAN, I.L. Space-time considerations forhematopoietic stem cell transplantation. Eur J Immunol, no.38, p.2060-7. 2008.
BILLER, J.; LOVE, B.B.; SCHNECK, M. Vascular diseases of the nervous system: ischemiccerebrovascular disease. Em Bradley WG Neurology in clinical practice - 5th Edition. Ed.Philadelphia. Ed. Elsevier, 2008. p.1165-1223.
BLADIN, C.F.; ALEXANDROV, A.V. Seizures after stroke: a prospective multicenter study.Arch Neurol, no.57, p.1617-1622. 2000.
BONITA, R.; SOLOMON, N.; BROAD, J.B. Prevalence of stroke and stroke-relateddisability. Estimates from the Auckland stroke studies. Stroke, no.29, p.866-867. 1997.
BORLONGAN, C.V.; et al. Central nervous system entry of peripherally injected umbilicalcord blood cells is not required for neuroprotection in stroke. Stroke, no.35, p.2385-2389.2004.
BROTT, T.; et al. Measurements of acute cerebral infarction : a clinical examination scale.Stroke, no.20, p.864-870. 1989.

BRYDER, D.; ROSSI, D.J.; WEISSMAN, I.L. Hematopoietic stem cells : the paradigmatictissue-specific stem cell. Am J Pathol, no.169, p.338-346. 2006
CAMILO, O.; GOLDSTEIN, L.B. Seizures and epilepsy after ischemic stroke. Stroke, no.35,p.1769-1775. 2004.
CAPLAN, A.I. Adult mesenchymal stem cells for tissue engineering versus regenerativemedicine. J Cell Physiol, no.213, p.341-347. 2007.
CARVALHO, A.B.; et al. Bone marrow multipotent mesenchymal stromal cells do not reducefibrosis or improve function in a rat model of severe chronic liver injury. Stem Cells, no.26,p.1307-1314. 2008.
CHARRUYER, A.; GHADIALLY, R. Stem cells and tissue-engineered skin. SkinPharmacol Physiol, no.22, p.55-62. 2009.
CHEN, J.; et al. Intravenous bone marrow stromal cell therapy reduces apoptosis andpromotes endogenous cell proliferation after stroke in female rat. J Neurosci Res, no.73,p.778-786. 2003.
CHEN, J.; et al. Intravenous administration of human bone marrow stromal cells inducesangiogenesis in the ischemic boundary zone after stroke in rats. Circ Res, no.92, p.692-699.2003.
CORREA, P.L. ; et al. Assesment of intra-arterial injected autologous bone marrowmononuclear cell distribution by radioactive labeling in acute ischemic stroke. Clin NuclMed, no.32, p.839-841. 2007.
CRAMER, S.C. Repairing the human brain after stroke: I. Mechanisms of spontaneousrecovery. Ann Neurol, no.63, p.272-287. 2008.
EINSTEIN, O.; BEN-HUR, T. The changing face of neural stem cell therapy in neurologicdiseases. Arch Neurol, no.65, p.452-456. 2008.
ELY, E.W.; et al. Monitoring sedation status over time in ICU patients: reliability and validityof the Richmond Agitation-Sedation Scale (RASS). JAMA , no.289, p.2983-2991. 2003.

ENDRES, M.; et al. Improving outcome after stroke : overcoming the translational roadblock.Cerebrovasc Dis, no.25, p.268-278. 2008.
ENGLAND, T.; MARTIN, P.; BATH, P.M.W. Stem cells for enhancing recovery afterstroke: a review. Int J Stroke, no.4, p.101-110. 2009.
ENGLUND, U.; et al. Grafted neural stem cells develop into functional pyramidal neuronsand integrate into host cortical circuitry. Proc Natl Acad Sci USA, no.99, p.17089-17094.2002.
FREITAS, G.R. de; et al. Safety and feasibility of intra-arterial autologous bone marrowmononuclear cell transplantation in acute ischemic stroke. Proceedings of the 58th annualmeeting of the American academy of neurology. San Diego, CA, USA, April 1-8,2006.
FARIN, A.; et al. The biological restoration of central nervous system architecture andfunction: part 1- foundations and historical landmarks in contemporary stem cell biology.Neurosurgery, no.64, p.15-39. 2009.
FEIGIN, V.L. ; et al. Stroke epidemiology: a review of population-based studies of incidence,prevalence, and case-fatality in the late 20th century. Lancet Neurology, no.2, p.43-53. 2003.
FILIP, S.; et al. Stem cells and the phenomena of plasticity and diversity: a limiting propertyof carcinogenesis. Stem Cells Dev, no.17, p.1031-8. 2008.
GARCIA-CASTRO, J.; et al. Mesenchymal stem cells and their use as cell replacementtherapy and disease modelling tool. J Cell Mol Med, no.12, p.2552-65. 2008.
GINSBERG, M.D. Neuroprotection for ischemic stroke: past, present and future.Neuropharmacology, no.55, p.363-389. 2008.
GIRALDI-GUIMARÃES, A. ; et al. Treatment with bone marrow mononuclear cells inducesfunctional recovery and decreases neurodegeneration after sensorimotor cortical ischemia inrats. Brain Res, no.1266, p.108-120. 2009.
GOUSSETIS, E.; et al. Intracoronary infusion of CD133+ and CD133 - CD34+ selectedautologous bone marrow progenitor cells in patients with chronic ischemic cardiomyopathy:cell isolation, adherence to the infracted area, and body distribution. Stem Cells, no.24,p.2279-2283. 2006.

GUPTA, S.R.; RUBINO, F.A. Postinfarction seizures. A clinical study. Stroke, no.19,p.1477-1481. 1988.
GUTFILEN, B.; et al. Tc-99-m-leucocytes - is it an intracellular labeling? J Clin LabImmunol , no.51, p.1-7. 1999.
HACKE, W.; et al. Intravenous thrombolysis with recombinant tissue plasminogen activatorfor acute hemispheric stroke : the European Cooperative Acute Stroke Study (ECASS).JAMA , no.274, p.1017-25. 1995.
HACKE, W.; et al. Randomized double-blind placebo-controlled trial of thrombolytic therapywith intravenous alteplase in acute ischemic stroke (ECASS II). Lancet, no.352, p.1245-51.1998.
HACKE, W.; et al. Thrombolysis with alteplase 3 to 4.5 hours after Acute Ischemic Stroke. NEngl J Med, no.359, p.1317-29. 2008.
HAROUSSEAU, J.H. Role of stem cell transplantation. Hematol Oncol Clin N Am:, no.21,p.1157-1174. 2007.
HOFMANN, M.; et al. Monitoring of bone marrow cell homing into the infracted humanmyocardium. Circulation , no.111, p.2198-2202. 2005.
JAGANNATHAN, J.P. ; et al. Imaging of complications of hematopoietic stem celltransplantation. Radiol Clin N Am, no.46, p.397-417. 2008.
KLEINIG, T.J.; VINK, R. Suppression of inflammation in ischemic and hemorrhagic stroke:therapeutic options. Curr Opin Neurol , no.22, p.294-301. 2009.
KONDZIOLKA, D.; et al. Transplantation of cultured human neuronal cells for patients withstroke. Neurology, no.55, p.565-569. 2000.
KONDZIOLKA, D.; et al. Neurotransplantation for patients with subcortical motor stroke: aphase 2 randomized trial. J Neurosurg, no.103, p.38-45. 2005.
LAFLAMME, M.A.; MURRY, C.E. Regenerating the heart. Nat Biotechnol, no.23, p.845-856. 2005.

LI, L.; XIE, T. Stem cell niche: structure and function. Annu Rev Cell Dev Biol, no.21,p.605-31. 2005.
LI, Y.; et al. Intrastriatal transplantation of bone marrow nonhematopoietic cells improvesfunctional recovery after stroke in adult mice. J Cereb Blood Flow Metab, no.20, p.1311-1319. 2000.
LI, Y.; et al. Intracerebral transplantation of bone marrow stromal cells in a 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine mouse model of Parkinson’s disease. Neurosci Lett,no.316, p.67-70. 2001.
LI, Y.; et al. Gliosis and brain remodeling after treatment of stroke in rats with marrowstromal cells. Glia, no.49, p.407-417. 2005.
LI, Y.; CHOPP, M. Marrow stromal cell transplantation in stroke and traumatic brain injury.Neurosci Lett, no.456, p.120-123. 2009.
LOSSIUS, M.I. ; et al. Post-stroke epilepsy: occurrence and predictors – a long-termprospective controlled study (Akershus Stroke Study). Epilepsia, no.46, p.1246-1251. 2005.
LU, D.; et al. Intraarterial administration of marrow stromal cells in a rat modelo f traumaticbrain injury. J Neurotrauma, no.18, p.813-819. 2001.
LU, D.; et al. Adult bone marrow stromal cells administered intravenously to rats aftertraumatic brain injury migrate into brain and improve neurological outcome. Neuroreport,no.12, p.559-563. 2001.
LUTSEP, H.L.. Recent clinical trials of antiplatelet therapy in secondary stroke prevention:expectations and results for application in primary care settings. Am J Med, no.122, S21-S31.2009.
MAHMOOD, A.; et al. Intracerebral transplantation of marrow stromal cells cultured withneurotrophic factors promotes functional recovery in adult rats subjected to traumatic braininjury. J Neurotrauma, no.19, p.1609-1617. 2002.
McGLAVE, P. Overview of cell-and immune-based therapies. Em Hoffman: hematology:basic principles and practice. 5th Edition. Philadelphia. Ed. Elsevier, 2008; p1554-1557.

MENDEZ-OTERO, R. ; et al. Potential roles of bone marrow stem cells in stroke therapy.Regen Med, no.2, p.417-423. 2007.
MENDEZ-OTERO, R.; FREITAS, G.R. de; MENDONÇA, M.L.F.; ANDRÉ, C. Terapiascelulares em neurologia. Terapias avançadas. Primeira Edição. Rio de Janeiro. Ed. Atheneu,2007, p.55-71.
MENDONÇA, M.L.; et al. Safety of intra-arterial autologous bone marrow mononuclear celltransplantation for acute ischemic stroke. Arq Bras Cardiol , no.86, p.52-55. 2006.
MEZEY, E. Bone marrow-derived stem cells in neurological diseases: stones or masons?Regen Med, no.2, p.37-49. 2007.
MODO, M.; et al. Mapping transplanted stem cell migration after a stroke: a serial, in vivomagnetic resonance imaging study. Neuroimage, no.21, p.311-317. 2004.
MORRISON, S.J.; SPRADLING, A.C. Stem cells and niches: mechanisms that promote stemcell maintenance throughout life. Cell, no.132, p.598-611. 2008.
MURRAY, C.J.L.; LOPEZ, A.D. Mortality by cause for eight regions of the world: globalburden of disease study. Lancet., no.349, p.1269-1276. 1997.
PALESTRO, C.J.; LOVE, C.; BHARGAVA, K.K. Labeled leukocyte imaging: current statusand future directions. Q J Nucl Med Mol Imaging, no.53, p.105-123. 2009.
PENICKA, M.; et al. One-day kinetics of myocardial engraftment after intracoronaryinjection of bone marrow mononuclear cells in patients with acute and chronic myocardialinfarction. Heart, no.93, p.837-841. 2007.
PERIN, E.C. ; et al. Transendocardial, autologous bone marrow cell transplantation forsevere, chronic ischemic heart failure. Circulation , no.107, p.2294-2302. 2003.
PROSPER, F.; VERFAILLIE, C.M. Stem cells for tissue repair. Em Hoffman: hematology:basic principles and practice. 5th Edition. Philadelphia. Ed. Elsevier, 2008; p1749-1752.
ROSENZWEIG, A. Cardiac cell therapy – mixed results from mixed cells. N Engl J Med,no.355, p.1274-7. 2006.

RYVLIN, P.; MONTAVONT, A.; NIGHOGHOSSIAN, N. Optimizing therapy of seizures instroke patients. Neurology, no.67(Suppl 4):S3-S9. 2006.
SAVITZ, S.I.; et al. Cell transplantation for stroke. Ann Neurol, no.52, p.266-275. 2002.
SAVITZ, S.I. ; et al. Cell therapy for stroke. NeuroRx, no.1, p.406-414. 2004.
SAVITZ, S.I. ; et al. Neurotransplantation of fetal porcine cells in patients with basal gangliainfarcts : a preliminary safety and feasibility study. Cerebrovasc Dis, no.20, p.101-107. 2005.
SHAPIRO, E.M.; SKRTIC, S.; KORETSKY, A.P. Sizing it up: cellular MRI using micron-sized iron oxide particles. Magn Reson Med, no.53, p.329-338. 2005.
SHEN, L.H. ; et al. Therapeutic benefit of bone marrow stromal cells administered 1 monthafter stroke. J Cereb Blood Flow Metab, no.27, p.6-13. 2007.
SHUAIB, A.; et al. NXY-059 for the treatment of acute ischemic stroke. N Engl J Med,no.357, p.562-71. 2007.
SHYU, W.C. ; et al. Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells. Circulation , no.110, p.1847-1854. 2004.
SHYU, W.C. ; et al. Granulocyte colony-stimulating factor for acute ischemic stroke: arandomized controlled trial. CMAJ , no.174, p.927-33. 2006.
SYKOVA, E.; et al. Autologous bone marrow transplantation in patients with subacute andchronic spinal cord injury. Cell Transplant, no.15, p.675-687. 2006.
The NINDS (National Institute of Neurological Disorders) and Stroke rt-PA Stroke StudyGroup. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med, no.333,p.1581-7. 1995.
The STEPS participants: Stem cell therapies as an emerging paradigm in Stroke: bridgingbasic and clinical science for cellular and neurogenic factor therapy in treating stroke. Stroke,no.40, p.510-515. 2009.
TROUNSON, A. New perspectives in human stem cell therapeutic research. BMC Medicine,no.7, p.1-5. 2009.

van der WORP, H.B.; van GIJN, J. Clinical practice. Acute ischemic stroke. N Engl J Med,no.357, p.572-579. 2007.
VENDRAME, M.; et al. Anti-inflammatory effects of human cord blood cells in a rat modelof stroke. Stem Cells Dev, no.14, p.595-604. 2005.
WHITNALL, M.; et al. A class of iron chelators with a wide spectrum of potent antitumoractivity that overcomes resistance to chemotherapeutics. Proc Natl Acad Sci USA, no.103,p.14901-14906. 2006.
WU, Z.; et al. Sino-MONICA project. a collaborative study on trends and determinants incardiovascular diseases in china. Part I: morbidity and mortality monitoring. Circulation ,no.103, p.462-468. 2001.

ANEXOS

ANEXO 1 – TERMO DE CONSENTIMENTO LIVRE E ESCLARECID O
Eu fui convidado a participar do estudo "SEGURANÇA DO TRANSPLANTEAUTÓLOGO DE CÉLULAS MONONUCLEARES DA MEDULA ÓSSEA E MPACIENTES COM ACIDENTE VASCULAR CEREBRAL ISQUÊMICOSUBAGUDO" . Em relação ao estudo, eu fui informado das seguintes questões:
1. O estudo foi aprovado pelo Comitê de Ética do Hospital (n° 169/03) e pelaComissão Nacional de Ética em Pesquisa (n° 10385).
2. O objetivo deste estudo é avaliar se o transplante de células retirada da medula doosso é seguro no tratamento do AVC (acidente vascular cerebral, ou "derrame") em sereshumanos. O estudo está sendo realizado pois as células-tronco conseguiram ajudar narecuperação do AVC em ensaios em animais. Nesses ensaios, os animais que receberam ascélulas-tronco após o AVC tiveram menos seqüelas do que os animais que não receberamestas células. Não se sabe se as células-tronco se transformam em neurônios ou se produzemsubstâncias que ajudam na recuperação.
3. O estudo irá incluir apenas pessoas entre 18 e 75 anos que tenham apresentado umAVC isquêmico nos últimos 90 dias confirmado pela tomografia computadorizada de crânio.Não poderão ser incluídas pessoas que tenham alguma doença ou condição que possamdificultar a realização do estudo como, por exemplo, câncer, insuficiência do fígado, gravidez.
4. Uma vez que eu concorde em participar do estudo, eu serei submetido (a) aosseguintes procedimentos:a) Será realizada retirada de células através de punção da medula (parte interna) do osso dabacia, sob efeito de sedativos e analgésicos, por um especialista em hematologia. Esteprocedimento é semelhante aos já realizados para transplantes de medula utilizados em largaescala na medicina de hoje. Não constitui nenhuma novidade no meio médico, além deoferecer risco muito baixo de complicações. Estes riscos envolvem perfuração óssea einfecção do osso, e ocorrem em menos de 1% dos casos;b) O implante de células tronco ocorrerá no mesmo dia, e a via de administração será ocateterismo cerebral. O cateterismo consiste na colocação, após anestesia local, de um cateterem uma artéria na região da virilha, o que permite levar esse cateter até as artérias cerebraispara visualização destas e infusão das células-tronco de medula óssea. O cateterismo cerebralé o único procedimento do estudo que é considerado invasivo, porém é um procedimentoseguro, com risco de complicações em cerca de 1,4% dos casos. O cateterismo será realizadopor um especialista em radiologia intervencionista.c) Serão realizados dois exames de cintilografia cerebral para avaliar a "posição" das células-tronco no meu cérebro: 2 e 24horas após a injeção das células.
Eu vou ficar internado (a) no Hospital por dois dias após o implante de células troncoe, neste período serei submetido a novos exames de sangue, tomografia computadorizada (senecessário), eletroencefalograma, assim como escalas neurológicas para verificar o grau deindependência e recuperação. Depois da alta hospitalar, consultas e exames de sangue serãorealizados 7, 30, 60 e 120 dias após o transplante das células.
5. Eu estou consciente de que podem existir alguns efeitos colaterais relacionados aoestudo. Os riscos do implante de células em seres humanos são muito pouco conhecidos.Existem seres humanos que já receberam células parecidas com as da medula óssea nocérebro, em doenças degenerativas, como Doença de Parkinson através de procedimentocirúrgico, com implante direto. Outros pacientes já foram submetidos a implantes de célulasna fase aguda do acidente vascular cerebral. Não houve qualquer complicação relatada até omomento. Observe que apenas poucos pacientes já se submeteram a este procedimentopreviamente, o que é muito pouco para que possamos afirmar qualquer coisa com respeito às

complicações. No entanto, existe a possibilidade de algumas complicações, além das acima,ocorrerem: inflamação no cérebro, levando a aumento da lesão e inchaço no mesmo,sangramento cerebral,aparecimento de atividade epiléptica, infecção no cérebro e crescimentode tecidos não cerebrais no cérebro.
6. Eu estou consciente de que não existe remuneração referente à inclusão no estudo,nem ressarcimentos ou indenizações relacionadas às complicações dos procedimentos doestudo. Caso o paciente apresente alguma complicação, os investigadores serão responsáveispelo seu tratamento.
7. Eu estou consciente de que os pesquisadores do estudo terão acesso ao meuprontuário, para verificar doenças passadas ou futuras. A revisão dos prontuários e registrosmédicos será realizada de acordo com a legislação brasileira (resoluções do Conselho Federalde Medicina n° 1605/2000, 1638/2002, 1642/2002).
8. Eu estou consciente que, enquanto o estudo estiver sendo realizado, eu não sereiidentificado por quaisquer pessoas de fora do estudo, e de que os meus resultados serãoconfidenciais.
9.Eu estou consciente que posso me recusar a participar do estudo e que eu posso sairdo estudo quando quiser, e que isto não vai afetar o meu tratamento médico. Se eu apresentaralgum problema que eu suspeite que tenha resultado do meu envolvimento no estudo, euestou ciente que devo falar com meu neurologista. Conheço e posso telefonar, se necessário,para os Drs. Charles André (telefone pessoal: 9989.7937), Gabriel de Freitas (telefonepessoal: 9973.0164) e Valéria Battistella (telefone pessoal:9328.7596).
_____________________________________ _________________Assinatura do paciente ou responsável legal DataEu expliquei ao paciente ____________________________________________________ oprojeto de pesquisa e os efeitos do tratamento. Acredito que ele (a) tenha compreendido aminha explicação e que deu o seu consentimento de livre e espontânea vontade.
__________________________________ _________________ Gabriel R. de Freitas, CRM 52.60589-7 Data Charles André, CRM 52.38570-7 Valéria Battistella, CRM 52.70716-3

ANEXO 2 – NIHSS
1.a – Nível de consciência:0 - alerta 1 - acorda facilmente2 - torpor3 - coma
1.b – Orientação:0 - ambas corretas1 - uma correta2 - nenhuma resposta correta
1.c – Comandos0 - ambas corretamente 1 - apenas uma das tarefas 2 - não realiza nenhuma das tarefas
2. Olhar:0 - normal1 - paralisia parcial2 - desvio forçado ou paralisia total
3. Campos visuais:0 - normal1 - hemianopsia parcial2 - hemianopsia completa3 - hemianopsia bilateral
4. Paralisia facial:0 - normal1 - mínima2 - parcial 3 - completa
5.a – Motricidade MSE:0 - mantém posição1 - membro desce antes de 10s2 - esforço contra gravidade3 - nenhum esforço contra gravidade4 - nenhum movimento

5.b – Motricidade MSD:0 - mantém posição1 - membro desce antes de 10s2 - esforço contra gravidade3 - nenhum esforço contra gravidade4 - nenhum movimento
6.a – Motricidade MIE:0 - mantém posição1 - membro desce antes de 5s2 - esforço contra gravidade3 - nenhum esforço contra gravidade4 - nenhum movimento
6.b – Motricidade MID:0 - mantém posição1 - membro desce antes de 5s2 - esforço contra gravidade3 - nenhum esforço contra gravidade4 - nenhum movimento
7. Ataxia de membros:0 - ausente1 - presente em um membro2 - presente em dois membros
8. Sensibilidade:0 - normal1 - perda parcial2 - perda grave ou total
9. Linguagem:0 - normal1 - afasia leve/ moderada2 - afasia grave3 - afasia global/ mutismo
10. Disartria:0 - articulação normal1 - disartria leve/ moderada2 - disartria grave
11. Negligência:0 - atenção normal1 - negligência parcial2 - negligência grave

ANEXO 3 – ESCALA MODIFICADA DE RANKIN
Grau 0. Assintomático.
Grau 1. Sintomas sem incapacidade. Capaz de realizar suas tarefas e atividadeshabituais prévias.
Grau 2. Incapacidade leve. Incapaz de realizar todas suas atividades habituais prévias,mas capaz de realizar suas necessidades pessoais sem ajuda.
Grau 3. Incapacidade moderada. Requer alguma ajuda para as suas atividades, mas écapaz de andar sem ajuda de outra pessoa.
Grau 4. Incapacidade moderada a grave. Incapacidade de andar sem ajuda,incapacidade de realizar suas atividades sem ajuda.
Grau 5. Incapacidade grave. Limitado a cama, incontinência, requer cuidados deenfermeiros e atenção constante.
Grau 6. Óbito.

ANEXO 4 – ÍNDICE DE BARTHEL
Alimentação:10 = independente. O paciente pode alimentar-se sozinho quando alguém coloca comida deforma alcançável. Ele consegue cortar a comida, servir-se de sal e pimenta e passar manteiga.5 = alguma ajuda é necessária ou o paciente é incapaz de alimentar-se sozinho em umdeterminado tempo.
Movimentação da cadeira de rodas para cama e retornar ou levantar e deitar na cama ecadeira sem cadeira de rodas:15 = independente em todas as fases desta atividade.10 = necessita (mesmo que seja pequena ajuda) em algum passo desta atividade ou o pacientenecessita de ajuda física para transferir-se.5 = paciente consegue sentar-se sem ajuda de uma segunda pessoa, mas necessita deassistência física para transferência.
Higiene pessoal:5 = o paciente consegue lavar as mãos e face, pentear os cabelos, escovar os dentes e barbear-se. Ele deverá ser capaz de utilizar giletes, inclusive encaixando-as no barbeador e depois asguardando sem ajuda. Mulheres são capazes de maquiar-se, mas não de fazer penteados.
Asseio pessoal:10 = o paciente é capaz de entrar e sair do banheiro, retirar e colocar suas roupas e usar papelhigiênico sem ajuda. Ele pode usar barras de apoio ou outro objeto para apoiar-se. (Se fornecessário usar cadeira higiênica ao invés de banheiro, o paciente deve ser capaz de esvaziá-lae limpá-la)5 = o paciente necessita de ajuda para despir-se ou usar o papel higiênico.
Banho:5 = o paciente é capaz de usar banheira ou chuveiro de forma completa. Ele deve ser capaz derealizar todos os passos envolvidos em qualquer método escolhido sem estar presente outrapessoa.
Andar:15 = paciente pode andar sem ajuda ou supervisão. Ele pode usar muletas e ficar em pé ousentado com elas.10 = paciente necessita ajuda ou supervisão em qualquer dos passos acima, mas podecaminhar até 50 metros com pequena ajuda.5 = paciente pode andar curtas distâncias (menos que 50 metros) com assistência física ousupervisão.5 = utilizar cadeira de rodas, se a pessoa não pode deambular independentemente. Ele deveser capaz de realizar manobras para a mesa, cama, banheiro, etc. Ele deve ser capaz deutilizar, manualmente a cadeira por até 50 metros ou utilizar cadeira com movimentaçãoelétrica.
Subir e descer escadas:10 = o paciente é capaz de subir e descer escadas de forma segura, sem ajuda ou supervisão.Ele pode e deve usar corrimão, bengala e muletas, quando necessário. Ele deve ser capaz decarregar as muletas ou bengala, ao subir e descer escadas.5 = paciente necessita de ajuda ou supervisão para realizar qualquer tarefa supracitada.

Vestindo-se e despindo-se:10 = paciente é capaz de colocar e retirar toda a roupa, abotoando ou utilizando qualquermétodo adaptativo e realizar laços. Esta atividade inclui colocar e remover muletas, quandoprescrito. Algumas vestimentas especiais como suspensórios, sapatos sem cadarços ou roupasque abrem na frente podem ser usados quando necessário.5 = paciente necessita de ajuda para colocar e remover qualquer peça de roupa. Ele deve sercapaz de realizar pelo menos metade do trabalho sozinho. Ele deve realizar em um tempoplausível.
Continência fecal:10 = paciente é capaz de controlar suas evacuações ou independentemente manejar seuprograma fecal e sem acidentes.5 = paciente tem acidentes ocasionais ou necessita de ajuda para manejar seu programa fecal.
Continência urinária:10 = paciente é capaz de controlar sua bexiga dia e noite. Pacientes que usam acessóriosexternos devem ser capazes de colocá-los e retirá-los independentemente, esvaziar e lavar abolsa e permanecer seco noite e dia.5 = paciente tem acidentes ocasionais ou não pode esperar pela cadeira higiênica ou ir aobanheiro a tempo ou necessita de ajuda com acessórios externos.

ANEXO 5 – ARTIGO PUBLICADO
ANEXO 6 – ARTIGO ACEITO
ANEXO 7 – ARTIGO SUBMETIDO

ISSN: 1524-4539 Copyright © 2009 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online
72514Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
DOI: 10.1161/CIRCULATIONAHA.109.863084 2009;120;539-541 CirculationAndre
Wajnberg, Paulo Henrique Rosado de Castro, Rosalia Mendez-Otero and CharlesBianca Gutfilen, Regina Coeli dos Santos Goldenberg, Angelo Maiolino, Eduardo Lea Mirian Barbosa da Fonseca, Valeria Battistella, Gabriel Rodriguez de Freitas,
Intra-Arterial Delivery in a Patient With Chronic StrokeEarly Tissue Distribution of Bone Marrow Mononuclear Cells After
http://circ.ahajournals.org/cgi/content/full/120/6/539/DC1Data Supplement (unedited) at:
http://circ.ahajournals.org/cgi/content/full/120/6/539
located on the World Wide Web at: The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. E-mail:
Fax:Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters
http://circ.ahajournals.org/subscriptions/Subscriptions: Information about subscribing to Circulation is online at
by on August 24, 2009 circ.ahajournals.orgDownloaded from

Early Tissue Distribution of Bone Marrow MononuclearCells After Intra-Arterial Delivery in a Patient With
Chronic StrokeLea Mirian Barbosa da Fonseca, MD, PhD; Valeria Battistella, MD;
Gabriel Rodriguez de Freitas, MD, PhD; Bianca Gutfilen, PhD;Regina Coeli dos Santos Goldenberg, PhD; Angelo Maiolino, MD, PhD;
Eduardo Wajnberg, MD; Paulo Henrique Rosado de Castro;Rosalia Mendez-Otero, MD, PhD; Charles Andre, MD, PhD
A 24-year-old man with a cerebral infarct within the leftmiddle cerebral artery (MCA) territory was enrolled in a
study to assess the safety of autologous bone marrow mono-nuclear cell (BMMC) transplantation in patients with ische-mic stroke (NCT00473057). His National Institutes of HealthStroke Scale score was 7. Computed tomography (Figure 1A)and technetium-99m ethyl cysteinate dimer (99mTc ECD)single photon emission computed tomography (SPECT) (Fig-ures 1B and 2 and Movie I in the online-only Data Supple-ment) indicated the location of the infarct. Sixty-seven daysafter onset of symptoms, the patient underwent BMMCtransplantation. Bone marrow blood was aspirated under localanesthesia from both iliac crests and processed to isolate themononuclear cell fraction. A total of 5�108 BMMCs wassuspended into a volume of 10 mL, and 1 mL of the cellsuspension was radiolabeled with 99mTc (radioactivity 111MBq, physical half-life 6 hours), as described previously,1,2
and then added back to the unlabeled cell suspension. Aftercatheter navigation via femoral artery access under localanesthesia and conscious sedation, cells were injected into theM1 portion of the MCA, and the infusion was completedwithin �10 minutes. To monitor the fate of transplantedBMMCs, whole-body and planar scintigraphies were per-formed at 2, 24, and 48 hours after cell therapy. The patienthad no complications during the procedure or follow-up.
Planar and SPECT views revealed uptake and retention ofthe labeled BMMCs in the territory of the left MCA for up to48 hours (Figures 1C, 3, and 4 and Movie II in the online-onlyData Supplement). The remaining uptake occurred mainly inthe liver and spleen (Figure 4). To our knowledge, there hasbeen only 1 report of BMMC homing in cerebral infarction,which indicated the retention of BMMCs 8 hours afterintra-arterial injection in 1 patient in the subacute phase, 9
days after stroke.3 We here report for the first time themigration and homing of BMMCs to the brain of a patient inthe chronic phase of stroke, �2 months after the onset ofsymptoms. The mechanisms involved in the possible thera-peutic effect of BMMC therapy are still largely unknown, butaccumulating evidence from animal studies suggests thatthese cells may behave as minipumps producing cytokinesand/or trophic factors that support cell survival in the pen-umbra area and stimulate neurogenesis and angiogenesis,increasing brain remodeling and functional regeneration afterischemia.4 In vivo tracking of BMMCs after grafting is ofgreat importance because the retention of transplanted cells atthe site of the lesion may be critical for the success of celltherapy.3,4 In animal models, different methods have beenused to track the transplanted cells, and it has been suggestedthat signals that are involved in the transit of inflammatorycells to injured tissue may also direct the transplanted bonemarrow–derived cells.4 Our results indicate that labelingBMMCs with 99mTc is feasible and that noninvasive imagingmay be used to study the migration and homing of trans-planted cells in vivo in the setting of chronic stroke.
Figure 1. A, Computed tomography showing ischemic lesion inthe left MCA territory. B, Brain perfusion 99mTc ECD SPECTshowing left hypoperfusion. C, 99mTc BMMC brain SPECTrevealing accumulation of the BMMCs in the left brain hemi-sphere 2 hours after cell transplantation.
From Hospital Universitário Clementino Fraga Filho (L.M.B.d.F., V.B., G.R.d.F., B.G., A.M., E.W., P.H.R.d.C., C.A.) and Instituto de Biofísica CarlosChagas Filho (R.C.d.S.G., R.M.-O.), Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil.
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/cgi/content/full/120/7/539/DC1.Clinical trial registration information—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00473057.Correspondence to Lea Mirian Barbosa da Fonseca, MD, PhD, Hospital Universitário Clementino Fraga Filho, Departamento de Radiologia, subsolo,
Universidade Federal do Rio de Janeiro, Rua Professor Rodolpho Paulo Rocco 255, Ilha do Fundão, 21949-913, Rio de Janeiro, Brazil. [email protected]
(Circulation. 2009;120:539-541.)© 2009 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.109.863084
539
Images in Cardiovascular Medicine
by on August 24, 2009 circ.ahajournals.orgDownloaded from

Sources of FundingThis study was supported by grants from the Carlos Chagas FilhoFoundation for Research Support of the State of Rio de Janeiro to DrGutfilen (grant 180.011/2005) and to Dr Mendez-Otero (grant110.391/2007) and a grant from the Ministry of Health and Ministryof Science and Technology of Brazil to Dr Mendez-Otero (grant552201/2005-7).
DisclosuresNone.
References1. Carvalho AB, Quintanilha LF, Dias JV, Paredes BD, Mannheimer EG,
Carvalho FG, Asensi KD, Gutfilen B, Fonseca LM, Resende CM,Rezende GF, Takiya CM, de Carvalho AC, Goldenberg RC. Bone
marrow multipotent mesenchymal stromal cells do not reduce fibrosis orimprove function in a rat model of severe chronic liver injury. Stem Cells.2008;26:1307–1314.
2. Quintanilha LF, Mannheimer EG, Carvalho AB, Paredes BD, Dias JV,Almeida AS, Gutfilen B, Barbosa da Fonseca LM, Resende CM, RezendeGF, Campos de Carvalho AC, Goldenberg RC. Bone marrow celltransplant does not prevent or reverse murine liver cirrhosis. CellTransplant. 2008;17:943–953.
3. Correa PL, Mesquita CT, Felix RM, Azevedo JC, Barbirato GB, FalcãoCH, Gonzalez C, Mendonça ML, Manfrim A, de Freitas G, Oliveira CC,Silva D, Avila D, Borojevic R, Alves S, Oliveira AC Jr, Dohmann HF.Assessment of intra-arterial injected autologous bone marrow mono-nuclear cell distribution by radioactive labeling in acute ischemic stroke.Clin Nucl Med. 2007;32:839–841.
4. Mendez-Otero R, de Freitas GR, André C, de Mendonça ML, FriedrichM, Oliveira-Filho J. Potential roles of bone marrow stem cells in stroketherapy. Regen Med. 2007;2:417–423.
Figure 2. Transverse (A), sagittal (B), and coronal (C) images of99mTc ECD SPECT scintigraphy, demonstrating decreased perfu-sion in the left MCA territory.
Figure 3. Transverse (A), sagittal (B), and coronal (C) images of99mTc BMMC SPECT scintigraphy, demonstrating cell homing inthe left MCA territory 2 hours after cell transplantation.
540 Circulation August 11, 2009
by on August 24, 2009 circ.ahajournals.orgDownloaded from

Figure 4. Anterior whole-body scans performed 2 (A), 24 (B),and 48 hours (C) after infusion in the territory of the MCA showthe distribution of BMMCs labeled with 99mTc. Uptake in the leftbrain hemisphere is well visualized. The remaining activity wasdistributed mainly to the liver and spleen.
Barbosa da Fonseca et al Tracking Cell Therapy in Chronic Stroke 541
by on August 24, 2009 circ.ahajournals.orgDownloaded from

Migration and homing of bone-marrow mononuclear cells in chronic ischemic strokeafter intra-arterial injection
Lea Mirian Barbosa da Fonseca a,⁎, Bianca Gutfilen a, Paulo Henrique Rosado de Castro a, Valeria Battistella a,Regina C.S. Goldenberg b, Tais Kasai-Brunswick b, Claudia L.R. Chagas a, Eduardo Wajnberg a,Angelo Maiolino a, Sérgio Salles Xavier a, Charles Andre a, Rosalia Mendez-Otero b, Gabriel R. de Freitas a
a Hospital Universitário Clementino Fraga Filho, Departamento de Radiologia, subsolo, Universidade Federal do Rio de Janeiro, Ilha do Fundão, 21949-913, Rio de Janeiro, Brazilb Instituto de Biofísica Carlos Chagas Filho, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
a b s t r a c ta r t i c l e i n f o
Article history:Received 9 July 2009Revised 6 October 2009Accepted 15 October 2009Available online xxxx
Keywords:StrokeCell therapy99mTcScintigraphy
Cell-based treatments have been considered a promising therapy for neurological diseases. However,currently there are no clinically available methods to monitor whether the transplanted cells reach andremain in the brain. In this study we investigated the feasibility of detecting the distribution and homing ofautologous bone-marrowmononuclear cells (BMMCs) labeled with Technetium-99 m (99mTc) in a cell-basedtherapy clinical study for chronic ischemic stroke. Six male patients (ages 24–65 years) with ischemiccerebral infarcts within the middle cerebral artery (MCA) between 59 and 82 days were included. Cell doseranged from 1.25×108 to 5×108. Approximately 2×107 cells were labeled with 99mTc and intra-arteriallydelivered together with the unlabeled cells via a catheter navigated to the MCA. None of the patients showedany complications on the 120-day follow-up. Whole body scintigraphies indicated cell homing in the brain ofall patients at 2 h, while the remaining uptake was mainly distributed to liver, lungs, spleen, kidneys andbladder. Moreover, quantification of uptake in Single-Photon Emission Computed Tomography (SPECT) at2 h showed preferential accumulation of radioactivity in the hemisphere affected by the ischemic infarct inall patients. However, at 24 h homing could only distinguished in the brains of 2 patients, while in allpatients uptake was still seen in the other organs. Taken together, these results indicate that labeling ofBMMCs with 99mTc is a safe and feasible technique that allows monitoring the migration and engraftment ofintra-arterially transplanted cells for at least 24 h.
© 2009 Elsevier Inc. All rights reserved.
Introduction
Over the last decade, stem-cell-based therapy has been introducedas a promising attempt to improve recovery after stroke (Dobkin,2007, Kondziolka et al., 2005, 2000, Savitz et al., 2005). Autologousbone marrow-derived stem cells have been used more frequently,both in pre-clinical studies (Chopp and Li, 2002, Liu et al., 2006,Mezey, 2007, Tang et al., 2007) and in a few pilot and ongoing clinicaltrials (Bang et al., 2005, Mendez-Otero et al., 2007, Mendonca et al.,2006). In experimental models, it has been suggested that possibletherapeutic effects could be due to the production of trophic factors bybone marrow-derived cells and lead to an increase in angiogenesis,neurogenesis and synaptogenesis, allowing favorable remodeling ofthe brain (Chen et al., 2003, Chopp and Li, 2002).
Non-invasive in-vivo imaging of the transplanted cells may providebetter understanding ofmany unresolved issues in this field, such as theefficiency of different approaches to cell delivery and the correlationwith functional evaluation. Radioisotope cell labeling is a well-
established method that allows systemic monitoring of cells, and hasbeen applied in different clinical studies involving cell therapy formyocardial infarction (Goussetis et al., 2006, Hofmann et al., 2005, Kanget al., 2006, Penicka et al., 2007) and acute stroke (Correa et al., 2007).
In this study, we investigated the distribution and homing of intra-arterial-delivered radioactive-labeled bone-marrow mononuclearcells in patients enrolled in a research study to assess the safety ofthis procedure for chronic ischemic stroke.
Patients and methods
Patients
Six male patients (ages 24–65 years) with ischemic cerebralinfarcts within the territory of the middle cerebral artery (MCA) wereincluded in this non-randomized, open-label phase I clinical trial(NCT00473057). The following criteria were required for patientenrollment: (1) age between 18 and 75 years, (2) ischemic stroke inthe MCA territory within the last 90 days evidenced by computedtomography (CT) or magnetic-resonance imaging (MRI); (3) recan-alization of the involved MCA as assessed by transcranial Doppler
Experimental Neurology xxx (2009) xxx–xxx
⁎ Corresponding author. Fax: +55 21 2562 2399.E-mail address: [email protected] (L.M. Barbosa da Fonseca).
YEXNR-10373; No. of pages: 7; 4C: 4, 5
0014-4886/$ – see front matter © 2009 Elsevier Inc. All rights reserved.doi:10.1016/j.expneurol.2009.10.010
Contents lists available at ScienceDirect
Experimental Neurology
j ou rna l homepage: www.e lsev ie r.com/ locate /yexnr
ARTICLE IN PRESS
Please cite this article as: Barbosa da Fonseca, L.M., et al., Migration and homing of bone-marrow mononuclear cells in chronic ischemicstroke after intra-arterial injection, Exp. Neurol. (2009), doi:10.1016/j.expneurol.2009.10.010

(TCD) studies; and (4) a score between 4 and 17 according to theNational Institutes of Health Stroke Scale (NIHSS). We excludedpatients to whom any of the following criteria applied: (1) carotidstenosis ( N50%, by Doppler studies) ipsilateral to the stroke, (2)neurological worsening (N4 points in the NIHSS ) before injection, dueto either edema or intracerebral hemorrhage, (3) thrombophilias orprimary hematological diseases, (4) previous stroke with modifiedRankin Scale N2, (5) neurodegenerative disorders, (6) auto-immunedisorders, (7) intracardiac thrombus, (8) sepsis (according to the1992 criteria of the Society of Critical Care Medicine and the AmericanCollege of Chest Physicians), (9) history of neoplasia or othercomorbidity that could impact the patient's short-term survival,(10) bone disorders that could increase the risk of the bone-marrowharvesting procedure, (11) renal failure (creatinine N2 mg/ml), (12)liver failure, (13) lacunar stroke, (14) life-support dependence, (15)pregnancy or previous participation in other clinical trials, (16)difficulty in obtaining vascular access for percutaneous procedure,(17) any condition that in the judgment of the investigator wouldplace the patient at undue risk.
The Research Ethics Committee of the Institution and the NationalCommittee of Ethics and Scientific Research approved the studyprotocol. Written informed consent was obtained from all patients.They were informed in detail about the nature of the procedure andthe radiolabeling technique.
Bone-marrow aspiration, cell separation and labeling withTechnetium-99m
Bonemarrow (80ml) was aspirated under local anesthesia from theposterior iliac crest. BMMCs were isolated by density gradient on Ficollat 400×g for 30 min (Ficoll-Paque Plus 1.077, 1:2, AmershamBiosciences, São Paulo, Brazil). Mononuclear cellswerewashed in salinecontaining 5% human serum albumin and filtered through 100-μmnylon mesh to remove cell aggregates. After washing, counting andviability testing, the cells were resuspended in 10 ml of saline solutionwith 5% autologous serum. For each patient, 2×107 cells were labeledwith 99mTc based on previously published protocols (Carvalho et al.,2008, Gutfilen et al., 2006, 1999, Lopes de Souza et al., 2004, Quintanilhaet al., 2008). All the procedures for cell preparation and labeling werecarriedout in a laminarflow. In short, 500 μl of sterile SnCl2 solutionwasadded to the cell suspension in 0.9% NaCl, and the mixture wasincubated at room temperature for 10 min. Then, 45 mCi 99mTc wasadded and the incubation continued for another 10 min. Aftercentrifugation (500×g for 5 min), the supernatant was removed andthe cells were washed again in saline solution. The pellet wasresuspended in saline solution. Viability of the labeled cellswas assessedby the trypan blue exclusion test, and was estimated to be greater than93% in all cases. Labeling efficiency (%) was calculated by the activity inthe pellet divided by the sum of the radioactivity in the pellet plussupernatant, and was estimated to be greater than 90% in all cases.
Flow-cytometry analysis and fibroblast colony-forming assay
Isolated mononuclear bone-marrow cells were characterized byflow-cytometry analysis of specific surface antigens. Cells wereincubated for 20 min at room temperature with primary antibodiesconjugated with fluorescein isothiocyanate (FITC), phycoerythrin(PE), allophycocyanin (APC), peridinin chlorophyll protein (PercP)and phycoerythrin cyano 7 (PE-Cy7). The markers tested included:pan-leukocyte: CD45 (Immunostep); pan T cell: CD3 (BD BiosciencesPharmigen); cytotoxic T cell: CD8 (BD Biosciences Pharmigen); helperT cell: CD4 (BD Biosciences Pharmigen); pan B cell: CD19 (BDBiosciences Pharmigen); NK cell: CD56 (BD Biosciences Pharmigen);promonocyte: CD64 (Immunotech); monocyte: CD14 (IQP); hemato-poietic progenitor cells: CD117 (BD Biosciences Pharmigen) and CD34(BD Biosciences Pharmigen); mesenchymal cells: CD105 (Immuno-
step), CD73 (BD Biosciences Pharmigen) and CD90(BD BiosciencesPharmigen); neutrophils: CD31(BD Biosciences Pharmigen) and CD33(BD Biosciences Pharmigen); anti HLA-DR (MHC-II, BD BiosciencesPharmigen). After staining, erythrocyteswere lysedwith the B&D LysisBuffer Solution. Data acquisition was performed on a BD FACS CANTOcytometer (Beckton & Dickson) and analyzed with the “Paint-a-Gate”software. A fibroblast colony-forming assay was performed todetermine the presence of putative progenitor cells of mesenchymallineages, as previously described (Castro-Malaspina et al., 1980).
Cell transplantation
Cells labeled as described above were added back to the totalmononuclear cell suspension (final volume of 10 ml). Femoral arterialpunctures were done in all patients. A 6 Fr. Guiding catheter (Envoy-Cordis, Miami, Florida; or a Guider Soft tip, Boston Scientific, TargetTherapeutics, Fremont, California) was used. Patients underwentanticoagulation with intravenous heparin to obtain an activatedclotting time of two to three times baseline. A digital cerebralangiography was performed (Angiostar, Siemens Medical Systems,Erlangen, Germany) to allow visualization of the intracranialvasculature before injection and monitoring of flow normality andvessel patency. A large-inner-diameter micro catheter (SL 1018Boston Scientific, Target Therapeutics, Fremont, California) wasnavigated to the M1 portion of the middle cerebral artery, and theinfusion was done at the rate of approximately 1 ml/min.
Imaging
Whole-body and planar images were captured using a MillenniumGE camera (General Electric Medical Systems, Milwaukee, Wiscon-sin). Acquisition protocols were performed at 2 h and 24 h after celltherapy.Whole-body images were acquired for 20min in anterior andposterior views, using a dual-head whole-body scanner with high-resolution, low-energy collimator. Planar images were acquired for10 min, matrix 256×256, in anterior, right and left lateral, andposterior views. Single-Photon-Emission Computed Tomography(SPECT) was performed with two 180° opposed rotating detectorswith low-energy high-resolution collimators. The software andhardware for image reconstruction was a Xeleris-GE processingworkstation for reconstruction of the SPECT image data. Projectionswere collected over 24 min, with each detector rotating 180 to make acomplete 360 revolution in a circular orbit with the patient placed inthe supine position. Image volumes were reconstructed using theOSEM algorithm with axial smoothing and a Butterworth filter withan order of five and a cutoff of 0.45. Image volumes consisted of64×64×64 voxels each measuring 4.38 mm3. The detector distanceranged from 14 cm to 20 cm during rotation, resulting in a spatialresolution FWHM (full width at half-max) of approximately 12 mm.
For each patient, regions of interest were drawn for the brain, liver,spleen, lungs, kidneys, bladder, and for the whole body, and theradioactive counts were automatically quantified for these regions inwhole body planar images at 2 h after cell injection. Uptake wasdefined as the percentage of organ-originated number of countscompared to the total number of counts in the whole body. To allowbetter discrimination of the uptake in the brain, regions of interestcorresponding to the left and right hemispheres were drawn in SPECTimages and the radioactive counts were automatically quantified.Uptake in hemispheres ipsilateral and contralateral to the lesion wasdefined as the percentage of hemisphere-originated number of countscompared to the total number of counts in both hemispheres.
CT images were acquired before cell transplantation with a 40–detector row scanner (Brilliance-40, Philips Medical Systems).Volumetric analysis was performed to measure the approximatevolumes of the infarcted areas. Volumes were obtained bymultiplyingthe measured area per slice by the section thickness. SPECT and CT
2 L.M. Barbosa da Fonseca et al. / Experimental Neurology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Please cite this article as: Barbosa da Fonseca, L.M., et al., Migration and homing of bone-marrow mononuclear cells in chronic ischemicstroke after intra-arterial injection, Exp. Neurol. (2009), doi:10.1016/j.expneurol.2009.10.010

images were exported by DICOM protocol, and transferred to aMacintosh computer (MacOS X, version 10.4). Imageswere fusedwithdedicated image processing software (OsiriX imaging software,version 3.6, Geneva, Switzerland).
Clinical evaluation
Patients underwent neurological examination at admission, on theday of transplantation and at 3, 7, 30, 60, 90 and 120 days after cellinfusion. The examination included the Barthel Index, the modifiedRanking scale and the National Institutes of Health Stroke Scale.Laboratory tests (complete blood count and biochemical tests forurea, creatinine and electrolytes) were also performed at the sametime-points. An electroencephalogram (EEG) was performed within7 days of cell transplantation.
Statistical analysis
Because of the small sample size, the analysiswasmostly descriptive.The descriptive statistics of cell characteristics on FACS are given asmean values with standard deviation. Pearson and Spearman correla-tion tests were used to assess the relationship between total brainuptake and different variables (age, time from onset to cell therapy,number of injected cells, lesion volume and ipsilateral hemisphereuptake). Probability values of 0.05 or less were considered to indicatestatistical significance. Statistical analysis was performed with the SPSS17 (SPSS Science) statistical software package for Windows.
Results
Patients
The patient characteristics are presented in Table 1. All individualshad cerebral infarcts that involved the MCA territory as documented
by neuroimaging exams. Patients received between 1.25×108 and5×108 mononuclear cells, and cell transplantation took placebetween 59 and 82 days after the stroke. Clinical, laboratory andelectroencephalographic evaluations showed no adverse effectsduring the procedure or follow-up, and no patient scored worst onthe BI, mRS, or NIHSS tests. The cell immunophenotype is presented inTable 2.
Imaging
Whole-body scans obtained 2 h after transplantation of labeledBMMCs showed uptake in the brains of all patients, which rangedfrom 0.6% to 5.1 % when compared to the activity in the whole body.The location of cell homing could be better visualized in SPECT imagesthan in whole-body planar images. Transverse views of SPECTs, CTsand SPECT/CT fusion images for two representative patients areshown in Fig. 1. Quantification of cell uptake in SPECT imagesindicated preferential uptake on the side of the lesion in all patients(Table 3). Nevertheless, these differences were widely variable,ranging from 58% to 98% of total brain uptake (Table 3). Theremaining cell uptake was distributed mainly to the liver, lungs,spleen and kidneys in all patients (Table 3). Due to the 6-h half-life of99mTc, image resolution was greatly decreased at 24 h after celltransplantation, and regions of interest could not be adequatelydetermined to allow quantification of uptake in different organs (Fig.2). At 24 h, uptake could only be visualized in the brains of patients 1and 3, while in all patients uptake was seen in the liver, lungs, spleen,kidneys and bladder. Fig. 2 illustrates the whole-body images fromone of the patients in which cells could not be identified in the brain at24 h; and Fig. 3 shows brain planar views of one patient in whichuptake could be identified at 24 h. The presence of free 99mTc wasexcluded by thyroid region planar nuclear imaging. Movies 1 and 2correspond to dynamic three-dimensional SPECT images, demon-strating cell homing in the left MCA territory 2 h after cell
Table 1Patient characteristics.
Characteristics Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
Sex/age (years) M/24 M/65 M/47 M/65 M/57 M/47Infarct location Left Right Left Left Right RightNIHSS at admission 9 7 4 13 9 13Time from onset toBMMC infusion (days)
67 82 62 72 59 73
N° of injected cells 5×108 1.25×108 3.9×108 4×108 3.2×108 1×108
Lesion volume (cm3) 116 47 17 71 181 213
BMMC: Bone-marrow mononuclear cells; NIHSS: National Institutes of Health Stroke Scale.
Table 2Cell immunophenotype.
CD markers Phenotype % No of cells×107
CD45lowCD34highSSC↓ Hematopoietic stem cells 1.60±0.83 11.80±2.17CD45lowCD34+CD19+ B-cell progenitors 1.30±0.95 0.37±0.16CD45+CD34-CD33+CD64+CD14- Promonocytes 0.78±0.47 0.22±0.08CD105+CD90highCD73+CD45-CD34- Mesenchymal stem cells 0.12±0.09 0.03±0.01CD105+CD90highCD73+CD45-CD34+ Endothelial stem cells 0.04±0.07 0.01±0.01CD45+CD34-CD64+CD14+ Monocytes 4.45±3.97 1.28±0.68CD45+CD34-CD3+ T Lymphocytes 8.75±4.80 2.51±0.82CD45+CD34-CD3+CD4+ Helper T cells 5.84±3.87 1.68±0.67CD45+CD34-CD3+CD8+ Cytotoxic T cells 2.32±1.57 0.67±0.27CD45+CD34-CD3-CD19+ B cells 2.32±1.56 0.67±0.27CD45+CD34-CD56+ NK cells 7.86±3.076 2.26±0.53
Functional assay No of colonies×106 BMMC seeded
Fibroblast Colony-forming assay 35.75±7.63
The indicated percentages of immune cell subtypes have been calculated using the Paint-a-Gate PRO software (BD Biosciences), which displays a combination of the morphologicalcharacteristics (side scatter and forward scatter) and the specific CD marker expression, thus allowing a multiparametric analysis and identification of the cell subtype percentages.
3L.M. Barbosa da Fonseca et al. / Experimental Neurology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Please cite this article as: Barbosa da Fonseca, L.M., et al., Migration and homing of bone-marrow mononuclear cells in chronic ischemicstroke after intra-arterial injection, Exp. Neurol. (2009), doi:10.1016/j.expneurol.2009.10.010

transplantation in patients 3 and 4, respectively. Statistical analysisindicated that brain uptake at 2 h seemed to be inversely related toage (r=−0.883; p=0.02). Also, greater uptake in the brain wasrelated to a preferential uptake in the lesion's hemisphere (r=0.869;p=0.025). Volume of lesion (r=0.057; p=0.914), time from onsetto infusion (r=−0.314; p=0.544) and the number of cells injected(r=0.543; p=0.266) did not seem to be related to brain uptake.
Discussion
Bone-marrow mesenchymal stem cells (MSCs) and mononuclearcells (BMMCs) increase functional outcomes in animal models ofstroke when delivered by intravenous, intracerebral and intra-arterialroutes (Chen et al., 2001, 2003, Chopp and Li, 2002, Giraldi-Guimaraeset al., 2009, Kamiya et al., 2008, Li et al., 2001, 2000). It has beenshown that bone marrow cells target the ischemic lesion, and this isthought to be mediated by injury-induced chemokines (Hill et al.,2004, Shen et al., 2007a,b). Current preclinical evidence indicates thatthe main mechanism of cell-based therapy is not by direct cellreplacement, but by trophic, anti-inflammatory and immunomodu-latory effects that have an acute but persistent effect on the brainbefore these cells die (Barnabe et al., 2009, Bliss et al., 2007, Hess and
Borlongan, 2008, Mendez-Otero et al., 2007). Therefore, long-termcell persistence and engraftment in the brainmay not be necessary fora therapeutic effect (Bliss et al., 2007, Hess and Borlongan, 2008,Mendez-Otero et al., 2007). Cells may not even need to enter the brainto elicit an effect, but rather act in the periphery to increase trophic-factor expression in the brain, (Borlongan et al., 2004, Sarnowska etal., 2009) and positive effects have been seen even when cell injectiontakes place 1 month after the stroke (Shen et al., 2007a,b, Yasuhara etal., in press).
Radioisotope cell labeling is a well-established method that allowssystemic monitoring of cells in nuclear-medicine studies (Palestro etal., 2009) , and has already been applied for tracking cells in celltherapy for myocardial infarction (Goussetis et al., 2006, Hofmann etal., 2005, Kang et al., 2006, Penicka et al., 2007) and acute stroke(Correa et al., 2007) in humans. The 6-h half-life of 99mTc is animportant advantage over the half-life of 110 min of 18F-fluorodeox-yglycose (FDG). 111-Indium-oxine, another commonly used radio-pharmaceutical, allows cell tracking for up to 96 h, but hasdisadvantages that include suboptimal photon energies, low resolu-tion images and the 18- to 24-h interval between injection andimaging that is usually required (Banerjee et al., 2005, Palestro et al.,2009). 99mTc allows imaging for 24–48 h and results in higher image
Fig. 1. Transverse views of SPECTs (upper row), CTs (middle row) and SPECT/CT fusion images (lower row) of patients 3 (A) and 6 (B).
Table 3Quantification of uptake in different regions at 2 h after cell transplantation in percentages.
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Mean±SD
Uptake quantified in whole body planar imagesBrain/whole body 5.1 0.7 1.5 0.5 0.9 1.4 1.68±1.71Liver/whole body 42.4 39.9 47.7 38.5 48.7 44.2 43.56±4.10Spleen/whole body 5.2 3.1 2.2 4.1 5.6 3.7 3.98±1.27Kidneys/whole body 3.6 4.1 7.3 2.4 5.9 2.8 4.35±1.89Lungs/whole body 7.8 6.6 4.7 9.1 8.8 6.2 7.20±1.68Bladder/whole body 8.7 8.1 10.2 7.9 9.4 9.8 9.01±0.93
Uptake quantified in Brain SPECT imagesIpsilateral hemisphere/brain 97.8 65.7 82.2 77.4 58.3 79.2 76.76±13.72Contralateral hemisphere/brain 2.2 34.3 17.8 22.6 41.7 20,8 23.23±13.72
Uptake in the brain, liver, spleen, kidneys, lungs and bladder was defined as the percentage of organ-originated number of counts compared to the total number of counts in wholebody planar images 2 h after cell transplantation.To allow better discrimination of the uptake in the brain than in whole body planar images, uptake in hemispheres ipsilateral and contralateral to the lesion was defined as thepercentage of hemisphere-originated number of counts compared to the total number of counts in both hemispheres in SPECT images 2 h after cell transplantation.
4 L.M. Barbosa da Fonseca et al. / Experimental Neurology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Please cite this article as: Barbosa da Fonseca, L.M., et al., Migration and homing of bone-marrow mononuclear cells in chronic ischemicstroke after intra-arterial injection, Exp. Neurol. (2009), doi:10.1016/j.expneurol.2009.10.010

resolution and a lower radiation burden to the patient (Banerjee et al.,2005, Palestro et al., 2009).
In preclinical models, direct cell labeling with contrast agents suchas superparamagnetic iron oxides (SPIO) for MRI allows cell trackingfrom a few days to several weeks after transplantation (Budde andFrank, 2009, Lee et al., 2008, Modo et al., 2005). Moreover, thistechnique imaging provides higher spatial resolution and directanatomical correlation (Budde and Frank, 2009, Lee et al., 2008, Modoet al., 2005). Cell tracking with MRI suffers from common limitationsobserved with exogenous cell tagging, such as the sensitivity of theimaging technique, dilution of the contrast with cell division, andpotential transfer of the magnetic label to tissue macrophages (Buddeand Frank, 2009, Lee et al., 2008, Modo et al., 2005). Currently therehave been only 4 clinical studies in the literature involving a total of24 patients using magnetically labeled cells and MRI to monitor themigration of cells to target tissue (Callera and de Melo, 2007, de Vrieset al., 2005, Toso et al., 2008, Zhu et al., 2006) and at this timesuperparamagnetic or paramagnetic agents are not approved byregulatory agencies for cell labeling (Budde and Frank, 2009, Lee et al.,2008, Liu and Frank, 2009, Modo et al., 2005).
In humans, preliminary data from two Phase I clinical trialsinvolving intra-arterial injection of BMMCs for acute ischemic stroke(3–10 days post-ictus) with a total of 25 patients have suggested theprocedure is feasible and safe (Correa et al., 2007, Freitas et al., 2006,
Friedrich et al., 2006, Mendonca et al., 2006), but the final reports havenot been published. In one of these studies, one patient received cellslabeled with 99mTc-HMPAO, and whole-body scintigraphy and SPECTindicated cell accumulation in the brain 8 h after cell transplantation(Correa et al., 2007). Another Phase I study treated 5 patients with atotal of 1×108 intravenous bone marrow autologous MSCs in twodoses at 4–5 and at 7–9 weeks after stroke and found the procedure tobe feasible and safe (Bang et al., 2005).
Nonetheless, the safety and feasibility of BMMC injection in chronicstroke, as well as cell labeling, have never been studied in humans.Data from pre-clinical studies with acute ischemic models comparingdifferent administration routes suggest that there are differences incell retention rate (Lappalainen et al., 2008, Walczak et al., 2008).Intracerebral injection usually leads to poor cell distribution through-out the lesion (Li et al., 2000, Walczak et al., 2008), and intra-arterialinjection of BMMCs and MSCs provides greater cell retention whencompared to intravenous injection (Kamiya et al., 2008, Lappalainen etal., 2008, Walczak et al., 2008). Nevertheless, there are no reports onthe percentage of BMMCs grafted after intra-arterial injection, andonly limited reports for MSCs, where cell homing varied from 1%(Lappalainen et al., 2008) to 21% (Li et al., 2001). A recent studysuggested that intra-arterial injection of MSCs led to wide variation incerebral engraftment, and 17% of animals had no cells detectable in thebrain. The same study also suggested that high cerebral engraftmentrates of MSCs were associated with impeded cerebral blood flow asmeasured by laser Doppler flow (Walczak et al., 2008). Notwithstand-ing, there may be significant differences, depending on the ratiobetween the diameter of cells injected and the capillary size(Lappalainen et al., 2008, Walczak et al., 2008). Furthermore, thiseffect may have been increased by cerebral edema, because cellinjectionwas performed 30min after the stroke (Walczak et al., 2008),and therefore further studies are warranted to assess these questions.Early data from a clinical trial investigating the safety and feasibility ofBMMCs for acute stroke monitored cerebral blood flow by TCD andEEG, and found no evidence of embolization or electroencephalo-graphic changes (Freitas et al., 2006, Mendonca et al., 2006).
The total number of cells injected was the maximum obtainedfrom 80 ml of bone-marrow aspiration, and varied according to eachpatient (1.25×108 to 5×108). These differences in cell quantity werein accordance with the interval approved for this protocol. This celldose was consistent with other studies involving intra-arterial BMMCinjection in ischemic myocardial infarction (Huikuri et al., 2008,
Fig. 3. Anterior and left lateral views of brainplanar scans indicatehomingof BMMCsat 2h(A and B, respectively) and 24 h (C and D, respectively) after cell injection in patient 3.
Fig. 2. Anterior whole-body scans performed 2 h (A) and 24 h (B) after cell injection inthe territory of the MCA show the distribution of BMMCs labeled with 99mTc in patient4. Uptake in the left brain hemisphere could only be distinguished at 2 h. The remainingactivity was distributed mainly to the liver and spleen at 2 h and 24 h. Arrows indicatethe location of the liver, lungs, spleen, kidneys and bladder.
5L.M. Barbosa da Fonseca et al. / Experimental Neurology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Please cite this article as: Barbosa da Fonseca, L.M., et al., Migration and homing of bone-marrow mononuclear cells in chronic ischemicstroke after intra-arterial injection, Exp. Neurol. (2009), doi:10.1016/j.expneurol.2009.10.010

Lunde et al., 2006, Meyer et al., 2006, Penicka et al., 2007, Strauer et al.,2005, Tendera et al., 2009) and cerebral infarction (Correa et al., 2007,Mendonca et al., 2006). The transplanted cell population wascharacterized using a well-defined set of phenotypic markers, andwe observed many phenotypes that included different progenitorcells. Moreover, the functional characterization of fibroblastic likecells confirmed the presence of putative progenitor cells of mesen-chymal lineages.
We have previously reported preliminary data from this study thatindicated that the procedure was safe (Battistella et al., 2008) and thatthe cells labeled with 99mTc migrated to the brain of the first patientenrolled (Barbosa da Fonseca et al., 2009). Here, we provide furtherevidence that BMMC homing occurs in the brain after intra-arterialinjection in chronic stroke. Furthermore, we provide for the first timethe quantification of cell uptake in the brain and in other organs aftercell therapy for stroke. A study with an animal model of stroke hassuggested that the abundance and responsiveness of bone marrowprogenitor cells to gradients of factors such as Stromal Derived Factor-1 may decrease with age and reduce the chemoattraction of such cellsto the damaged tissue (Kucia et al., 2006). However, it is not currentlypossible to explain the wide variability of homing between patients,and there are probably multiple variables involved that remain to beinvestigated in future studies.
In summary, we would like to suggest that non-invasive imagingmodalities such as the one described in this study can be used tomonitor the delivery and tracking of cells, and may improveunderstanding of possible functional responses in the setting ofchronic stroke. Moreover, the advantages offered by other imagingmodalities, such as cell labelingwith SPIO forMRI, could be used in thefuture in conjunction with SPECT to provide further information oncell homing.
Acknowledgments
The authors thank Dr. Daniel Richard Mercante and Dr. CristianeAmaral GarciaMendonça for bone-marrowharvesting. Dr. JanetW. Reidrevised the English text. This study was supported by grants from theFundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio deJaneiro (FAPERJ) to Bianca Gutfilen (grant number 180.011/2005) andto Rosalia Mendez-Otero (grant number 110.391/2007); and a grantfrom the Ministry of Health and Ministry of Science and Technology ofBrazil to Rosalia Mendez-Otero (grant number 552201/2005-7).
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.expneurol.2009.10.010.
References
Banerjee, S.R., Maresca, K.P., Francesconi, L., Valliant, J., Babich, J.W., Zubieta, J., 2005.New directions in the coordination chemistry of 99mTc: a reflection on technetiumcore structures and a strategy for new chelate design. Nucl. Med. Biol. 32, 1–20.
Bang, O.Y., Lee, J.S., Lee, P.H., Lee, G., 2005. Autologous mesenchymal stem celltransplantation in stroke patients. Ann. Neurol. 57, 874–882.
Barbosa da Fonseca, L.M., Battistella, V., de Freitas, G.R., Gutfilen, B., Dos SantosGoldenberg, R.C., Maiolino, A., Wajnberg, E., Rosado de Castro, P.H., Mendez-Otero,R., Andre, C., 2009. Early tissue distribution of bonemarrowmononuclear cells afterintra-arterial delivery in a patient with chronic stroke. Circulation 120, 539–541.
Barnabe, G.F., Schwindt, T.T., Calcagnotto, M.E., Motta, F.L., Martinez Jr., G., de Oliveira,A.C., Keim, L.M., D'Almeida, V., Mendez-Otero, R., Mello, L.E., 2009. Chemically-induced RAT mesenchymal stem cells adopt molecular properties of neuronal-likecells but do not have basic neuronal functional properties. PLoS ONE e5222, 4.
Battistella, V., de Freitas, G., da Fonseca, L.M., Gutfilen, B., Goldenberg, R.C., Dias, V.J.,Mercante, D., Kasai-Brunswick, T., Bruno, F.P., Wajnberg, E., Mendez-Otero, R., Andre,C., 2008. Autologous bone marrow mononuclear cell transplantation in patients withischemic stroke, Abstracts of the 6th World Stroke Congress and Xth InternationalSymposium on Thrombolysis and Acute Stroke Therapy. Int. J. Stroke s1 (80), 3.
Bliss, T., Guzman, R., Daadi, M., Steinberg, G.K., 2007. Cell transplantation therapy forstroke. Stroke 38, 817–826.
Borlongan, C.V., Hadman, M., Sanberg, C.D., Sanberg, P.R., 2004. Central nervous systementry of peripherally injected umbilical cord blood cells is not required forneuroprotection in stroke. Stroke 35, 2385–2389.
Budde, M.D., Frank, J.A., 2009. Magnetic tagging of therapeutic cells for MRI. J. Nucl.Med. 50, 171–174.
Callera, F., de Melo, C.M., 2007. Magnetic resonance tracking of magnetically labeledautologous bone marrow CD34+ cells transplanted into the spinal cord via lumbarpuncture technique in patients with chronic spinal cord injury: CD34+ cells'migration into the injured site. Stem Cells Dev. 16, 461–466.
Carvalho, A.B., Quintanilha, L.F., Dias, J.V., Paredes, B.D.,Mannheimer, E.G., Carvalho, F.G.,Asensi, K.D., Gutfilen, B., Fonseca, L.M., Resende, C.M., Rezende, G.F., Takiya, C.M., deCarvalho, A.C., Goldenberg, R.C., 2008. Bone marrow multipotent mesenchymalstromal cells do not reduce fibrosis or improve function in a rat model of severechronic liver injury. Stem Cells 26, 1307–1314.
Castro-Malaspina, H., Gay, R.E., Resnick, G., Kapoor, N., Meyers, P., Chiarieri, D.,McKenzie, S., Broxmeyer, H.E., Moore, M.A., 1980. Characterization of human bonemarrow fibroblast colony-forming cells (CFU-F) and their progeny. Blood 56,289–301.
Chen, J., Li, Y., Wang, L., Zhang, Z., Lu, D., Lu, M., Chopp, M., 2001. Therapeutic benefit ofintravenous administration of bone marrow stromal cells after cerebral ischemia inrats. Stroke 32, 1005–1011.
Chen, J., Zhang, Z.G., Li, Y., Wang, L., Xu, Y.X., Gautam, S.C., Lu, M., Zhu, Z., Chopp, M.,2003. Intravenous administration of human bone marrow stromal cells inducesangiogenesis in the ischemic boundary zone after stroke in rats. Circ. Res. 92,692–699.
Chopp, M., Li, Y., 2002. Treatment of neural injury with marrow stromal cells. LancetNeurol. 1, 92–100.
Correa, P.L., Mesquita, C.T., Felix, R.M., Azevedo, J.C., Barbirato, G.B., Falcao, C.H.,Gonzalez, C., Mendonca, M.L., Manfrim, A., de Freitas, G., Oliveira, C.C., Silva, D.,Avila, D., Borojevic, R., Alves, S., Oliveira Jr., A.C., Dohmann, H.F., 2007. Assessmentof intra-arterial injected autologous bone marrowmononuclear cell distribution byradioactive labeling in acute ischemic stroke. Clin. Nucl. Med. 32, 839–841.
de Vries, I.J., Lesterhuis, W.J., Barentsz, J.O., Verdijk, P., van Krieken, J.H., Boerman, O.C.,Oyen, W.J., Bonenkamp, J.J., Boezeman, J.B., Adema, G.J., Bulte, J.W., Scheenen, T.W.,Punt, C.J., Heerschap, A., Figdor, C.G., 2005. Magnetic resonance tracking of dendriticcells in melanoma patients for monitoring of cellular therapy. Nat. Biotechnol. 23,1407–1413.
Dobkin, B.H., 2007. Behavioral, temporal, and spatial targets for cellular transplants asadjuncts to rehabilitation for stroke. Stroke 38, 832–839.
Freitas, G.R., Mendonca, M.L., Bezerra, D.C., Silva, S.A., Falcão, C.H., Gonzales, C., Moreira,R.C., Haddad, A.F., Tuche, F.A., Santos, D.P., Andre, C., Mesquita, C.T., Oliveira Jr., A.C.,Elia, V., Dohmann, H.J., Borojevic, R., Mendez-Otero, R., Dohmann, H.F., 2006. Safetyand feasibility of intra-arterial autologous bone marrow mononuclear celltransplantation in acute ischemic stroke. Abstracts of the International StrokeConference 2006. Stroke 37, 624–625.
Friedrich, M.A., Machado, D.C., Raupp, E., Araujo, M.D., Garicochea, B., Carrion, M.J.,Martins, M.P., Klamt, C.L., da Costa, J.C., 2006. Transplantation of autologous bonemarrowmononuclear cells in acute large middle cerebral artery stroke, Abstracts ofthe Joint World Congress on Stroke, Int. J. Stroke 1 (s1), 35.
Giraldi-Guimaraes, A., Rezende-Lima, M., Bruno, F.P., Mendez-Otero, R., 2009.Treatment with bone marrow mononuclear cells induces functional recovery anddecreases neurodegeneration after sensorimotor cortical ischemia in rats. BrainRes. 1266, 108–120.
Goussetis, E., Manginas, A., Koutelou, M., Peristeri, I., Theodosaki, M., Kollaros, N.,Leontiadis, E., Theodorakos, A., Paterakis, G., Karatasakis, G., Cokkinos, D.V.,Graphakos, S., 2006. Intracoronary infusion of CD133+ and CD133-CD34+selected autologous bone marrow progenitor cells in patients with chronicischemic cardiomyopathy: cell isolation, adherence to the infarcted area, andbody distribution. Stem Cells 24, 2279–2283.
Gutfilen, B., Lopes de Souza, S.A., Martins, F.P., Cardoso, L.R., Pinheiro Pessoa, M.C.,Fonseca, L.M., 2006. Use of 99mTc-mononuclear leukocyte scintigraphy innosocomial fever. Acta Radiol. 47, 699–704.
Gutfilen, B., Rossini, A., Martins, F.P., da Fonseca, L.M., 1999. Tc-99m-leukocytes—is it anintracellular labelling? J. Clin. Lab. Immunol. 51, 1–7.
Hess, D.C., Borlongan, C.V., 2008. Cell-based therapy in ischemic stroke. Expert Rev.Neurother. 8, 1193–1201.
Hill, W.D., Hess, D.C., Martin-Studdard, A., Carothers, J.J., Zheng, J., Hale, D., Maeda, M.,Fagan, S.C., Carroll, J.E., Conway, S.J., 2004. SDF-1 (CXCL12) is upregulated in theischemic penumbra following stroke: association with bonemarrow cell homing toinjury. J. Neuropathol. Exp. Neurol. 63, 84–96.
Hofmann, M., Wollert, K.C., Meyer, G.P., Menke, A., Arseniev, L., Hertenstein, B., Ganser,A., Knapp, W.H., Drexler, H., 2005. Monitoring of bone marrow cell homing into theinfarcted human myocardium. Circulation 111, 2198–2202.
Huikuri, H.V., Kervinen, K., Niemela, M., Ylitalo, K., Saily, M., Koistinen, P., Savolainen, E.R.,Ukkonen, H., Pietila, M., Airaksinen, J.K., Knuuti, J., Makikallio, T.H., 2008. Effects ofintracoronary injectionofmononuclear bonemarrowcells on left ventricular function,arrhythmia risk profile, and restenosis after thrombolytic therapy of acutemyocardialinfarction. Eur. Heart J. 29, 2723–2732.
Kamiya, N., Ueda, M., Igarashi, H., Nishiyama, Y., Suda, S., Inaba, T., Katayama, Y., 2008.Intra-arterial transplantation of bone marrowmononuclear cells immediately afterreperfusion decreases brain injury after focal ischemia in rats. Life Sci. 83, 433–437.
Kang, W.J., Kang, H.J., Kim, H.S., Chung, J.K., Lee, M.C., Lee, D.S., 2006. Tissue distributionof 18F-FDG-labeled peripheral hematopoietic stem cells after intracoronaryadministration in patients with myocardial infarction. J. Nucl. Med. 47, 1295–1301.
Kondziolka, D., Steinberg, G.K., Wechsler, L., Meltzer, C.C., Elder, E., Gebel, J., Decesare, S.,Jovin, T., Zafonte, R., Lebowitz, J., Flickinger, J.C., Tong, D., Marks, M.P., Jamieson, C.,
6 L.M. Barbosa da Fonseca et al. / Experimental Neurology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Please cite this article as: Barbosa da Fonseca, L.M., et al., Migration and homing of bone-marrow mononuclear cells in chronic ischemicstroke after intra-arterial injection, Exp. Neurol. (2009), doi:10.1016/j.expneurol.2009.10.010

Luu, D., Bell-Stephens, T., Teraoka, J., 2005. Neurotransplantation for patients withsubcortical motor stroke: a phase 2 randomized trial. J. Neurosurg. 103, 38–45.
Kondziolka, D., Wechsler, L., Goldstein, S., Meltzer, C., Thulborn, K.R., Gebel, J., Jannetta, P.,DeCesare, S., Elder, E.M.,McGrogan,M.,Reitman,M.A.,Bynum, L., 2000.Transplantationof cultured human neuronal cells for patients with stroke. Neurology 55, 565–569.
Kucia, M., Zhang, Y.P., Reca, R., Wysoczynski, M., Machalinski, B., Majka, M., Ildstad, S.T.,Ratajczak, J., Shields, C.B., Ratajczak, M.Z., 2006. Cells enriched in markers of neuraltissue-committed stem cells reside in the bone marrow and are mobilized into theperipheral blood following stroke. Leukemia 20, 18–28.
Lappalainen, R.S., Narkilahti, S., Huhtala, T., Liimatainen, T., Suuronen, T., Narvanen, A.,Suuronen, R., Hovatta, O., Jolkkonen, J., 2008. The SPECT imaging shows theaccumulation of neural progenitor cells into internal organs after systemicadministration in middle cerebral artery occlusion rats. Neurosci. Lett. 440, 246–250.
Lee, Z., Dennis, J.E., Gerson, S.L., 2008. Imaging stem cell implant for cellular-basedtherapies. Exp. Biol. Med. (Maywood) 233, 930–940.
Li, Y., Chopp, M., Chen, J., Wang, L., Gautam, S.C., Xu, Y.X., Zhang, Z., 2000. Intrastriataltransplantation of bone marrow nonhematopoietic cells improves functionalrecovery after stroke in adult mice. J. Cereb. Blood Flow Metab. 20, 1311–1319.
Li, Y., Chen, J., Wang, L., Lu, M., Chopp, M., 2001. Treatment of stroke in rat withintracarotid administration of marrow stromal cells. Neurology 56, 1666–1672.
Liu, W., Frank, J.A., 2009. Detection and quantification of magnetically labeled cells bycellular MRI. Eur. J. Radiol. 70, 258–264.
Liu, D.D., Shyu, W.C., Lin, S.Z., 2006. Stem cell therapy in stroke: strategies in basic studyand clinical application. Acta Neurochir. Suppl. 99, 137–139.
Lopes de Souza, S.A., Barbosa da Fonseca, L.M., Torres Goncalves, R., Salomao Pontes, D.,Holzer, T.J., Proenca Martins, F.P., Gutfilen, B., 2004. Diagnosis of renal allograftrejection and acute tubular necrosis by 99mTc-mononuclear leukocyte imaging.Trans. Proc. 36, 2997–3001.
Lunde, K., Solheim, S., Aakhus, S., Arnesen, H., Abdelnoor, M., Egeland, T., Endresen, K.,Ilebekk, A., Mangschau, A., Fjeld, J.G., Smith, H.J., Taraldsrud, E., Grogaard, H.K.,Bjornerheim, R., Brekke, M., Muller, C., Hopp, E., Ragnarsson, A., Brinchmann, J.E.,Forfang, K., 2006. Intracoronary injection of mononuclear bone marrow cells inacute myocardial infarction. N. Engl. J. Med. 355, 1199–1209.
Mendez-Otero, R., de Freitas, G.R., Andre, C., de Mendonca, M.L., Friedrich, M., Oliveira-Filho, J., 2007. Potential roles of bone marrow stem cells in stroke therapy. Regen.Med. 2, 417–423.
Mendonca, M.L., Freitas, G.R., Silva, S.A., Manfrim, A., Falcao, C.H., Gonzales, C., Andre, C.,Dohmann, H.F., Borojevic, R., Otero, R.M., 2006. Safety of intra-arterial autologousbonemarrowmononuclear cell transplantation for acute ischemic stroke. Arq. Bras.Cardiol. 86, 52–55.
Meyer, G.P., Wollert, K.C., Lotz, J., Steffens, J., Lippolt, P., Fichtner, S., Hecker, H., Schaefer,A., Arseniev, L., Hertenstein, B., Ganser, A., Drexler, H., 2006. Intracoronary bonemarrow cell transfer after myocardial infarction: eighteen months' follow-up datafrom the randomized, controlled BOOST (BOne marrOw transfer to enhance ST-elevation infarct regeneration) trial. Circulation 113, 1287–1294.
Mezey, E., 2007. Bone marrow-derived stem cells in neurological diseases: stones ormasons? Regen. Med. 2, 37–49.
Modo, M., Hoehn, M., Bulte, J.W., 2005. Cellular MR imaging. Mol. Imaging 4, 143–164.Palestro, C.J., Love, C., Bhargava, K.K., 2009. Labeled leukocyte imaging: current status
and future directions. Q. J. Nucl. Med. Mol. Imaging 53, 105–123.
Penicka, M., Lang, O., Widimsky, P., Kobylka, P., Kozak, T., Vanek, T., Dvorak, J., Tintera, J.,Bartunek, J., 2007. One-day kinetics of myocardial engraftment after intracoronaryinjection of bone marrow mononuclear cells in patients with acute and chronicmyocardial infarction. Heart 93, 837–841.
Quintanilha, L.F., Mannheimer, E.G., Carvalho, A.B., Paredes, B.D., Dias, J.V., Almeida, A.S.,Gutfilen, B., Barbosa da Fonseca, L.M., Resende, C.M., Rezende, G.F., Campos deCarvalho, A.C., Goldenberg, R.C., 2008. Bone marrow cell transplant does notprevent or reverse murine liver cirrhosis. Cell Transplant 17, 943–953.
Sarnowska, A., Braun, H., Sauerzweig, S., Reymann, K.G., 2009. The neuroprotectiveeffect of bone marrow stem cells is not dependent on direct cell contact withhypoxic injured tissue. Exp. Neurol. 215, 317–327.
Savitz, S.I., Dinsmore, J., Wu, J., Henderson, G.V., Stieg, P., Caplan, L.R., 2005.Neurotransplantation of fetal porcine cells in patients with basal ganglia infarcts:a preliminary safety and feasibility study. Cerebrovasc. Dis. 20, 101–107.
Shen, L.H., Li, Y., Chen, J., Cui, Y., Zhang, C., Kapke, A., Lu, M., Savant-Bhonsale, S., Chopp,M., 2007a. One-year follow-up after bone marrow stromal cell treatment inmiddle-aged female rats with stroke. Stroke 38, 2150–2156.
Shen, L.H., Li, Y., Chen, J., Zacharek, A., Gao, Q., Kapke, A., Lu, M., Raginski, K., Vanguri, P.,Smith, A., Chopp, M., 2007b. Therapeutic benefit of bone marrow stromal cellsadministered 1 month after stroke. J. Cereb. Blood Flow Metab. 27, 6–13.
Strauer, B.E., Brehm, M., Zeus, T., Bartsch, T., Schannwell, C., Antke, C., Sorg, R.V., Kogler,G., Wernet, P., Muller, H.W., Kostering, M., 2005. Regeneration of human infarctedheart muscle by intracoronary autologous bone marrow cell transplantation inchronic coronary artery disease: the IACT Study. J. Am. Coll. Cardiol. 46, 1651–1658.
Tang, Y., Yasuhara, T., Hara, K., Matsukawa, N., Maki, M., Yu, G., Xu, L., Hess, D.C.,Borlongan, C.V., 2007. Transplantation of bone marrow-derived stem cells: apromising therapy for stroke. Cell Transplant 16, 159–169.
Tendera, M., Wojakowski, W., Ruzyllo, W., Chojnowska, L., Kepka, C., Tracz, W.,Musialek, P., Piwowarska, W., Nessler, J., Buszman, P., Grajek, S., Breborowicz, P.,Majka, M., Ratajczak, M.Z., 2009. Intracoronary infusion of bone marrow-derivedselected CD34+CXCR4+ cells and non-selected mononuclear cells in patients withacute STEMI and reduced left ventricular ejection fraction: results of randomized,multicentre Myocardial Regeneration by Intracoronary Infusion of SelectedPopulation of Stem Cells in Acute Myocardial Infarction (REGENT) Trial. Eur.Heart J. 30, 1313–1321.
Toso, C., Vallee, J.P., Morel, P., Ris, F., Demuylder-Mischler, S., Lepetit-Coiffe, M.,Marangon, N., Saudek, F., James Shapiro, A.M., Bosco, D., Berney, T., 2008. Clinicalmagnetic resonance imaging of pancreatic islet grafts after iron nanoparticlelabeling. Am. J. Transp. 8, 701–706.
Walczak, P., Zhang, J., Gilad, A.A., Kedziorek, D.A., Ruiz-Cabello, J., Young, R.G., Pittenger,M.F., van Zijl, P.C., Huang, J., Bulte, J.W., 2008. Dual-modality monitoring of targetedintraarterial delivery ofmesenchymal stem cells after transient ischemia. Stroke 39,1569–1574.
Yasuhara, T., Matsukawa, N., Hara, K., Maki, M., Ali, M. M., Yu, S., Bae, E., Yu, G., Xu, L.,McGrogan, M., Bankiewicz, K., Case, C., and Borlongan, C. V., in press. Notch-inducedrat and human bone marrow stromal cell grafts reduce ischemic cell loss andameliorate behavioral deficits in chronic stroke animals. Stem Cells Dev. Epubahead of print. doi:10.1089/scd.2009.0011.
Zhu, J., Zhou, L., XingWu, F., 2006. Tracking neural stem cells in patients with braintrauma. N. Engl. J. Med. 355, 2376–2378.
7L.M. Barbosa da Fonseca et al. / Experimental Neurology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Please cite this article as: Barbosa da Fonseca, L.M., et al., Migration and homing of bone-marrow mononuclear cells in chronic ischemicstroke after intra-arterial injection, Exp. Neurol. (2009), doi:10.1016/j.expneurol.2009.10.010
JOURNAL OF THE AMERICAN HEART ASSOCIATION
STROKE/2009/567016 VERSION 1 Mendez-Otero, and Charles André
Regina C Goldenberg, Juliana V Dias, Tais Kasai-Brunswick, Eduardo Wajnberg, Rosália Valéria Battistella, Gabriel de Freitas, Lea MB da Fonseca, Daniel Mercante, Bianca Gutfilen,
subacute ischaemic strokeSafety of autologous bone-marrow mononuclear cell transplantation in patients with
This information is current as of September 28, 2009
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

SAFETY OF AUTOLOGOUS BONE-MARROW MONONUCLEAR CELL TRANSPLANTATION IN PATIENTS WITH SUBACUTE ISCHAEMIC STROKE
Authors: Battistella V1; de Freitas GR1; Barbosa da Fonseca LM2; Mercante D3; Gutfilen B2; Goldenberg RC3,4; Dias VJ3,4; Kasai-Binswick TH3,4; Wajnberg E2; Mendez-Otero R3,4; Andre C1. From the Departments of Neurology1, Radiology2 and Cell Therapy Program3 of the Clementino Fraga Filho University Hospital and Carlos Chagas Filho Biophysic Institute4 of the Rio de Janeiro Federal University. Background: To assess the safety and feasibility of bone-marrow mononuclear cell (BMMC) transplantation in patients with middle cerebral artery (MCA) territory ischaemic stroke within 90 days of stroke onset. Methods: Six male patients (aged 24 to 65 years) received intra-arterial BMMC 60 to 90 days after mild to moderate MCA infarcts (National Institutes of Health Stroke Scale [NIHSS] between 4 and 13) according to a defined protocol (NCT00473057). Iliac-crest bone-marrow aspiration was performed under sedation and local anaesthesia. BMMC were isolated using a Ficoll gradient, and 10% of the cells were separated and labelled with 99mTc and re-injected in the MCA (minimum: 1 x 108 and maximum: 5 x 108 injected cells) after navigation (Seldinger technique). SPECT was done 2 h after the procedure, and whole-body scan and planar images were also taken after 24 h. Electroencephalogram was done within 7 days after transplantation. Patients were evaluated with blood tests, NIHSS, modified Rankin Scale (mRS), and Barthel Index (BI) before treatment, and 1, 3, 7, 30, 60, 90, 120, and 180 days after the infusion. Findings: No patient exhibited any complication or adverse events during the procedure. There was no worsening in NIHSS, mRS, or BI until the end of follow-up. Two patients had generalized seizure after the end of follow-up. Interpretation: In this small pilot study, BMMC intra-arterial injection in patients with ischaemic strokes proved feasible and safe. Phase II studies are required to further evaluate efficacy and safety. INTRODUCTION:
Stroke is the third cause of death in developed countries1 and the leading cause of death in some developing countries2 including Brazil3. Stroke remains a leading cause of disability in the world: at least 30% of stroke survivors make an incomplete recovery, and a further 20% require assistance for activities of daily living4. Although acute-stroke care facilities such as stroke units and the use of thrombolytics may improve prognosis, there are few clinical trials evaluating effective ways to enhance recovery in patients with residual disability5. In recent years, several studies have investigated the potential restorative role of stem cells from different sources in animal models of brain ischaemia6. They showed that stem-cell administration ameliorates the functional loss observed after ischaemia, making stem-cell transplantation an attractive approach to restore brain function after stroke in humans.
Two different Brazilian institutions (phase I clinical trials) evaluated the safety of stem-cell transplantation in the first ten days of ischaemic stroke7,8. Twenty-six patients (the sum of two studies) with middle cerebral artery (MCA) territory infarction received intra-arterial autologous bone-marrow mononuclear cells (BMMC) transplantation. One patient presented neurological deterioration (recurrent embolisation) during arteriography, before the injection of stem cells. Treated patients exhibited uneventful clinical courses, with no new lesions appearing in sequential magnetic resonance imaging (MRI) evaluation, including diffusion-weighted imaging (DWI) and
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

no epileptic activity on frequent electroencephalography studies9. These studies suggest that intra-arterial autologous BMMC transplantation is safe in patients in the first 10 days after ischaemic stroke, and that SPECT imaging with labelled BMMC is a feasible noninvasive method for studying the homing of transplanted cells in vivo.
Transplantation of stem cells after the first few days of ischaemia may present several obstacles. The formation of scar tissue and the restoration of the blood-brain barrier might adversely affect implanted cells. Moreover, there are few reliable animal models of chronic stroke to investigate transplantation several months after the infarction10. Nevertheless, there are some phase I and II clinical studies evaluating stem cell transplantation in patients with chronic stroke, including patients even 10 years after the index event11,12,13,14. However, two of these studies employed cells derived from a human teratocarcinoma11,12 and porcine cells13,which may provoke severe rejection responses. Bang and colleagues examined the safety and efficacy of cultured expanded autologous mesenchymal stem cells administered intravenously 4-5 and 7-9 weeks after symptom onset14. The five patients who received these cells had no adverse effects and presented better outcomes at 3 and 6 months than the control group. In this study the bone marrow cells were cultivated for several weeks before transplantation, which may increase the risk of contamination. In addition, none of these studies evaluated the fate of the transplanted cells in vivo.
The aim of this study was to examine the feasibility and safety of intra-arterial transplantation of autologous BMMC in patients with MCA territory infarction, between 2 and 3 months after the ictus. METHODS: Subjects: This study is an unblinded, uncontrolled Phase I clinical trial. The protocol and the consent form were approved by the Institutional Research Ethics Committee and the National Committee of Ethic and Scientific Research. Written informed consent was obtained from all subjects.
Eighteen to seventy-five year-old individuals were eligible for the study if they had the following characteristics: (1) ischaemic stroke in the MCA territory evidenced by computed tomography (CT) or MRI occurring within 90 days; (2) recanalisation of the involved MCA as assessed by transcranial Doppler (TCD) studies or by magnetic resonance angiography (MRA); and (3) a score between 4 and 17 according to the National Institutes of Health Stroke Scale (NIHSS). We excluded patients who met any of the following criteria: difficulty in obtaining vascular access for percutaneous procedure, ipsilateral carotid stenosis (>50%, by Doppler studies), neurological worsening (>4 points in the NIHSS) before injection due to either edema or intracerebral hemorrhage, thrombophilias or primary haematological diseases, neurodegenerative disorders, previous stroke with modified Rankin Scale > 2, intracardiac thrombus, auto-immune disorders, sepsis (according to the Society of Critical Care Medicine and the American College of Chest Physicians 1992 criteria), history of neoplasia or other comorbidity that could impact a patient's short-term survival, any condition that in the judgment of the investigator would place the patient under undue risk, bone disorders that could increase the risk of the bone-marrow harvesting procedure, liver failure, renal failure (serum creatinine > 2mg/mL), haemodynamic or respiratory instability, lacunar stroke, pregnancy, or previous participation in other clinical trials. Bone-marrow aspiration, cell separation, and cell injection: Cells were obtained by marrow aspiration of the iliac crest (50-80ml) and processed by Ficoll density centrifugation. After washing, counting and viability testing (greater than 98%), cells were resuspended in 10 mL of saline solution with 5% autologous serum. One mL of this solution was labelled with 99 mTc15.
Labelled cells were added back to the total mononuclear cell suspension (final volume 10 mL) and slowly injected into the territory of the MCA, via the femoral artery, after navigation (Seldinger technique). Intravascular infusion of mononuclear cells was performed under local anaesthesia and conscious sedation. A routine coaxial technique with femoral arterial puncture was used. A 6 Fr. Guiding catheter (Envoy-Cordis, Miami, Florida or Guider Soft tip, Boston Scientific, Target Therapeutics, Fremont, California) was positioned at the cervical level with continuous
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

flushing with normal saline. Intravenous heparin was used (bolus of 80 Units/ Kg of body weight) and as needed to maintain the activated clotting time between two and three times baseline values. A large-inner-diameter microcatheter (SL 1018 Boston Scientific, Target Therapeutics, Fremont, California) was navigated to the M1 portion of the MCA and the infusion was performed in about 10 minutes. Neurologic evaluation: All individuals were evaluated at admission, on the day of transplantation, and 1, 3, 7, 30, 60, 90, 120 and 180 days after cell infusion using the NIHSS, the Barthel Index (BI), and the mRS by a single board-certified neurologist (VB). Routine laboratory tests (complete blood count and biochemical examinations: urea, creatinine, and electrolytes) were done at these points. An Electroencephalogram (EEG) was obtained within 7 days after transplantation.
RESULTS:
Baseline characteristics: The clinical and radiologic characteristics and the number of injected cells of the included patients are shown in Table 1. Two patients were taking an oral anticoagulant drug to prevent recurrent strokes, and were switched to low-molecular-weight heparin (enoxaparine 1 mg/Kg b.i.d.) one week before the procedure.
Safety of the procedure: There were no significant adverse effects related to the procedures.
The EEG showed polymorphic slow activity in the ischaemic area, and only one patient exhibited spike-wave activity. Two patients suffered generalized seizures after the end of follow-up, around 200 days after the BMMC infusion; one was successfully treated with phenytoin, the other was treated with a combination of oxcarbazepine and lamotrigine.
Functional Outcome: Only one patient (patient 3) was independent in daily activities at
BMMC infusion day (BI 95 and mRS 1). At the 180-day follow-up evaluation, all patients had improved their scores (Table 1 and Figure 1). NIHSS scores improved (range -1 to -8 points) during follow-up in all patients. No patient scored lower on the BI, mRS, or NIHSS tests.
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

TABLE 1 : Baseline characteristics and follow-up:
Characteristics Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Sex/ Age M / 24 M / 65 M /47 M / 65 M / 57 M / 47 Risk factor PFO Hypertension,
DM, Dislipidaemia
Hypertension AF, DM Hypertension DM, Hypertension
Symptoms Aphasia, Hemiplegia
Dysarthria, Hemiplegia
Aphasia, Hemiparesis
Aphasia, Hemiplegia
Dysarthria, Hemiplegia
Dysarthria, Hemiplegia
Infarct location Left Right Left Left Right Right Stroke Mechanisms
Cardioembolism Athero During aneurism clipping
Cardioembolism Athero Athero
Acute treatment Conservative Conservative Conservative IV Thrombolytics
IV Thrombolytics
IV + IA Thrombolytics + craniectomy
Haemorrhagic transformation
No Yes No Yes No Yes
Infusion day: NIHSS/BI/mRS (days since stroke)
7/ 100/ 2 (67)
9/ 35/ 4 (82)
4/ 95/ 1 (62)
13/ 25/ 5 (72)
9/ 30/ 4 (59)
13/ 10/ 5 (73)
NIHSS/BI/mRS at day 3
6/ 100/ 2 9/ 35/ 4 3/ 95/ 1 12/ 25/ 5 6/ 30/ 4 13/ 10/ 5
NIHSS/BI/mRS at day 7
5/ 100/ 2 8/ 35/ 4 3/ 95/ 1 12/ 25/ 5 5/ 30/ 4 12/ 15/ 5
NIHSS/BI/mRS at day 30
5/ 100/ 1 6/ 50/ 4 3/ 100/ 1 11/ 25/ 4 3/ 50/ 3 12/ 25/ 5
NIHSS/BI/mRS at day 60
4/ 100/ 1 6/ 55/ 4 3/ 100/1 9/ 30/ 4 4/ 90/ 1 12/ 30/ 5
NIHSS/BI/mRS at day 90
4/ 100/ 1 6/ 65/ 3 3/ 100/1 10/ 35/ 4 4/ 90/ 1 12/ 30/ 5
NIHSS/BI/mRS at day 120
4/ 100/ 1 6/ 75/ 3 3/ 100/1 10/ 35/ 4 1/ 100/ 0 11/ 50/ 3
NIHSS/BI/mRS at day 180
4/ 100/ 1 6/ 80/ 3 3/ 100/1 10/ 35/ 4 1/ 100/ 0 11/ 50/ 3
No. of injected cells
5 x 108 1.25 x 108 3.9 x 108 4 x 108 3.2 x 108 1 x 108
PFO: Patent Foramen Ovale DM: Diabetes mellitus AF: Atrial fibrillation NIHSS: National Institutes of Health Stroke Scale Cardioemb: cardioembolism Athero: atherosclerotic mRS: modified Rankin Scale BI: Barthel Index IV: intra-venous, IA: intra-arterial
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

DISCUSSION: In the present series, BMMC transplantation proved to be safe and feasible in 6 patients with
ischaemic stroke in the MCA territory within 90 days after onset. There were no complications or unexpected outcomes related to the procedure. All the patients improved their scores (NIHSS, BI, and mRS) at the end of follow-up (Table 1 and Figure 1). Two patients suffered seizures about 200 days after the cell infusion These patients are under extended follow-up.
Stem-cell-based therapies may represent new and important strategies for the treatment of stroke. In animal models of ischaemia, stem cells from different sources have been used with promising results, and different mechanisms of action have been suggested to explain these functional benefits16-18. For example, the introduction of neural stem cells/ neural progenitors into areas of cell loss may result in repair and restoration of circuitry19. Alternatively, when bone-marrow-derived stem cells (mesenchymal or mononuclear cells) are employed, the functional benefits observed are probably due to the release of cytokines and/or trophic factors which may have an immunomodulatory effect and/or contribute to a reduction in apoptosis in the penumbra area in earlier periods after ischaemia20. In addition, it has been suggested that cell-based therapies amplify endogenous processes of brain repair and plasticity, including neurogenesis, angiogenesis, and synaptogenesis, which could explain the benefits observed in experimental models of stroke, even when cells are administered at later times21-23.
Up to now, only a few clinical studies involving cellular therapies in patients with acute and chronic stroke have been published6,11,12 ; only two of these studies involved therapy with autologous bone-marrow-derived stem cells7,14. In one, Bang and cols. investigated intravenous infusion of autologous mesenchymal bone-marrow cells, expanded in vitro, in patients with acute cerebral infarcts14. The procedure was safe and feasible; the group receiving mesenchymal cells (n=5) had their BI increased after the MSC infusion on 3 and 6 months after the onset of symptoms. However, the changes in NIHSS and mRS were not statistically significant. Another point of discussion is cell preparation: although feasible, it is potentially dangerous and is also expensive. Another study carried out during the acute phase of stroke (3-10 days post-ictus) evaluated the safety of intra-arterial bone-marrow mononuclear cell transplantation in patients with MCA territory infarcts in two different Brazilian institutions. In one of them, six patients were enrolled and received approximately 30 x 106 cells into the territory of the middle cerebral artery, via the femoral artery, after navigation (Seldinger technique). Preliminary reports showed that the procedure is safe and feasible7,8. With respect to chronic stroke, Savitz and cols studied neurotransplantation of fetal porcine cells in patients who had suffered a stroke 3 months to 10 years prior to study. The patients underwent CT-guided stereotactic implantation of fetal cells pretreated with an antibody to prevent rejection. The study was terminated by the Food and Drug Administration (FDA) because of adverse events (cortical-vein occlusion secondary to the surgery in one patient, and seizures in two patients)13. Kondziolka and cols carried out a phase II randomized trial that included patients for whom the mean time after onset of stroke was 3.5 years. They received stereotactic implants of human cultured neuronal cells, derived from a human embryonic carcinoma cell line. The study was negative for the primary outcome measure, although a measurable improvement, without statistical significance, was noted in some patients. One patient developed a single seizure 1 day after surgery, while another developed a subdural haematoma that required drainage 1 month after surgery12. The results of these two studies suggest that intracranial transplantation does carry risk.
Some issues need to be addressed. Although the transplantation seems to be safe and feasible, many questions remain unanswered, including the origin and dose of stem cells, administration route, timing of the infusion (acute x sub-acute x chronic stage of stroke), the territory of stroke (cortical x subcortical territories, anterior x posterior circulation), and the mechanisms of action of bone-marrow-derived stem cells in the setting of stroke. In our study, the rationale for selecting the cell dose was based on the results of the safety studies described above7,8 and the reason for selecting non-acute patients was based the on results from experimental models of cell therapy in stroke24, although the two issues are interconnected. A therapeutic window should be determined as a function of therapeutic dose, and the repeated-dose regimen could optimize
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

recovery benefit25. It is not clear whether late seizures in two patients were caused by some late reaction of the
mononuclear cells injected, by misdirection of regenerating nerve fibres (aberrant reinervation) or by the anatomic substrate of the ischaemic tissue itself. Although several risk factors for early or late seizures have been identified, there is no clear predictor of post-stroke epilepsy26. Approximately 5-10 percent of acute ischaemic-stroke patients have early seizures, which typically occur within 24 hours27. Late seizures, usually occurring at least 2 weeks after the stroke28,29 occur in 3% to 67%, varying considerably among series27,30. The potential impact of seizure on stroke mortality and neurologic outcome is a matter of concern that may influence the treatment decision after a first seizure. However, this issue remains a matter of debate, with limited data regarding the specific impact of late and recurrent seizures on functional recovery26. Since our sample is very small, we cannot rule out that the 33% incidence (2 out of 6) of seizures is explained by chance.
In conclusion, transplantation of BMMC is feasible and seems to be safe in patients with subacute ischemic stroke. Further randomized clinical trials are necessary to establish the efficacy and long term safety of this procedure.
Conflict of interest:
The authors have no conflicts of interest regarding this work.
Acknowledgments:
This study was supported by a grant from the Ministry of Health and Ministry of Science and Technology of Brazil to Rosalia Mendez-Otero (grant number 552201/2005-7). References:
1. Murray CJL, Lopez AD. Mortality by cause for eight regions of the world. Global burden of disease study. Lancet. 1997;349:1269-1276.
2. Wu Z, Yao C, Zhao D, et al. Sino-MONICA project. A collaborative study on trends and determinants in cardiovascular diseases in China. Part I: morbidity and mortality monitoring. Circulation 2001;103:462-468.
3. André C, Curioni CC, da Cunha CB. Progressive decline in stroke mortality in Brazil from 1980 to 1982, 1990 to 1992 and 2000 to 20002. Stroke 2006;37:2784-2789.
4. Bonita R, Solomon N, Broad JB. Prevalence of stroke and stroke-related disability. Estimates from the Auckland stroke studies. Stroke 1997;29:866-867.
5. Cramer SC. Repairing the human brain after stroke: I. Mechanisms of spontaneous recovery. Ann Neurol 2008;63:272-287.
6. Mendez-Otero R, de Freitas GR, André C. Potential roles of bone marrow stem cells in stroke therapy. Regen Med 2007;2(4):417-423.
7. Mendonça ML, de Freitas GR, Silva SA, et al. Safety of intra-arterial autologous bone marrow mononuclear cell transplantation for acute ischemic stroke. Arq Bras Cardiol 2006;86(1):52-55.
8. de Freitas GR, Mendonça MFL, Bezerra DC, et al. Safety and feasibility of intra-arterial autologous bone marrow mononuclear cell transplantation in acute ischemic stroke. Proceedings of the 58th Annual meeting of the American academy of neurology. San Diego, CA, USA, April 1-8, 2006.
9. Correa PL, Mesquita CT, Felix RM, et al. Assesment of intra-arterial injected autologous bone marrow mononuclear cell distribution by radioactive labeling in acute ischemic stroke. Clin Nucl Med 2007;32:839-841.
10. Savitz SI, Rosenbaum DM, Dinsmore JH, et al. Cell transplantation for stroke. Ann Neurol 2002;52:266-275.
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

11. Kondziolka D, Wechsler L, Goldstein S, et al. Transplantation of cultured human neuronal cells for patients with stroke. Neurology 2000;55:565-569.
12. Kondziolka D, Steiberg GK, Wechsler L, et al. Neurotransplantation for patients with subcortical motor stroke: a phase 2 randomized trial. J Neurosurg 2005;103:38-45.
13. Savitz SI, Dinsmore J, Wu J, et al. Neurotransplantation of fetal porcine cells in patients with basal ganglia infarcts : a preliminary safety and feasibility study. Cerebrovasc Dis 2005;20:101-107.
14. Bang OY; Lee JS; Lee PH, et al. Autologous mesenchymal stem cell transplantation in stroke patients. Ann Neurol 2005;57:874-882.
15. Barbosa da Fonseca LM; Battistella V; Freitas GR, et al. Early tissue distribution of bone-marrow mononuclear cells after intra-arterial delivery in a patient with chronic stroke. Circulation 2009;120:539-541.
16. Li Y; Chopp M; Chen J, et al. Intrastriatal transplantation of bone marrow nonhematopoietic cells improves functional recovery after stroke in adult mice. J Cereb Blood Flow Metab 2000;20:1311-1319.
17. Borlongan CV, Hadman M, Sanberg CD, et al. Central nervous system entry of peripherally injected umbilical cord blood cells is not required for neuroprotection in stroke. Stroke 2004;35:2385-2389.
18. Shyu WC, Lin SZ, Yang HI, et al. Functional recovery of stroke rats induced by granulocyte colony-stimulating factor-stimulated stem cells. Circulation 2004;110:1847-1854.
19. Englund U, Björklund A, Wictorin K, et al. Grafted neural stem cells develop into functional pyramidal neurons and integrate into host cortical circuitry. Proc Natl Acad Sci USA 2002;99:17089-17094.
20. Giraldi-Guimarães A, Rezende-Lima M, Bruno FP, et al. Treatment with bone marrow mononuclear cells induces functional recovery and decreases neurodegeneration after sensorimotor cortical ischemia in rats. Brain Res 2009;108-120.
21. Savitz SI, Dinsmore J, Wechsler L, et al. Cell therapy for stroke. NeuroRx 2004;1:406-414. 22. Caplan AI. Adult mesenchymal stem cells for tissue engineering versus regenerative
medicine. J Cell Physiol 2007;213:341-347. 23. Vendrame M, Gemma C, de Mesquita D, et al. Anti-inflammatory effects of human cord
blood cells in a rat model of stroke. Stem Cells Dev 2005;14:595-604. 24. Shen LH, Li Y, Chen J, et al. Therapeutic benefit of bone marrow stromal cells administered
1 month after stroke. J Cereb Blood Flow Metab 2007;27:6-13. 25. Stem Cell Therapies as an Emerging Paradigm in Stroke Participants. Stem Cell Therapies
as an Emerging Paradigm in Stroke Participants (STEPS): bridging basic and clinical science for cellular and neurogenic factor therapy in treating stroke. Stroke 2009;40:510-515.
26. Ryvlin P, Montavont A, Nighoghossian N. Optimizing therapy of seizures in stroke patients. Neurology 2006;67(Suppl 4):S3-S9.
27. Camilo O; Goldstein LB. Seizures and epilepsy after ischemic stroke. Stroke 2004;35:1769-1775.
28. Bladin CF, Alexandrov AV. Seizures after stroke: a prospective multicenter study. Arch Neurol 2000;57:1617-1622.
29. Gupta SR, Rubino FA. Postinfarction seizures. A clinical study. Stroke 1988;19:1477-1481. 30. Lossius MI, Ronning OM, Slapo GD, et al. Post-stroke epilepsy: occurrence and predictors
– a long-term prospective controlled study (Akershus Stroke Study). Epilepsia 2005;46:1246-1251.
on September 28, 2009 http://submit-stroke.ahajournals.orgDownloaded from

0
2
4
6
8
10
12
14
D1 D3 D7 D30 D60 D90 D120 D180
123456
NIHSS
on Septem
ber 28, 2009 http://subm
it-stroke.ahajournals.orgD
ownloaded from

Livros Grátis( http://www.livrosgratis.com.br )
Milhares de Livros para Download: Baixar livros de AdministraçãoBaixar livros de AgronomiaBaixar livros de ArquiteturaBaixar livros de ArtesBaixar livros de AstronomiaBaixar livros de Biologia GeralBaixar livros de Ciência da ComputaçãoBaixar livros de Ciência da InformaçãoBaixar livros de Ciência PolíticaBaixar livros de Ciências da SaúdeBaixar livros de ComunicaçãoBaixar livros do Conselho Nacional de Educação - CNEBaixar livros de Defesa civilBaixar livros de DireitoBaixar livros de Direitos humanosBaixar livros de EconomiaBaixar livros de Economia DomésticaBaixar livros de EducaçãoBaixar livros de Educação - TrânsitoBaixar livros de Educação FísicaBaixar livros de Engenharia AeroespacialBaixar livros de FarmáciaBaixar livros de FilosofiaBaixar livros de FísicaBaixar livros de GeociênciasBaixar livros de GeografiaBaixar livros de HistóriaBaixar livros de Línguas

Baixar livros de LiteraturaBaixar livros de Literatura de CordelBaixar livros de Literatura InfantilBaixar livros de MatemáticaBaixar livros de MedicinaBaixar livros de Medicina VeterináriaBaixar livros de Meio AmbienteBaixar livros de MeteorologiaBaixar Monografias e TCCBaixar livros MultidisciplinarBaixar livros de MúsicaBaixar livros de PsicologiaBaixar livros de QuímicaBaixar livros de Saúde ColetivaBaixar livros de Serviço SocialBaixar livros de SociologiaBaixar livros de TeologiaBaixar livros de TrabalhoBaixar livros de Turismo