who obstetric emergencies
DESCRIPTION
emergency during laborTRANSCRIPT
Clinical Practice Guidelines – Obstetrics
Obstetrics• Breechdelivery
• Cordprolapse
• Ectopicpregnancy
• Miscarriage
• Normalcephalicdelivery
• Placentalabruption
• Placentapraevia
• Pre-eclampsia
• Primarypostpartumhaemorrhage
• Secondarypostpartumhaemorrhage
• Shoulderdystocia
• Uterineinversion
• Uterinerupture

Version 1.0 – September 2011
Clinical practice guidelines Breech delivery
Clinical features
Signs of imminent delivery• increasingfrequencyandseverityofcontractionswithanurgetopush
• bloodstainedshow–althoughtthismaynotbeanimminentsign
• membranerupture
• bulgingperineum
• appearanceofthepresentingpart
Abreechbirthoccurswhenthefetusentersthebirthcanalwiththebuttocksorfeetfirst,withcommonvariationsbeingcomplete,frank,footingandknee(seeBreechbirthCPP).[1]
Theincidenceofbreechpresentationisaround3–4%withthemajorriskfactorsbeingmultiplepregnancyandpretermlabour.[2]
Breechdeliveryhasanassociatedhighriskofmaternalandfetalmorbidityandmortality.
Theprimaryfocusofpre-hospitalmanagementisrapidrecognitionofabreechbirthandlimitingmanipulationofthebabyuntilrequired,beinggentlebuttimelywiththenecessarytechniques.[2]
Page1of4
Complete breech
Footling breech Kneeling breech
Frank breech
Risk assessment
• Complicationsofbreechdeliveryinclude:[3]
- fetalhypoxia
- prolapsedcord
- headentrapment
- meconiumaspiration
- postpartumhaemorrhage
- inversionoftheuterus.
• Incorrectmanoeuvresorroughhandlingcaninjuretheinfant:
- spleenorliverdamage
- spinaldamageorfractures
- fracturedbonesordislocations
- softtissueinjuries
- cerebralhaemorrhage,ifthedeliveryistoorapid.
Additional information
• Preparationforneonateresuscitationshouldbemadeattheearliestsignofbreechpresentation.[4]
• ConsiderationshouldbesoughttoearlyICPorobstetricretrievalteambackup.
• Ensureanaseptictechniquewithappropriateinfectioncontrolmeasurestobetakenatalltimes.
• BeforeperformingtheLovesetsmanoeuvre,ensurethatadrycloth/padiswrappedaroundthepelvisofthebaby.Thiswillpreventtheparamedic’shandsfromslippingduringtheprocedureandprovidesomeprotectionforthebaby.
Breechdelivery–Page2of4
Version 1.0 – September 2011
Clinical practice guidelines Breech delivery
Standard Cares
Cordcompressedagainstpubicarch?
Gentlypulldownloopofcord.
Allowneonatetodescendfreely.
Gentlypullcordaroundtoperineum
Positionmothersoneonatecanhangfreely
Page3of4
Armsextended?
Observedescentuntilocciputvisible
Mauriceau-Smellie-Viet(MSVmanoeuvre)
Lovesetsmanoeuvre
Meconium/amnioticfluidpresentinmouth?
ManageasperCPG:
• Resuscitation–newborn
Clearairway
Isneonatebreathingorcryingwith
goodmuscletone? • Drybaby• Maintainwarmth• Provideskintoskincontact• Clampandcutthecord• Apgarscoreat1&5min• Conductpostnatalcares
TransporttohospitalPre-notifyasappropriate
Breechdelivery–Page4of4
Version 1.0 – September 2011
Clinical practice guidelines Cord prolapse
Clinical features
• Umbilicalcordvisibleat,orexternalto,thevaginalopening
• Evidenceofmembraneshavingruptured
• Anonreassuringfetalstatus:[4]
- changeinfetalmovementpattern
- meconiumintheamnioticfluid(vaginaldischargemaybestainedgreen)
- fetaltachycardia>160bpm- fetalbradycardia<110bpm(morecommon).
Risk assessment
• Cautionisrequiredifmanoeuvringtheumbilicalcordaspinchingwillcancausevasospasm.[5]
• Anon-labouringpatienthasadecreasedriskofcordprolapse,butanypresentationcancompressthecord.
Cordprolapseisarareobstetricemergencythatisassociatedwithahighperinatalmortalityrate.[1]Itoccursafterthemembraneshaveruptured,whentheumbilicalcordslipsdowninfrontofthepresentingpartofthefetusandprotrudesintothevagina.Diagnosisismadebyvisualisingthecordatthevaginalopening,whichwillappearasabluishwhite,shiny,pulsatingstructure.
Thisconditionbecomesanissueaslabourprogressesandthepresentingpartdescends,compressingthecordandcuttingoffthefetalbloodsupply,leadingtohypoxiaandeventualfetaldemise.[2]
Theprincipleofpre-hospitalmanagementistomonitorthecordforpulsationsandusematernalpositioningtopreventcompression.Ifthecordstopspulsating,thepressurefromthepresentingpartwillneedtobealleviated,eitherindirectlyusinggravity(maternalknee-chestposition)ordirectly,bygentlypushingthefetusoffthecord.[2]
Riskfactorsforcordprolapseinclude:[3]
• Abnormalfetalpresentation
• Multiparity
• Lowbirthweight
• Prematurity
• Polyhydramnios
• Spontaneousruptureofmembranes.
Page1of2
Standard Cares
Pulsatilecordevident?
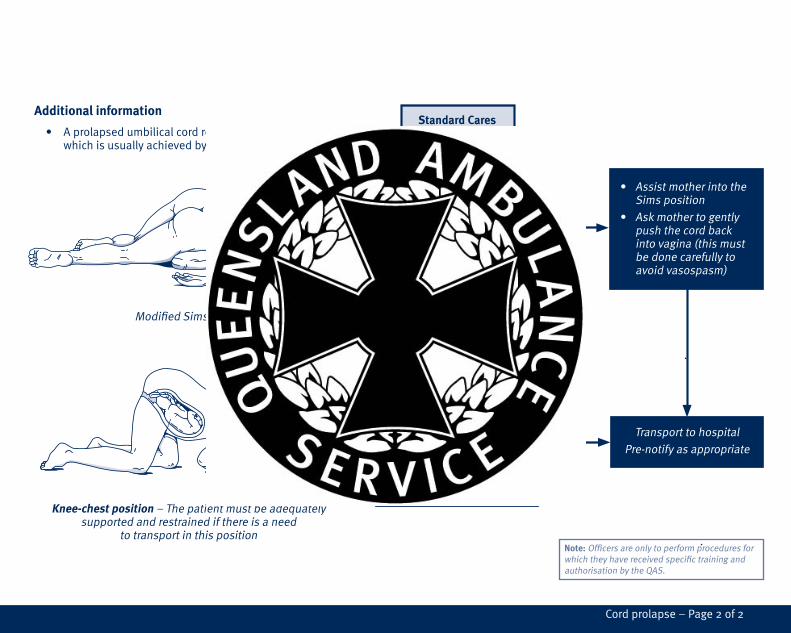
• AssistmotherintotheSimsposition
• Askmothertogentlypushthecordbackintovagina(thismustbedonecarefullytoavoidvasospasm)
TransporttohospitalPre-notifyasappropriate
• Assistmothertoassumetheknee-chestposition
• Carefullyattempttopushthepresentingpartoffthecord
• Useamoistdressingtomaintaincordtemperatureandavoiddrying
ModifiedSimsposition
Knee-chest position–Thepatientmustbeadequatelysupportedandrestrainedifthereisaneed
totransportinthisposition
Additional information
• Aprolapsedumbilicalcordrequiresanimmediatedelivery,whichisusuallyachievedbyCaesareansection.[3]
Note:OfficersareonlytoperformproceduresforwhichtheyhavereceivedspecifictrainingandauthorisationbytheQAS.
Cordprolapse–Page2of2
Version 1.0 – September 2011
Clinical practice guidelines Ectopic pregnancy
Clinical features
Unruptured ectopic pregnancy• Historyofamenorrhea(usuallyonlyonemissedperiod)
• Abnormalvaginalbleeding
• Pelvicand/orabdominalpain
• Nausea
• Presyncopalsymptoms
Ruptured ectopic pregnancy• Collapse
• Shock
• Acuteseverepelvicand/orabdominalpain
• Shouldertippain(Kehr’ssign),fromfreebloodirritatingthediaphragmwhensupine
• Abdominaldistention
• Reboundtenderness
Ectopicpregnanciesoccurwhenthedevelopingembryoimplantsoutsidetheuterinecavity,withover98%occurringintheFallopiantubes.[1]Althoughthisconditioncanbelife-threatening,inthelastdecadedeathsinAustraliahavebeenextremelyrare.[2]Thiscanbeattributedtoimprovedearlydiagnosisandtreatment,despiteaworldwideincreaseofcasesfrommoreprevalentriskfactors,[1][3]suchas:
• Invitrofertilizationandfertilitytreatments
• Sexuallytransmittedinfections(e.g.chlamydia)
• Useofintrauterinedevices
• Advancedmaternalage
• Smoking
• Previoushistoryofectopicpregnancy
• Tubaldamageasaresultofsurgery
Themostsignificantcomplicationofectopicpregnancyistubalrupture,whichusuallyoccursbetween6–10weeksofgestationandcanresultinsignificanthaemorrhageandshock.[4]
Risk assessment
Ahighindexofsuspicionforectopicpregnancyshouldbemaintainedwithanyfemalepatientofchild-bearingageexhibitinganyoftheassociatedclinicalfeatures.
Page1of2

Standard Cares
Suspectedrupture? Patientshocked?
Consider:• Analgesia• Antiemetic• IVfluid
Transporttohospital
Pre-notifyasappropriate
ManageasperCPG:• Shock
Ectopicpregnancy–Page2of2
Version 1.0 – September 2011
Clinical practice guidelines Miscarriage
Risk assessment
Pre-hospitaldiagnosisofmiscarriagecanbedifficulttodetermine,particularlywherethePOCarenotobvious.
DefinitivediagnosisofmiscarriageisbasedonconfirmedpassageofPOCorultrasoundfindingsconsistentwithASUMcriteriaformiscarriagediagnosisatthereceivingfacility.[5]
Thereforedifferentialdiagnosisofantepartum/PVhaemorrhagemustinclude:
• Normalearlypregnancybleeding.
• Ectopicpregnancy.
• Sexualassault/nonaccidental-injury.
Ifpossible,alltissueandlargeclotsshouldberetainedandtransportedtothereceivingfacility.Ifterminationoccursintothefirsttrimesterorlatergestation,afetusmaybepassedoutofthevagina.Oftentheplacentawillnotseparate.Ifthisoccurs:
• Cutandclampthecord
• Wrapthefetus(Themothermayormaynotwishtoholdthefetus.)
Somefetuses<20weekswillshowsignsoflife(movement/gasp).Ifthefoetusislessthan20weeks,thenresuscitationisfutile.[6]
Europeanresuscitationguidelinesstatethatitispossibletoidentifyconditionsassociatedwithhighmortalitywherewithholdingrescusitationmaybeconsideredreasonable.Theseincludegestationalage<23weeksand/orbirthweight<400g.[7]
Miscarriageisdefinedasthespontaneouslossofpregnancybefore24weeksofgestation,withtheaetiologyforthemajorityofcasesbeingunknown.[1]Thereareseveraldifferentcategoriesofmiscarriage,someofwhicharemoresusceptibletointrauterineinfectionduetoretainedproductsofconception(POC),whichmayleadtosepticshock.[2]
Althoughvaginalbleedingandabdominalpainarecharacteristicsofamiscarriage,about25%ofpregnanciesareassociatedwithbleedinginthefirst12weeks.[3]Withthisinmind,itisimportantnottomakecommentsthatcouldbeinterpretedasadiagnosis.
Miscarriagehasbeenassociatedwithsignificantpsychologicalconsequencesandpatientshavebeenshowntobenefitfromappropriatecounsellingandsupport,whichshouldbeinitiatedinthepre-hospitalsetting.[4]
Miscarriageistheleadingcauseofante-partumhaemorrhage.Themostsignificantcomplicationsinclude:
• Haemorrhagicshock
• Uterinesepsis.
Clinical features
Clinical presentation includes:• Generalisedweakness
• Lowerabdominaldiscomfort
• Vaginalbleeding
• Hypotension
• Tachycardia.
Signs suggestive of intrauterine infection include:• Severeuterinepain/rigidity/guarding
• Purulentdischarge
• Fever.
Page1of2
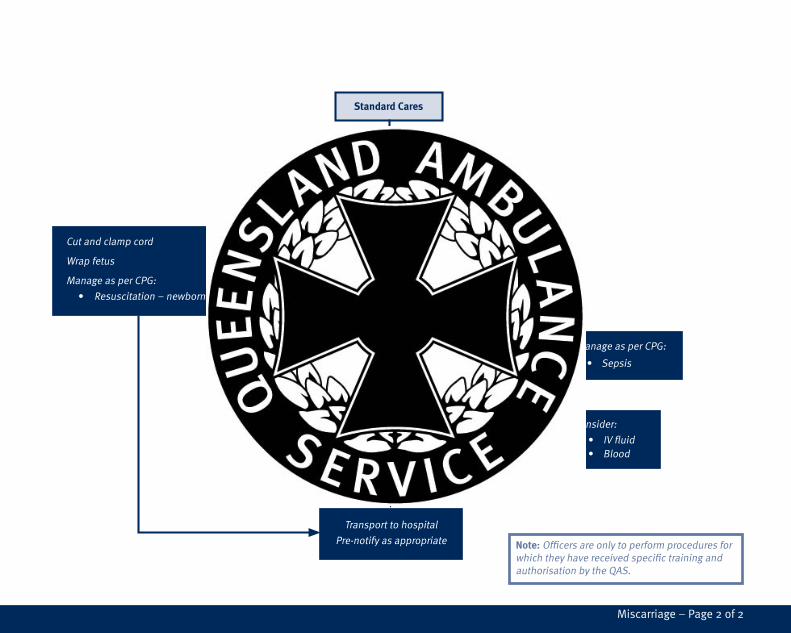
Standard Cares
Consider:
• Analgesia
Evidenceoffetus?
Cutandclampcord
Wrapfetus
ManageasperCPG:
• Resuscitation–newborn
Suspectedsepsis?ManageasperCPG:
• Sepsis
Significanthaemorrhage?Consider:
• IVfluid• Blood
Transporttohospital
Pre-notifyasappropriate
Miscarriage–Page2of2
Version 1.0 – September 2011
Clinical practice guidelines Normal cephalic delivery
Risk assessment
Gainingadequateprenatalhistorymaypre-emptcomplicationsassociatedwithdeliveryandinclude:
• Mal-presentation
• Multiplepregnancy
• Pre-eclampsia
• Placentaprevia
• Substanceabusedisorders
• Historyofobstetricorgynaecologicaldisorderoremergency.
Ensureanaseptictechniqueandalwaysuseappropriateinfectioncontrolmeasures.
Definitive care
Note –RefertoCPPfornormalcephalicdeliveryprocedures.
Normalcephalicdeliveryisdefinedasthemeansbywhichthenewborn,placentaandmembranesaredeliveredviathebirthcanalinwhich:
• Asinglenewbornpresentsviathevertex
• Thenewbornisbornbyvaginaldeliveryattermbetween37–42weeksgestation
• Thebirthiscompletedspontaneouslywithin18hours
• Nocomplicationsoccur.
Clinical features
Signs of imminent delivery• Increasingfrequencyandseverityofcontractionswithanurgetopush
• Showofoperculumplug–Whenthecervixdilates,theoperculumplugdislodgesfromthecervicalcanal
• Membranerupture(Thismaynotoccurandactivemembranerupturewillberequirediftheheadhasbeendeliveredwithoutmembranerupture)
• Bulgingperineum
• Appearanceofthepresentingpartatthevulva
Note –IfimminentdeliveryisinitiatedduetotraumarefertoTraumainpregnancyCPG.
Page1of4
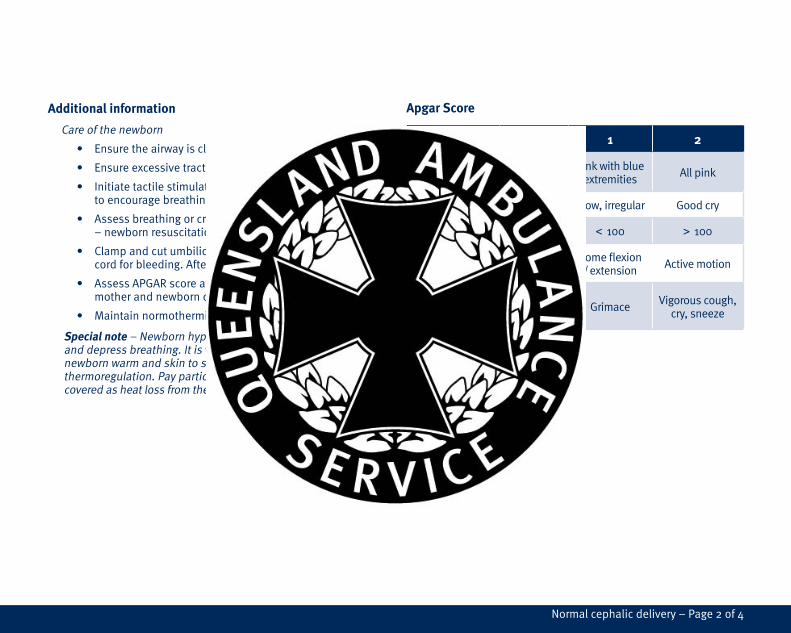
Additional information
Careofthenewborn
• Ensuretheairwayisclearofamnioticfluid/meconium.
• Ensureexcessivetractionisnotplacedonthecord.
• Initiatetactilestimulationanddryingofthenewborntoencouragebreathing.
• Assessbreathingorcrying,muscletone,heartrate–newbornresuscitationCPG.
• Clampandcutumbilicalcordasrequired.Reassesscordforbleeding.After15minutesreclampifrequired.
• AssessAPGARscoreat1and5minutes,thenassessmotherandnewborncontinuallyeveryfiveminutes.
• Maintainnormothermiaandwarmenvironment.
Special note–Newbornhypothermiacanoccurquicklyanddepressbreathing.Itisveryimportanttokeepthenewbornwarmandskintoskincontactwillgreatlyassistthermoregulation.Payparticularattentiontokeepingtheheadcoveredasheatlossfromthenewbornheadcanbesubstantial.[1]
Apgar Score
0 1 2
Colour Blue/pale Pinkwithblueextremities Allpink
Respirations Absent Slow,irregular Goodcry
Heart Rate Absent < 100 > 100
Muscle Tone Limp Someflexion/extension Activemotion
Reflex / irritability
Noresponse Grimace Vigorouscough,
cry,sneeze
Normalcephalicdelivery–Page2of4
Version 1.0 – September 2011
Clinical practice guidelines Normal cephalic delivery
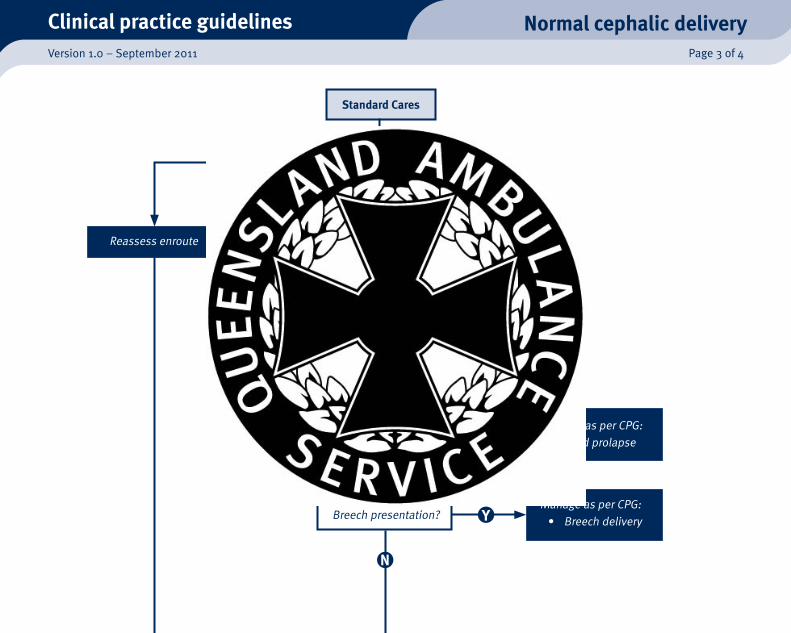
Standard Cares
Patientinlabour?
Signsofimminentdelivery?Reassessenroute
Positionmother
Prepareequipment
Consideranalgesia
Cordprolapsed?ManageasperCPG:• Cordprolapse
Breechpresentation?ManageasperCPG:• Breechdelivery
Page3of4
TransporttohospitalPre-notifyasappropriate
Ensurecontrolleddeliveryofhead
Cordlooparoundneck?Unloopcordoverhead,oriftootightclampandcutcord
Shouldersobstructed?
Controlrateofdelivery
Isamnioticfluidclear?• Goodbreathing/crying• Goodmuscletone
ManageasperCPG:
• Resuscitation–newborn
Postdeliverycares
ManageasperCPP:
• Shoulderdystocia
Normalcephalicdelivery–Page4of4

Version 1.0 – September 2011
Clinical practice guidelines Placental abruption
Clinical features [1]
• Vaginalbleedingmaybeprofuseandoccurastheuteruscontracts.
• Constantpainintheabdomino-pelvicregion
• Bleedingmayrangefromabsenttoprofuse,occurringinwavesastheuteruscontracts.
• Tetanicuterinecontractions
• Uterinehypertonicity–feelsrigidonpalpation
• Fundalheightmayincreaseduetoexpandingintrauterinehaemorrhage.
• Signsofmaternalshock
• Nonreassuringfetalheartratepatterns
Risk assessment
• Diagnosisofplacentalabruptionshouldbeconsideredinanypregnantwomanwithabdominalpain,evenwithoutevidenceofhaemorrhageduetothepossibilityofanoccultbleed.
• Mildcasesmaynotbeclinicallyobvious.
Placentalabruptionoccurswhenanormallysituatedplacentaseparateseitherpartiallyorcompletelyfromtheuterinewall,resultinginhaemorrhagepriortothedeliveryofthefetus.ItisanobstetricemergencythatisassociatedwithseriousmaternalcomplicationssuchasDIC,shock,uterinerupture,oracuterenalfailure,andalsocontributestohighratesoffetalperinatalmortality.[1]
Theincidenceofplacentalabruptionisapproximatelyonein100–200pregnancies;howeverthefrequencyisincreasing,possiblyduetoatrendtowardslatermotherhood,orahigherincidenceofCaesareansections.[1]
Althoughblunttraumacanbeafactor,themajorityofcasesareidiopathic,howevernumerousriskfactorshavebeenidentified,[2]suchas:
• Gestationalhypertensionandpre-eclampsia
• PrevioushistoryofabruptionorCaesareansection
• Multiparityandadvancedmaternalage
• Intrauterineinfection
• Rupturedmembranesinthepresenceofpolyhydramnios
• Tobaccoorcocaineuse.
Managementisbaseduponearlyrecognition,especiallyinoccultbleeds,andpreventingmaternalhypotensioninordertoavoidfetalhypoxia.
Page1of2
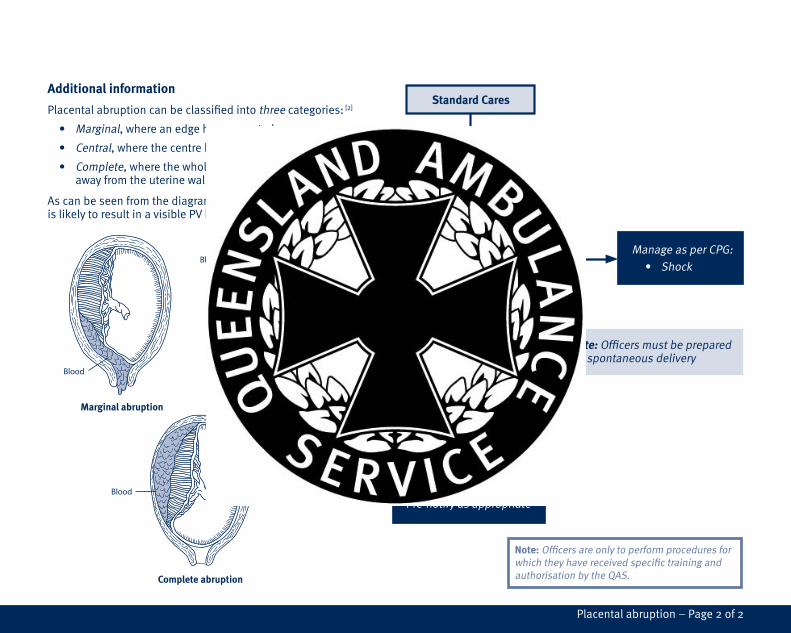
Additional information Placentalabruptioncanbeclassifiedintothreecategories:[2]
• Marginal,whereanedgehasseparatedaway
• Central,wherethecentrehasdetached
• Complete,wherethewholeplacentahascomeawayfromtheuterinewall.
Ascanbeseenfromthediagrams,onlyamarginalabruptionislikelytoresultinavisiblePVhaemorrhage.
Standard Cares
Evidenceofshock?
Avoidaortocavalcompression
ManageasperCPG:• Shock
Consider:•IVaccess•IVfluid•Analgesia•Antiemetics
Transporttohospital
Pre-notifyasappropriate
Note:Officersmustbepreparedforspontaneousdelivery
Blood
Complete abruption
Central abruptionMarginal abruption
Blood
Blood
Placentalabruption–Page2of2

Version 1.0 – September 2011
Clinical practice guidelines Placenta praevia
Risk assessment
Note:Undernocircumstancesperformadigitalinternalexaminationorallowanythingtobeplacedintothevaginatocontrolbloodlossasthiscanresultincatastrophichaemorrhage.[5]
Placentapraeviaoccurswhentheplacentaissituatedeitherpartiallyorwhollyintheloweruterinesegment.Thisbecomesrelevantduringthethirdtrimester(28–40weeks)whenthedownwardandoutwardthrustofthedevelopingfetusisaccommodatedbythethinningandstretchingoftheloweruterinewall.Thisexpansioncausessomedegreeofplacentalseparationandsubsequentbleeding.Thiscanworsenduringeffacementofthecervix,iftheplacentaisnearoroverthecervicalos.[1]
Furthermore,thepositionoftheplacentamayphysicallypreventnormalvaginaldelivery(seeadditionalnotes)andtherefore,appropriatemanagementreliesuponsuitableantenatalassessmentsandmonitoring.[2]
Theconditionbecomesanobstetricemergencyinthepresenceofantepartumhaemorrhage,asinitialsmallbleedshavethepotentialtodevelopintoprofusebloodlossthatcanthreatenboththemotherandthefetus.[3]
Pre-hospitalmanagementisfocusedonpreventingmaternalhypotension,asthiswillresultinbloodbeingshuntedawayfromthefetustomaintainmaternalbloodpressure,whichcancausefetalhypoxia.[4]
Clinical features
Clinical presentation can include:
• Severalsmallwarningbleeds
• Brightredblood
• Nopain,otherthanthatassociatedwithcontractions
• Asoft,non-tenderuterus
• Significantbloodloss,whichmayleadtohypovolaemicshock.
Additional information
Grade 1–Thereisonlyasmallamountofplacentaencroachingonthelowersegmentwhichisclearofthecervicalos.Vaginalbirthispossible.
Grade 2–Theplacentaextendstothemarginoftheosbutdoesnotcoverit.Vaginalbirthmaybepossible.
Page1of2

Grade 3–Theplacentacompletelycoverstheinternalos,butisnotcentrallyoverit.Vaginalbirthisnotpossibleasthefetalpassagewillcausetheplacentatoseparateprematurely,causingcatastrophichaemorrhage.
Grade 4–Theplacentacompletelycoverstheinternalosandiscentrallyoverit.Vaginalbirthisnotpossiblebecausethefetalpassageisprevented.
Standard Cares
Signsofshock?
Avoidaortocavalcompression
ManageasperCPG:• Shock
Consider:•IVaccess•IVfluid•Analgesia•Antiemetic
Transporttohospital
Pre-notifyasappropriate
Note:Officersmustbepreparedforspontaneousdelivery
Placentapraevia–Page2of2
Version 1.0 – September 2011
Clinical practice guidelines Pre-eclampsia
Theprinciplepre-hospitalmanagementofthisconditionissupportivecareandthepreventionofeclampsia,withthelatterdefinedastheoccurrenceofoneormoreseizuressuperimposedonahistoryofpre-eclampsia.[1]
Ifeclampsiadevelops,thefocusofmanagementistoterminateanyseizuresinordertopreventmaternalandanysubsequentfetalhypoxia.
Clinical features
Clinical features can include:
• Neurological
- headache
- visualdisturbance
- seizure
- hyperreflexia
- clonus
• Respiratory
- acutepulmonaryoedema
• Cardiovascular
- hypertension
- generalisedoedema
• Gastrointestinal
- epigastricpain
- nauseaandvomiting.
Pre-eclampsiaisdefined[1]asamultisystemdisorderthatonlyoccursduringpregnancyafter20weeksgestation,andisdiagnosedbyeithera:
• Systolicbloodpressure(SBP)≥140mmHgand/or• Diastolicbloodpressure(DBP)≥90mmHg
plusoneormoreof:
• Neurologicalproblems
• Proteinuria
• Renalinsufficiency
• Liverdisease
• Haematologicaldisturbances
• Fetalgrowthrestriction.
Eclampsiaandpre-eclampsiaareleadingcausesofperinatalandmaternalmorbidityandmortality.Theycanleadtoplacentalabruption,DIC,cerebralhaemorrhage,hepaticfailureandacuterenalfailure.[2]
Thepre-hospitalmanagementofeclampsiaandpre-eclampsiaissupportivecareandthepreventionofeclampsia.
HELELP syndromeisconsideredavariantofseverepre-eclampsia(H aemolysis,E levatedL iverE nzymesandL owP latlets)[2]
RiskFactorsforpre-eclampsia:
• Primagravida
• Historyofpre-eclampsia
• Extremesofmaternalage
• Renaldisease
• Diabetes
• Obesity
• Familyhistory
Page1of2

Standard Cares
Evidenceofeclampsia?
Consider:• IVfluid• Magnesiumsulphate
Highriskofeclampsia?• CNSdysfunction• Severepre-eclampsia
Minimise risk of eclampsia:• Maintainquietenvironment• Minimisebodymotion• Attainpositionofcomfort
Eclampsia• 1stlineoftreatmentismagnesiumsulphate
• 2ndlineoftreatmentismidazolamifmagnesiumsulphateisunavailableorseizureprolonged
Transporttohospital
Pre-notifyasappropriate
Risk assessment
• Fluidadministrationshouldbeconservative,duetothehighriskofpulmonaryoedema.
• Patientssuspectedordiagnosedwithseverepre-eclampsiaaredeemedhighriskofeclampsia.
Definitive care
Theonlycureforpre-eclampsiaisdeliveryoftheplacenta,thereforecontinuedgestationpost-diagnosisisbasedonabalancebetweenpotentialmaternalmorbidityandcontinuedfetaldevelopment,withbothpatientsrequiringclosesurveillance.Drugtherapyoftenincludesantihypertensivesforthemotherandantenatalcorticosteroidstoacceleratefetallungmaturation.[3]
Pre-eclampsia–Page2of2
Version 1.0 – September 2011
Clinical practice guidelines Primary postpartum haemorrhage
Risk assessment
• Nil
Additional information
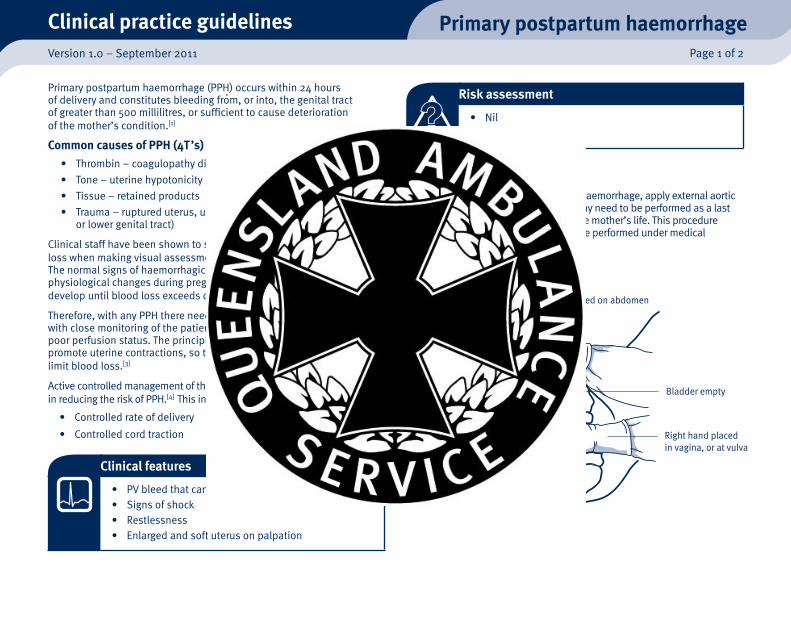
Inthecaseoftorrentialoruncontrolledhaemorrhage,applyexternalaorticcompression.Bimanualcompressionmayneedtobeperformedasalastresortwhenallelsehasfailedtosavethemother’slife.Thisprocedureisdifficult,extremelypainfulandmustbeperformedundermedicalconsultation.
Primarypostpartumhaemorrhage(PPH)occurswithin24hoursofdeliveryandconstitutesbleedingfrom,orinto,thegenitaltractofgreaterthan500millilitres,orsufficienttocausedeteriorationofthemother’scondition.[1]
Common causes of PPH (4T ’s)• Thrombin–coagulopathydisorders
• Tone–uterinehypotonicity
• Tissue–retainedproducts
• Trauma–ruptureduterus,uterineinversion,tearsofupperorlowergenitaltract)
ClinicalstaffhavebeenshowntosignificantlyunderestimatePPHbloodlosswhenmakingvisualassessments,sometimesbymorethan50%.[2]
Thenormalsignsofhaemorrhagicshockareoftenmaskedbythephysiologicalchangesduringpregnancyandsotachycardiamaynotdevelopuntilbloodlossexceedsonelitre.[2]
Therefore,withanyPPHthereneedstobeahighdegreeofsuspicion,withclosemonitoringofthepatienttoensureearlyrecognitionofapoorperfusionstatus.TheprinciplemanagementofprimaryPPHistopromoteuterinecontractions,sothatthe‘livingligatures’cannaturallylimitbloodloss.[3]
ActivecontrolledmanagementofthethirdstageoflabourisaleadingfactorinreducingtheriskofPPH.[4]Thisincludes:
• Controlledrateofdelivery
• Controlledcordtraction
Clinical features
• PVbleedthatcanbetorrentialanduncontrolled• Signsofshock• Restlessness• Enlargedandsoftuterusonpalpation
Uterus is pressedbetween hands
Left hand placed on abdomen
Bladder empty
Right hand placed in vagina, or at vulva
Bimanualcompression
Page1of2
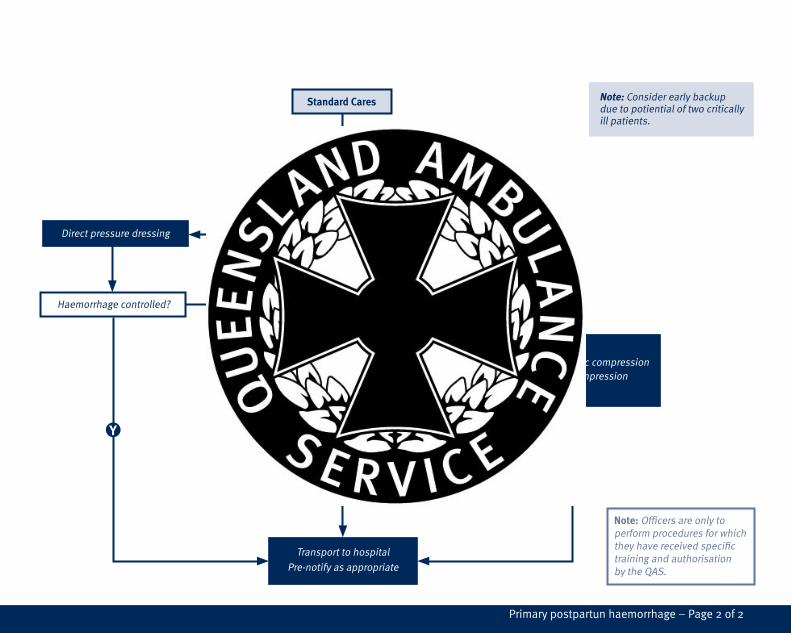
Standard Cares
Torrential/uncontrolledhaemorrhage?
Note: Considerearlybackupduetopotientialoftwocriticallyillpatients.
Obviousexternaltearing?Directpressuredressing
Massagefundus
Consider:• Externalaorticcompression• Bimanualcompression• IVfluid
TransporttohospitalPre-notifyasappropriate
Haemorrhagecontrolled?
Haemorrhagecontrolled?
Consider:• Suckling• Emptyingbladder• IVfluid
Note:OfficersareonlytoperformproceduresforwhichtheyhavereceivedspecifictrainingandauthorisationbytheQAS.
Primarypostpartunhaemorrhage–Page2of2

Version 1.0 – September 2011
Clinical practice guidelines Secondary postpartum haemorrhage
Clinical features
• OngoingPVbleed
• Changeinlochia–regressiontobrightredincreasingamounts,thelochiamaybeoffensive
• Pain–usuallylowerabdominal/pelvic
• Anaemia
• Pyrexia
• Sepsis
Risk assessment
• Nil
Secondarypostpartumhaemorrhage(PPH)isdefinedasbleedingfrom,orinto,thegenitaltract>24hours,oruptosixweeksafterdelivery.[1]Furthermore,theamountofbloodshouldbe500millilitresormore,orsufficientlosstocauseadeteriorationinthepatient’scondition.SecondaryPPHcanbecausedby:
• Infection
• Retainedfragmentsoftheplacentaormembranes.
Thisresultsinafailureoftheuterustocontract(sub-involution)leadingtoSPPH.
Definitive Care
• Drugtherapy–antibiotic,oxytocics,hormonetherapy
• Surgicalmanagement.
Page1of2

Standard Cares
Haemodynamicallyunstable?ManageasperCPG:• Sepsis
Transporttohospital
Pre-notifyasappropriate
Consider:
• IVfluid• Analgesia
Seondarypostpartumhaemorrhage–Page2of2
Version 1.0 – September 2011
Clinical practice guidelines Shoulder dystocia
Clinical features
Shoulderdystociausuallybecomesobviousafterthefetalheademergesandretractsupagainsttheperineum,failingtoundergoexternalrotation(turtlesign).[3]
Shoulderdystociaisconfirmedwhenthestandarddeliverymanoeuvres(downwardtraction)failtodeliverthefetusandtheheadtobodydeliveryintervalisprolonged≥60seconds.[4]
Risk assessment [5]
Anincreasedriskofshoulderdystociaisreportedinassociationwith:
• Prolongedsecondstageoflabour
• Assisteddelivery
• Maternaldiabeteswithorwithoutmacrosomia
• Previousshoulderdystocia
• Alargefetus>4.5kg(macrosomia)• Historyofalargefoetus
• Maternalobesity
• Multiparity.
Anycombinationoftheabovefactorsmaysignificantlyincreasetheriskofshoulderdystocia.
Inshoulderdystocia,disproportionoccursbetweenthebisacromialdiameterofthefetusandtheantero-posteriordiameterofthepelvicinlet,resultinginimpactionoftheanteriorshoulderofthefetusbehindthesymphysispubis.[1]
Difficultdeliveryensues,requiringtheuseofadditionalmanoeuvresbeyondthedownwardtractionofthefetalhead.
Shoulderdystocia–WoodsScrewManoeuvre
Shoulderdystociaisassociatedwithseriouscomplicationsforboththemotherandbaby.[1]Perinatalmorbidityincludesasphyxia,birthtraumasuchasbrachialplexusinjuryandfracturedclavicles,andpermanentneurologicaldamage.
Fetaldeathcanalsooccurifnotrecognisedimmediatelyandtreatedpromptly.[2]
Impacted anterior shoulder
Page1of4
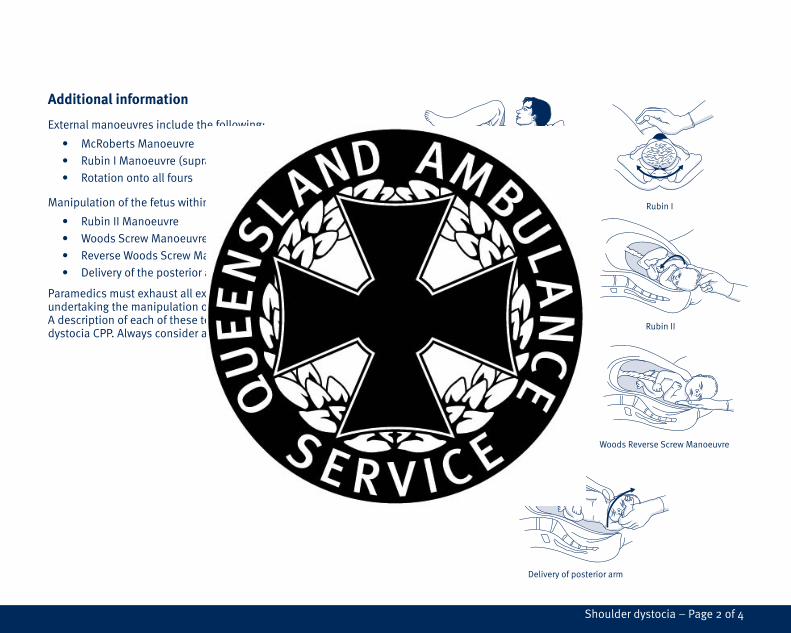
Additional information
Externalmanoeuvresincludethefollowing:
• McRobertsManoeuvre
• RubinIManoeuvre(suprapubicpressure)
• Rotationontoallfours
Manipulationofthefetuswithinthebirthcanalinclude:
• RubinIIManoeuvre
• WoodsScrewManoeuvre
• ReverseWoodsScrewManoeuvre
• Deliveryoftheposteriorarm
Paramedicsmustexhaustallexternalmanoeuvresfirstbeforeundertakingthemanipulationofthefetuswithinthebirthcanal.AdescriptionofeachofthesetechniquesisgivenintheshoulderdystociaCPP.Alwaysconsiderappropriatepainreliefasrequired.
Rubin II
Woods Screw Manoeuvre Woods Reverse Screw Manoeuvre
Rotation to all fours
Delivery of posterior arm
Rubin IMcRoberts Manoeuvre
Shoulderdystocia–Page2of4
Version 1.0 – September 2011
Clinical practice guidelines Shoulder dystocia
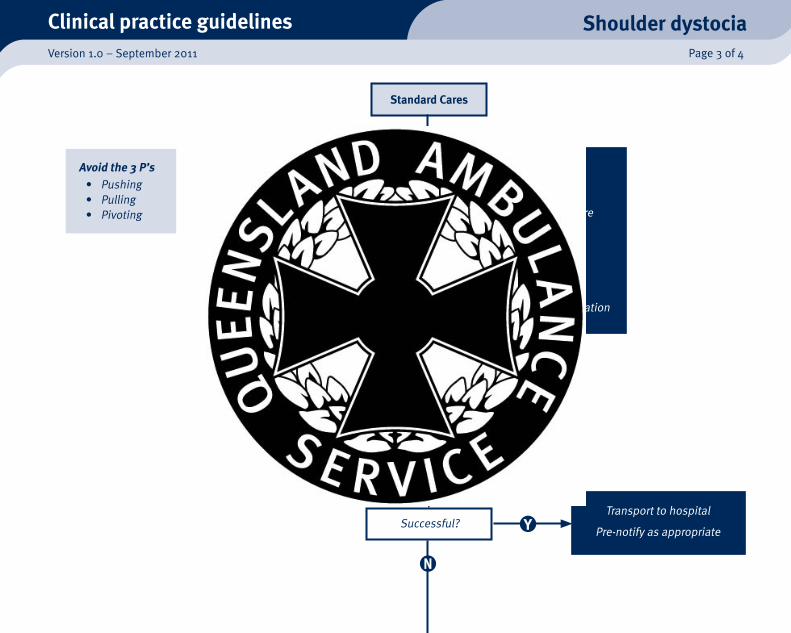
Standard Cares
Position• Drawmaternalbuttockstotheedgeofthebed(removeorlowerthebottomofthebed)
• Flattentopofbed(onepillowonly)–McRobertsmanoeuvre
Consider:•Needforbackup•Urgency-Starttimerwhenshoulderdystociaisrecognised-Aimtodeliverbabywithin4minutes
• ExternalmanoeuvresBEFOREattemptinginternalmanipulation
Successful?
External Manoeuvres• McRobertsmanoeuvre• Suprapubicpressure(RubinI)• Applymoderatedownwardtractiontofetalheadaimingtodelivertheanteriorshoulder
Transporttohospital
Pre-notifyasappropriate
Avoid the 3 P’s• Pushing• Pulling• Pivoting
Page3of4
Transporttohospital
Pre-notifyasappropriate
Internal manoeuvres
Listedinorderofimplementation:•RubinII•Woodsscrew•ReverseWoodsscrew•Deliveryoftheposteriorarm
Consider:•Gainingconsent•Timing-Donotspendtoolongoneachmanoeuvre
Document of events:Definetheseverityoftheshoulderdystocia(relativetothemanoeuvresrequired).Documentevents,managementandtheirtiming.Be prepared for sequelae:Mother: Postpartumhaemorrhage Perinealtrauma PsychologicaltraumaBaby: Birthtrauma Hypoxia
Shoulderdystocia–Page4of4
Version 1.0 – September 2011
Clinical practice guidelines Uterine inversion
Clinical features
• Themostcommonpresentationispostpartumhaemorrhage.[1]
• Visualexaminationmayrevealamassatthevulva,butthisisonlyinaprolapseduterineinversion.
• Evidenceofshockiscommon.
• Severeabdominal/pelvicpainoccursduetoexcessivetractiononthebroadligamentandovarianligaments.
Risk assessment
• Thesepatientsareathighriskforinfection.Therefore,useanaseptictechniqueandalwaystakeappropriateinfectioncontrolmeasures.
Uterineinversionisarare,butpotentiallylife-threatening,obstetricemergencywheretheuteruscollapsesinonitselftovaryingdegrees:[1]
• Incomplete–thefundusreachesthecervix.
• Complete –thefunduspassesthroughthecervix,butdoesnotreachthevaginalopening.
• Prolapsed–thefundusextendsthroughthevaginalopening.
Thereisafurtherdifferentiationbytiming:
• Acute–lessthan24hourspostdelivery.
• Subacute–from24hoursto4weeks.
• Chronic –beyond4weeks.
Althoughtherearenodefinitivecauses,acommonfactorisanover-aggressivemanagementofthethirdstageoflabour,whichincludesexcessivefundalmassageandcordtractionpriortoplacentalseparation.[1]
Theprinciplepre-hospitalmanagementisaimedatsupportivecare,treatmentforshockandrapidtransporttoanappropriatefacility.[2]
Page1of2
Standard Cares
Istherepostpartumhaemorrhage?
Transporttohospital
Pre-notifyasappropriate
Consider:• Analgesia• Assistpatienttoattainpositionofcomfort
• Protectanyexposeduteruswithmoiststeriledressings
Consider:• IVfluid• Analgesia
Uterineinversion–Page2of2
Version 1.0 – September 2011
Clinical practice guidelines Uterine rupture
Clinical features
Clinicalpresentationcanvaryfromsubtletosevere:[1]
• Uterinetenderness
• Nonreassuringfetalheartpatterns
• Lossofintrauterinepressureorcessationofcontractions
• Abnormallabourorfailuretoprogress
• Severelocalisedabdominalpain
• Vaginalbleeding
• Maternalhypovolaemicshock.
Risk assessment
• Nil
Uterineruptureisdefinedasatearingoftheuterinewallduringpregnancyordelivery.Itisoneofthemostlife-threateningobstetricemergencieswithahighrateofbothfetalandmaternalmortality.[1]AlthoughthemajorityofcasesarecausedbyapreviousCaesareanscar,[2]spontaneousincidencesdooccurandshouldbesuspectedifthereis:
• Evidenceofmaternalshock
• Difficultydefiningtheuterusonpalpation
• Easilypalpablefetalparts.
OtherthanahistoryofCaesareansectionoruterinesurgery,riskfactorsinclude:[1]
• Trauma
• Uterineanomalies
• Dystocia
• Useofuterotonicdrugs(inducedlabour)[3]
• Abnormalplacentation
• Advancedmaternalage
• Highbirthweight.
Page1of2
Standard Cares
Avoidaortocavalcompression
Traumarelated?
Evidenceofshock?
Transporttohospital
Pre-notifyasappropriate
Consider:• IVaccess• Analgesia• Assistpatienttoattainpositionofcomfort
ManageasperCPG:• Traumainpregnancy
ManageasperCPG:• Shock
Uterinerupture–Page2of2