ct guided electromagnetic navigational bronchoscopy · manual registration is used when a 3d map is...
TRANSCRIPT
CT Guided Electromagnetic Navigational Bronchoscopy
Thomas A. D’Amico MDGary Hock Professor of Surgery
Chief Thoracic Surgery, Chief Medical OfficerDuke Cancer Institute
Duke Thoracoscopic Lobectomy WorkshopMarch 21, 2018
Disclosures
• Consultant for Scanlan
• No conflicts related to this presentation
Electromagnetic Navigational Bronchoscopy
• Distal bronchoscopic and trans-bronchoscopicnavigation based on registration of CT scans with proximal bronchoscopy
• Provides multi-dimensional views during navigation: axial, coronal, sagittal, local
• Guides the placement of the tip of the navigation catheter within 3-4 mm of the target
Goals of ENB
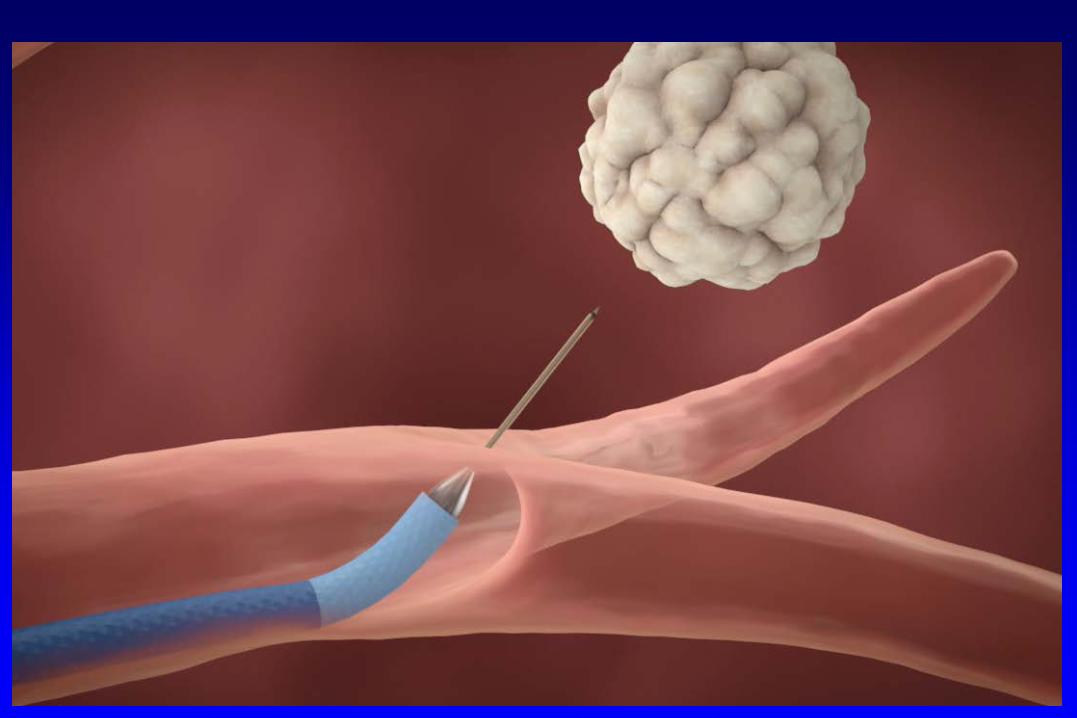
1. Biopsy (needle, core, brush, forceps)
2. Marking small lesions with dye or fiducials for resection
3. Ablation
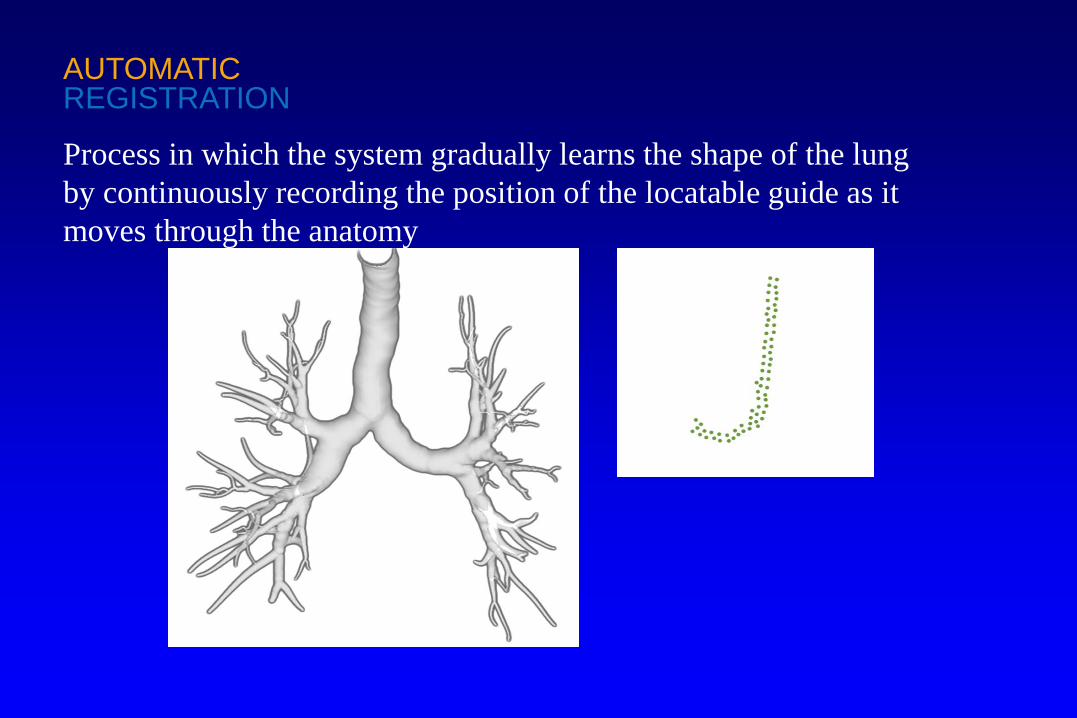
AUTOMATICREGISTRATION
Process in which the system gradually learns the shape of the lung by continuously recording the position of the locatable guide as it moves through the anatomy
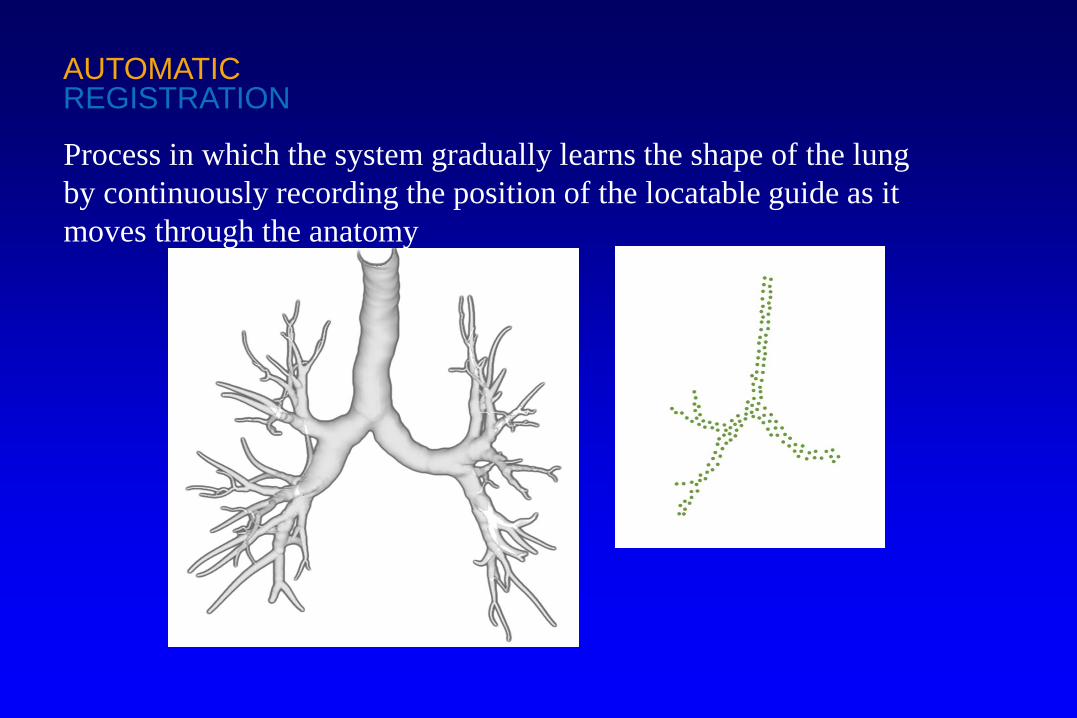
AUTOMATICREGISTRATION
Process in which the system gradually learns the shape of the lung by continuously recording the position of the locatable guide as it moves through the anatomy
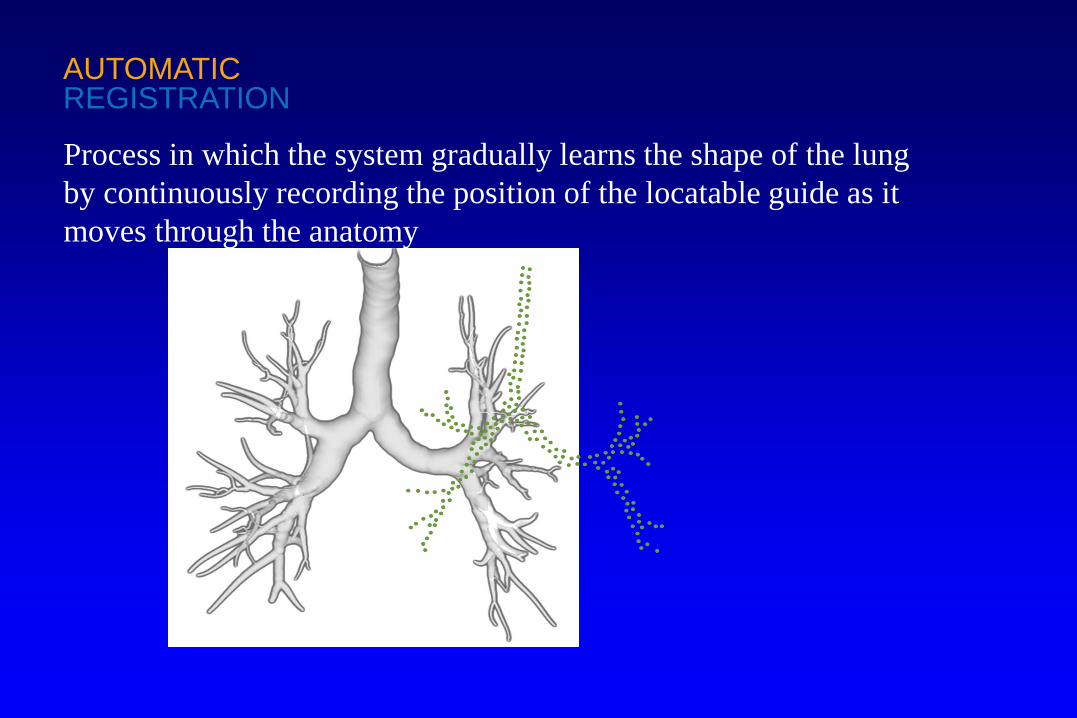
AUTOMATICREGISTRATION
Process in which the system gradually learns the shape of the lung by continuously recording the position of the locatable guide as it moves through the anatomy
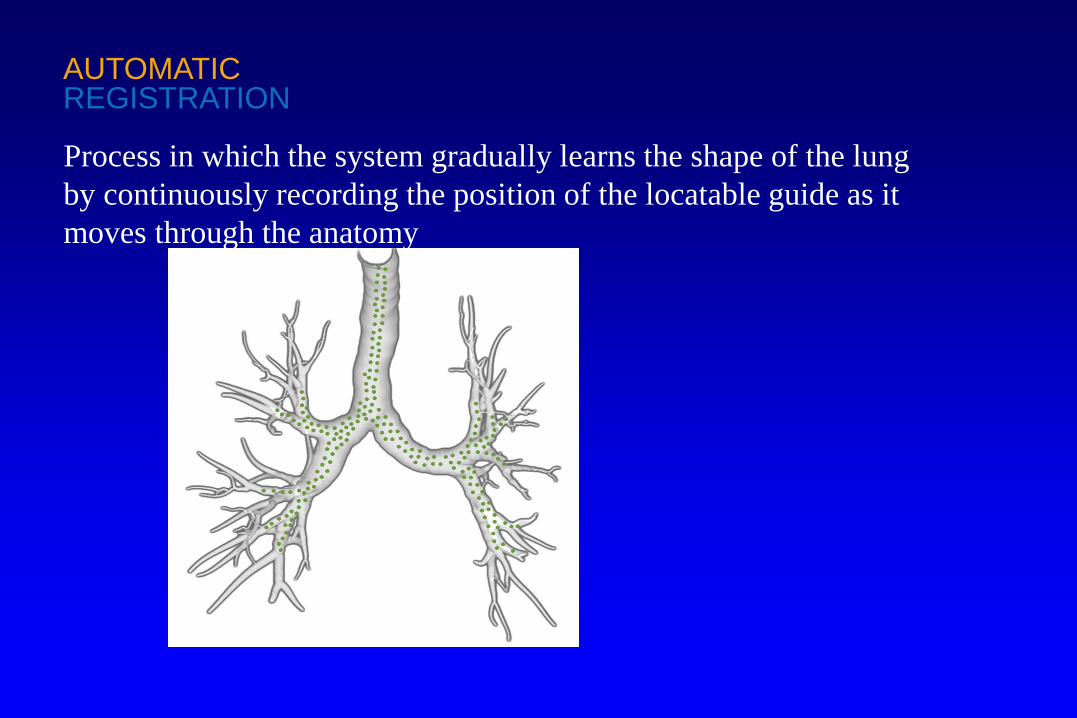
AUTOMATICREGISTRATION
Process in which the system gradually learns the shape of the lung by continuously recording the position of the locatable guide as it moves through the anatomy
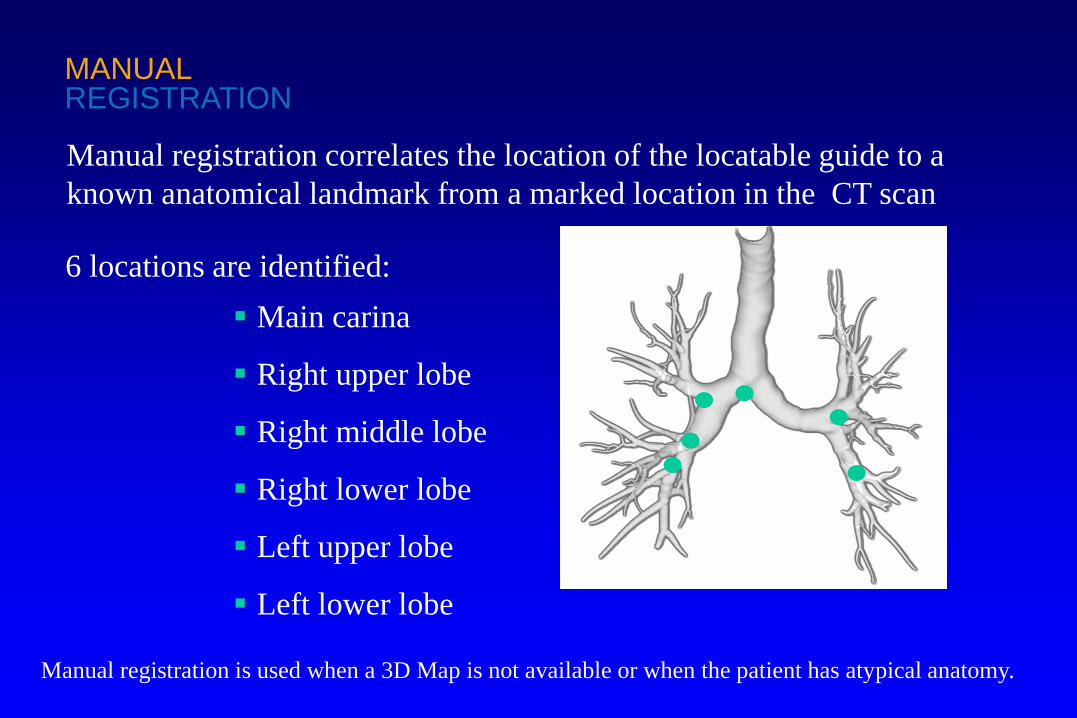
Manual registration is used when a 3D Map is not available or when the patient has atypical anatomy.
6 locations are identified: Main carina
Right upper lobe
Right middle lobe
Right lower lobe
Left upper lobe
Left lower lobe
MANUALREGISTRATION
Manual registration correlates the location of the locatable guide to a known anatomical landmark from a marked location in the CT scan
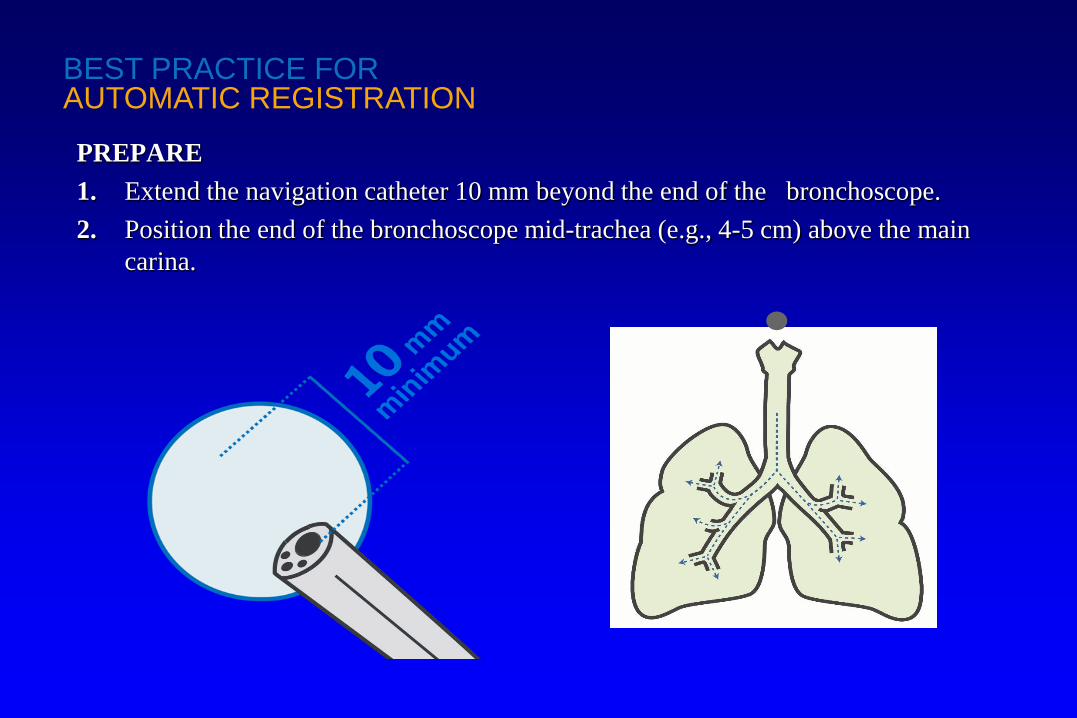
PREPARE1. Extend the navigation catheter 10 mm beyond the end of the bronchoscope.2. Position the end of the bronchoscope mid-trachea (e.g., 4-5 cm) above the main
carina.
BEST PRACTICE FORAUTOMATIC REGISTRATION

PREPARE1. Extend the navigation catheter 10 mm beyond the end of the bronchoscope.2. Position the end of the bronchoscope mid-trachea (e.g., 4-5 cm) above the main
carina.
BEST PRACTICE FORAUTOMATIC REGISTRATION
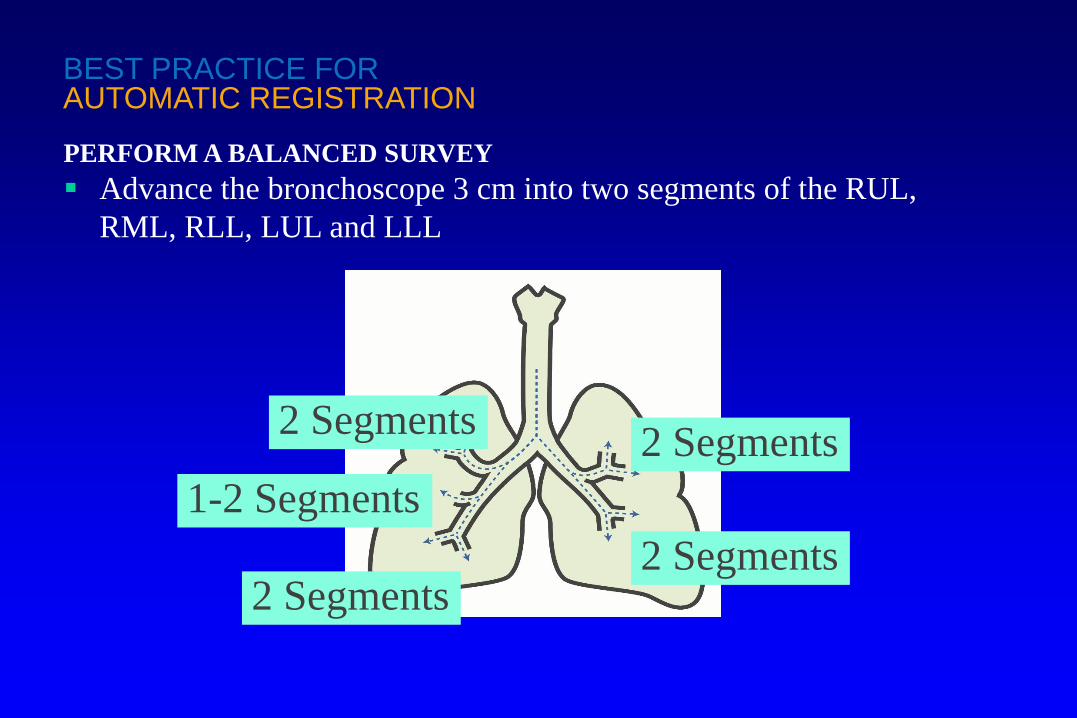
PERFORM A BALANCED SURVEY Advance the bronchoscope 3 cm into two segments of the RUL,
RML, RLL, LUL and LLL
1-2 Segments2 Segments
2 Segments2 Segments
2 Segments
BEST PRACTICE FORAUTOMATIC REGISTRATION
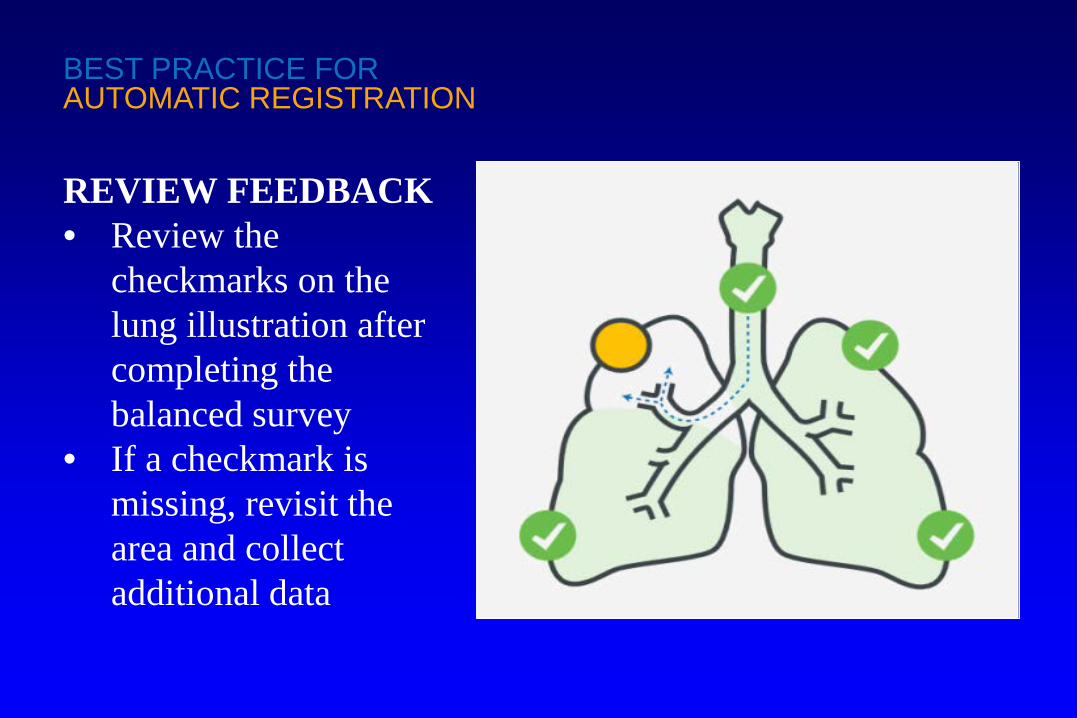
REVIEW FEEDBACK• Review the
checkmarks on the lung illustration after completing the balanced survey
• If a checkmark is missing, revisit the area and collect additional data
BEST PRACTICE FORAUTOMATIC REGISTRATION

VERIFICATION1. Verify alignment on the
CT views2. Verify on at least two
carinas along the planned pathway, preferably until the bronchoscope approaches a wedged position
BEST PRACTICE FORAUTOMATIC REGISTRATION
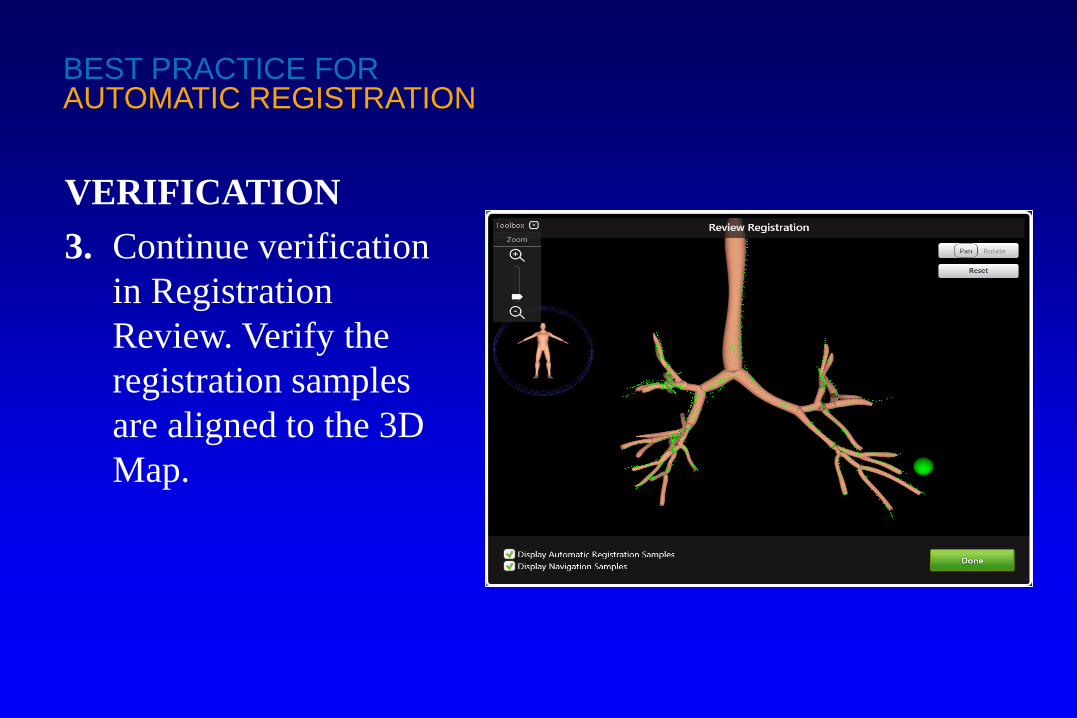
VERIFICATION3. Continue verification
in Registration Review. Verify the registration samples are aligned to the 3D Map.
BEST PRACTICE FORAUTOMATIC REGISTRATION
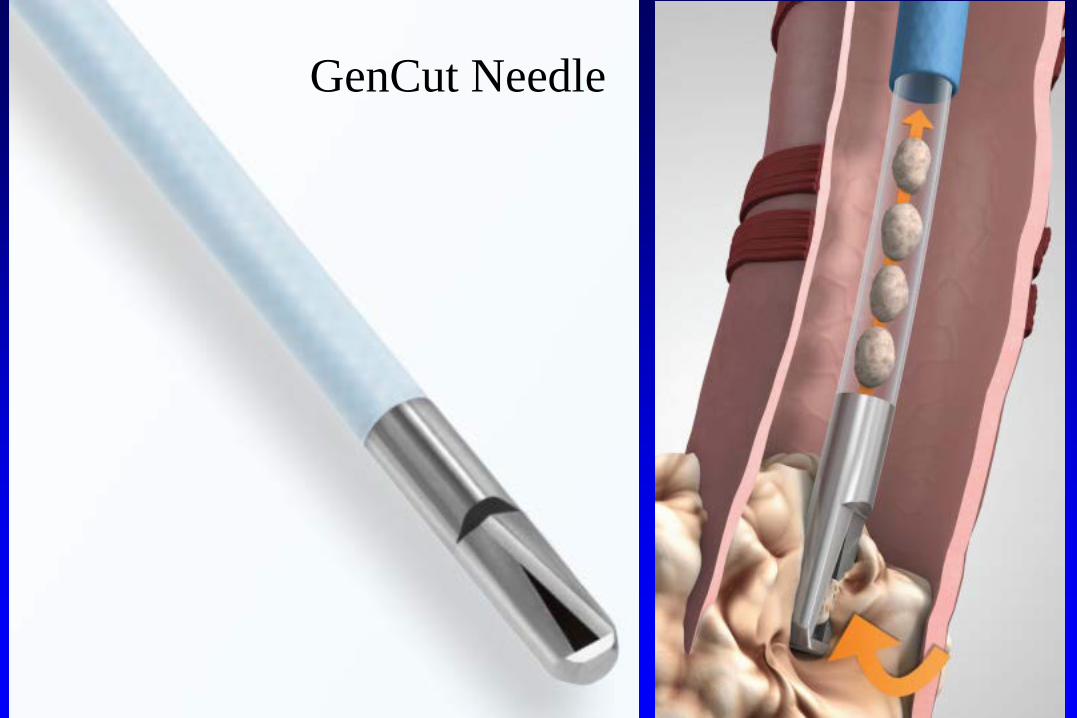
GenCut Needle
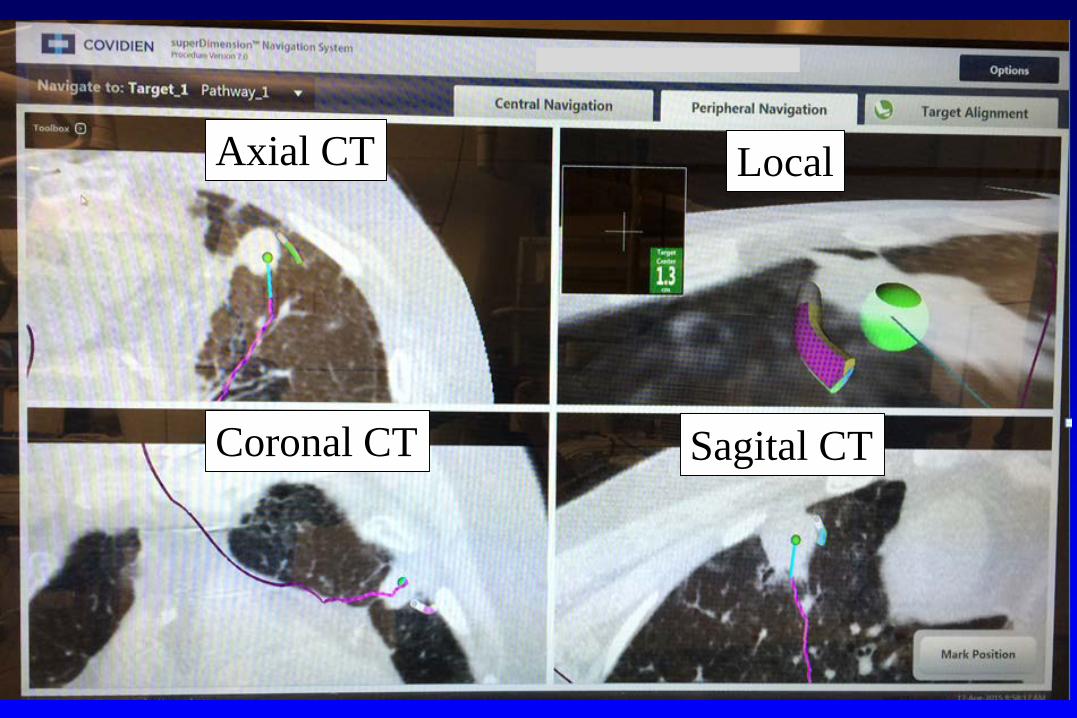
Axial CT
Coronal CT Sagital CT
Local
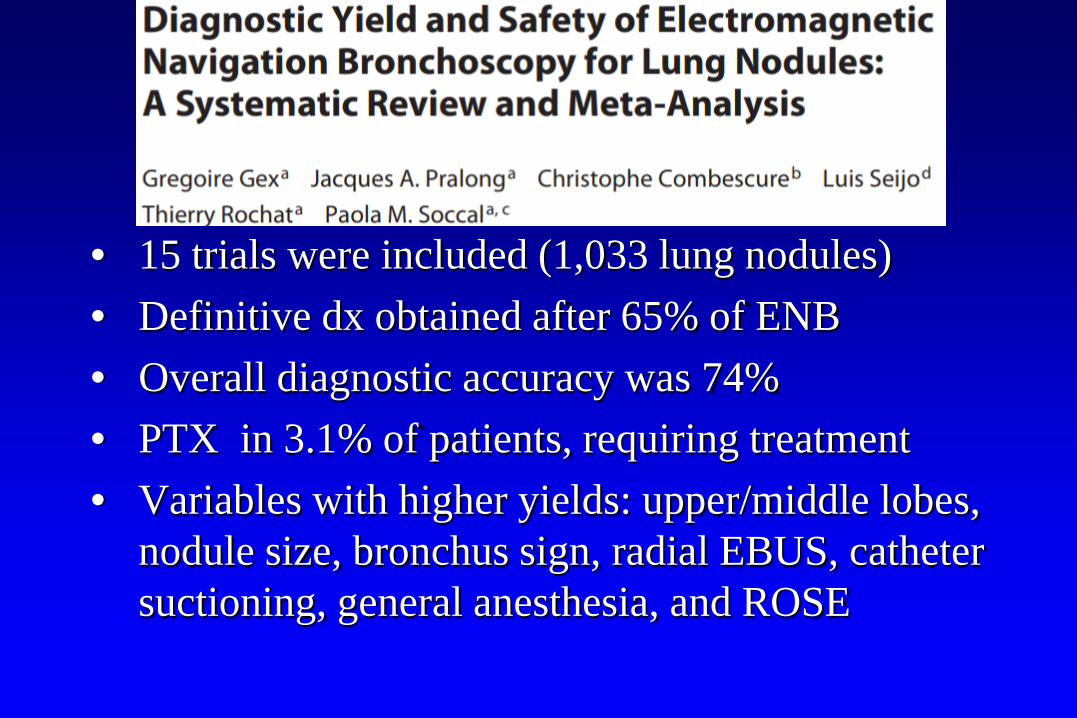
• 15 trials were included (1,033 lung nodules)• Definitive dx obtained after 65% of ENB• Overall diagnostic accuracy was 74% • PTX in 3.1% of patients, requiring treatment• Variables with higher yields: upper/middle lobes,
nodule size, bronchus sign, radial EBUS, catheter suctioning, general anesthesia, and ROSE

Accuracy for Malignancy
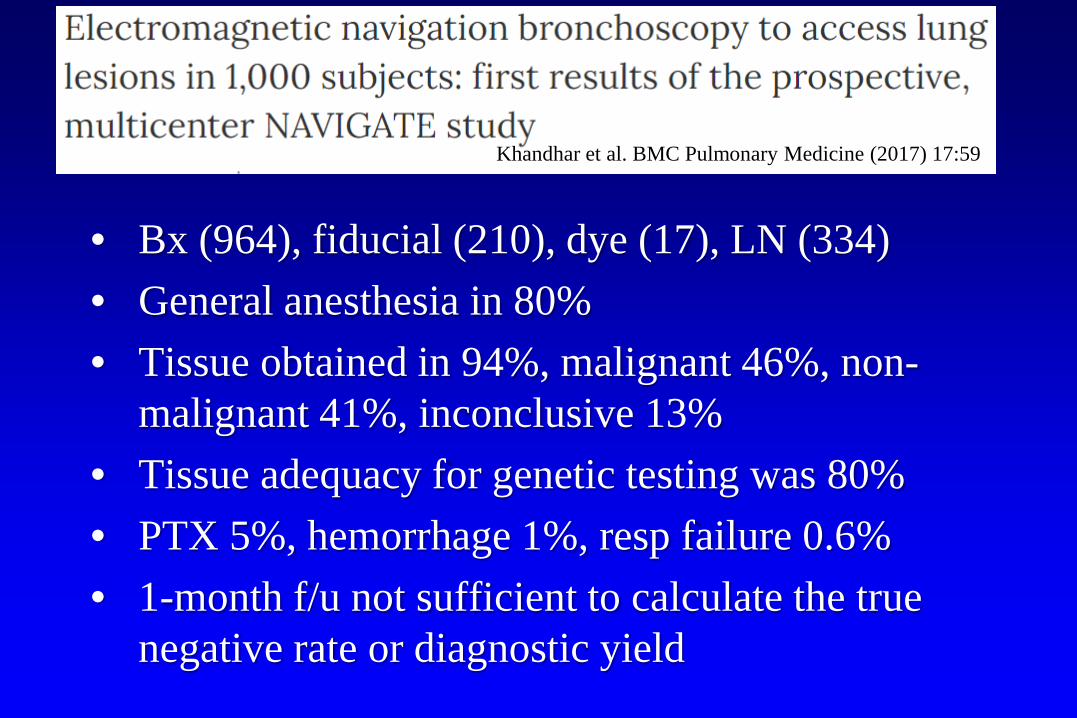
• Bx (964), fiducial (210), dye (17), LN (334)• General anesthesia in 80% • Tissue obtained in 94%, malignant 46%, non-
malignant 41%, inconclusive 13%• Tissue adequacy for genetic testing was 80%• PTX 5%, hemorrhage 1%, resp failure 0.6%• 1-month f/u not sufficient to calculate the true
negative rate or diagnostic yield
Khandhar et al. BMC Pulmonary Medicine (2017) 17:59
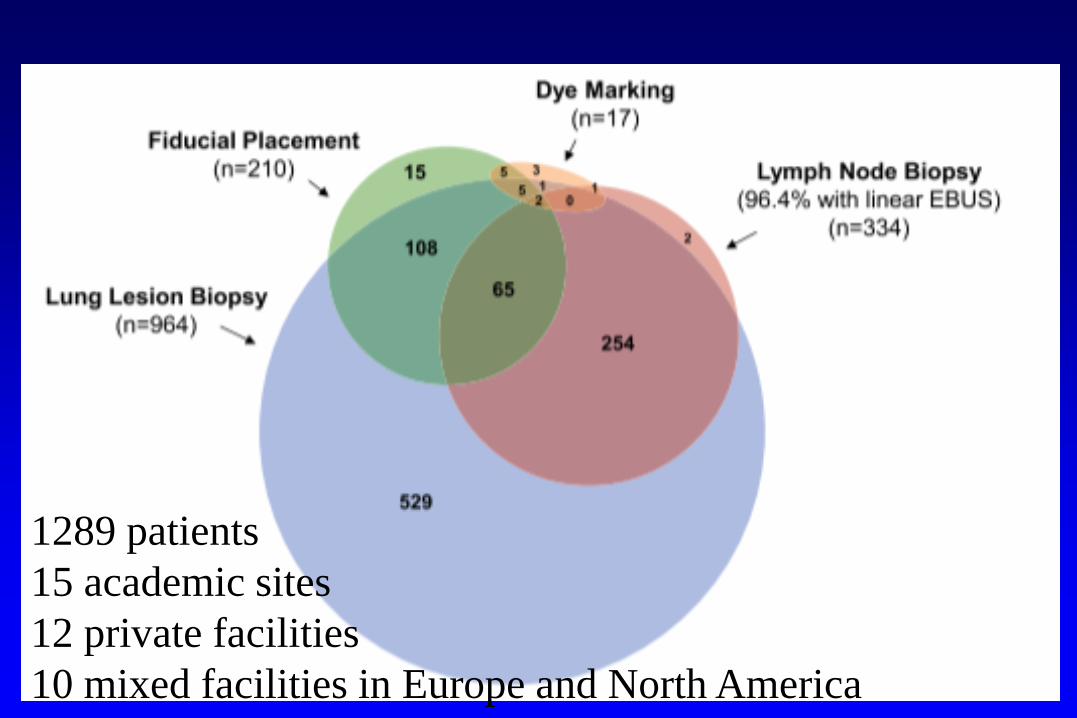
1289 patients15 academic sites12 private facilities10 mixed facilities in Europe and North America

CT-Guided Navigational Bronchoscopy
• Fluoroscopy is limited• 2-dimensional• Small lesions are difficult to visualize• Ground glass opacities are impossible to
visualize• CT-Guided ENB may improve success rate of
biopsy and may be used in the future for ablation
CT Options
1. Cone beam CT
2. Airo Mobile Intraoperative CT
3. Dedicated CT

Airo Mobile Intraoperative CT
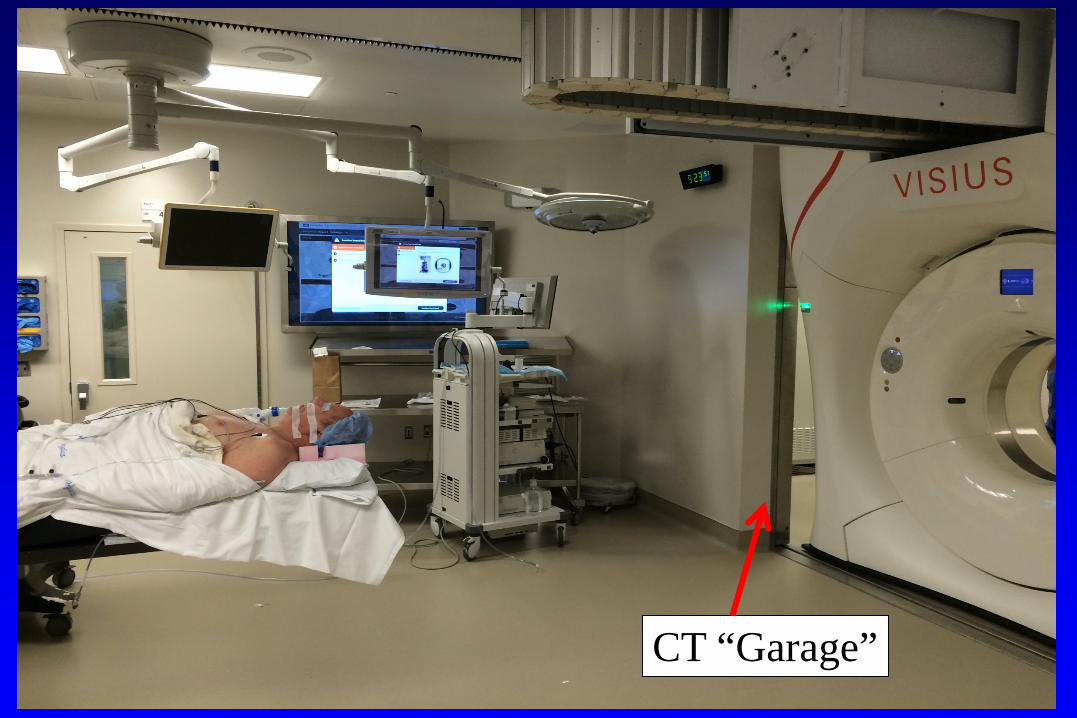
CT “Garage”
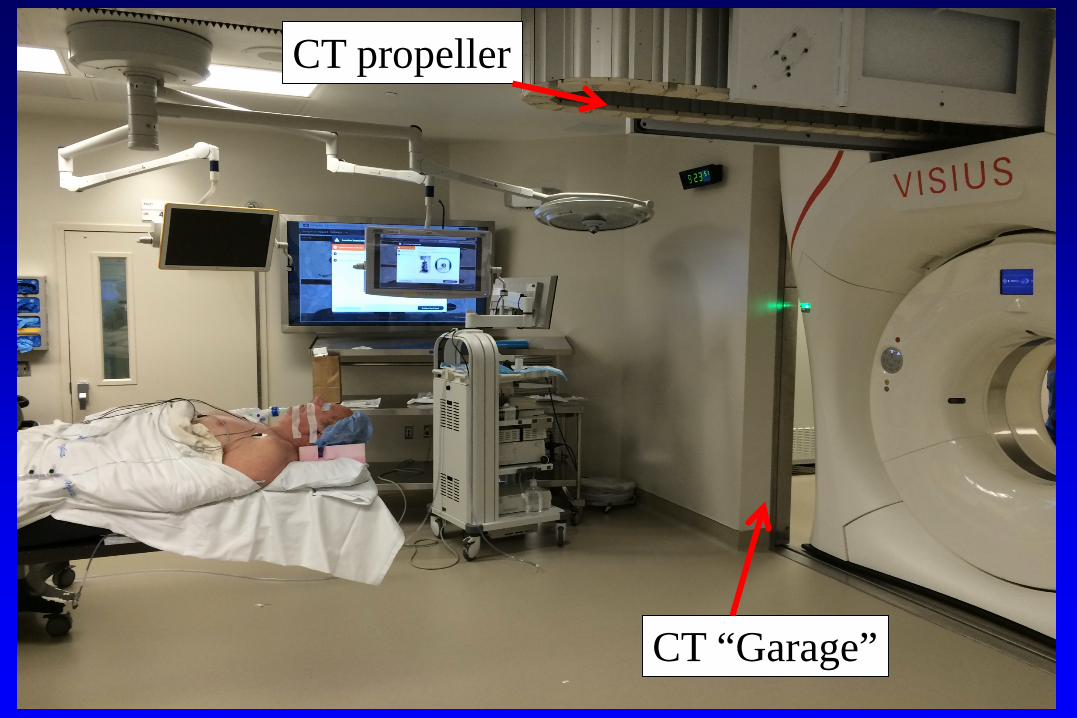
CT “Garage”
CT propeller

un
CT “Garage”
CT propeller
CT compatible bed
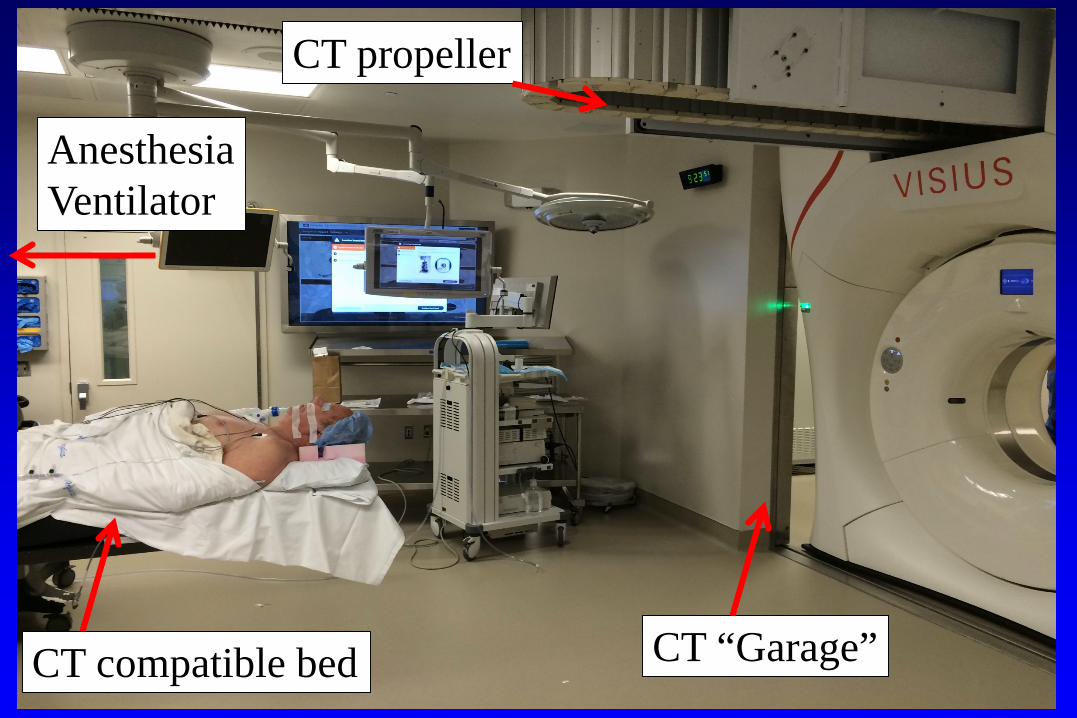
CT “Garage”
CT propeller
CT compatible bed
AnesthesiaVentilator

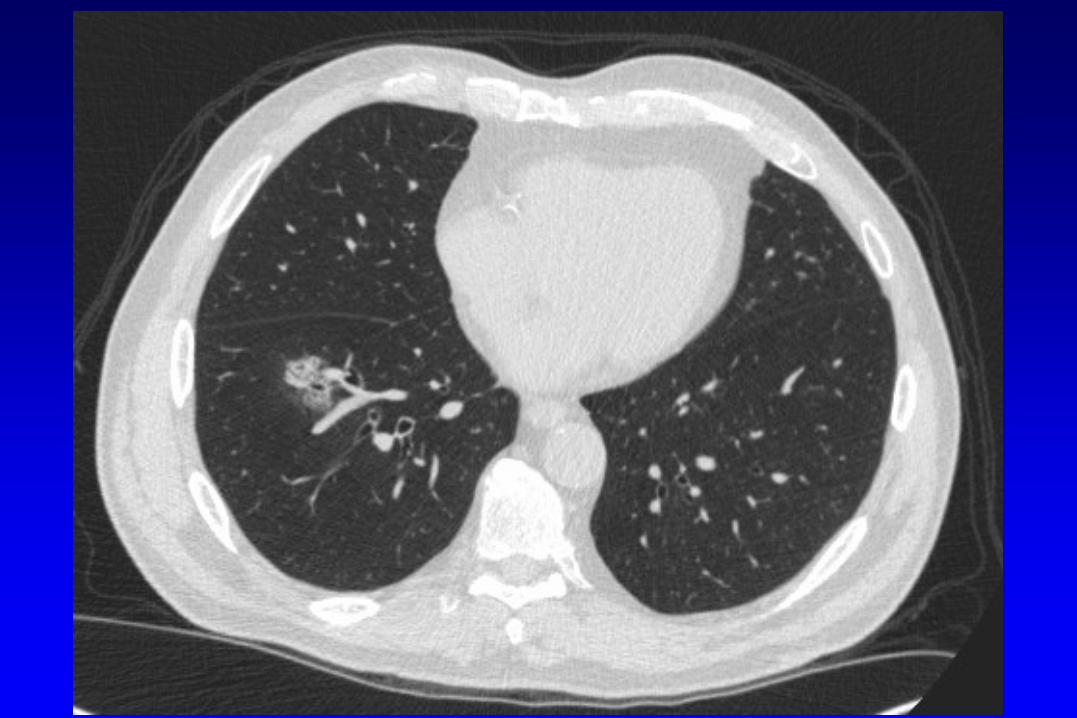
Case
• 68 year old man with a mixed GGO• CT-guided biopsy negative• Anatomically unsuitable for segmentectomy• High-risk surgical candidate to proceed with
lobectomy without a diagnosis
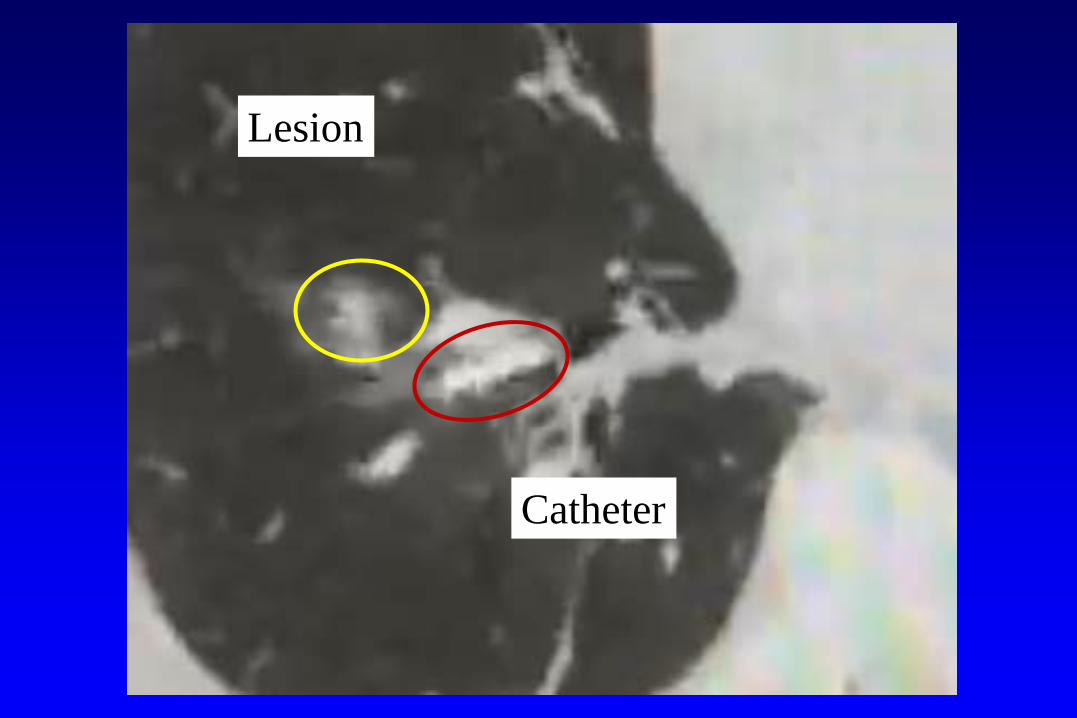
Lesion
Catheter


Lesion
Catheter

Cross Country

Emprint™ Microwave Ablation System with Thermosphere™ Technology
• Thermal control: minimizes uncontrolled thermal factors that contribute to a passive ablation zone
• Field control: delivers a precise, scalable spherical field
• Wavelength control: prevents wavelength elongation as tissue becomes desiccated or charred and its properties change during ablation

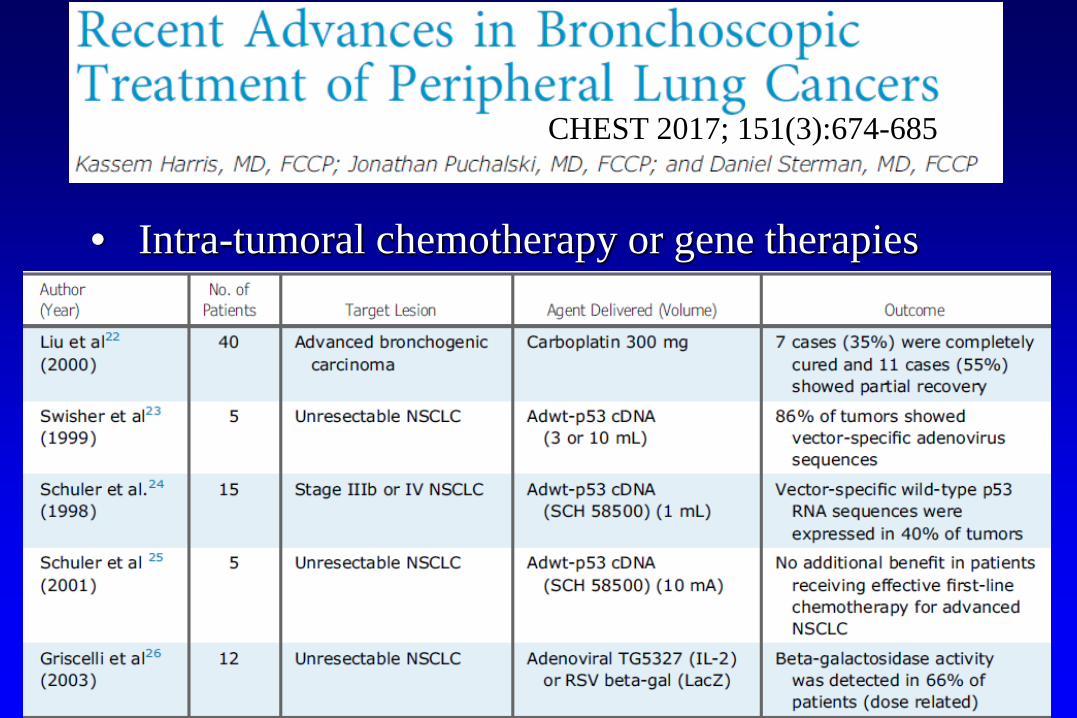
• Intra-tumoral chemotherapy or gene therapies
CHEST 2017; 151(3):674-685

CT Guided ENB
• Facilitates precise location of nodules for biopsy• Would be mandatory for ablation• Cross-country trans-bronchoscopic technology
will improve the ability to biopsy, mark or ablate more lesions
The Future
• CT screening: Higher proportion of early stage patients, and preoperative biopsy is needed in a subgroup
• Some patients may elect for resection; others may choose ablation
• Thoracic surgeons should be able to diagnose, stage, resect, and ablate lung cancer