hiponatremia
DESCRIPTION
Artikel penelitianTRANSCRIPT
CASE REPORT
220 Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
An HIV Positive Man with Single Erythema Skin Lesion: a Case Report of Neglected Tropical Disease
Umar Zein1, Hadiki Habib2
1 Dr. Umar Zein Tropical Diseases and Infectious Clinic, Medan, Indonesia. 2 Department of Internal Medicine, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia.
Correspondence mail:Dr. Umar Zein Tropical Diseases and Infectious Clinic. Jl.Denai No.269 Medan, Indonesia. email: [email protected].
ABSTRAKLesi kulit sering dijumpai di penderita infeksi HIV. Kami melaporkan kasus seorang laki-laki usia 42
tahun dengan status HIV positif yang menderita lesi kulit kemerahan di kaki. Pemeriksaan fisik, anamnesis dan pemeriksaan laboratorium menunjukkan bahwa lesi kulit adalah cutaneous larva migrant akibat infeksi parasit. Cutaneous larva migrant akibat infeksi cacing tambang merupakan salah satu penyakit tropis yang terlupakan namun dapat menginfeksi individu dengan immunokompromi. Penyakit ini jarang dibahas dan mungkit tidak ditemukan di Negara-negara maju, namun merupakan penyakit yang sering dijumpai didaerah tropis. Lesi kulit pada pasien ini menghilang setelah diberikan terapi albendazole, cetirizine, chlorethyl semprot dan krim betamethasone.
Kata kunci: lesi kulit, cutaneous larva migrant, HIV.
ABSTRACTSkin lesion is common in person living with HIV. We reported a 42 years old HIV positive man with single
erythema skin lesion on the right foot. Clinical examination, anamnesis and laboratory examination revealed that it was cutaneous larva migrant due to parasitic infection. The cutaneous larva migrant due to hookworms is one of neglected tropical disease that might occur in adult with immunocompromised. This neglected disease is discussed rarely and might not be found in developed country, but it is still a common disease in the tropical region. Patient was treated successfully with albendazole, cetirizine, chlorethyl spray and betamethasone cream.
Key words: skin lesion, cutaneous larva migrant, HIV.
INTRODUCTIONSkin lesions are common in persons living
with the Human Immunodeficiency Virus (HIV). Dermatologic manifestations affect 80 to 90 percent of individuals infected with the HIV.1
Importantly, the number of mucocutaneous diseases in HIV-infected patients has been shown to correlate with prognosis and time to development of AIDS.1
The immunodeficiency state promote various unusual manifestasion of skin disease and unspesific laboratory findings in HIV. Due to this condition, a careful anamnesis and clinical evaluation is required in order to make accurate diagnosis and prompt treatment. Misdiagnosis will guide to mistreatment and this can subsequently lead to complication.
Vol 45 • Number 3 • July 2013 An HIV positive man with single erythema skin lesion
Here we report an HIV positive man with single erhytema skin lesion on the right foot. Clinical examination, anamnesis and laboratory examination revealed that it was cutaneous larva migrant due to parasitic infection. The cutaneous larva migrant is one of neglected tropical disease that might occur in adult with immunocompromised. Nowadays this neglected disease is discussed rarely and might not be found in developed country, but it is still a common disease in the tropical region and awareness should be addressed in traveler who just come back from tropical region.2 We also review the clinical manifestation, diagnosis, and treatment of cutaneous larva migrant.
CASE ILLUSTRATIONA 42 years-old HIV positive man attended
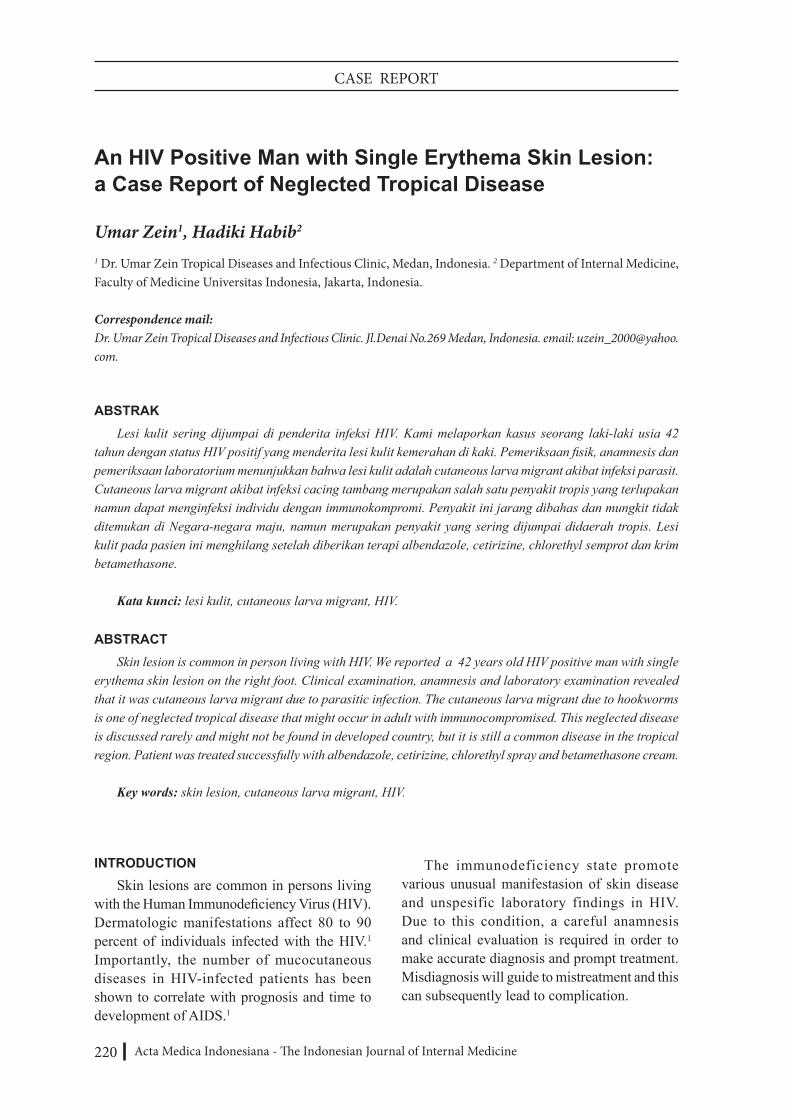
the infectious clinic because of itchy and redness in the right foot developed for one week (Figure 1). The symptoms was getting worse everyday, there was no different on severity of itch between day or night. The patient also complaint of localized rash on the right foot but no skin rash in other part of the body. The patient had neither fever nor cough and malaise. There was no complaint in defecation and miction.
Physical examination revealed normal vital sign, no abnormality in chest and abdomen. Local examination in dorsal region of right foot showed a redness serpiginous burrow extended from proximal third and fourth metatarsophalangeal to lower one third dorsal of the foot.
Neither anaemia nor leucocytosis showed in laboratory examination (Hb 13 g% and white blood cell 8600/ml, but there was eosinophilia (eosinophil: 8.5 %). Fecal examination showed no eggs worm or larvae.
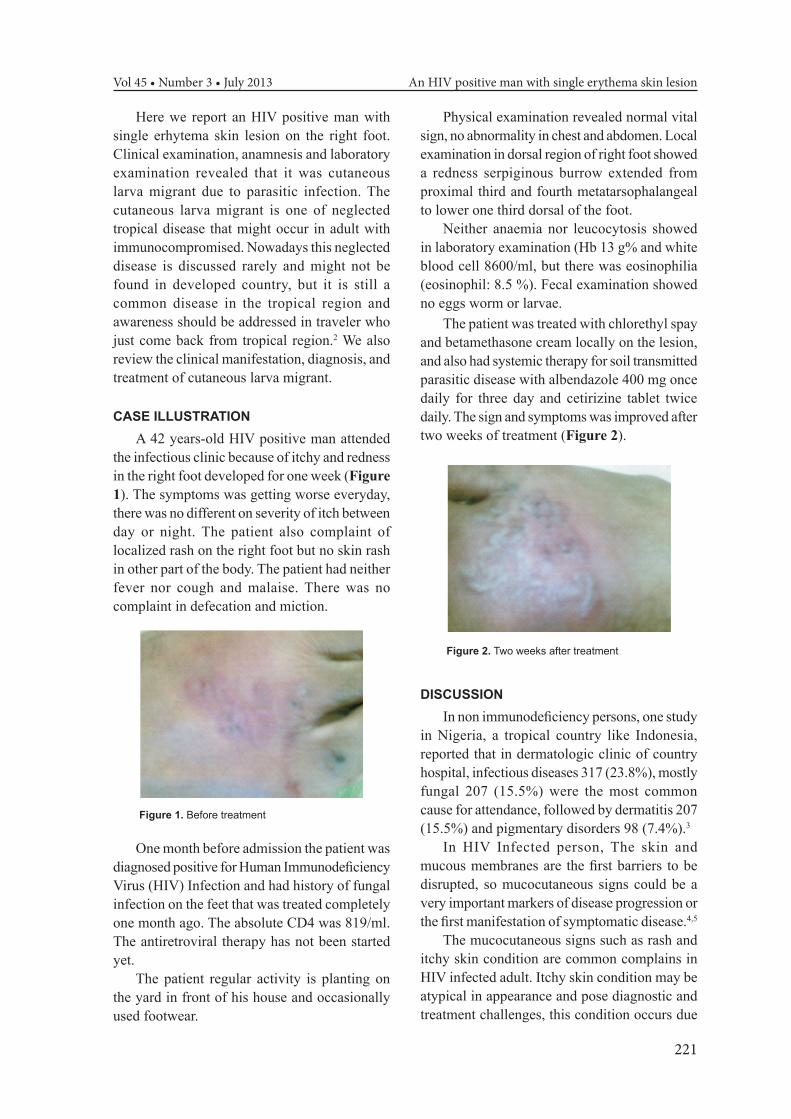
The patient was treated with chlorethyl spay and betamethasone cream locally on the lesion, and also had systemic therapy for soil transmitted parasitic disease with albendazole 400 mg once daily for three day and cetirizine tablet twice daily. The sign and symptoms was improved after two weeks of treatment (Figure 2).
Figure 1. Before treatment
One month before admission the patient was diagnosed positive for Human Immunodeficiency Virus (HIV) Infection and had history of fungal infection on the feet that was treated completely one month ago. The absolute CD4 was 819/ml. The antiretroviral therapy has not been started yet.
The patient regular activity is planting on the yard in front of his house and occasionally used footwear.
Figure 2. Two weeks after treatment
DISCUSSIONIn non immunodeficiency persons, one study
in Nigeria, a tropical country like Indonesia, reported that in dermatologic clinic of country hospital, infectious diseases 317 (23.8%), mostly fungal 207 (15.5%) were the most common cause for attendance, followed by dermatitis 207 (15.5%) and pigmentary disorders 98 (7.4%).3
In HIV Infected person, The skin and mucous membranes are the first barriers to be disrupted, so mucocutaneous signs could be a very important markers of disease progression or the first manifestation of symptomatic disease.4,5
The mucocutaneous signs such as rash and itchy skin condition are common complains in HIV infected adult. Itchy skin condition may be atypical in appearance and pose diagnostic and treatment challenges, this condition occurs due
221

Umar Zein Acta Med Indones-Indones J Intern Med
to the immunological state, concurrent use of HAART, and pattern of endemic infections.6,7
Etiology of disorders of the skin and mucous membranes including various infections, Kaposi sarcoma, and miscellaneous conditions, occur throughout the course of HIV infection, affecting more than 90% of patients at some time.4 Of the various infections, fungal is the most common skin disorder in HIV infected adult and children In the United States,5,7 parasitic infections with cutaneous manifestations are not common in HIV-infected patients with the exception of scabies, which has a worldwide distribution.1
But in the tropical country such as Indonesia, skin infection due to worm called cutaneous larva migrant is still a common problem, and should considered in differential diagnosis of pruritic, erhytematous, serpigious lesion and could concurrent with fever.8,9
One research in West Java, Indonesia at 2008 showed that among 843 HIV patients, 14.4% had a skin complaint. The most common skin manifestations were drug eruptions, pruritic papular eruptions, seborrhoeic dermatitis, herpes, zoster, dermatophytosis, and bacterial skin infections.10
There is not enough data report on how often the cutaneus larva migrant in HIV infected person in tropical country. This could lead to unawareness and misdiagnosis of helminth infection in HIV infected persons.
Cutaneous larva migrant is a parasitic infection that caused by the larval stages of dog and cat hookworms (Ancylostoma spp.). Although other worms, such as Strongyloides and Gnathostoma spp, can also migrate through the skin.11,12
Among many causes of cutaneous larva migrant, Necator americanus are the most common hookworm that cause larva migrant in Indonesia followed by Ancylostoma duodenale13
and A. ceylanicum, A. caninum, A. Braziliense.14
Infection occurs by contact of skin with contaminated soil or beach sand. Eggs shed in the feces of infected hosts hatch in the soil and develop into third-stage larvae, which penetrate the skin and migrate through the epidermis. In humans, larvae are generally confined to the dermis and only rarely penetrate deeper. Deeper
penetration is thought to be species specific (such as A. caninum).12
Third-stage larvae results in cutaneous larva migrans, or “creeping eruption,” a self-limited dermatologic condition characterized by serpiginous burrows, 1 to 5 cm long. Created by third-stage larvae migrating in the epidermis, the burrows appear on the feet in 39 percent of cases, the buttocks in 18 percent, and sometimes followed by nausea, vomiting, pharyngeal irritation,cough, dyspnea, and hoarseness. Increased circulating levels of IgE occur in response to migrations of third-stage larvae in the lungs and intestines.14
Due to the clinical manifestation and his activity history (gardening) the patient was diagnosed cutaneous larva migrant, we could not find any egg worms or larva in the stool so that the etiology was unknown, but if the epidemiological data was took into consideration, we could pressumed that the skin lesion was caused by hookworm N americanus or A dudoenale.
The eosinophilia in the blood was sign of systemic infection and could be found in first month of infection,13 that is why the patient consumed systemic antihelminthic drug along with local therapy.
Albendazole, 400 mg once daily per oral, for 3 days, is considered the treatment of choice for systemic treatment. Ivermectin (200 µg/kg/day per oral, for 1–2 days) is effective but not approved by the Food and Drug Administration for this indication,11 other treatment options are mebendazole 100 mg twice daily for three days, tetrachloretilen 0.12ml/kg bodyweight single dose, pyrantel pamoat 10 mg/kg bodyweight single dose, and heksilresolsinol.13
To be noted, the worm are included in one of Tropical Neglected Diseases. These diseases are a subset of infectious diseases, including (1) vector-borne protozoa (such as Trypanosoma cruzi), bacteria (ocular serovars of Chlamydia trachomatis) and filarial worms(such as Onchocerca volvulus); (2) soil-transmitted helminthes (ascaris, hookworm) and (3) the two species of non-tuberculosis mycobacteria that produce Buruli ulcer and leprosy, for which the mechanisms of acquiring infection are not yet fully understood.2,15,16
222

Vol 45 • Number 3 • July 2013 An HIV positive man with single erythema skin lesion
Since 2004 there has been an increased recognition of the importance of NTDs as impediments to development. These diseases cause a diversity of clinical conditions throughout the tropics and responsible for the decrease in the individual health status.17
The World Health Organization (WHO) has promoted expand control of these diseases through an integrated approach of mass drug administration referred to as preventive chemotherapy via community based distribution systems and through schools.17 There was no guideline of preventive treatment for immunocompromised person in tropical country.
CONCLUSIONWe have reported a case of a HIV positive
man with cutaneus larva migrant that was treated successfully with albendazole, cetirizine, chlorethyl spray and betamethasone cream. Published literature showed that parasitic infection is less common in HIV and the most common parasitic infection in HIV is scabies. The cutaneous larva migrant is one of neglected tropical disease that might occur in adult with immunocompromised. Nowadays this neglected disease is discussed rarely and might not be found in developed country, but it is still a common disease in the tropical region.
REFERENCES1. Lopez FA, Sanders CV. Fever and rash in HIV infected
patient. Up to Date ver 19.1. 2. Yamey G, Hotez P. Neglected tropical diseases.
These diseases could be controlled or eliminated in our lifetimes if efforts are better coordinated. BMJ. 2007;335:269-70.
3. Atraide DD, Akpa MR, George IO. The pattern of skin disorders in a Nigerian tertiary hospital. J. Public Health Epidemiol. 2011;3(4):177-81.
4. Tschachler E, Paul R, Bergstresser PR, Stingl G. HIV-related skin diseases. Lancet. 1996;348(9028):659-63.
5. Stefanaki Ch, Stratigos AJ. Skin manifestations of HIV-1 infection in children. Clin Dermatol Y. 2002;20:74–86.
6. Serling SLC, Leslie K, Maurer T. Approach to pruritus in the adult HIV-positive patient. Cutaneous Med Surg. 2011;30(2):101–6.
7. Ho KM, Wong KH. Dermatologic manifestations in HIV disease. In: Chan KCW, Wong KH, Lee SS, eds. HIV Manual; 2001. p. 231-45.
8. O’quinn JC, Dushin R. Cutaneous larva migrans :case report with current recommendations for treatment. J Am Podiatr Med Assoc. 2005;95(3):291–4.
9. Persico VS. HIV, cutaneous larva migrans and fever. Int J STD AIDS. 2007;18(6):433-4.
10. Dwiyana RF, Rowawi R, Lestari M, et al. Skin disorders in HIV infected patients from West Java. Acta med Indones. 2009;41 Suppl 1:18-22.
11. Singh S. Human strongyloidiasis in AIDS era: its zoonotic importance. J Assoc Physicians India. 2002;50:415-22.
12. Montgomery S. Cutaneous larva migrans. Downloaded at December 31, 2011. Available online from http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-3-infectious-diseases-related-to-travel/cutaneous-larva-migrans.htm.
13. Pohan HT. Penyakit cacing yang ditularkan melalui tanah. In: Sudoyo AW, Setiyohadi B, Setiati S, Alwi I, Simadibrata M, eds. Buku ajar ilmu penyakit dalam. 3rd volume. 4th edition. Jakarta: Pusat Penerbitan Ilmu Penyakit Dalam FKUI/RSCM; 2006.p. 1786-8.
14. Hotez PJ. Brooker S, Bethony JM, Bottazzi ME, Loukas A, Xiao S. Hookworm infection. N Engl J Med. 2004;351:799-807.
15. Feasey N, Wansbrough-Jones M, Mabey DCW, Solomon AW. Neglected tropical diseases. British Med Bulletin. 2010;93:179–200.
16. Hotez PJ, Molyneux DH, Fenwick A, Kumaresan J, Sachs SE, Sachs JD, Savioli L. Control of neglected tropical diseases. N Engl J Med. 2007;357:1018-27.
17. Molyneux HD, Malecela MN. Neglected tropical diseases and the millennium development goals-why the “other diseases” matter: reality versus rhetoric. Parasites & Vectors. 2011;4:234-47.
223