how to talk so your patients will listen
TRANSCRIPT
HOW TO TALK SO YOUR PATIENTS WILL LISTEN
Lunch & LearnApril 16, 2013
Simplify My Meds
• Adherence can be improved when patients coordinate refills (“refill synchronization”) at a single pharmacy
• Facilitates improved adherence• Improves pharmacy operations
Medication Synchronization Revenue Calculatorwww.ncpanet.org/revenuecalculator
NCPA Program Support
• Program Materials– Pharmacy Operations Manual– Customizable Program Forms– Physician Outreach Tools
• Marketing Materials– FREE Starter Kit
• Training and Support– Tutorials – Lunch & Learns
Learn More
• For More Information– www.ncpanet.org/adherence – [email protected]
• Online Tutorial– www.ncpanet.org/SMMtutorial/smmtutorial.html
HOW TO TALK SO YOUR PATIENTS WILL LISTEN
Jerry Meece, RPH, FACA, CDEPlaza Pharmacy and Wellness Center
What Has Been Your Experience With Trying to Facilitate Behavior
Change in Your Patients?
Chronic Care Coaching
• Asthma
• Diabetes
• CV disease
• Obesity
• COPD

Adherence to What?
Physical Activity
Nutrition
Medication
Monitoring
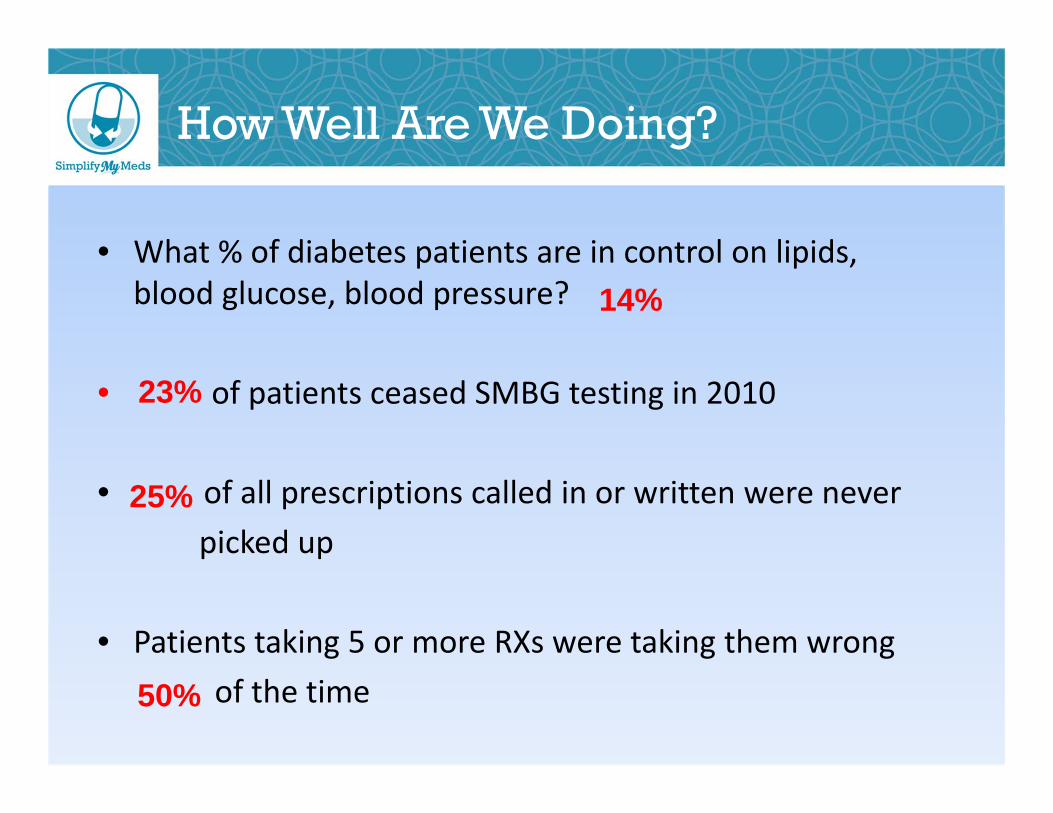
• What % of diabetes patients are in control on lipids, blood glucose, blood pressure?
• of patients ceased SMBG testing in 2010
• of all prescriptions called in or written were never picked up
• Patients taking 5 or more RXs were taking them wrongof the time
How Well Are We Doing?
14%
23%
25%
50%

Chronic Disease Adherence Rates in US
51%Adherence to Treatment for Hypertension in US
“In developed countries, adherence to medications among patients suffering chronic diseases averages only 50 percent.”
– World Health Organization 2003Adherence to Long‐Term Therapies: Evidence for Action
Sources: Adherence to Long-Term Therapies: Evidence for action. World Health Organization 2003. Available at: http://www.who.int/chronic_conditions/adherencereport/en/.
.
Why Is This Issue Important To Pharmacists and Health Care?
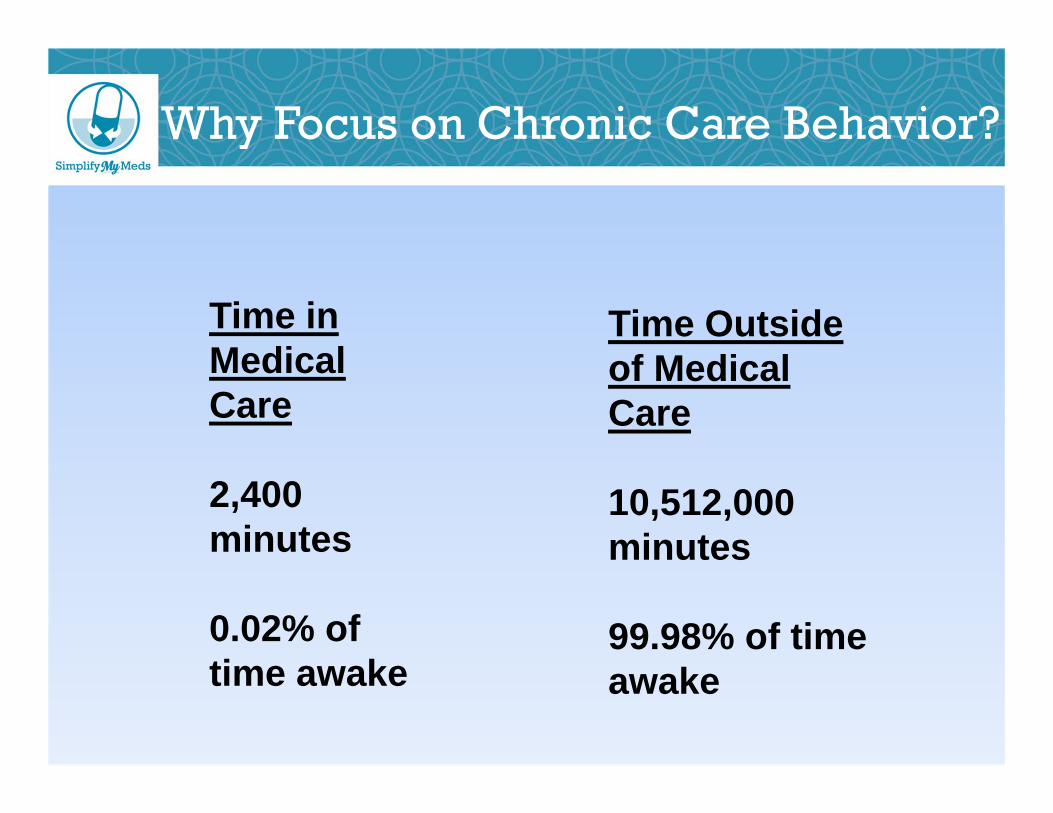
Time in Medical Care
2,400 minutes
0.02% of time awake
Time Outside of Medical Care
10,512,000 minutes
99.98% of time awake
Why Focus on Chronic Care Behavior?
Source: Adherence to Long-Term Therapies: Evidence for action. World Health Organization 2003.
U.S. Annual Costs of Poor Adherence
• $75 billion – $100 billion
• 125,000 deaths
• 10% – 25% of hospital and nursing home admissions
Why Aren’t We Doing Better?
What’s the Difference?
• Compliance: The extent to which a patient follows medical instructions. (How well you do and follow what I say)
• Adherence: The extent to which a person’s behavior corresponds with agreed recommendations from a health care provider. (How well you apply a plan that we agreed upon)
• Persistence: Adherence to the plan over time
Reasons for Poor Adherence
• Poor Patient Provider Communication– 21% completely disagree on decisions made and course of action
• No plan for implementing recommendations
• Poor understanding of the plan
• Enthusiasm (or lack of) of execution by the HCP
Parkin and Skinner, 2003
Sources: Adherence to Long‐Term Therapies: Evidence for action. World Health Organization 2003. Available at: http://www.who.int/chronic conditions/adherence report
For a Patient to be Adherent
• Must fully understand and comprehend the plan
• Be in full agreement with the course of action
• Be committed to the execution and what is increasingly a multi‐step solution
• Have follow‐up provided as changes occur
• Diabetes • Obesity• Hypertension• Hyperlipidemia• Medications• Inactive lifestyle• Financial Issues• Beliefs about ability to change
• Keeping records• Keeping appointments• Changes at home• Diet• Exercise• Glucose monitoring• Environment• Culture• Confidence/Ability
Paralysis By Ambivalence
Typical Health Care Encounter
“The pill for your lipids is to be taken at bedtime”
“Walk 30-45 minutes 5 days a week”
“Watch your salt intake”
“Check your blood sugar 4 times a daybefore a meal and 2 hours after but rotate times”
“You need to lose 25 pounds”“Take your diabetes meds am and pm after meals, except the capsule, take it at bedtime”
“If this doesn’t improve we’ll have to start insulin”
“Don’t eat anything white”
“We’ve got to get that A1C down”
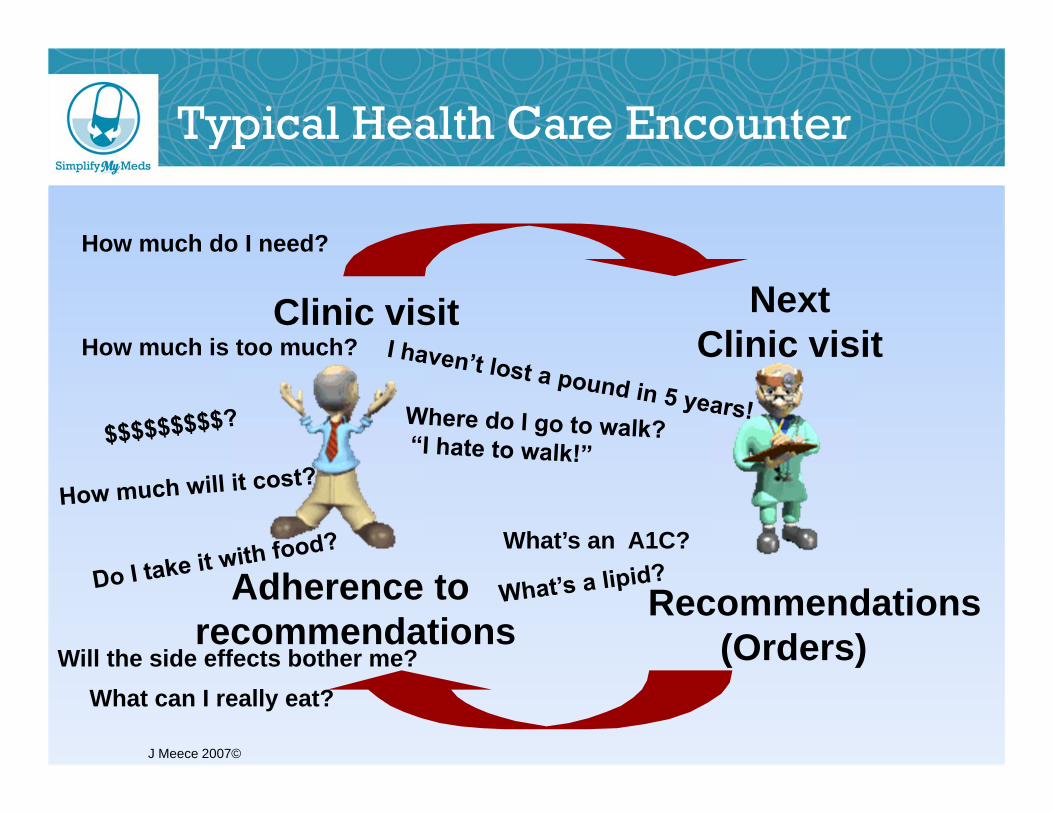
Typical Health Care Encounter
Clinic visit NextClinic visit
Recommendations(Orders)
Adherence to recommendations
J Meece 2007©
Will the side effects bother me?
How much do I need?
How much is too much?
What’s an A1C?
What can I really eat?
But…
Happens!
Do diabetes patients tell their doctors when they cut‐back on medication use due to cost?
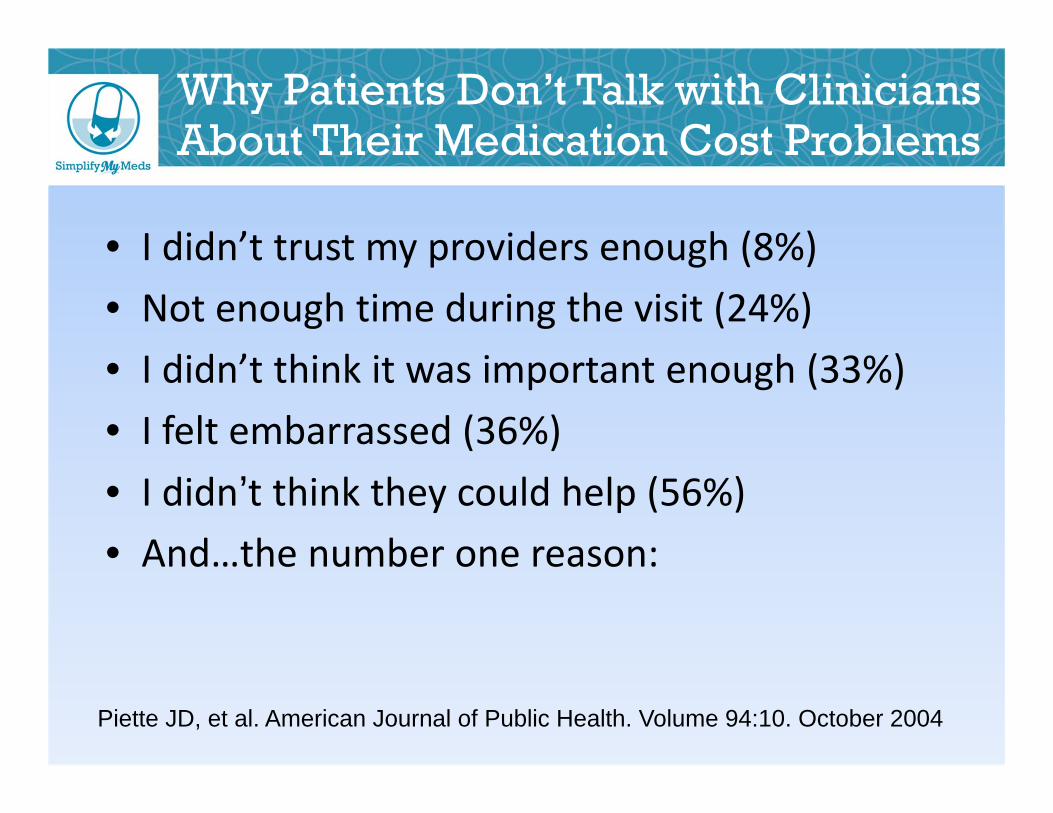
Why Patients Don’t Talk with Clinicians About Their Medication Cost Problems
• I didn’t trust my providers enough (8%)• Not enough time during the visit (24%)• I didn’t think it was important enough (33%)• I felt embarrassed (36%)• I didn’t think they could help (56%)• And…the number one reason:
Piette JD, et al. American Journal of Public Health. Volume 94:10. October 2004
Number 1 Reason?
“No one ever asked me.” (61%)
Piette JD, et al. American Journal of Public Health. Volume 94:10. October 2004
Solutions Aren’t Easy: What We Know
• No single strategy works for everyone
• Interventions must be tailored to the individual
Family Medicine Net Guide. Patient Adherence Explained. Available at: http://www.fmnetguide.com/vo2iss1/feature.html.
Com∙mu∙ni∙ca∙tion /kəˌmyo͞oniˈkāSHən/Noun:
The exchanging of information or news
Patients have most of their answers within them
It is our job to help them find them
Rollnick S, Miller WR, Butler CC. Motivational Interviewing in Health Care: Helping patients change behavior. The Guiford Press, New York, NY. 2008 pp. 3-10

Teen Daughters Lift 3,000-Pound Tractor Off Dad
Jesse Skoubo/Albany Democrat-Herald via AP Photo April 10th, 2013
Core Components of Motivational Interviewing (MI)
• Collaborative goal setting
• Open ended questions
• Reflective listening
• Empathy
Rosengren DB. Building Motivational Interviewing Skills: a practitioner workbook.The Guilford Press. New York, NY. 2009
Examples ‐‐ Discussion• Simple request ‐ “Tell me….”
• “What” and “How” questions are effective
• “Why” questions aren’t effective; provoke defenses
• If a person can answer in one word (yes, no, a number) the question was not open‐ended.
Open Ended Questions or Inquiry
Rosengren DB. Building Motivational Interviewing Skills: a practitioner workbook.The Guilford Press. New York, NY. 2009 p59
Two Biggest Clinician Fears:
• I’ll miss something if they don’t go for the facts right away
• The patient will ramble on forever
Reflective Listening
• Be present• Show you are trying to understand• Listen, listen, listen!• To be a mirror reflecting the speaker:
– repeat the words you have heard– short summaries– reflect meaning
• Non‐verbal: – Attentive, open, non‐judgmental
Rollnick S, Miller WR, Butler CC. Motivational Interviewing in Health Care: Helping patients change behavior. The Guiford Press, New York, NY. 2008 pp. 3-10
Examples of “stems”:• So, you are saying …. • It sounds like …..• You are wondering if....• I hear you saying….• You are…
Reflective Listening
Rosengren DB. Building Motivational Interviewing Skills: a practitioner workbook.The Guilford Press. New York, NY. 2009 p35
Empathy
• Goals– Seek to understand emotions, thoughts and values
– Patient experiences being seen, heard and understood
• Tasks– Attend to and reflect expressed thoughts, emotions, values
– Express a degree of understanding
Examples of Empathy
• “You seem pretty frustrated.”• “So, it’s really hard to …• “Most people I know would be distressed about …
• “I think I understand how you feel. Many of my colleagues also …
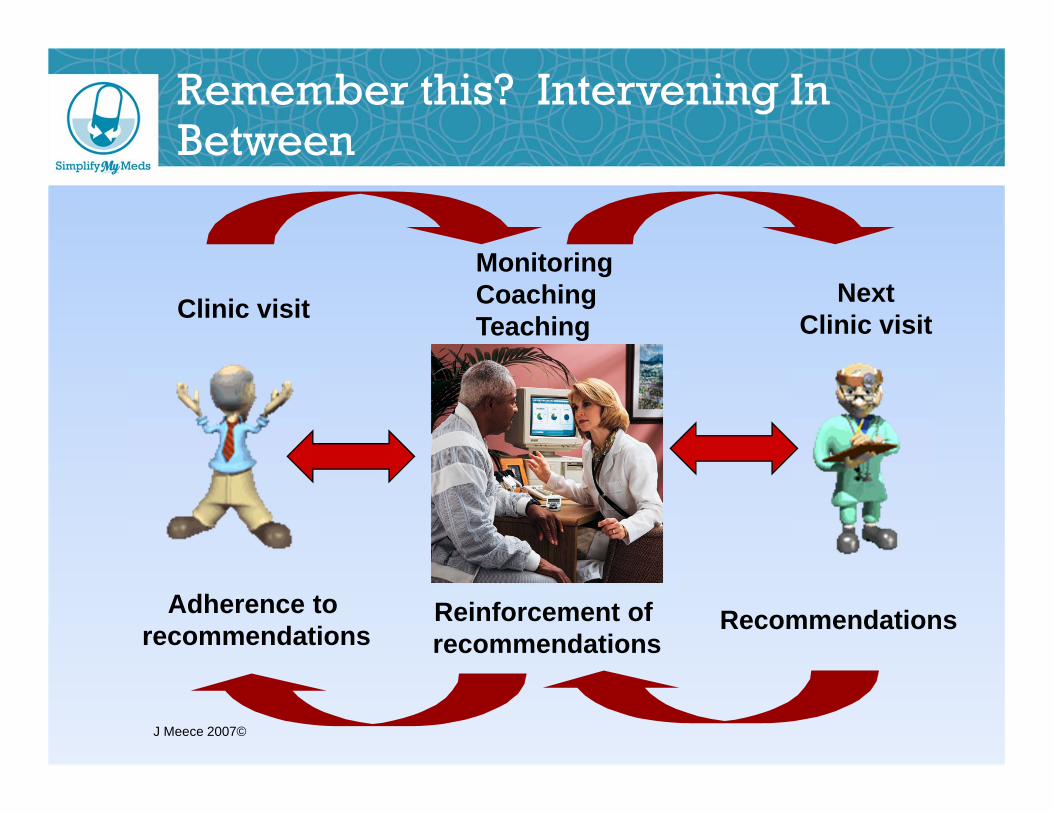
Remember this? Intervening In Between
Clinic visit NextClinic visit
RecommendationsAdherence to recommendations
Reinforcement of recommendations
MonitoringCoachingTeaching
J Meece 2007©
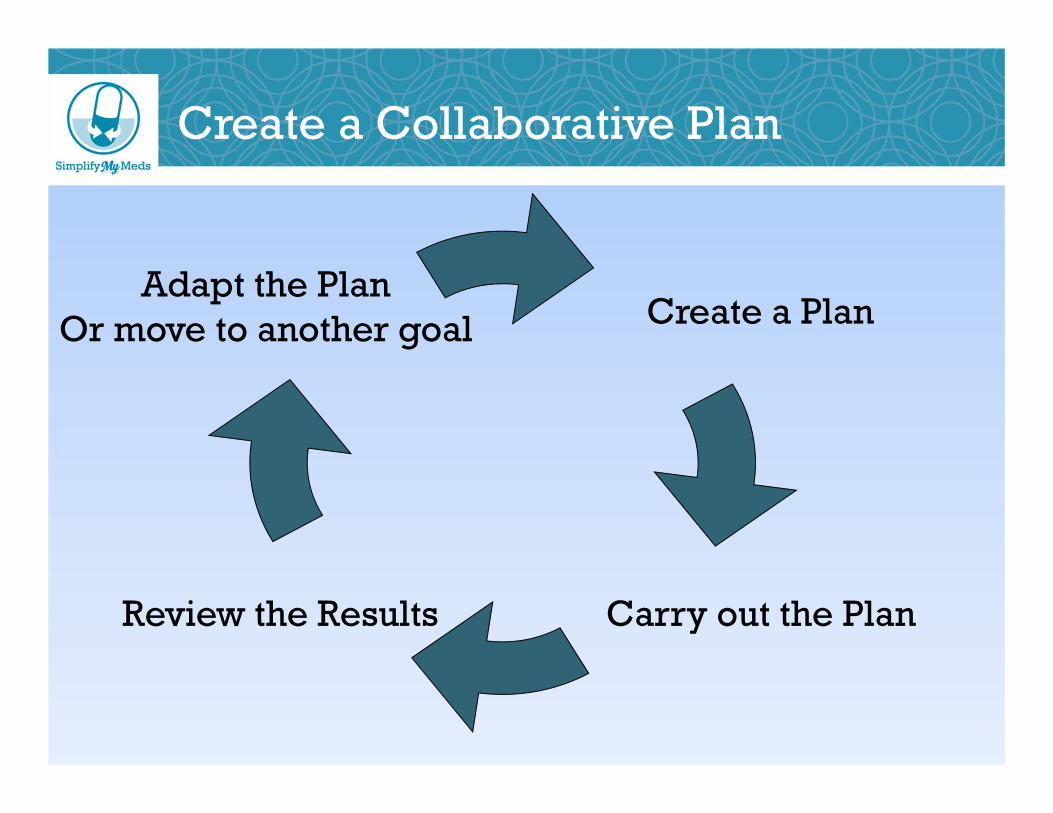
Create a Collaborative Plan
Create a Plan
Carry out the Plan
Adapt the PlanOr move to another goal
Review the Results
• Specific• Measurable• Attainable• Realistic• Timely
Setting Goals
TDI Education News Vol 2:1 January 2010
“The most important thing in communication is to hear what isn't being said. ”
‐‐‐‐Peter Drucker
How Do YOU Learn The Best?


The Star Spangled Banner

Star Spangled Banner -- Chords
sl hp sle-------------0-|-2/4-2--0--------|-----4--2-020----|-----0-0------|b-0--------0----|-----------------|--------------2/4|-2-4-----0----|g---1----1------|-----------1-3-4~|-4-4-------------|-----------1--|d-----2---------|-----------------|-----------------|-------------2|a---------------|-----------------|-----------------|--------------|e---------------|-----------------|-----------------|--------------|
sl trl trl trl trle-----------0-|-2/4-24242424-020202020-|-------------|------------------|b-0-------0---|------------------------|-------------|------------------|g---1---1-----|------------------------|-1-1/3/1/3/4-|-6-6-8^-6868-4646-|d-----2-------|------------------------|-------------|------------------|a-------------|------------------------|-------------|------------------|e-------------|------------------------|-------------|------------------|
hp sl e-----------------|-----0-0-------|b-0-0-7^~-7-575/4-|-2-4-----0-----|g-----------------|-----------1---|d-----------------|-------------2-|a-----------------|---------------|e-----------------|---------------|
hpp e---------------12^|-5-4-2-4-5-5------|-5-4--2420--0----|b-9-9-9-10-12-12---|------------------|------------4^-4~|g------------------|------------3--3-2|-----------------|d------------------|-------------2--2-|-----------------|a------------------|------------------|-----------------|e------------------|------------------|-----------------|
e--------------16|-----16------16-----16~|-----0-0-0|b-------17---17--|---17------17-----17~--|-0-0-----4|g-16-16----16----|-16------16-----16~----|----------|d----------------|-----------------------|----------|a----------------|-----------------------|----------|e----------------|-----------------------|----------|
turbo-pickinge-----------------------22222222-44444444-55545-444|b-22222222-44444444-5555---------------------------|g--------------------------------------------------|d--------------------------------------------------|a--------------------------------------------------|e--------------------------------------------------|
hpp sl sl p SLe-2420~-----|--------------7\/-|-0-2-4-454/2~0~|-4-4/9/11|b-----4^~-4~|-0-0-5-5/7-7/9----|---------------|-4-4/9/11|g-----------|------------------|---------------|-5-5/10/12|d-----------|------------------|---------------|-6-6/11/13|a-----------|------------------|---------------|----------|e-----------|------------------|---------------|----------|
e-0~-------|e----------|
Tablature Jimmi Hendrix - Woodstock 1968 - Star Spangled Banner
Communication Strategies
• Explain things clearly in plain (non‐medical) language– “Blood pressure pill” instead of “antihypertensive”– “Take one pill right before breakfast and one pill right before dinner”
• Connect activities to things already in their daily routine
• Focus on key messages and repeat• Use a “teach back” technique to check understanding
– “To be sure I was clear can you show me how you would give your insulin”
• Use patient‐friendly educational materialshttp://www.sowegaahec.org/uploads/130_Handout.pdf?PHPSESSID=dbe331d55a0022384c15ac40f7de3dcf
Herndon E and Joyce L. Getting the Most from Language Interpreters Family Practice Management 2004 (June) p37
Problem Solving – A Five Step Process
• Step 1: Explore the Problem or Issue– What is the hardest thing about caring for your diabetes? Tell me more about that.
• Step 2: Clarify Feelings and Meaning– So how does that make you feel? OR– How do you feel about that?
Funnell MM, Anderson RM. Empowerment and Self-Management of Diabetes. Clinical Diabetes. 2004; 22(3); 123-127
Problem Solving – A Five Step Process
• Step 3: Develop a plan – Ask the patient– What would you like to do about this?– Where would you like to be with this problem 3 months from now?
– What are your options? What might get in the way?
– Who could help you? – What would happen if you do nothing?– Use the conviction and confidence ruler
Funnell MM, Anderson RM. Empowerment and Self-Management of Diabetes. Clinical Diabetes. 2004; 22(3); 123-127
Problem Solving – A Five Step Process
• Step 4: Commit to Action– What are some of the steps you could take?– When are you going to do it?– How will you know if you are successful?– What is the one thing you will do when you leave here today?
• Step 5: Evaluate the patient’s progress and continuously modify the planFunnell MM, Anderson RM. Empowerment and Self-Management of Diabetes. Clinical Diabetes. 2004; 22(3); 123-127
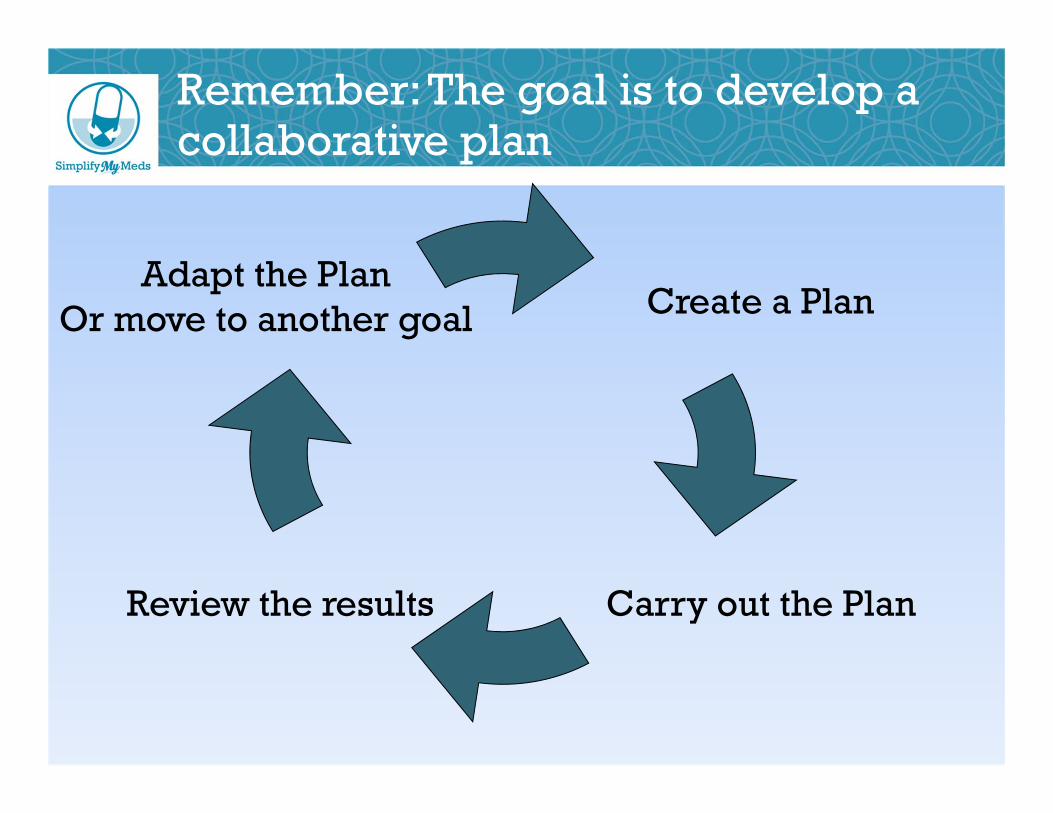
Remember: The goal is to develop a collaborative plan
Create a Plan
Carry out the Plan
Adapt the PlanOr move to another goal
Review the results
Take Home Messages
• Everyone wants to life a long happy life• Our patients are more confused than unmotivated
• Management of a chronic care disease is tough
• Our patients face many obstacles to self‐care and those obstacles change
• Good conversations lead to good outcomes
And If You Have Time To Ask Only One Question:
• “What do you find most challenging about managing your (insert chronic condition)?”
And listen