maurizio paciaroni stroke unit – university of … paciaroni has participated over the last 5...
TRANSCRIPT

Ictus ischemico ed emorragico
Maurizio Paciaroni Stroke Unit – University of Perugia

DISCLOSURES
Maurizio Paciaroni has participated over the last 5 years for the following speakers’ bureaus: - Aspen - Bayer - Boehringer Ingelheim - Bristol-Myers Squibb - Daiichi Sankyo - Medtronic - Pfizer - Sanofi Aventis

Secondary prevention of stroke
Non Cardioembolic stroke - Lacunar stroke - Cryptogenic stroke Antiplatelets, statins - Atherosclerotic stroke - Carotid atherosclerotic stroke Carotid revascularization
Cardioembolic stroke Anticoagulants*
* In patients with AF, indication also for primary prevention

Perugia Stroke Registry
• 2257 patients (Ischemic stroke – TIA – ICH)
- 506 atherosclerosis (22,4%) - 431 small vessels disease (19,1%) - 580 undetermined origin or
≥ 1 possible causes (25.7%) - 182 rare causes (8.1%)
- 558 Cardioembolic (24.7%) Cardioembolic Stroke: NVAF 428/558 (76.7%)
Paciaroni, Unpublished data
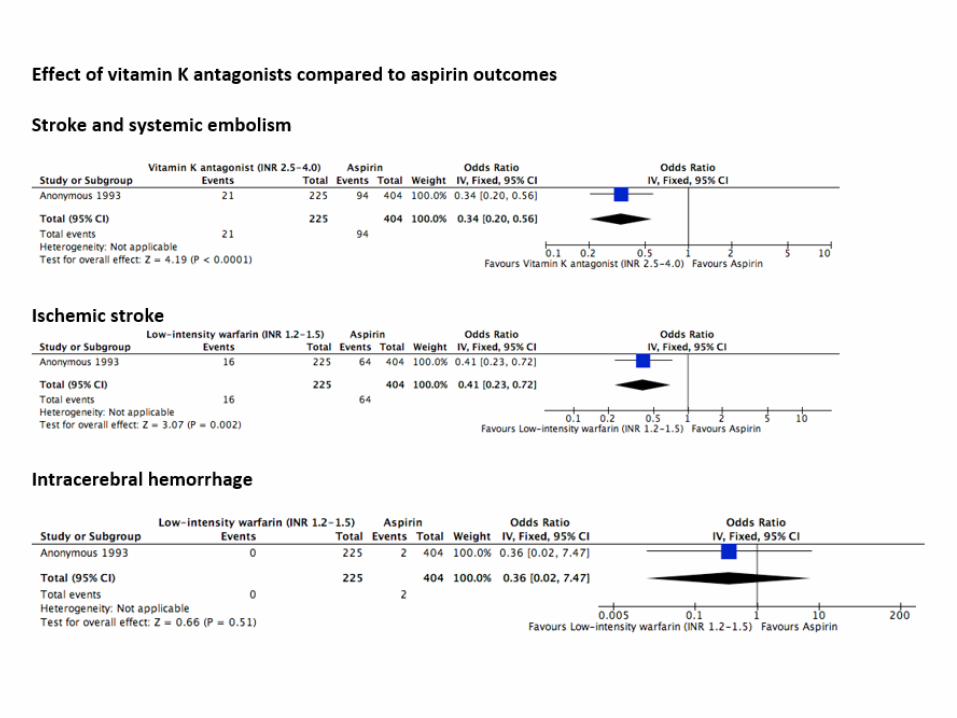

Storia di Stroke/TIA

DOACs in secondary stroke prevention Recurrent ischemic stroke
Intracranial bleeding
Ntaios et al, International Journal of Stroke 2017
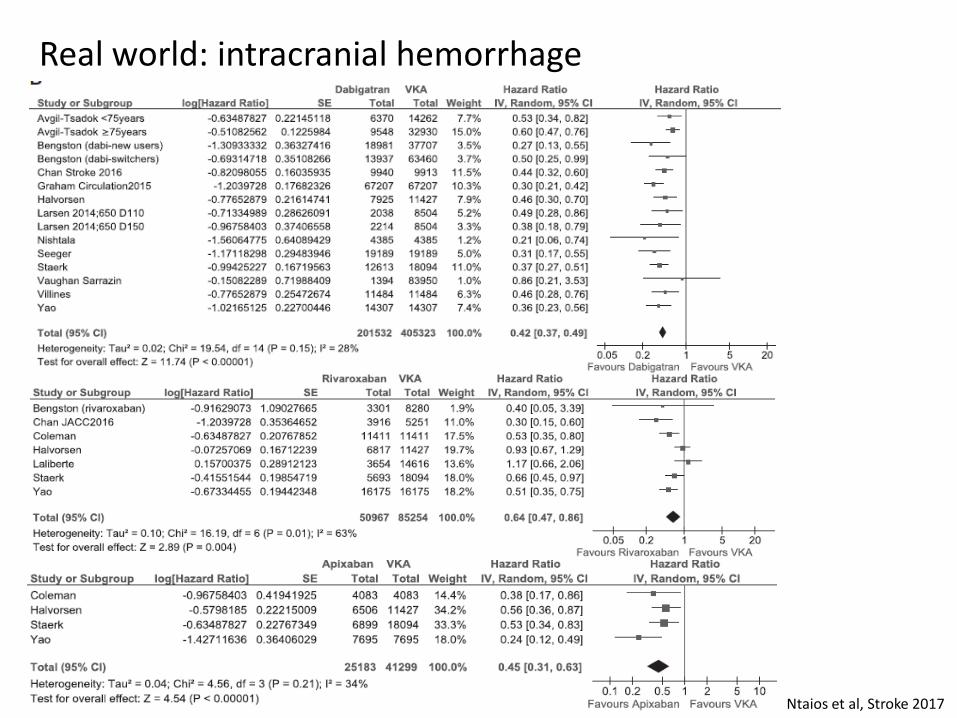
Real world: intracranial hemorrhage
Ntaios et al, Stroke 2017
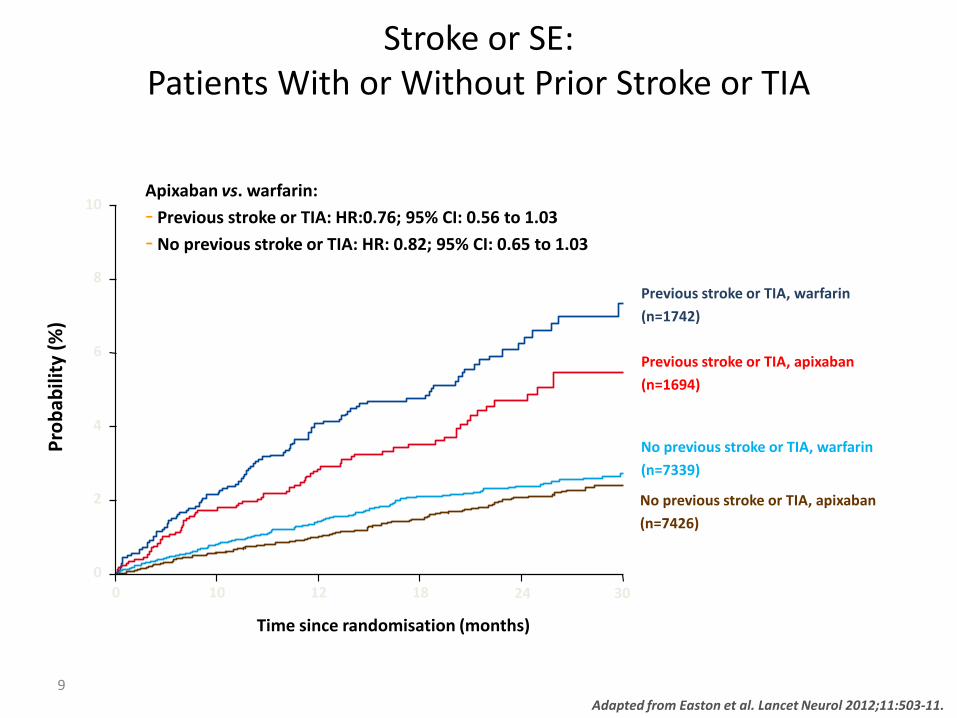
9 Adapted from Easton et al. Lancet Neurol 2012;11:503-11.
0
2
4
6
8
Prob
abili
ty (%
)
0 10 12 18 24 30
Time since randomisation (months)
10
Previous stroke or TIA, warfarin (n=1742)
Previous stroke or TIA, apixaban (n=1694)
No previous stroke or TIA, warfarin (n=7339)
No previous stroke or TIA, apixaban (n=7426)
Apixaban vs. warfarin: - Previous stroke or TIA: HR:0.76; 95% CI: 0.56 to 1.03 - No previous stroke or TIA: HR: 0.82; 95% CI: 0.65 to 1.03
Stroke or SE: Patients With or Without Prior Stroke or TIA
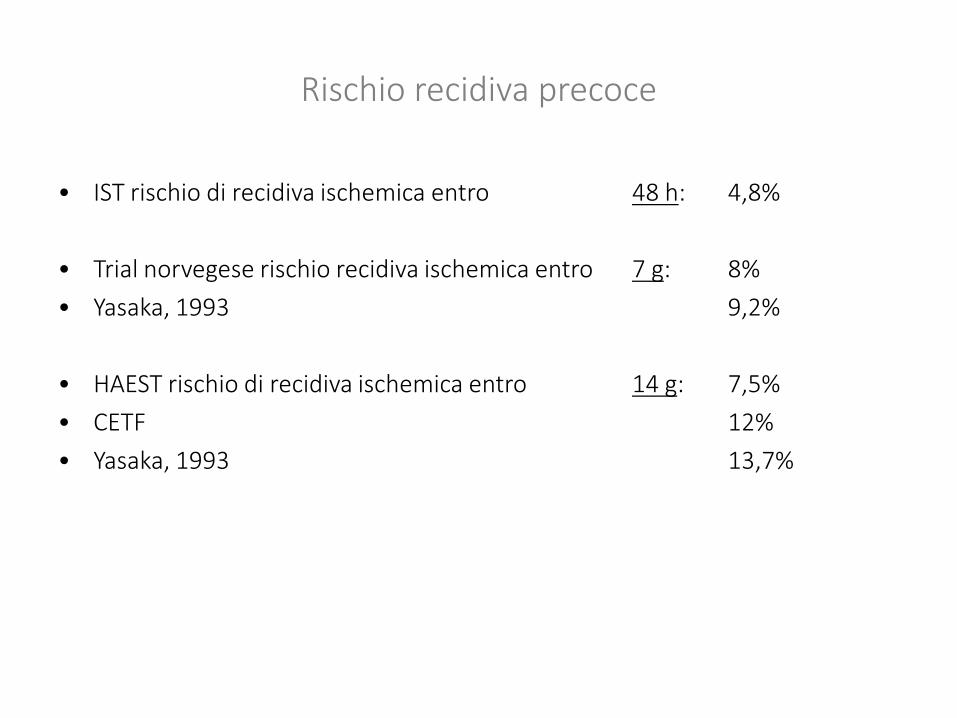
Rischio recidiva precoce
• IST rischio di recidiva ischemica entro 48 h: 4,8% • Trial norvegese rischio recidiva ischemica entro 7 g: 8% • Yasaka, 1993 9,2%
• HAEST rischio di recidiva ischemica entro 14 g: 7,5% • CETF 12% • Yasaka, 1993 13,7%
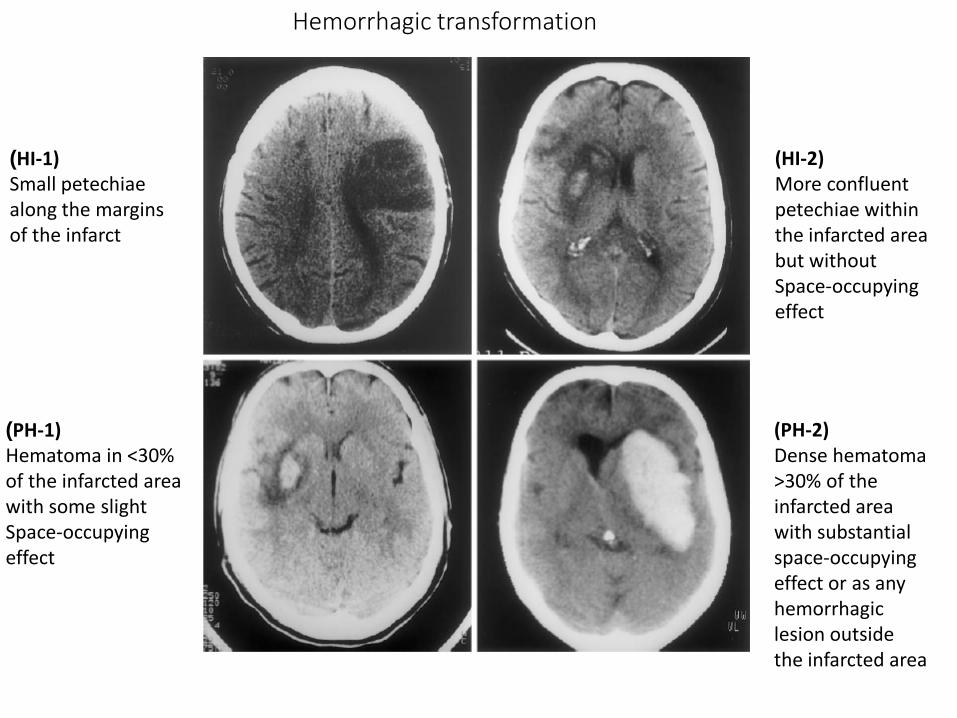
Hemorrhagic transformation
(HI-1) Small petechiae along the margins of the infarct
(HI-2) More confluent petechiae within the infarcted area but without Space-occupying effect
(PH-1) Hematoma in <30% of the infarcted area with some slight Space-occupying effect
(PH-2) Dense hematoma >30% of the infarcted area with substantial space-occupying effect or as any hemorrhagic lesion outside the infarcted area

Paciaroni et al, Stroke 2008

Combined outcome events
Paciaroni et al, Stroke 2015

Inizio della terapia
• ARISTOTLE: Patients with a previous intracranial haemorrhage (ICH) or any stroke within 7 days before random assignment were excluded.
• RE-LY: excluded patients with a stroke within 14 days or severe stroke within 6 months before screening
• ROCKET AF: excluded patients with a severe, disabling stroke within 3 months or any stroke within 14 days before randomization
• ENGAGE AF-TIMI 48: excluded patients with stroke within the previous 30 days
Easton JD et al. Lancet Neurol. 2012;11:503–511.
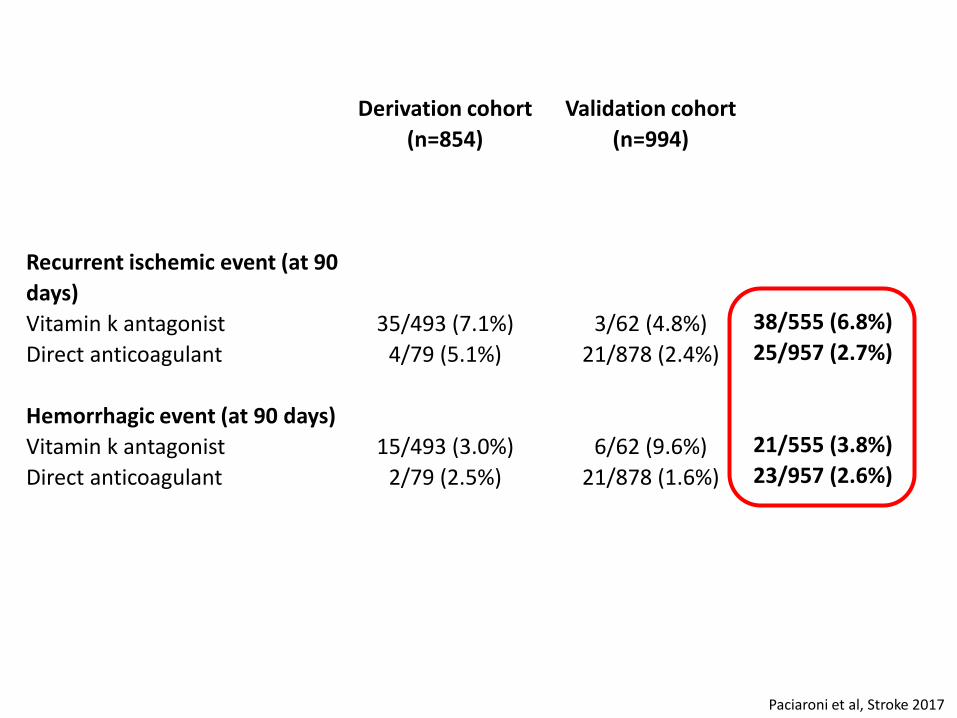
Derivation cohort (n=854)
Validation cohort (n=994)
Recurrent ischemic event (at 90 days)
Vitamin k antagonist 35/493 (7.1%) 3/62 (4.8%) Direct anticoagulant 4/79 (5.1%) 21/878 (2.4%) Hemorrhagic event (at 90 days) Vitamin k antagonist 15/493 (3.0%) 6/62 (9.6%) Direct anticoagulant 2/79 (2.5%) 21/878 (1.6%)
Paciaroni et al, Stroke 2017
38/555 (6.8%) 25/957 (2.7%)
21/555 (3.8%) 23/957 (2.6%)
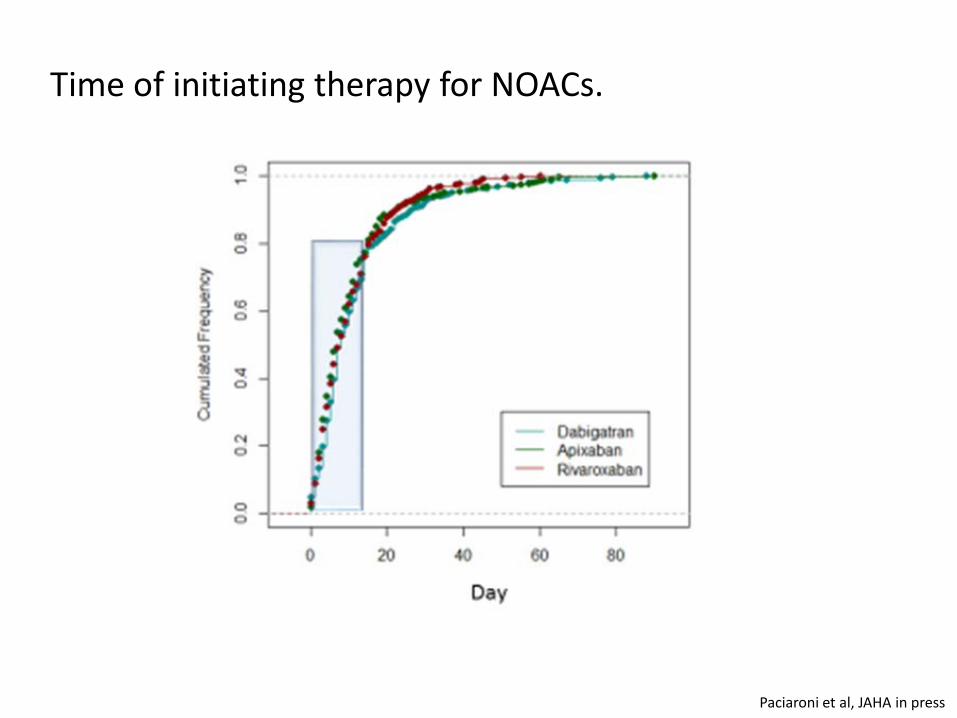
Time of initiating therapy for NOACs.
Paciaroni et al, JAHA in press

Risk of combined outcome events based upon the day of initiating NOAC
Outcome events (ischemic and hemorrhagic) depending on the time between onset and initiation of therapy with NOACs.
12.4% 2.1% 9.1%
Paciaroni et al, JAHA in press
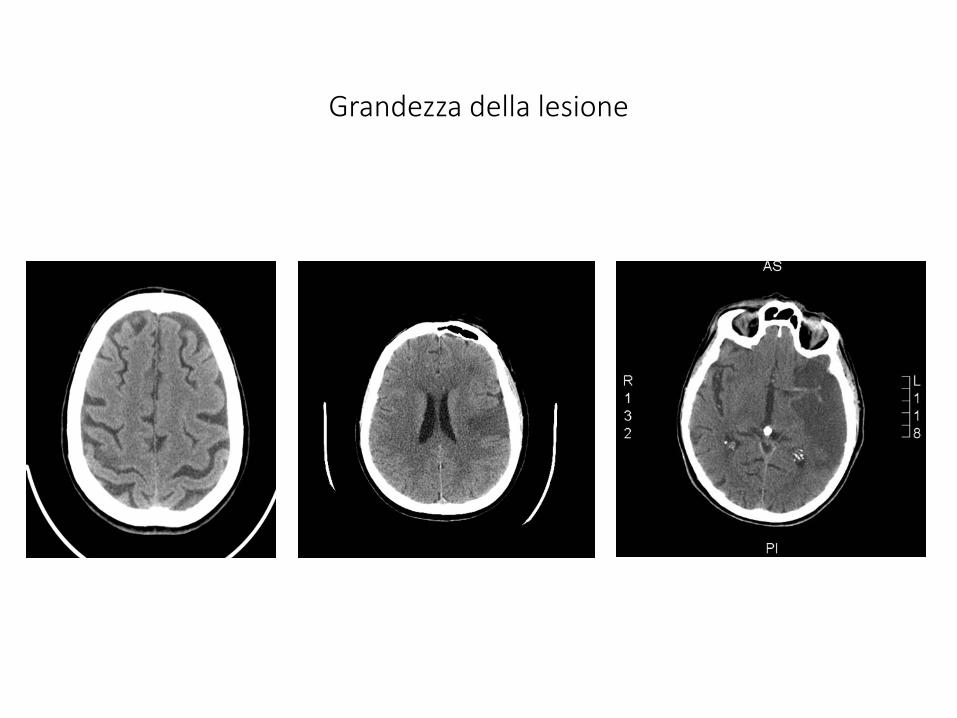
Grandezza della lesione
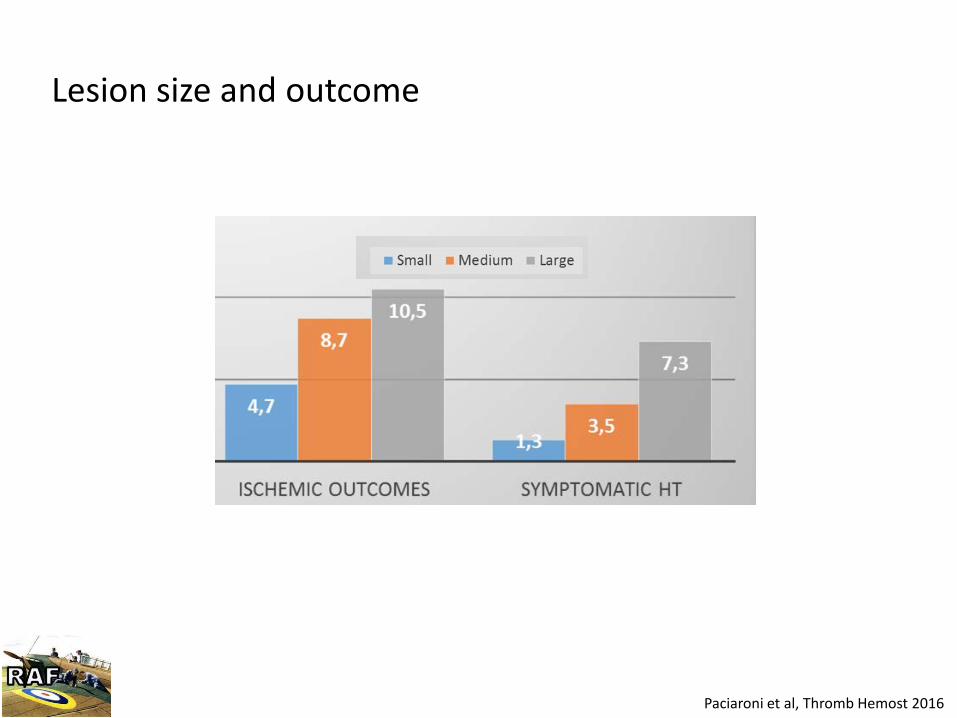
Lesion size and outcome
Paciaroni et al, Thromb Hemost 2016
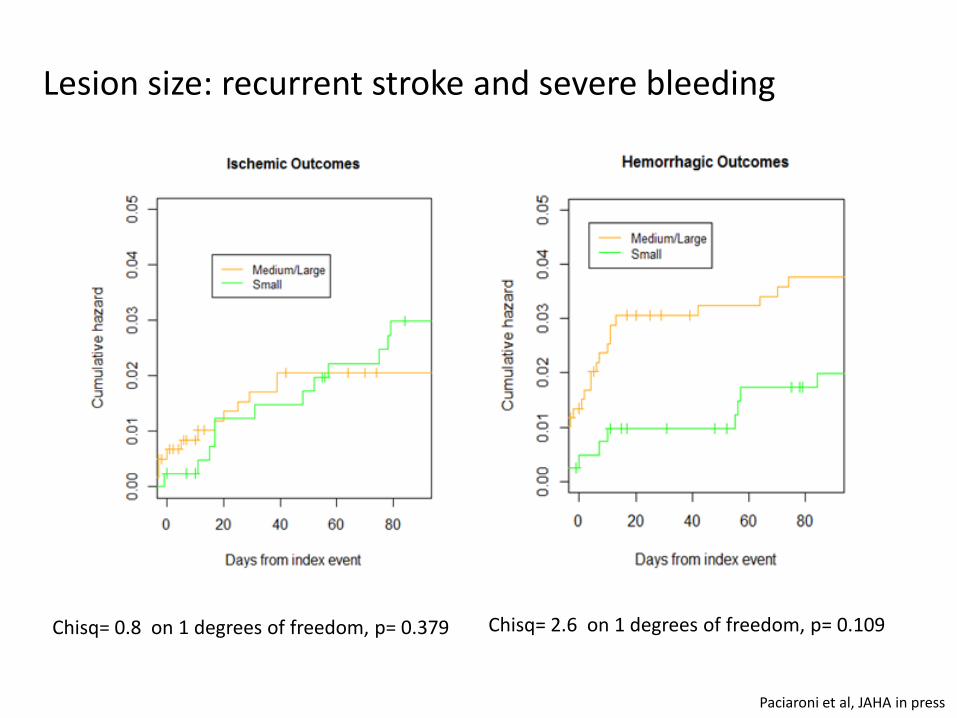
Chisq= 0.8 on 1 degrees of freedom, p= 0.379 Chisq= 2.6 on 1 degrees of freedom, p= 0.109
Lesion size: recurrent stroke and severe bleeding
Paciaroni et al, JAHA in press

Paciaroni et al, Thromb Hemost 2016
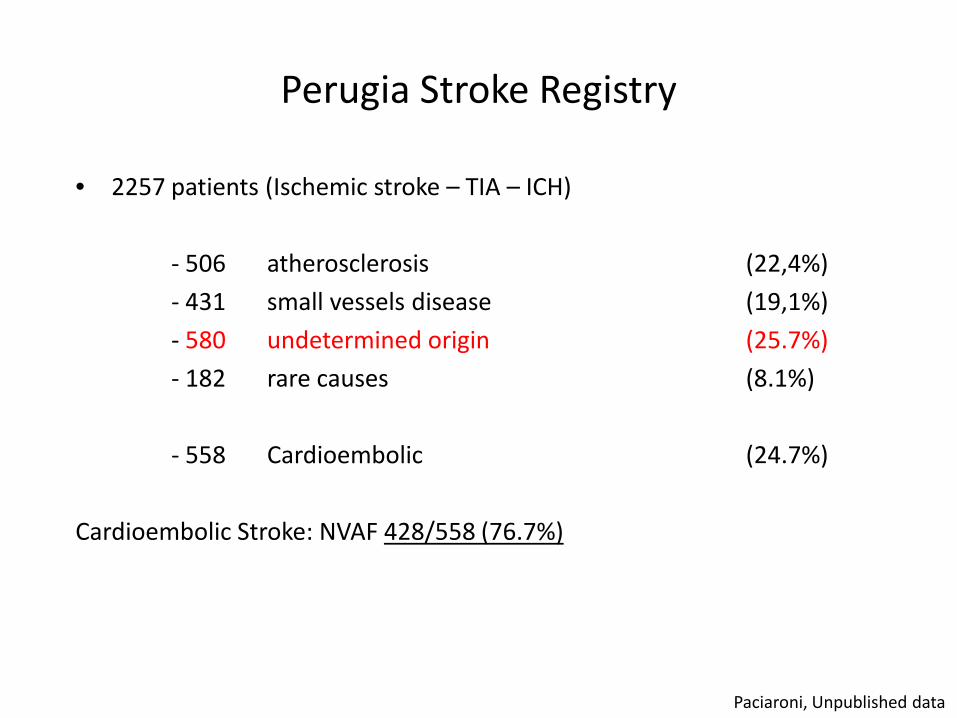
Perugia Stroke Registry
• 2257 patients (Ischemic stroke – TIA – ICH)
- 506 atherosclerosis (22,4%) - 431 small vessels disease (19,1%) - 580 undetermined origin (25.7%) - 182 rare causes (8.1%) - 558 Cardioembolic (24.7%) Cardioembolic Stroke: NVAF 428/558 (76.7%)
Paciaroni, Unpublished data
Ictus da causa indeterminata
• Non si possono effettuare tutti gli esami diagnostici: - severità dell’ictus (morte precoce)
- rifiuto del paziente
• Esami diagnostici effettuati in tempi impropri • Paziente con 2-3 cause potenziali • Tutti gli esami fatti ma tutti risultati negativi
Ictus da causa indeterminata
• Non si possono effettuare tutti gli esami diagnostici: - severità dell’ictus (morte precoce)
- rifiuto del paziente
• Esami diagnostici effettuati in tempi impropri • Paziente con 2-3 cause potenziali • Tutti gli esami fatti ma tutti risultati negativi

Fibrillazione atriale
• Parossistica • Persistente • Permanente
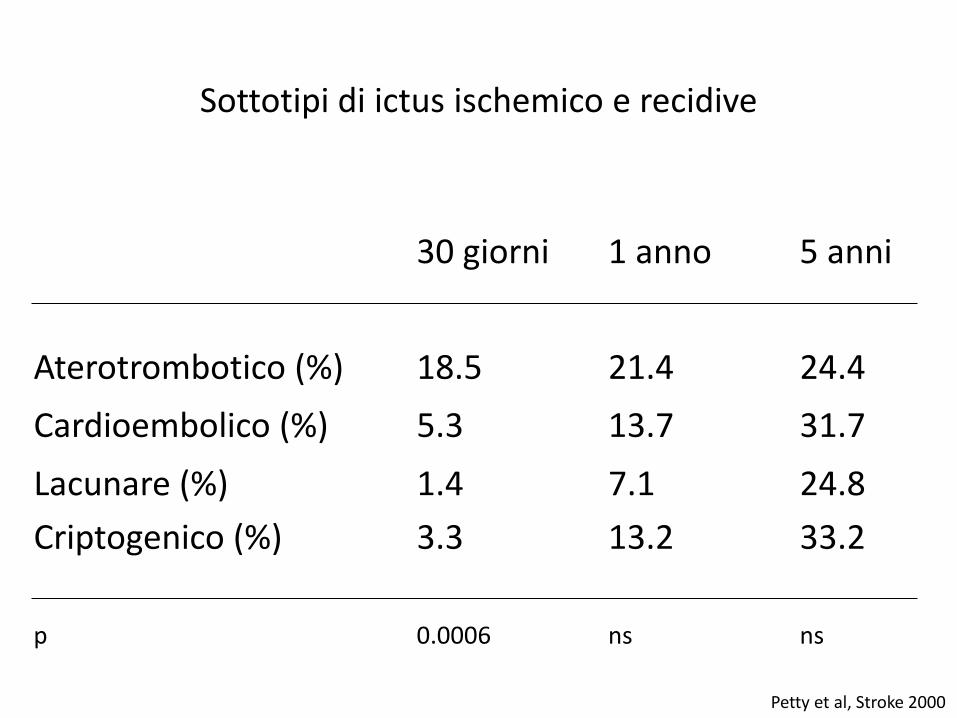
30 giorni 1 anno 5 anni
Aterotrombotico (%) 18.5 21.4 24.4 Cardioembolico (%) 5.3 13.7 31.7 Lacunare (%) 1.4 7.1 24.8 Criptogenico (%) 3.3 13.2 33.2 p 0.0006 ns ns
Sottotipi di ictus ischemico e recidive
Petty et al, Stroke 2000

Evoluzione degli strumenti per la registrazione ECG
Norman Holter Holter ECG 1950s Contemporary Holter ECG
Implantable recorders since 2000s
M

Sanna et al, 2014 N Engl J Med
Apr 2012
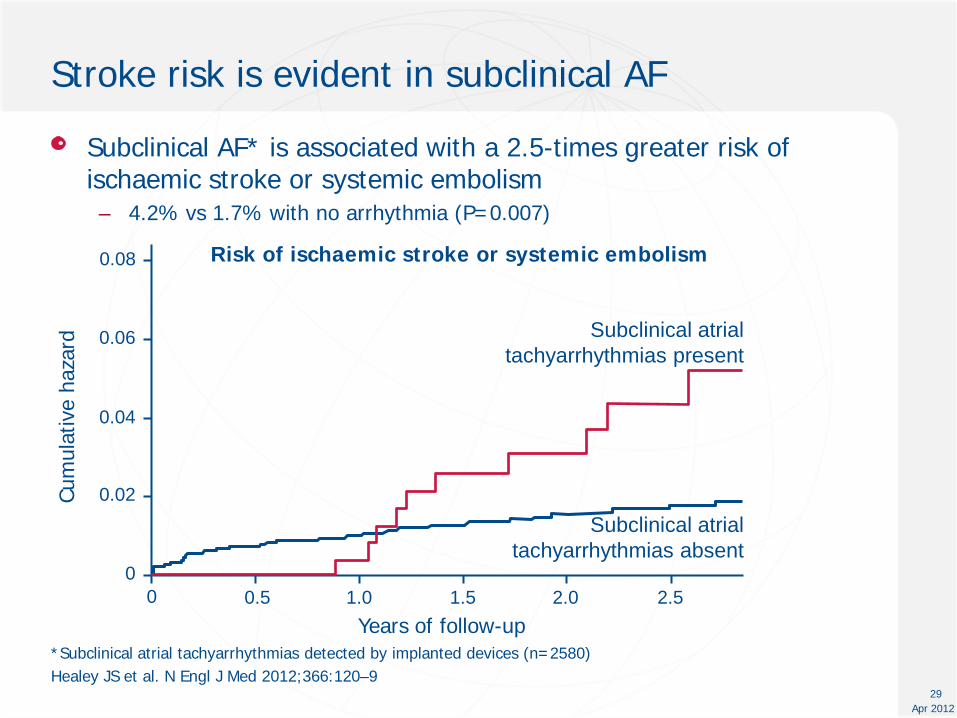
Stroke risk is evident in subclinical AF
Subclinical AF* is associated with a 2.5-times greater risk of ischaemic stroke or systemic embolism – 4.2% vs 1.7% with no arrhythmia (P=0.007)
*Subclinical atrial tachyarrhythmias detected by implanted devices (n=2580) Healey JS et al. N Engl J Med 2012;366:120–9
29
Risk of ischaemic stroke or systemic embolism
Years of follow-up
0.06
0.08
0 0.5 1.0
Cum
ulat
ive
haza
rd
0.04
0.02
0 1.5 2.0 2.5
Subclinical atrial tachyarrhythmias absent
Subclinical atrial tachyarrhythmias present
Cliniche
• Riduzione dello stato di coscienza all’inizio dei sintomi
• Rapida regressione dei sintomi (shrinking syndrome)
• Improvvisa comparsa del massimo deficit (<5 min.)
• Disturbi visivi campimetrici, neglect o afasia
• Embolia in distretti extracerebrali
• Palpitazioni all’onset.
Caratteristiche suggestive di stroke cardioembolico

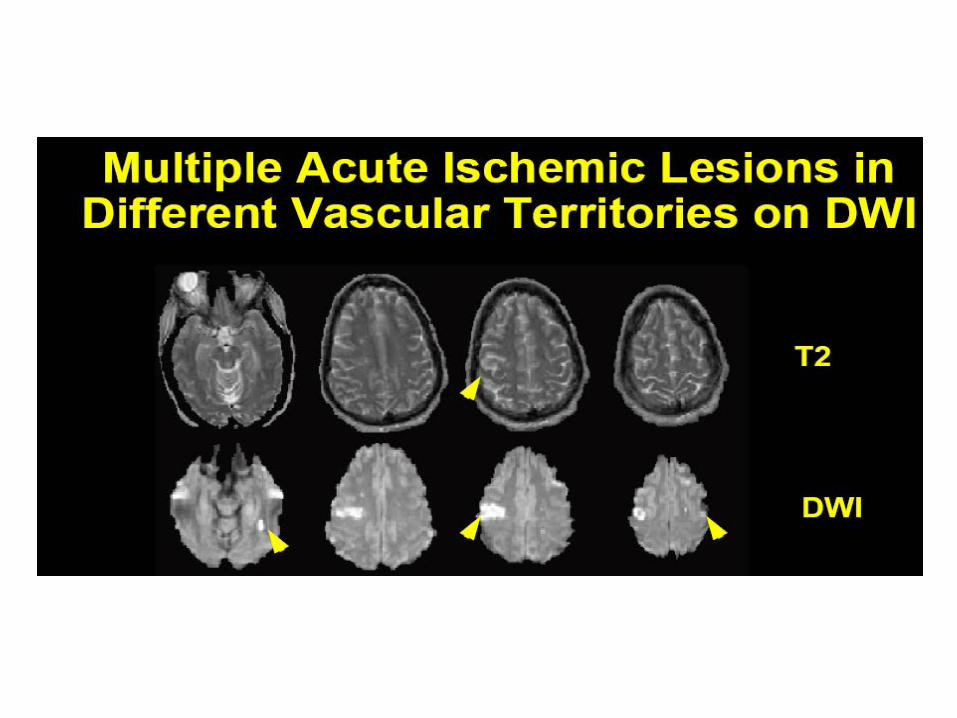

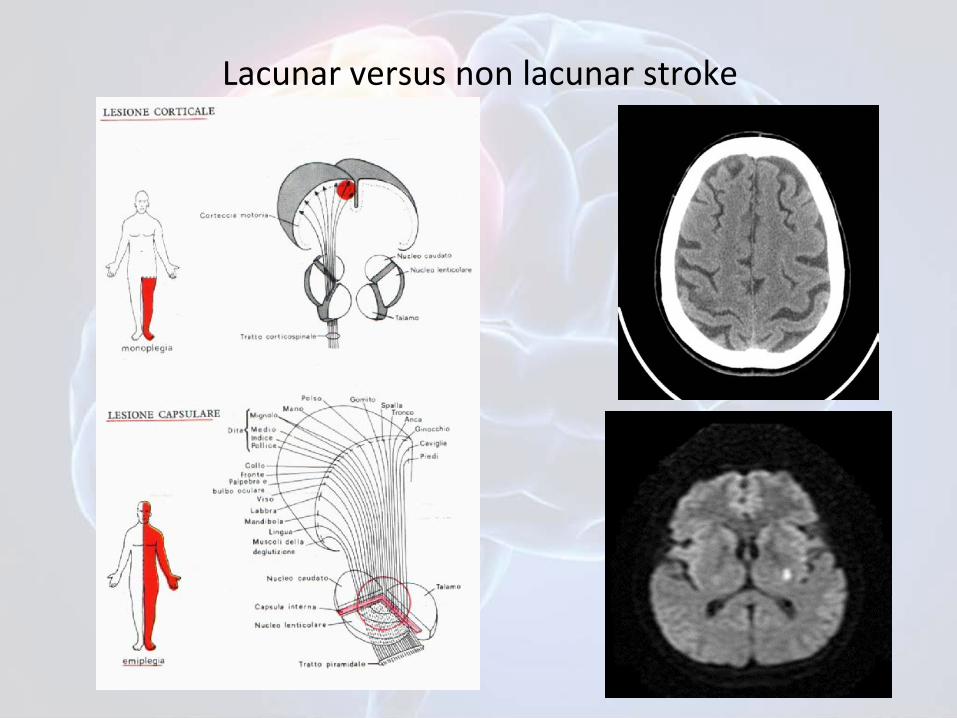
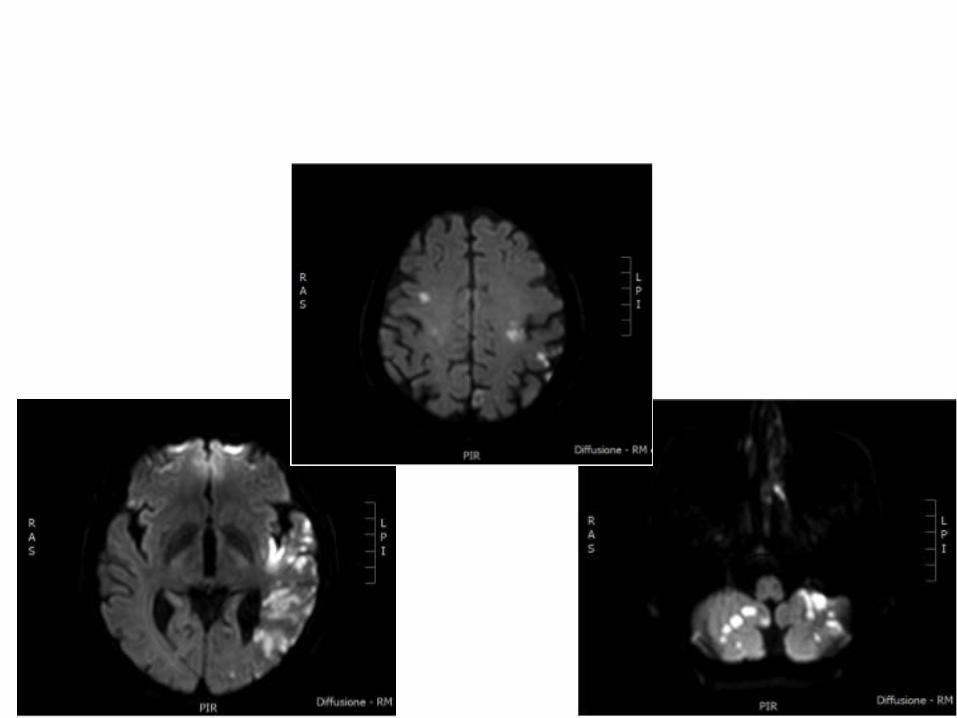
Lacunar versus non lacunar stroke

arteria perforante: ictus lacunare

Sanna et al, 2014 N Engl J Med
Ictus da causa indeterminata
• Non si possono effettuare tutti gli esami diagnostici: - severità dell’ictus (morte precoce)
- rifiuto del paziente
• Esami diagnostici effettuati in tempi impropri • Paziente con 2-3 cause potenziali • Tutti gli esami fatti ma tutti risultati negativi
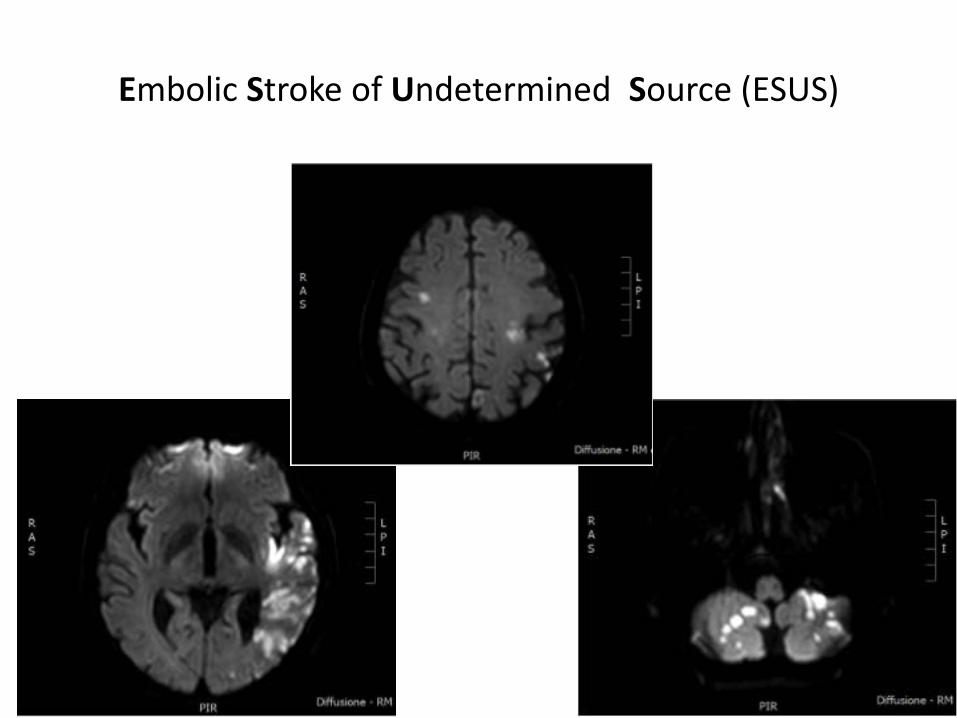
Embolic Stroke of Undetermined Source (ESUS)
1. Hart et al. Lancet Neurol. 2014;13:429–438.
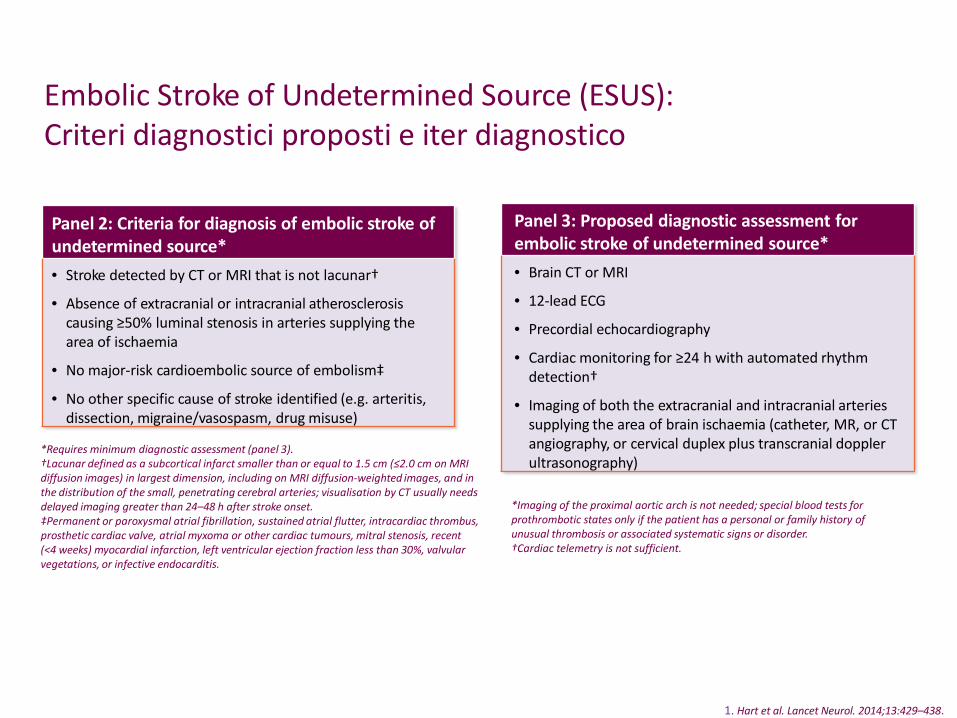
Embolic Stroke of Undetermined Source (ESUS): Criteri diagnostici proposti e iter diagnostico
Panel 2: Criteria for diagnosis of embolic stroke of undetermined source* • Stroke detected by CT or MRI that is not lacunar†
• Absence of extracranial or intracranial atherosclerosis causing ≥50% luminal stenosis in arteries supplying the area of ischaemia
• No major-risk cardioembolic source of embolism‡
• No other specific cause of stroke identified (e.g. arteritis, dissection, migraine/vasospasm, drug misuse)
*Requires minimum diagnostic assessment (panel 3). †Lacunar defined as a subcortical infarct smaller than or equal to 1.5 cm (≤2.0 cm on MRI diffusion images) in largest dimension, including on MRI diffusion-weighted images, and in the distribution of the small, penetrating cerebral arteries; visualisation by CT usually needs delayed imaging greater than 24–48 h after stroke onset. ‡Permanent or paroxysmal atrial fibrillation, sustained atrial flutter, intracardiac thrombus, prosthetic cardiac valve, atrial myxoma or other cardiac tumours, mitral stenosis, recent (<4 weeks) myocardial infarction, left ventricular ejection fraction less than 30%, valvular vegetations, or infective endocarditis.
Panel 3: Proposed diagnostic assessment for embolic stroke of undetermined source* • Brain CT or MRI
• 12-lead ECG
• Precordial echocardiography
• Cardiac monitoring for ≥24 h with automated rhythm detection†
• Imaging of both the extracranial and intracranial arteries supplying the area of brain ischaemia (catheter, MR, or CT angiography, or cervical duplex plus transcranial doppler ultrasonography)
*Imaging of the proximal aortic arch is not needed; special blood tests for prothrombotic states only if the patient has a personal or family history of unusual thrombosis or associated systematic signs or disorder. †Cardiac telemetry is not sufficient.
Management of cryptogenic stroke ESUS
• Patient education • Risk factors control • Anti-hypertensives • Statins • Antiplatelet drugs

Management of cryptogenic stroke ESUS
• Patient education • Risk factors control • Anti-hypertensives • Statins • Antiplatelet drugs • Randomized studies

NAVIGATE-ESUS: trial design 475 sites in 31 Countries
Study number NCT02227550. Details available from www.ClinicialTrials.gov .
1 month post study
drug observation
period
Prospective, randomised, double blind, active-comparator, event-driven, superiority, phase III trial
R
Rivaroxaban 15 mg OD n = 3.500
ASA 100 mg OD n = 3.500
Patients with recent ischemic stroke and: 1. visualized by brain CT or MRI
that is not lacunar 2. absence of cervical carotid
atherosclerotic artery stenosis ≥ 50% or occlusion
3. no AF after ≥ 24 hrs cardiac rhythm monitoring
4. no intra-cardiac thrombus on transthoracic on echocardiography
5. no other specific etiology for cause of stroke (eg. arteritis, dissection, migraine/vasospasm, drug abuse
Age ≥ 18 years (max 10% patients < 60 years
Randomization 7 days to 6 months after acute ESUS Day 1
Randomization Efficacy
Cut off date
30 ± 7 days EOS
- Target RRR 30%; superiority; 90% power α=0.05 - Enrollment 24 months; minimum treatment 12 months; study duration 36 months - Estimated mean treatment duration 18-24 months
N = 7.000
Two substudies: MRI substudy assessing covert strokes Biomarker/genetics substudy to identify biomarkers linked
with ESUS, recurrent stroke and treatment response
Expected timelines: Recruitment started Dec 2014 Topline result Q1 2018

To evaluate the efficacy and safety of Dabigatran for secondary stroke prevention in patients with an embolic stroke of undetermined source (ESUS) • 6,000 patients who had an ESUS within six months prior to enrollment • ASA 100 mg vs Dabigatran 150 mg BID or 110 mg BID for pts older than 75 or who have reduced renal function
Clinicaltrials.gov
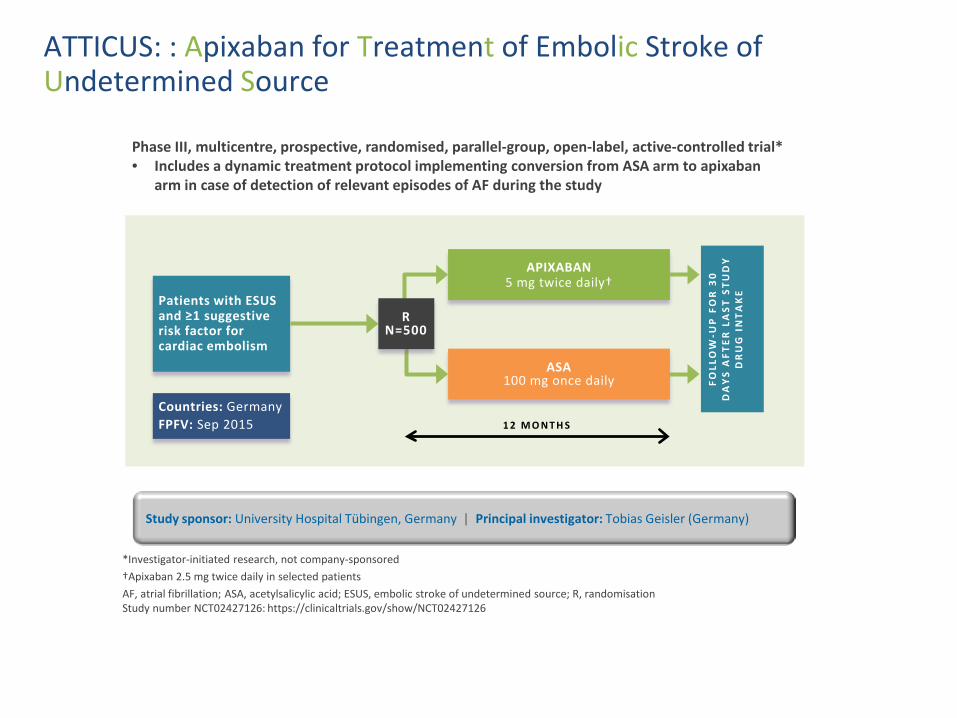
ATTICUS: : Apixaban for Treatment of Embolic Stroke of Undetermined Source
Phase III, multicentre, prospective, randomised, parallel-group, open-label, active-controlled trial* • Includes a dynamic treatment protocol implementing conversion from ASA arm to apixaban
arm in case of detection of relevant episodes of AF during the study
Study sponsor: University Hospital Tübingen, Germany | Principal investigator: Tobias Geisler (Germany)
*Investigator-initiated research, not company-sponsored †Apixaban 2.5 mg twice daily in selected patients AF, atrial fibrillation; ASA, acetylsalicylic acid; ESUS, embolic stroke of undetermined source; R, randomisation Study number NCT02427126: https://clinicaltrials.gov/show/NCT02427126
Patients with ESUS and ≥1 suggestive risk factor for cardiac embolism
APIXABAN 5 mg twice daily†
ASA 100 mg once daily FO
LLO
W-U
P F
OR
30
D
AY
S A
FTER
LA
ST S
TUD
Y
DR
UG
IN
TAK
E
1 2 M O N T H S
Countries: Germany FPFV: Sep 2015
R N=500
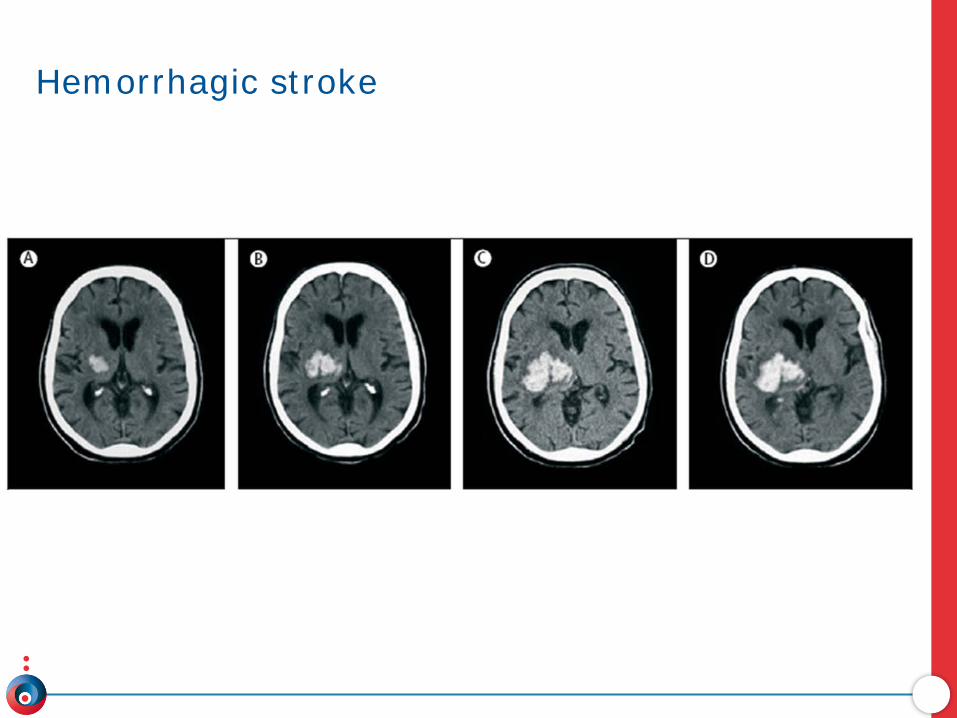
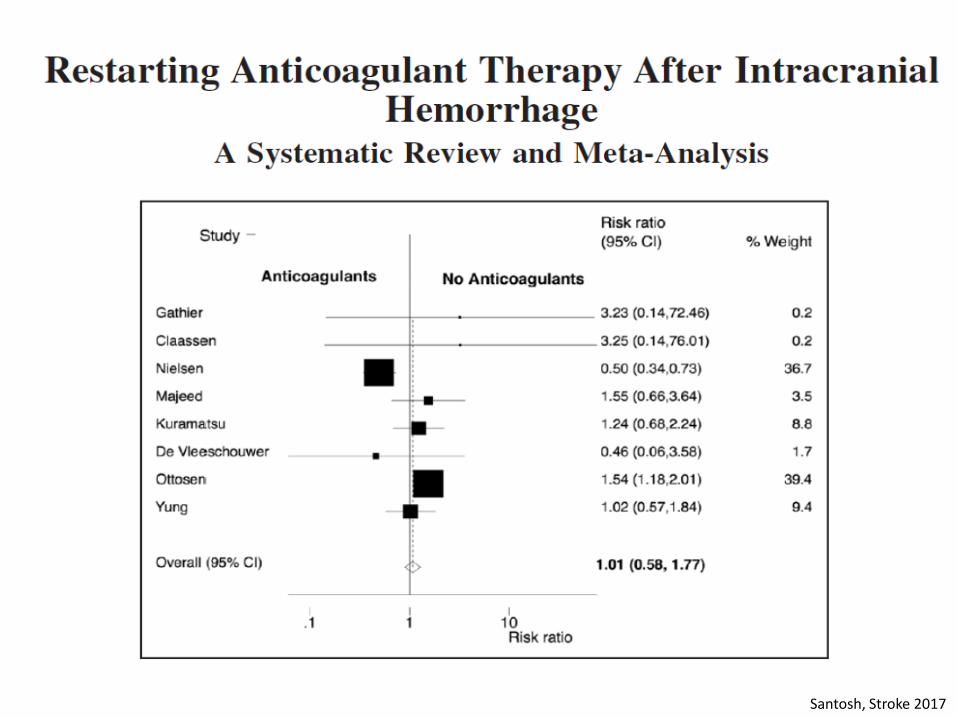
Hemorrhagic stroke

Santosh, Stroke 2017
Santosh, Stroke 2017

Santosh, Stroke 2017

Risk of recurrence
Weimar et al; Cerebrovascular Dis 2011; 32: 283-288

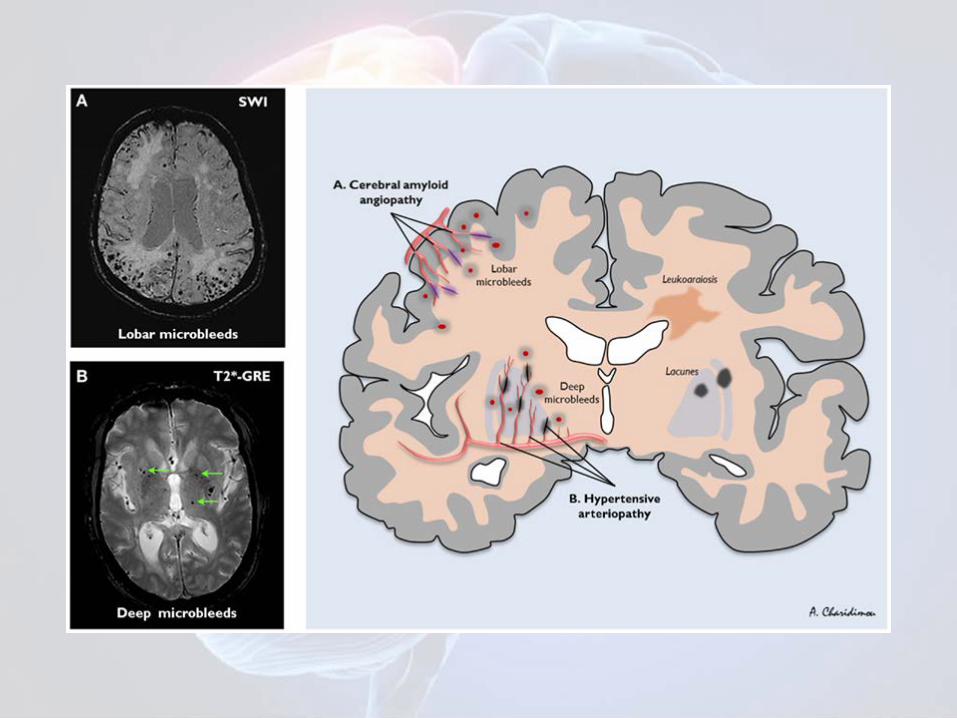
ICH location in patients treated with anticoagulants
Pezzini et al, Neurology 2014
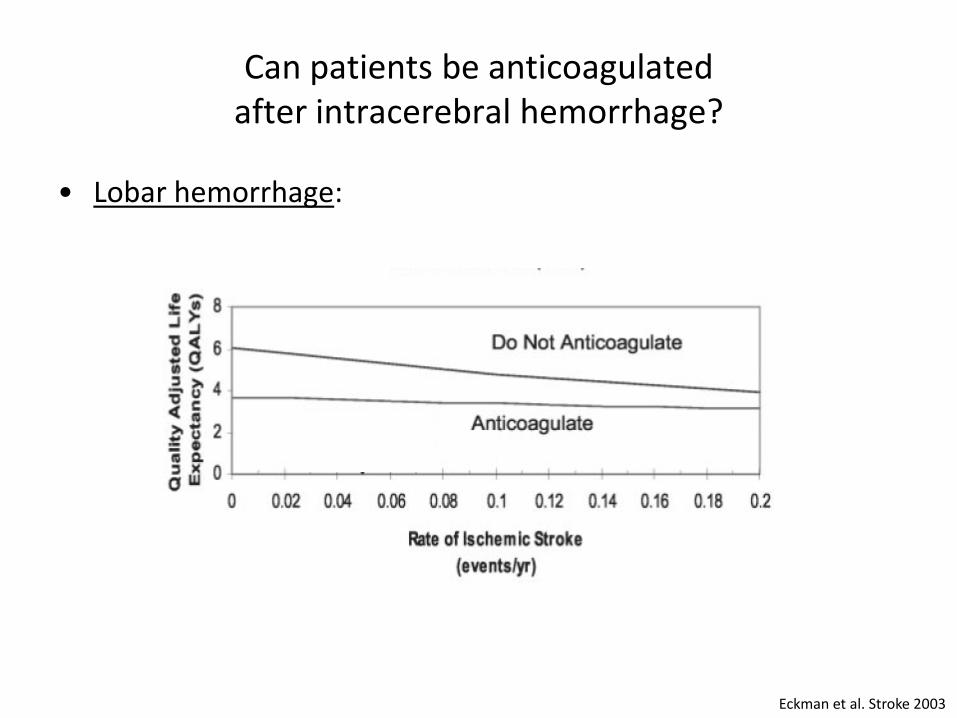
Can patients be anticoagulated after intracerebral hemorrhage?
• Lobar hemorrhage:
Eckman et al. Stroke 2003

Can patients be anticoagulated after intracerebral hemorrhage?
• Deep hemorrhage:
Eckman et al. Stroke 2003

Risk of thromboembolic events
CHADS-Vasc score rate (% year) 1 1.3 2 2.2 3 3.2 4 4.0 5 6.7 6 9.8 >6 >10

Apixaban versus aspirin
Connolly et al, N Engl J Med 2011
