controlled dcd - clodlog.com pathway.pdf · controlled dcd the clinical pathway! dr paul murphy ......
TRANSCRIPT
Controlled DCD The clinical pathway
Dr Paul Murphy National Clinical Lead for Organ Donation NHS Blood and Transplant, UK
1 Swedish Inquiry into organ donation and transplantation. April 2014
Controlled DCD – background
• Background • Key elements of the pathway
• Specific issues – Identification of potential DCD donors
– Family consent
– Resources
• Contribution of DCD to transplantation in the UK
Objectives
Controlled DCD – background
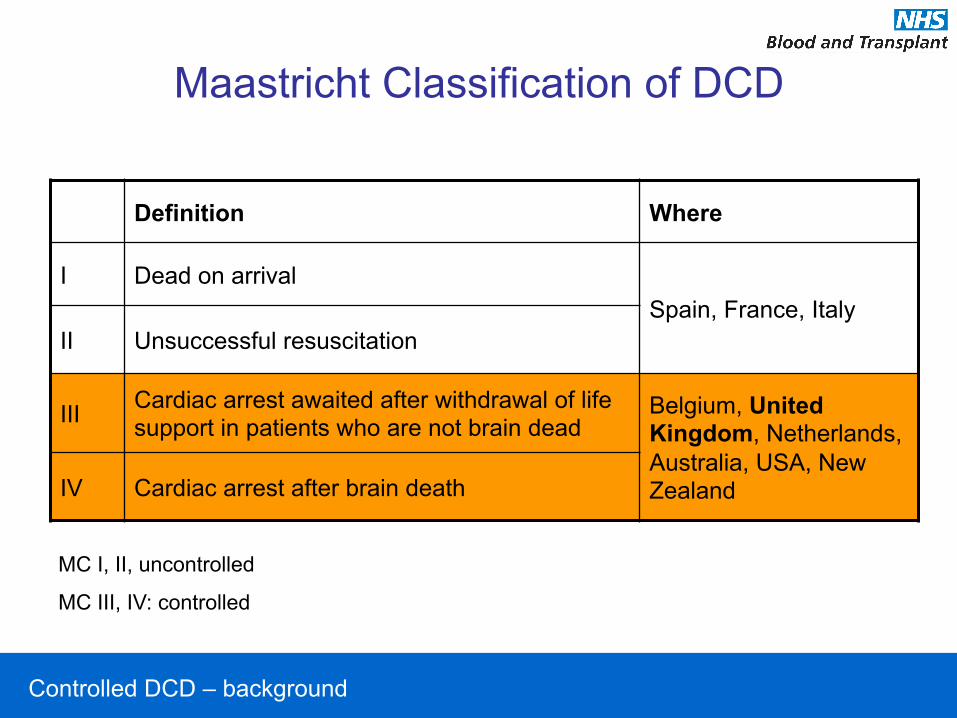
Maastricht Classification of DCD
Definition Where
I Dead on arrival Spain, France, Italy
II Unsuccessful resuscitation
III Cardiac arrest awaited after withdrawal of life support in patients who are not brain dead
Belgium, United Kingdom, Netherlands, Australia, USA, New Zealand IV Cardiac arrest after brain death
MC I, II, uncontrolled
MC III, IV: controlled
Controlled DCD – background
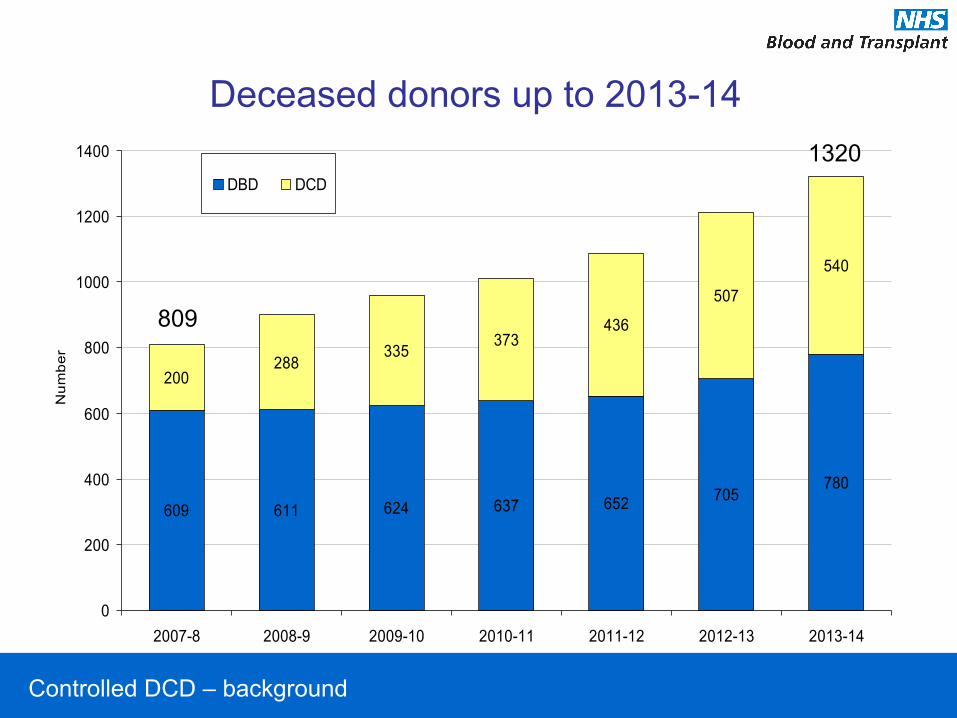
609 611 624 637 652 705780
200288
335373
436
507
540
0
200
400
600
800
1000
1200
1400
2007-8 2008-9 2009-10 2010-11 2011-12 2012-13 2013-14
Num
ber
DBD DCD
809
1320
Deceased donors up to 2013-14
Controlled DCD – background
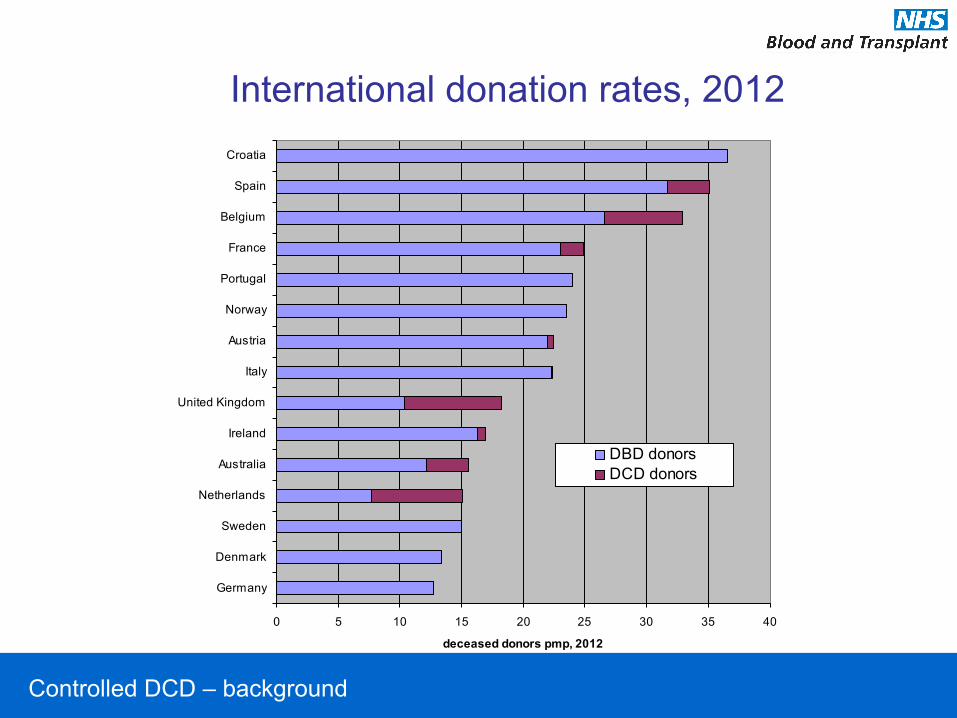
International donation rates, 2012
0 5 10 15 20 25 30 35 40
Germany
Denmark
Sweden
Netherlands
Australia
Ireland
United Kingdom
Italy
Austria
Norway
Portugal
France
Belgium
Spain
Croatia
deceased donors pmp, 2012
DBD donorsDCD donors

Controlled DCD – key elements of the pathway
The Maastricht Category III DCD Pathway
Irreversible loss of circulatory function
Permanent loss of consciousness and respiration
Biochemical collapse and decomposition
ischaemia
Organ retrieval
Organ retrieval after death that follows planned withdrawal of life-sustaining treatments

Controlled DCD – key elements of the pathway
Death on ICU
lack of overall benefit from further treatments
withdrawal
asystole
Multi-organ failure Intolerable disability
diagnosis of death
last offices
As many as 70% of ICU deaths in the UK follow the planned limitation or withdrawal of cardio-respiratory support

Controlled DCD – key elements of the pathway
Impact of DCD on the end of life care
lack of overall benefit
withdrawal
asystole
Multi-organ failure Intolerable disability
diagnosis of death
last offices
lack of overall benefit
delayed withdrawal
asystole
Referral and initial assessment Approach family Continued support Detailed donor assessment and offering Arrival of retrieval team
Expedient diagnosis of death Transfer to theatre Perfusion / retrieval Last offices
?
death death and donation
Controlled DCD – key elements of the pathway
DCD pathway Key considerations
End of life care has to be adjusted if DCD is to be possible
• Donation considered before death – Assessment – who can donate?
– Family approach
• Requires delay in treatment withdrawal – ? Physiological instability
• Altered management of death – Location of treatment withdrawal
– Rapid diagnosis of death
– Rapid transfer to theatre
• Organ ischaemia and stand down of retrieval
Controlled DCD – key elements of the pathway
50% of DCD retrievals in the UK are stood down.
DCD pathway Key considerations
• Donation considered before death – Assessment
– Family approach
• Requires delay in treatment withdrawal – ? Physiological instability
• Altered management of death – Location of treatment withdrawal
– Rapid diagnosis of death
– Rapid transfer to theatre
• Organ ischaemia and stand down of retrieval
Controlled DCD – identification of potential donors
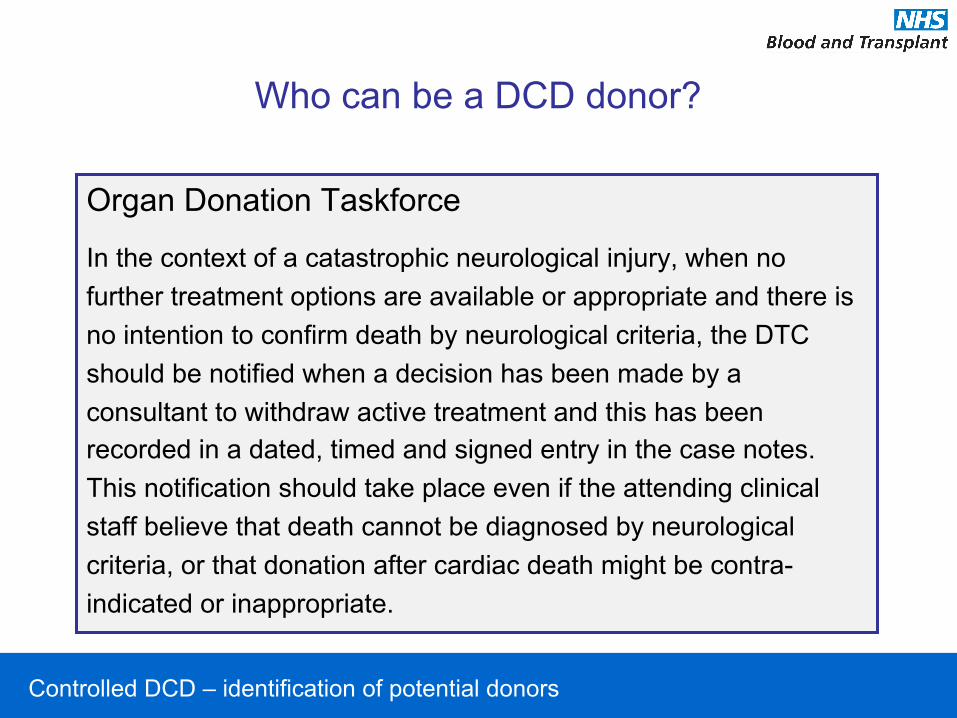
Who can be a DCD donor?
Organ Donation Taskforce
In the context of a catastrophic neurological injury, when no further treatment options are available or appropriate and there is no intention to confirm death by neurological criteria, the DTC should be notified when a decision has been made by a consultant to withdraw active treatment and this has been recorded in a dated, timed and signed entry in the case notes. This notification should take place even if the attending clinical staff believe that death cannot be diagnosed by neurological criteria, or that donation after cardiac death might be contra-indicated or inappropriate.

Controlled DCD – identification of potential donors
Who can donate?
10.4
16.2
12.4
25.9
3.2
5.6
26.3
3.5
4.2
6.2
27.5
7.8
8.0
42.8
0 5 10 15 20 25 30 35 40 45
Other Miscellaneous
Other Medical Disease
Primary Respiratory Disease
Hypoxic Brain Injury
Trauma (including head injury)
Other CVA (thrombotic or unclassified)
Intracranial haemorrhage (non traumatic)
Dia
gnos
tic c
ateg
orie
s
Percentage
Actual DCDs %
Potential DCDs %
UK Potential Donor Audit (October 2009 – March 2012) 7504 patients referred as potential DCD donors 877 actual DCD donors
Controlled DCD – identification of potential donors
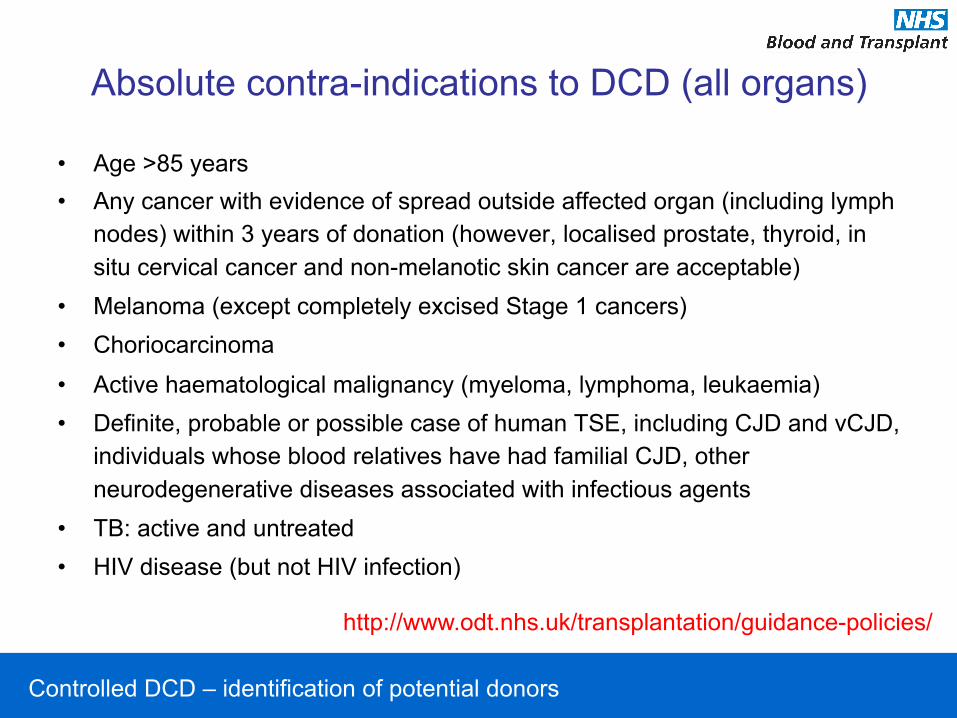
Absolute contra-indications to DCD (all organs)
• Age >85 years • Any cancer with evidence of spread outside affected organ (including lymph
nodes) within 3 years of donation (however, localised prostate, thyroid, in situ cervical cancer and non-melanotic skin cancer are acceptable)
• Melanoma (except completely excised Stage 1 cancers) • Choriocarcinoma
• Active haematological malignancy (myeloma, lymphoma, leukaemia) • Definite, probable or possible case of human TSE, including CJD and vCJD,
individuals whose blood relatives have had familial CJD, other neurodegenerative diseases associated with infectious agents
• TB: active and untreated • HIV disease (but not HIV infection)
http://www.odt.nhs.uk/transplantation/guidance-policies/
Controlled DCD – identification of potential donors
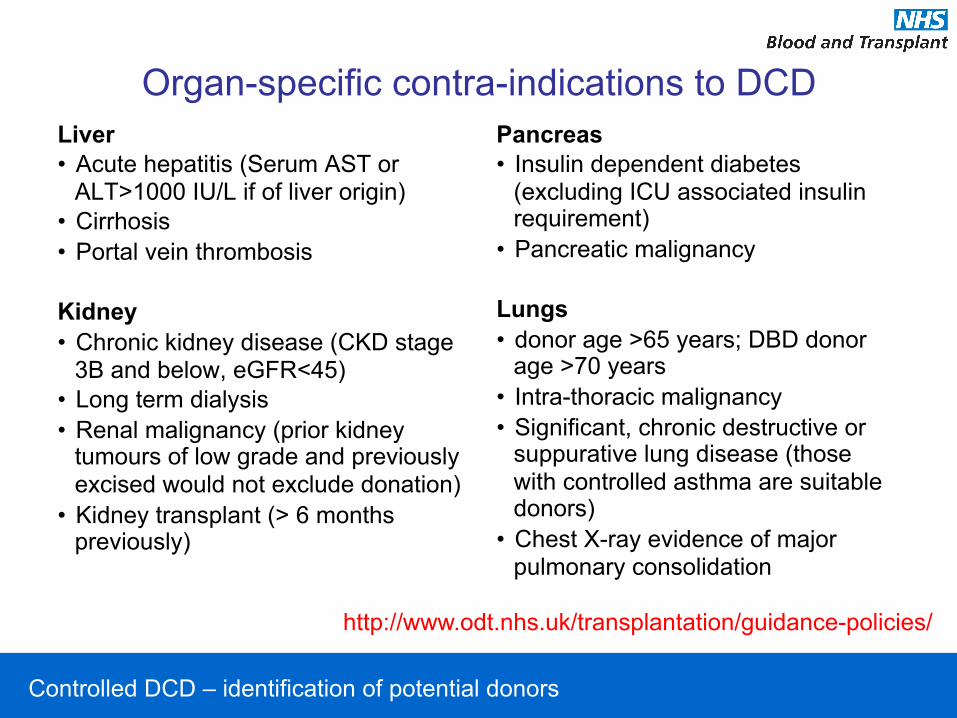
Organ-specific contra-indications to DCD Liver • Acute hepatitis (Serum AST or
ALT>1000 IU/L if of liver origin) • Cirrhosis • Portal vein thrombosis Kidney • Chronic kidney disease (CKD stage
3B and below, eGFR<45) • Long term dialysis • Renal malignancy (prior kidney
tumours of low grade and previously excised would not exclude donation)
• Kidney transplant (> 6 months previously)
Pancreas • Insulin dependent diabetes
(excluding ICU associated insulin requirement)
• Pancreatic malignancy Lungs • donor age >65 years; DBD donor
age >70 years • Intra-thoracic malignancy • Significant, chronic destructive or
suppurative lung disease (those with controlled asthma are suitable donors)
• Chest X-ray evidence of major pulmonary consolidation
http://www.odt.nhs.uk/transplantation/guidance-policies/
Controlled DCD – family consent
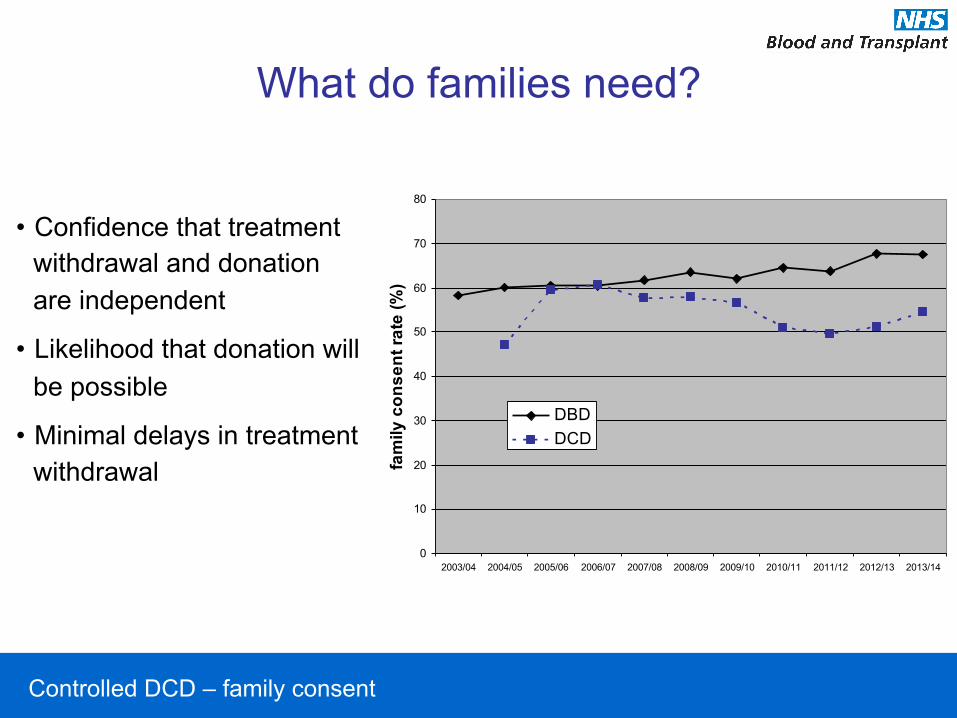
What do families need?
• Confidence that treatment withdrawal and donation are independent
• Likelihood that donation will be possible
• Minimal delays in treatment withdrawal
0
10
20
30
40
50
60
70
80
2003/04 2004/05 2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14
fam
ily c
onse
nt ra
te (%
)DBDDCD

Controlled DCD – family consent
20
30
40
50
60
70
80
2005
/6
2006
/7
2007
/8
2008
/9
2009
/10
2010
/11
2011
/12
2012
/13
2013
/14
Fam
ily c
onse
nt ra
te (%
)
Consent rate when coordinator involved
Consent rate when coordinator not
involved
Impact of coordinator on family consent

Controlled DCD – family consent
Time intervals for the DCD pathway
Time interval Median (hours)
Referral to family consent
3.5
Family consent to arrival of retrieval team(s)
7.7
Arrival of retrieval teams to treatment withdrawal
1.0
Referral to treatment withdrawal
13.8
Speeding up the DCD pathway is a key objective for future interventions in the UK

Controlled DCD – family consent
Reasons for family refusal

Controlled DCD – resource implications
MC III DCD in UK, 2012-13 %
of p
oten
tial D
CD
don
ors
0 10 20 30 40 50 60 70 80 90
100
Potential donors 1
Neurological death tests performed
Neurological death
confirmed Contraindications Family
approach Consent/
authorisation Donation
Potential DCD donor: a patient who had treatment withdrawn and death anticipated within 4 hours Conversion rate 14%
6517
3114
1816
931 449

Controlled DCD – resource implications
Consented donors in UK
0
50
100
150
200
250
300
350
400
450
500
Oct 09 - Mar 10
Apr 10 - Sep 10
Oct 10 - Mar 11
Apr 11 - Sep 11
Oct 11 - Mar 12
Apr 12 - Sep 12
Num
ber o
f pot
entia
l don
ors
whe
re c
onse
nt fo
r do
natio
n ob
tain
ed fr
om fa
mily
Quarter
Consents by quarter
DBD
DCD

Controlled DCD – resource implications
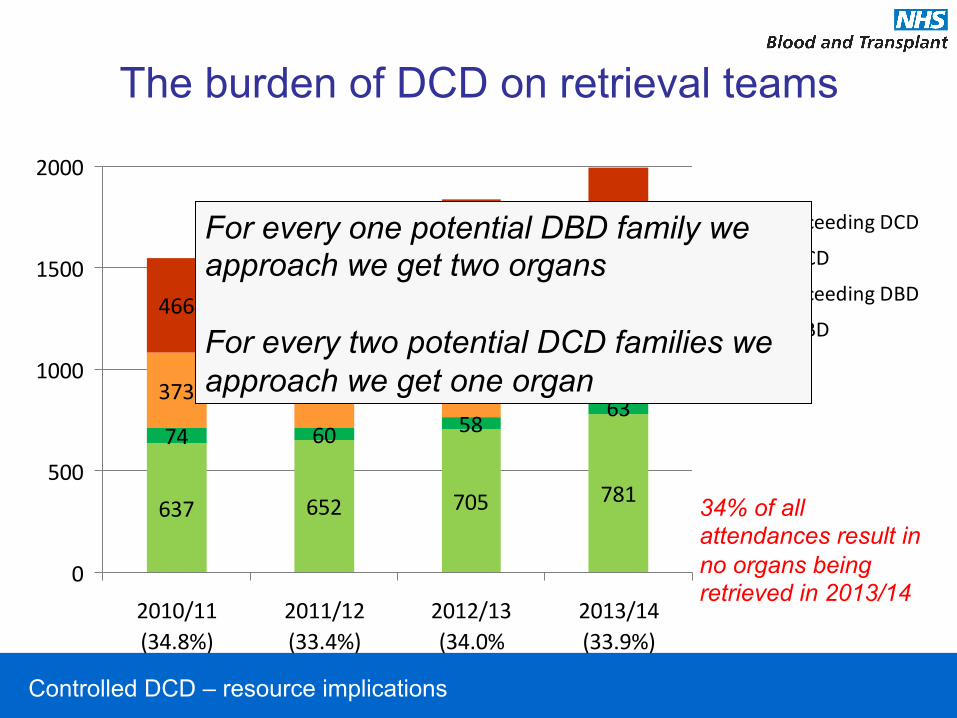
The burden of DCD on retrieval teams
637 652 705 781
74 60 5863
373 436507
539
466 486567
614
0
500
1000
1500
2000
2010/11(34.8%)
2011/12(33.4%)
2012/13(34.0%
2013/14(33.9%)
Non-‐proceeding DCD
Actual DCD
Non-‐proceeding DBD
Actual DBD
34% of all attendances result in no organs being retrieved in 2013/14
Controlled DCD – resource implications
The burden of DCD on retrieval teams
637 652 705 781
74 60 5863
373 436507
539
466 486567
614
0
500
1000
1500
2000
2010/11(34.8%)
2011/12(33.4%)
2012/13(34.0%
2013/14(33.9%)
Non-‐proceeding DCD
Actual DCD
Non-‐proceeding DBD
Actual DBD
34% of all attendances result in no organs being retrieved in 2013/14
For every one potential DBD family we approach we get two organs For every two potential DCD families we approach we get one organ

Controlled DCD – outcomes
Contribution of DCD to organ transplantation in the UK, 2012-13
living DBD DCD % total
Kidney1 1068 1167 749 25
Liver 31 637 136 17
Lung 0 153 34 18
Pancreas
0 33 5 13
Heart - 145 0 0
1Includes kidney and pancreas
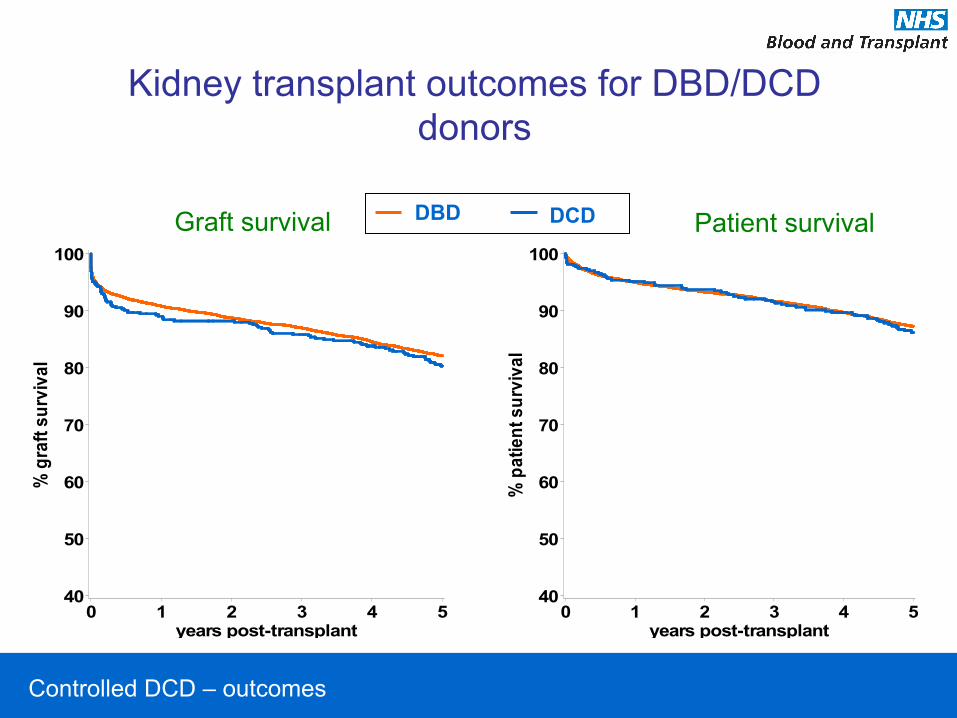
Controlled DCD – outcomes
Kidney transplant outcomes for DBD/DCD donors
Graft survival
% g
raft
surv
ival
40
50
60
70
80
90
100
years post-transplant0 1 2 3 4 5
% p
atie
nt s
urvi
val
40
50
60
70
80
90
100
years post-transplant0 1 2 3 4 5
DCD DBD Patient survival
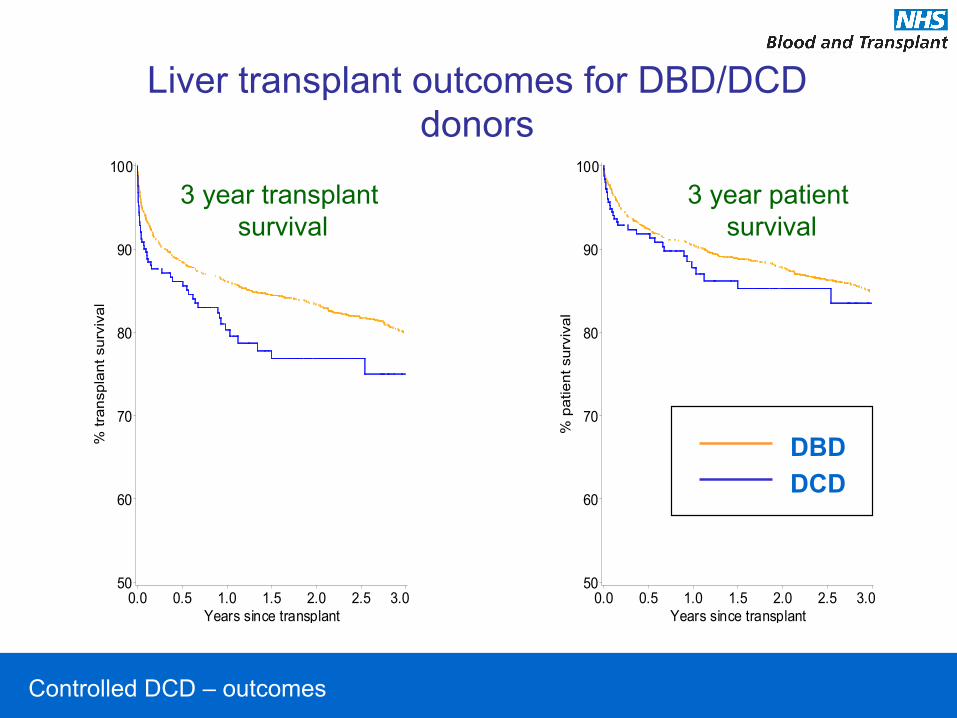
Controlled DCD – outcomes
DBDDCD
3 year patient survival
% p
atie
nt s
urvi
val
50
60
70
80
90
100
Years since transplant0.0 0.5 1.0 1.5 2.0 2.5 3.0
3 year transplant survival
% tr
ansp
lant
sur
viva
l
50
60
70
80
90
100
Years since transplant0.0 0.5 1.0 1.5 2.0 2.5 3.0
Liver transplant outcomes for DBD/DCD donors

Controlled DCD – key elements of the pathway
Summary
• MC III DCD embedded into UK donation and transplantation
• Not restricted to patients dying of acute brain injury
• The needs of the donor families are rather different compared to DBD
• Very resource intensive