figo’s updated recommendations for misoprostol used alone...
TRANSCRIPT

Int J Gynecol Obstet 2017; 1–4 wileyonlinelibrary.com/journal/ijgo | 1© 2017 International Federation of Gynecology and Obstetrics
DOI: 10.1002/ijgo.12181
F I G O S P E C I A L A R T I C L E
FIGO’s updated recommendations for misoprostol used alone in gynecology and obstetrics
Jessica L. Morris1,* | Beverly Winikoff2 | Rasha Dabash2 | Andrew Weeks3 | Anibal Faundes4 | Kristina Gemzell-Danielsson5 | Nathalie Kapp6 | Laura Castleman6,7 | Caron Kim8 | Pak Chung Ho9 | Gerard H.A. Visser10
1InternationalFederationofGynecologyandObstetrics,London,UK2GynuityHealthProjects,NewYork,NY,USA3DepartmentofWomen’sandChildren’sHealth,UniversityofLiverpool,Liverpool,UK4DepartmentofObstetricsandGynecology,UniversityofCampinas,SãoPaulo,Brazil5DepartmentofWomen’sandChildren’sHealth,KarolinskaInstitutet,Stockholm,Sweden6Ipas,ChapelHill,NC,USA7UniversityofMichigan,AnnArbor,MI,USA8Independentconsultant9TheUniversityofHongKong,HongKong,China10UniversityMedicalCenter,Utrecht,Netherlands
*CorrespondenceJessicaL.Morris,InternationalFederationofGynecologyandObstetrics,London,UK.Email:[email protected]
1 | BACKGROUND
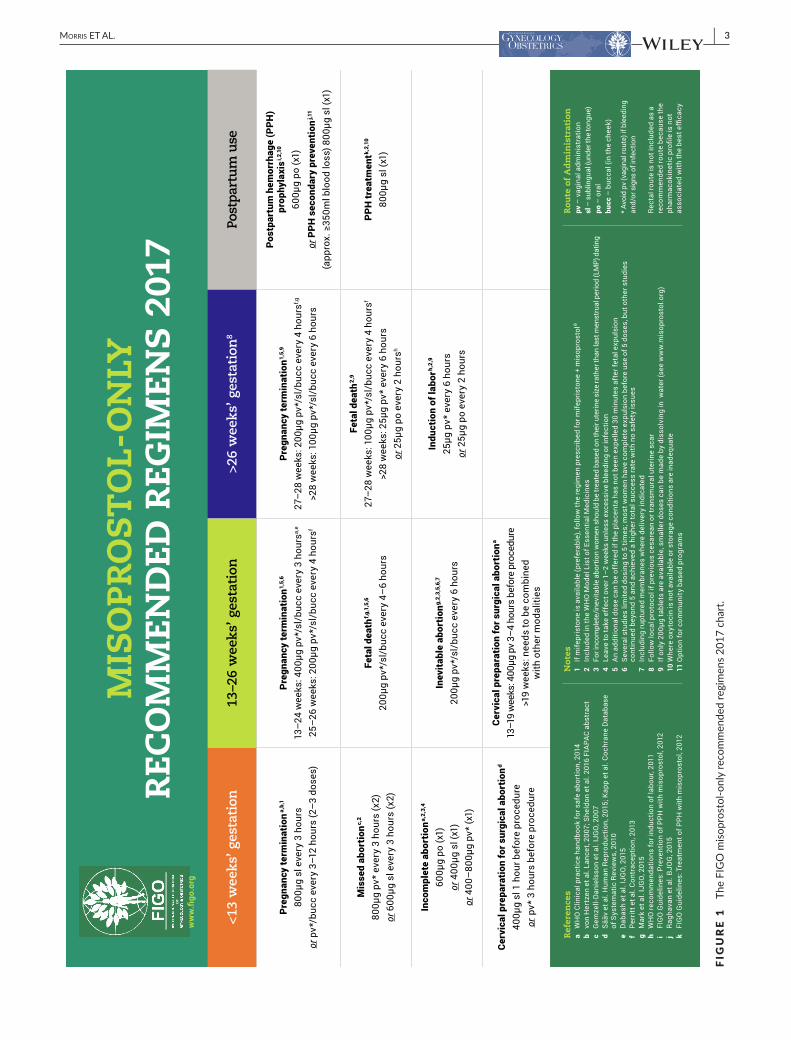
In 2012, the International Federation of Obstetrics andGynecology(FIGO)producedachartdetailingrecommendeddos-agesofmisoprostolwhenusedalone,foravarietyofgynecologicandobstetricindications.Inlightofnewevidence1–13andthroughexpertdeliberation,thischarthasnowbeenrevisedandexpanded(Fig.1).Someareaswereparticularlychallengingtodevelopgiventhe limited, low-quality, or inconsistent evidence. The presentcommentaryisintendedtoexplainsomeofthechangesanddeci-sionsmade.
2 | GENERAL CHANGES
Thelayoutisnowcategorizedverticallybygestationandhorizontallyby indication.Gestation is labelledandreferredtoasthenumberofweeksofgestation (<13weeks,13–26weeks, and>26weeks),withthefinal columnbeing forpostpartumuse.However, in the caseofincompleteabortionunder13weeks,andinevitableabortionbetween13–26weeks,womenshouldbetreatedonthebasisoftheiruterinesizeratherthanlastmenstrualperioddating.Recommendationshavebeenaddedforinevitableabortionandcervicalpreparationbetween
13 and 26weeks, and for termination of pregnancy at more than26weeks.
3 | NUMBER OF DOSES
Forlessthan13weeks’gestation,wedecidedtorecommendafixednumberofdoseswithoutspecifyingamaximum.Thisisbecausemanyearlypregnancyregimenswillbeusedonanoutpatientbasis,soitisusefulforhealthcareproviderstoknowinadvancehowmanydosestogivetheclient;thereisalsosufficientevidencetosupportafixednumberofdosesforuseinpregnanciesoflessthan13weeks’gesta-tion,aswellasevidencethatitissafetogivefurtherdosesiftheyarerequired.1–4,14
For13–26weeks’gestation,thenotionofamaximumnumberofdoseshasbeenextrapolatedfromclinicalresearchinwhichmaximumdosesarecommonlynotednotonthebasisofpatientsafetyissuesorefficacy,9butratherastangibleendpoints.Inclinicalpractice,however,they might not have great utility, and dosing should continue untilexpulsion,intheabsenceofrarecomplications.Suggestingthatprovid-ersshoulddiscontinuedosingcouldactuallyincreaserisks,particularlywhenprovidershavefewalternativesavailableifexpulsionhasnotyetoccurred.Someunpublishedstudiesandclinicalexperiencehaveshown

2 | Mooris ET AL
thatcompleteexpulsioncanbesafelyachievedbycontinuingtheregi-menupto72hours,withoutcompromisingthewoman’ssafety.9
4 | ROUTE OF ADMINISTRATION
Given recently published evidence,2–9 we have added alternativeroutes for taking misoprostol; in most cases, this has meant theadditionofthebuccalroute,inwhichthetabletsareplacedinthecheekfor30minutesafterwhichanyremnantsareswallowed.Thisroute has a similar pharmacokinetic profile to the vaginal route.Furtherongoingstudiesareindicatingthistobeapromisingrouteforother indicationson the chart, but these indicationshavenotbeen included because data on efficacy have not been reported.Future studies will continue to provide evidence on what mightbe a variety of effective regimens and routes of administration.Althoughthiscouldresultinseveralavailableoptionsforproviders,it will also enable women’s preferences to be taken into consid-eration.Women’spreferences canvary,with somepreferring thevaginalroute(ifinsertingthepillsthemselves)andsomepreferringnon-vaginalroutes.However,thevaginalrouteshouldbeavoidedwhenthereisbleedingand/orsignsofinfection.Thechartdoesnotinclude the rectal route.We recommend against using this routebecausethepharmacokineticprofileisnotassociatedwiththebestefficacy.
5 | MISOPROSTOL USE IN PREGNANCIES WITH PREVIOUS CESAREAN OR TRANSMURAL UTERINE SCAR
The use of misoprostol at 13–26weeks’ gestation in women withpreviouscesareanortransmuraluterinescarwasdebatedbecauseofconcernsaboutan increasedriskofuterinerupture.Forfetaldeath,aCochranemeta-analysis15reportedmixedfindings,concludingthatthedatawereinsufficienttoassesstheoccurrenceofuterinerupture.Afewstudieshavereportednoincreasedlikelihoodofrupture,16 but oftenwomenwithpriorcesareanoruterinesurgeryareexcludedfromstudiesorreviews,ortrialsareinsufficientlypoweredtodetectadif-ferenceinsafetyoutcomesasaresultoftherarityofmajoradverseevents.Thereissomeevidencethat,forterminationsinthisperiod,theriskofuterineruptureamongwomenwithapriorcesareandeliveryusingmisoprostolislessthan0.3%1,17;otherstudies9,18–20concludedthattherearenosignificantdifferencesinoutcomesforwomenwithpreviouscesarean(s).Wethereforeconcludedthatmisoprostolcanbeusedforwomenwithpreviouscesareanorothertransmuraluterinescarthroughout13–26weeks.
Thereisinsufficientevidenceavailabletorecommendaregimenofmisoprostolforuseatmorethan26weeks’gestationinwomenwho have had a previous cesarean or transmural uterine scar.Therefore,withoutevidencetosupportasaferegimen,wedonotprovide one, other than to recommend following local protocol inthesecases.
6 | MANAGEMENT OF PREGNANCY TERMINATION AND FETAL DEATH OVER 26 WEEKS’ GESTATION
Althoughthere issomeevidencetosupportadecreasingdosewithincreasinggestationalage,thereislittleevidencetosupporttheadvicegiven in some international and national clinical guidelines to uselowerdosesofmisoprostolincasesoffetaldeath.Irrespectiveoftheissueofrecommendationsfordifferentdoses,variousreviews15,20,21 haveconcludedthatthereisinsufficientevidenceoverallofsuperior-ity of onedoseor schedule ofmisoprostol over another for use inpregnancies at or over 13weeks’ gestation. In making recommen-dations,weacknowledged thatprovidersmightbekeen to identifylowestpossibledosesbecauseofreducedadverseeffects,21butthatitwasalsoimportanttoconsidersuccessratesandtimetodelivery:lowdoseshavebeenshowntobeassociatedwithalongerinduction-to-delivery interval and lower overall effectiveness,15,21 and evi-dencehassupportedthesafetyofthe“higher”dosesforwomen.7–9 Recommendationsinthechartwerecompiledwiththisinmind,whilealsoacknowledgingthatitispossiblethatarangeofdosagescouldbeeffectiveandsafe.
7 | RETAINED PLACENTA
Therehavebeentwostudiesoftheuseofmisoprostolforthetreat-mentofretainedplacentafollowinglivebirth,neitherofwhichshowany benefit over placebo.22We therefore do not recommendmis-oprostolforretainedplacentainlatepregnancy.
8 | SECONDARY PREVENTION OF POSTPARTUM HEMORRHAGE FOR COMMUNITY- BASED PROGRAMS
Secondaryprevention isacommunity-basedstrategy thathasbeenshown to be a comparable alternative to a universal prophylaxisapproachintwolargecommunitytrials(oneinpress).12Ratherthanmedicatingallwomenduringthethirdstageoflaborwithaprophy-lacticdose,aregimenof800μgsublingualmisoprostol(thesameasfor treatment) can be used to treat onlywomenwith higher-than-averagebleeding(e.g.approximately350mLormore).Althoughthereislimitedpublisheddata,itwasagreedthatsecondarypreventionofPPHisastrongalternativeapproachtouniversalprophylaxis,becauseit involves medicating far fewer women (5%–10% vs 100%), thuscausingfeweradverseeffectsandreducingcosts.
9 | CONCLUSION
The FIGO Misoprostol-only Recommended Regimens 2017 chart(Fig.1)istheresultofextensivecollaborationamonganinternational
| 3Mooris ET AL
FIGURE 1 TheFIGOmisoprostol-onlyrecommendedregimens2017chart.

4 | Mooris ET AL
expert group. It has been endorsed by the FIGO Prevention ofUnsafe AbortionWorking Group and the FIGO SafeMotherhoodandNewbornHealthCommittee,andapprovedbytheFIGOOfficers.Available in other languages and formats fromhttp://figo.org, it ishopedthatitwillbeaswidelydistributedandusedasthepreviousversion.Although these recommendeddosageshavebeendecidedonthebasisofcurrentevidenceavailableandexpertopinion,newevidenceisregularlyemergingandthusthereisaneedtoreviewandrevisetheserecommendationsinthefuture.
Misoprostolisanimportantmedicineand,althoughitshouldnotbe used in preference over oxytocin for postpartum hemorrhage,or instead of mifepristone plusmisoprostol for pregnancy termina-tion, it couldbe theonlymedicineavailable insomecircumstances,which iswhyFIGObelievesthis “misoprostol-only”chart isneeded.Misoprostolmustcontinuetobehighlightedasanessentialmedicineand included in international documents, national guidelines, andessentialmedicines lists.Further,wemustworktoensuretheavail-abilityofhigh-qualitymisoprostol,andtheestablishmentofpolicyandprogramsthatsupportitsavailabilityanduse.
The recentWHOguidelinesonhealthworker roles inprovidingsafeabortioncare23outlineawidevarietyofhealthcareproviderswhocanmanagemedical abortion andpostabortion care in thefirst tri-mester,withauxiliarynurses,nurses,andmidwives listed,aswellaslayhealthworkersanddoctorsofcomplementarysystemsforsomesubtasks.Womencanalsofulfillsomeofthecomponentsofassess-mentandmanagementthemselvesoutsideofahealthcarefacility.ItisanticipatedthatthismisoprostolchartcanbeusedbyallhealthcareprovidersidentifiedintheWHOpublicationandthatbyimplementingboth,wewillcomeclosertoachievingoptimalcareforthewomenweaimtoserve.
AUTHOR CONTRIBUTIONS
Allauthorscontributedtothedevelopmentofthechartandthewrit-ingofthecommentary.
REFERENCES
1. WHO. Clinical Practice Handbook for Safe Abortion. Geneva:WorldHealthOrganization;2014.
2. vonHertzenH,PiaggioG,HuongNT,etal.Efficacyoftwointervalsand two routesof administrationofmisoprostol for terminationofearly pregnancy:A randomised controlled equivalence trial. Lancet. 2007;369:1938–1946.
3. SheldonW,DzubaI,SayetteH,DurocherJ,WinikoffB.BuccalversussublingualmisoprostolaloneforearlypregnancyterminationinlegallyrestrictedLatinAmericansettings:A randomized trial.PresentedatFIAPAC;2016,Lisbon,Portugal.FC25.
4. Gemzell-Danielsson K, Ho PC, Gómez Ponce de León R,Weeks A, Winikoff B. Misoprostol to treat missed abortionin the first trimester. Int J Gynecol Obstet. 2007;99(Suppl.2): S182–S185.
5. Sääv I, Kopp Kallner H, Fiala C, Gemzell-Danielsson K. Sublingualversus vaginal misoprostol for cervical dilatation 1 or 3 h prior to
surgical abortion: A double-blinded RCT. Hum Reprod. 2015;30: 1314–1322.
6. Kapp N, Lohr PA, Ngo TD, Hayes JL. Cervical preparation forfirst trimester surgical abortion. Cochrane Database Syst Rev. 2010;2:CD007207.
7. Dabash R, Chelli H, Hajri S, ShochetT, Raghavan S,Winikoff B.Adouble-blindrandomizedcontrolledtrialofmifepristoneorplacebobeforebuccalmisoprostolforabortionat14–21weeksofpregnancy.Int J Gynecol Obstet. 2015;130:40–44.
8. MarkAG,EdelmanA,BorgattaL.Second-trimesterpostabortioncareforrupturedmembranes,fetaldemise,andincompleteabortion.Int J Gynecol Obstet. 2015;129:98–103.
9. Perritt JB, Burke A, Edelman AB. Interruption of nonviable preg-nanciesof24-28weeks’ gestationusingmedicalmethods:Releasedate June 2013 SFP guideline #20133. Contraception. 2013;88: 341–349.
10. WHO.WHO recommendations for induction of labour.Geneva:WorldHealthOrganization;2011.
11. InternationalFederationofGynecologyandObstetrics.PreventionofPost-PartumHaemorrhagewithMisoprostol:FIGOGuidelineinbrief.Published 2012. http://www.figo.org/sites/default/files/uploads/project-publications/Miso/PPH%20prevention/Prevention%20of%20PPH%20with%20Misoprostol_In%20Brief_2012_English.pdf.AccessedOctober17,2016.
12. RaghavanS,GellerS,MillerS,etal.Misoprostolforprimaryversussec-ondarypreventionofpostpartumhaemorrhage:Acluster-randomisednon-inferioritycommunitytrial.BJOG. 2016;123:120–127.
13. InternationalFederationofGynecologyandObstetrics.TreatmentofPost-PartumHaemorrhagewithMisoprostol:FIGOGuidelineinbrief.Published 2012. http://www.figo.org/sites/default/files/uploads/project-publications/Miso/PPH%20treatment/Treatment%20of%20PPH%20with%20Misoprostol_In%20Brief_2012_English.pdf.AccessedOctober17,2016.
14. GynuityHealthProjects.AbortionInductionwithMisoprostolAloneinPregnanciesThrough9Weeks’LMP.Published2013.http://gynu-ity.org/resources/read/misoprostol-for-early-abortion-en/.AccessedOctober17,2016.
15. DoddJM,CrowtherCA.Misoprostol for inductionof labourtoter-minatepregnancyinthesecondorthirdtrimesterforwomenwithafetalanomalyorafterintrauterinefetaldeath.Cochrane Database Syst Rev.2010;4:CD004901.
16. Gómez PdLR, Wing D, Fiala C. Misoprostol for intrauterine fetaldeath.Int J Gynecol Obstet.2007;99(Suppl.2):S190–S193.
17. Goyal V. Uterine rupture in second-trimester misoprostol-inducedabortionaftercesareandelivery:Asystematicreview.Obstet Gynecol. 2009;113:1117–1123.
18. NaguibAH,MorsiHM,BorgTF,FayedST,HemedaHM.Vaginalmiso-prostolforsecond-trimesterpregnancyterminationafteroneprevi-ouscesareandelivery.Int J Gynecol Obstet. 2010;108:48–51.
19. FawzyM,Abdel-HadyE-S.Midtrimesterabortionusingvaginalmiso-prostolforwomenwiththreeormorepriorcesareandeliveries.Int J Gynecol Obstet. 2010;110:50–52.
20. AllenR,O’BrienBM.Usesofmisoprostolinobstetricsandgynecol-ogy. Rev Obstet Gynecol. 2009;2:159–168.
21. WildschutH,BothMI,MedemaS,ThomeeE,WildhagenMF,KappN. Medical methods for mid-trimester termination of pregnancy.Cochrane Database Syst Rev.2011;1:CD005216.
22. Grillo-Ardila CF, Ruiz-Parra AI, Gaitán HG, Rodriguez-Malagon N.Prostaglandins for management of retained placenta. Cochrane Database Syst Rev.2014;5:CD010312.
23. WHO.Health worker roles in providing safe abortion care and post-abor-tion contraception.Geneva:WorldHealthOrganization;2015.